A Pervasive Pulmonary Function Estimation System with Six-Minute Walking Test


Abstract
:1. Introduction
2. Methods
2.1. Enrolled Subjects and Study Design
2.2. The Six-Minute Walking Test
2.3. Pulmonary Function Test
2.4. BORG Scale
2.5. The Predicted Formula Development
2.6. Statistics
3. Pervasive Estimation System
3.1. Information Management
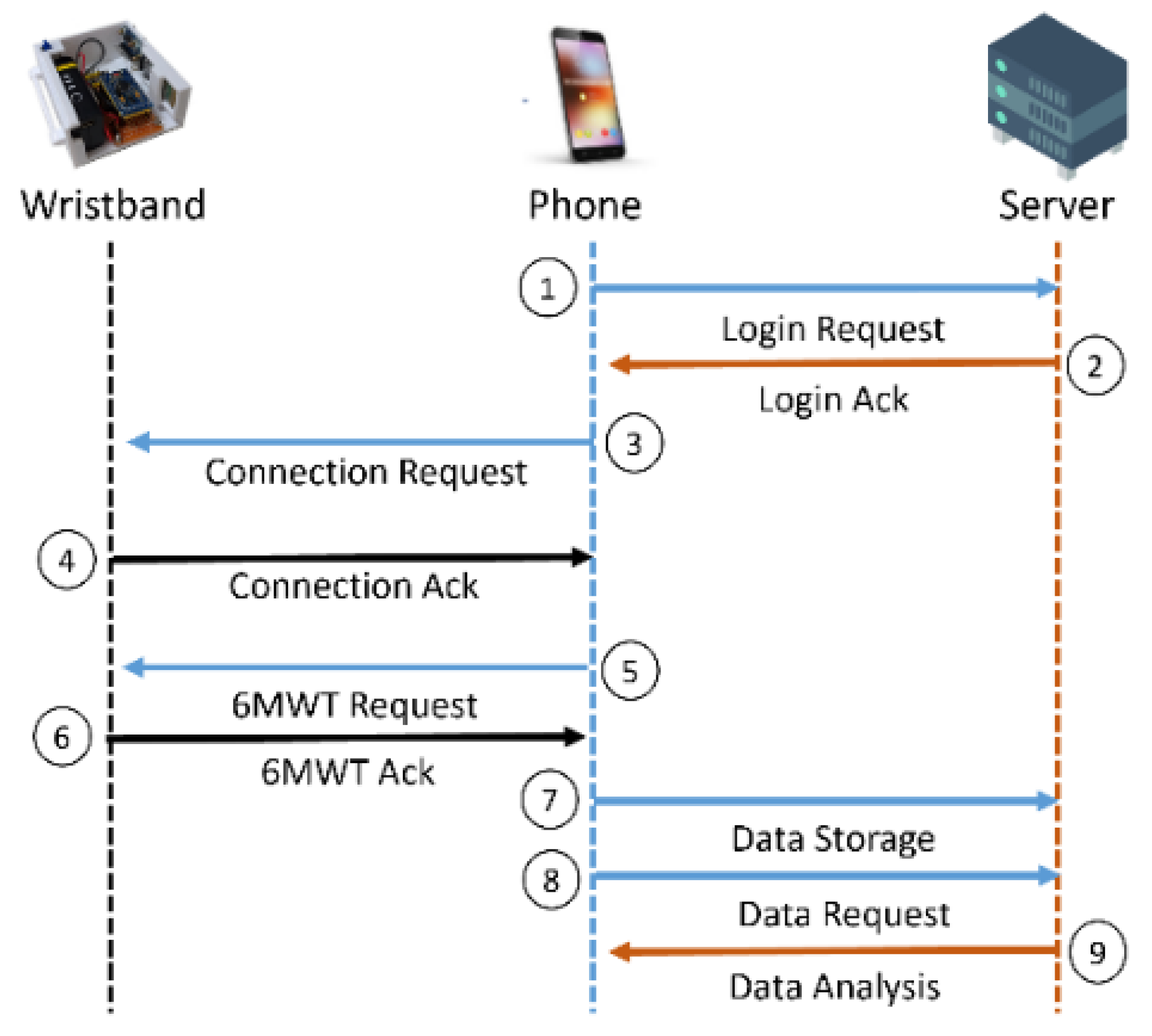
3.2. Communication Protocol
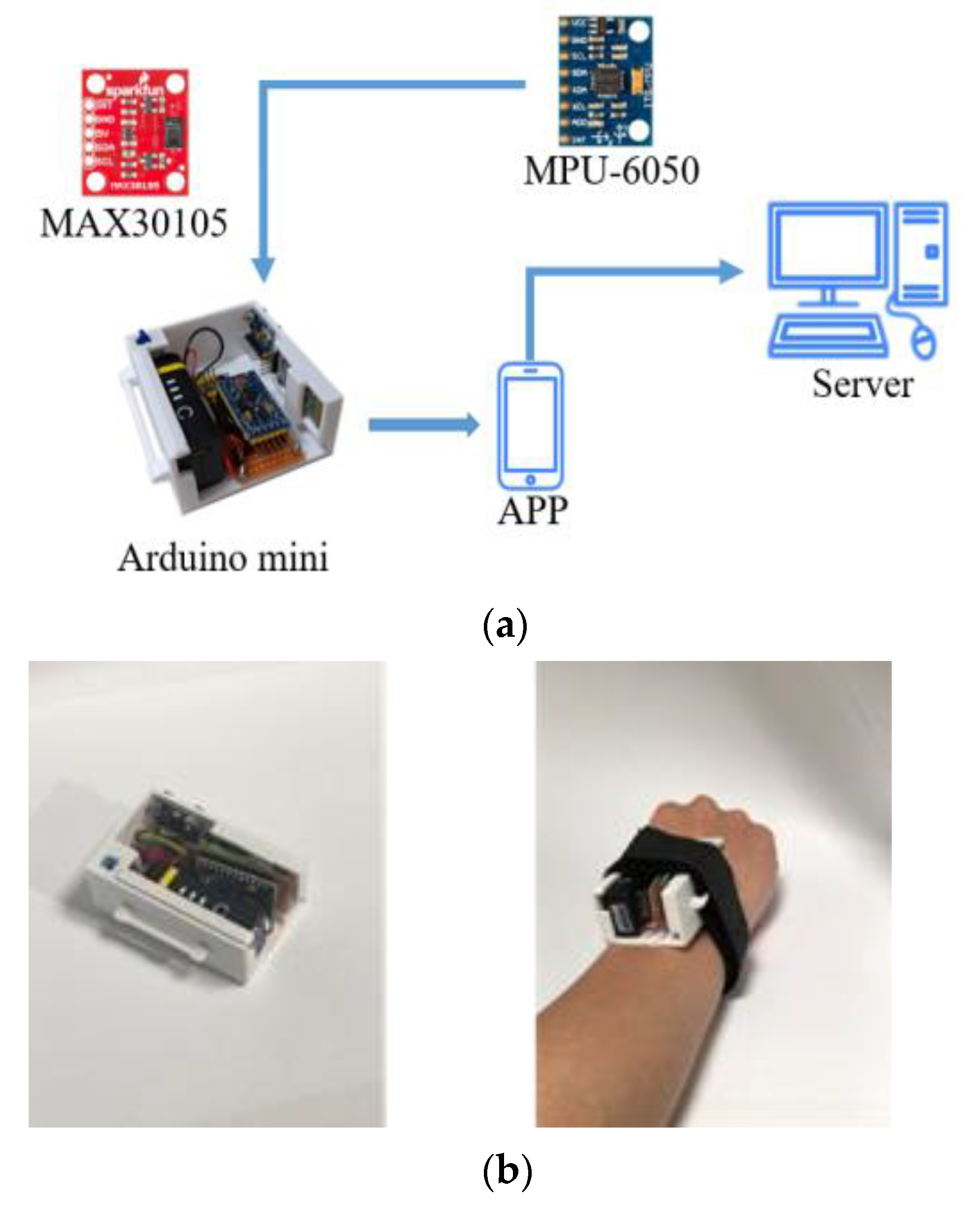
3.3. Hardware/Software Implementation
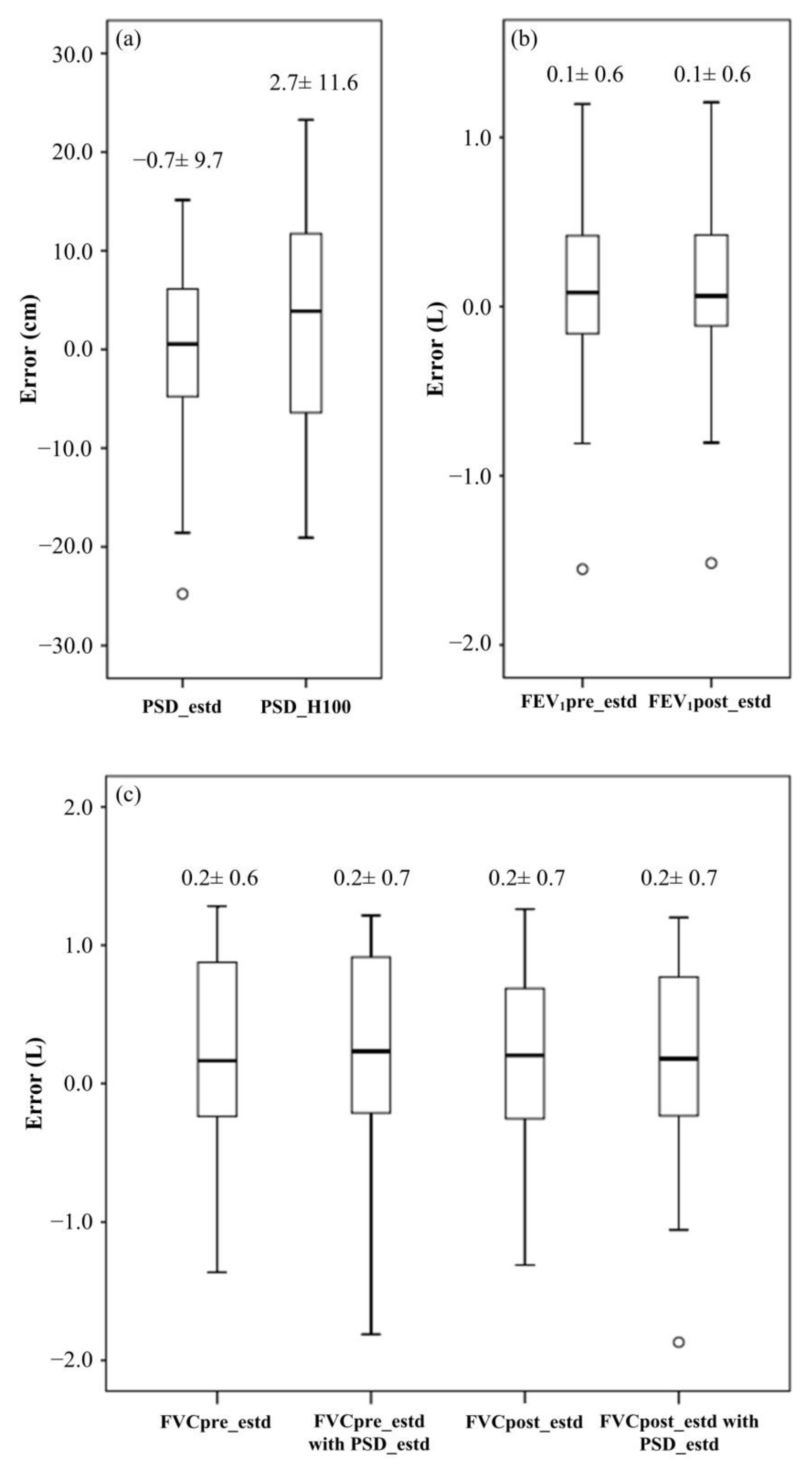
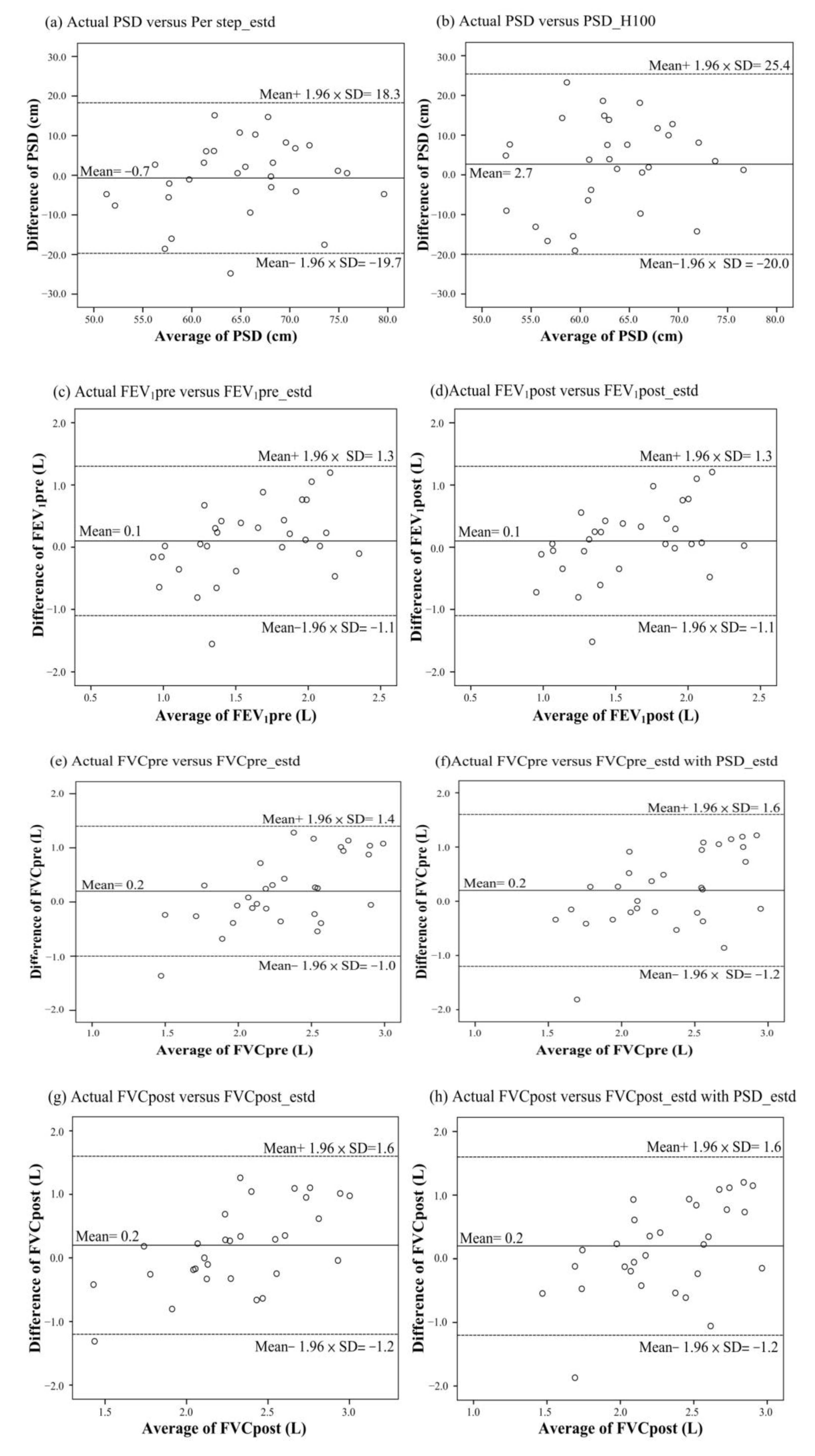
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Heckman, E.J.; O’Connor, G.T. Pulmonary function tests for diagnosing lung disease. JAMA 2015, 313, 2278–2279. [Google Scholar] [CrossRef] [PubMed]
- Ranu, H.; Wilde, M.; Madden, B. Pulmonary function tests. Ulster Med. J. 2011, 80, 84–90. [Google Scholar] [PubMed]
- Gallucci, M.; Carbonara, P.; Pacilli, A.M.G.; di Palmo, E.; Ricci, G.; Nava, S. Use of Symptoms Scores, Spirometry, and Other Pulmonary Function Testing for Asthma Monitoring. Front. Pediatr. 2019, 7, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lommatzsch, M.; Virchow, J.C. Severe asthma: Definition, diagnosis and treatment. Dtsch. Arztebl. Int. 2014, 111, 847–855. [Google Scholar] [PubMed] [Green Version]
