Magnetic Bead-Based Electrochemical Immunoassays On-Drop and On-Chip for Procalcitonin Determination: Disposable Tools for Clinical Sepsis Diagnosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagent and Solutions
2.2. Apparatus and Electrodes
2.3. Samples
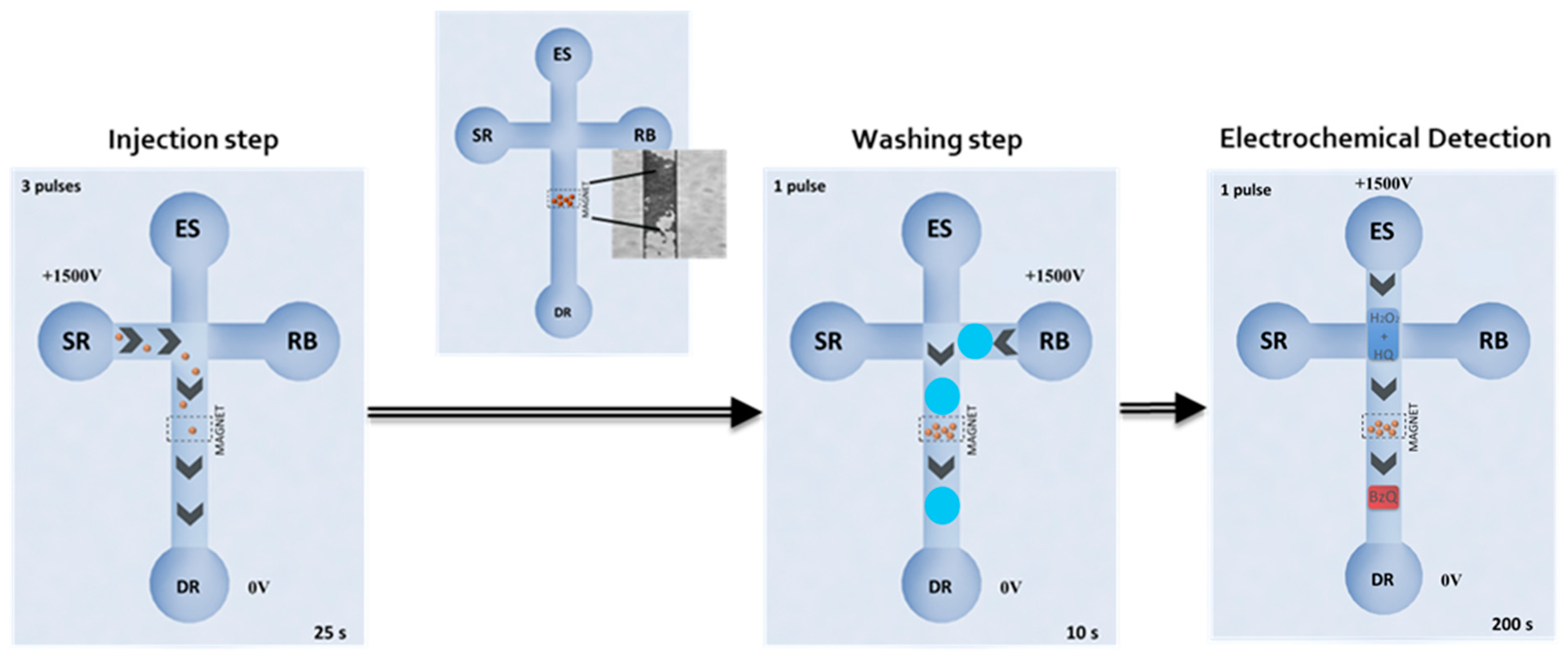
2.4. Immunoassay Procedures
2.5. Electrochemical Detection On-Drop onto SPE-C
2.6. Electrochemical Detection into EMC-Au
3. Results and Discussion
3.1. Optimization of the Immunoassay