- Bateman, E.D.; Hurd, S.S.; Barnes, P.J.; Bousquet, J.; Drazen, J.M.; FitzGerald, J.M.; Gibson, P.; Ohta, K.; O’Byrne, P.; Pedersen, S.E.; et al. Global strategy for asthma management and prevention: GINA executive summary. Eur. Respir. J. 2008, 31, 143–178. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Diego, I.; Bueno, P.; Casas-Maldonado, F.; Miravitlles, M. Geographic distribution of COPD prevalence in the world displayed by Geographic Information System maps. Eur. Respir. J. 2019, 54, 1900610. [Google Scholar] [CrossRef]
- Ho, T.; Cusack, R.P.; Chaudhary, N.; Satia, I.; Kurmi, O.P. Under- and over-diagnosis of COPD: A global perspective. Breathe 2019, 15, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Troosters, T.; Casaburi, R.; Gosselink, R.; Decramer, M. Pulmonary rehabilitation in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 172, 19–38. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.H.; Cho, Y.S.; Joo, S.Y.; Seo, C.H. The Effect of a Pulmonary Rehabilitation on Lung Function and Exercise Capacity in Patients with Burn: A Prospective Randomized Single-Blind Study. J. Clin. Med. 2020, 9, 2250. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories, ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. Available online: https://www.atsjournals.org/doi/10.1164/ajrccm.166.1.at1102 (accessed on 14 December 2021). [CrossRef] [PubMed]
- Hernandes, N.A.; Wouters, E.F.; Meijer, K.; Annegarn, J.; Pitta, F.; Spruit, M.A. Reproducibility of 6-minute walking test in patients with COPD. Eur. Respir. J. 2011, 38, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, S.; Nagaya, N.; Satoh, T.; Kyotani, S.; Sakamaki, F.; Fujita, M.; Nakanishi, N.; Miyatake, K. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension. Comparison with cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2000, 161, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coquart, J.B.; Lemaître, F.; Castres, I.; Saison, S.; Bart, F.; Grosbois, J.M. Reproducibility and Sensitivity of the 6-Minute Stepper Test in Patients with COPD. Copd 2015, 12, 533–538. [Google Scholar] [CrossRef]
- Iritani, O.; Okuno, T.; Hama, D.; Kane, A.; Kodera, K.; Morigaki, K.; Terai, T.; Maeno, N.; Morimoto, S. Clusters of COVID-19 in long-term care hospitals and facilities in Japan from 16 January to 9 May 2020. Geriatr. Gerontol. Int. 2020, 20, 715–719. [Google Scholar] [CrossRef]
- Kronenfeld, J.P.; Penedo, F.J. Novel Coronavirus (COVID-19): Telemedicine and remote care delivery in a time of medical crisis, implementation, and challenges. Transl. Behav. Med. 2021, 11, 659–663. [Google Scholar] [CrossRef]
- Ryu, S. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth 2009 (Global Observatory for eHealth Series, Volume 2). Healthc. Inform. Res. 2012, 18, 153–155. [Google Scholar] [CrossRef]
- Mendez, I.; Van den Hof, M.C. Mobile remote-presence devices for point-of-care health care delivery. CMAJ 2013, 185, 1512–1516. [Google Scholar] [CrossRef] [Green Version]
- Aalam, A.A.; Hood, C.; Donelan, C.; Rutenberg, A.; Kane, E.M.; Sikka, N. Remote patient monitoring for ED discharges in the COVID-19 pandemic. Emerg. Med. J. 2021, 38, 229–231. [Google Scholar] [CrossRef]
- Larson, E.C.; Goel, M.; Boriello, G.; Heltshe, S.; Rosenfeld, M.; Patel, S.N. SpiroSmart: Using a microphone to measure lung function on a mobile phone. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing (UbiComp ‘12), Pittsburgh, PA, USA, 5–8 September 2012; ACM: New York, NY, USA, 2012; pp. 280–289. [Google Scholar]
- Alam, M.Z.; Simonetti, A.; Brillantino, R.; Tayler, N.; Grainge, C.; Siribaddana, P.; Nouraei, S.A.R.; Batchelor, J.; Rahman, M.S.; Mancuzo, E.V.; et al. Predicting Pulmonary Function From the Analysis of Voice: A Machine Learning Approach. Front. Digit. Health 2022, 4, 5. [Google Scholar] [CrossRef]
- San Chun, K.; Nathan, V.; Vatanparvar, K.; Nemati, E.; Rahman, M.M.; Blackstock, E.; Kuang, J. Towards passive assessment of pulmonary function from natural speech recorded using a mobile phone. In Proceedings of the 2020 IEEE International Conference on Pervasive Computing and Communications (PerCom), Austin, TX, USA, 23–27 March 2020; pp. 1–10. [Google Scholar]
- Rossmax, SA310 Oxygen Monitor. Available online: https://medaval.ie/device/rossmax-sa310/ (accessed on 14 December 2021).
- Knudson, R.J.; Lebowitz, M.D.; Holberg, C.J.; Burrows, B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am. Rev. Respir. Dis. 1983, 127, 725–734. [Google Scholar] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.C.; Chen, Y.R.; Wu, H.Y.; Huang, Y.J. Wearable sensor for measurement of gait walking and running motion. Sens. Mater. 2019, 31, 629–644. [Google Scholar] [CrossRef]
- Husted, H.M.; Llewellyn, T.L. The Accuracy of Pedometers in Measuring Walking Steps on a Treadmill in College Students. Int. J. Exerc. Sci. 2017, 10, 146–153. [Google Scholar]
- Rick, O.; Metz, T.; Eberlein, M.; Schirren, J.; Bölükbas, S. The Six-Minute-Walk Test in assessing respiratory function after tumor surgery of the lung: A cohort study. J. Thorac. Dis. 2014, 6, 421–428. [Google Scholar] [PubMed]
- Agrawal, M.B.; Awad, N.T. Correlation between Six Minute Walk Test and Spirometry in Chronic Pulmonary Disease. J. Clin. Diagn. Res. 2015, 9, OC01–OC04. [Google Scholar] [CrossRef]
- Zeng, G.S.; Chen, L.C.; Fan, H.Z.; Wu, L.L.; Wu, X.P.; Fang, Z.K.; He, X.; Yu, H.P. The relationship between steps of 6MWT and COPD severity: A cross-sectional study. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Wasilewska, E.; Sobierajska-Rek, A.; Małgorzewicz, S.; Soliński, M.; Jassem, E. Benefits of Telemonitoring of Pulmonary Function-3-Month Follow-Up of Home Electronic Spirometry in Patients with Duchenne Muscular Dystrophy. J. Clin. Med. 2022, 11, 856. [Google Scholar] [CrossRef]
- Russell, A.M.; Adamali, H.; Molyneaux, P.L.; Lukey, P.T.; Marshall, R.P.; Renzoni, E.A.; Wells, A.U.; Maher, T.M. Daily Home Spirometry: An Effective Tool for Detecting Progression in Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2016, 194, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.Y.; He, Y.D.; Chen, K.Q.; Zhao, Y.; Zhao, Y.X.; Xu, K.F. Home-based spirometry in the self-management of chronic obstructive pulmonary disease. Chin. Med. J. 2021, 134, 1789–1791. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, P.; Mycroft, K.; Korczyński, P.; Kołtowski, Ł.; Soliński, M.; Krenke, R.; Górska, K. Primary care spirometry with a new mobile phone-linked spirometer—A feasibility study. Eur. Respir. J. 2020, 56, 2691. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 60) | Training (n = 30) | Validation (n = 30) | p-Value | |
|---|---|---|---|---|
| Age (years old) | 63.4 ± 12.5 | 62.6 ± 11.7 | 64.3 ± 13.3 | 0.601 |
| Body height (cm) | 161.7 ± 7.8 | 161.6 ± 8.1 | 161.8 ± 7.7 | 0.909 |
| Body weight (Kg) | 60.1 ± 8.6 | 58.9 ± 10.2 | 61.4 ± 6.7 | 0.275 |
| BMI (Kg/m2) | 23.0 ± 3.1 | 22.5 ± 2.9 | 23.6 ± 3.2 | 0.170 |
| FVCpre (L) | 2.4 ± 0.63 | 2.3 ± 0.6 | 2.4 ± 0.7 | 0.473 |
| FEV1pre (L) | 1.6 ± 0.6 | 1.6 ± 0.6 | 1.6 ± 0.6 | 0.723 |
| FVCpost (L) | 2.34 ± 0.64 | 2.3 ± 0.6 | 2.4 ± 0.7 | 0.536 |
| FEV1post (L) | 1.62 ± 0.6 | 1.6 ± 0.6 | 1.7 ± 0.6 | 0.678 |
| FEV1pre/FVCpre (%) | 69.6 ± 20.8 | 70.5 ± 22.3 | 68.6 ± 19.6 | 0.727 |
| FEV1post/FVCpost(%) | 70.7 ± 20.9 | 71.3 ± 22.3 | 70.2 ± 19.8 | 0.839 |
| FEV1pre/FEV1pred (%) | 67.3 ± 22.0 | 64.8 ± 20.1 | 70.0 ± 23.8 | 0.400 |
| FEV1post/FEV1pred (%) | 68.0 ± 22.3 | 65.4 ± 20.7 | 70.6 ± 23.9 | 0.369 |
| FVCpre/FVCpred (%) | 80.0 ± 20.2 | 76.7 ± 16.7 | 82.4 ± 23.1 | 0.278 |
| FVCpost/FVCpred (%) | 79.3 ± 21.4 | 76.7 ± 18.5 | 82.0 ± 23.9 | 0.342 |
| Peak of heart beat | 136.3 ± 25.7 | 140.1 ± 32.1 | 132.6 ± 16.8 | 0.261 |
| SpO2pre (%) | 95.3 ± 2.3 | 95.5 ± 2.3 | 95.1 ± 2.3 | 0.503 |
| SpO2nidar (%) | 84.7 ± 5.9 | 85.5 ± 5.7 | 83.9 ± 6.0 | 0.285 |
| Total distance (m) | 418.1 ± 99.9 | 420.1 ± 107.3 | 416.1 ± 93.7 | 0.879 |
| Total steps | 638.9 ± 116.5 | 634.4 ± 127.2 | 643.3 ± 106.6 | 0.772 |
| Per step distance (m) | 0.7 ± 0.10 | 0.7 ± 0.1 | 0.6 ± 0.1 | 0.589 |
| Borg scale | 4.4 ± 1.3 | 4.4 ± 1.4 | 4.3 ± 1.2 | 0.845 |
| COPD | 33 (55.0) | 17 (56.7) | 16 (53.3) | 0.500 |
| ILD | 33 (55.0) | 17 (56.7) | 16 (53.3) | 0.500 |
| Asthma | 8 (13.3) | 3 (10.0) | 5 (16.7) | 0.353 |
| Bronchiectasis | 6 (10.0) | 2 (6.7) | 4 (13.3) | 0.335 |
| Estimation | Significant Factor | Correlation Coefficient | Stepwise Regression Model | Statistical Power (%) |
| PSD (m) | FVCpred | 0.592 | Formula (1) (R2adj = 0.339) | 92.2 |
| FEV1pred | 0.602 | |||
| Body height | 0.488 | |||
| FVCpre (L) | FVCpred | 0.586 | Formula (2) (R2adj = 0.476) | 99.6 |
| FEV1pred | 0.551 | |||
| PSD | 0.584 | |||
| Body height | 0.646 | |||
| Body weight | 0.474 | |||
| FEV1pre (L) | FVCpred | 0.597 | Formula (3) (R2adj = 0.356) | 94.1 |
| FEV1pred | 0.615 | |||
| PSD | 0.418 | |||
| TD | 0.457 | |||
| Body height | 0.408 | |||
| FVCpost (L) | FVCpred | 0.539 | Formula (4) (R2adj = 0.470) | 99.5 |
| FEV1pred | 0.500 | |||
| PSD | 0.619 | |||
| Body height | 0.608 | |||
| Body weight | 0.465 | |||
| FEV1post (L) | FVCpred | 0.575 | Formula (5) (R2adj = 0.317) | 89.4 |
| FEV1pred | 0.584 | |||
| PSD | 0.410 | |||
| TD | 0.413 | |||
| Body height | 0.408 |
| Pre-Exercise (Obstruction, n = 11) | Post-Exercise (Obstruction, n = 11) | |
|---|---|---|
| True positive (n) | 9 | 10 |
| False positive (n) | 7 | 7 |
| False negative (n) | 2 | 1 |
| True negative (n) | 12 | 12 |
| Sensitivity (%) | 81.8 | 90.9 |
| Specificity (%) | 63.2 | 63.2 |
| Accuracy (%) | 70.0 | 73.3 |
| Systems | Features | Limitations | Performance |
|---|---|---|---|
| Larson [20] |
|
|
|
| Alam [21] |
|
|
|
| Chun [22] |
|
|
|
| Proposed system |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-F.; Teng, C.-M.; Kuo, T.-H.; Huang, W.-C.; Wen, C.-Y. A Pervasive Pulmonary Function Estimation System with Six-Minute Walking Test. Biosensors 2022, 12, 824. https://doi.org/10.3390/bios12100824
Wu M-F, Teng C-M, Kuo T-H, Huang W-C, Wen C-Y. A Pervasive Pulmonary Function Estimation System with Six-Minute Walking Test. Biosensors. 2022; 12(10):824. https://doi.org/10.3390/bios12100824
Chicago/Turabian StyleWu, Ming-Feng, Chi-Min Teng, Tz-Hau Kuo, Wei-Chang Huang, and Chih-Yu Wen. 2022. "A Pervasive Pulmonary Function Estimation System with Six-Minute Walking Test" Biosensors 12, no. 10: 824. https://doi.org/10.3390/bios12100824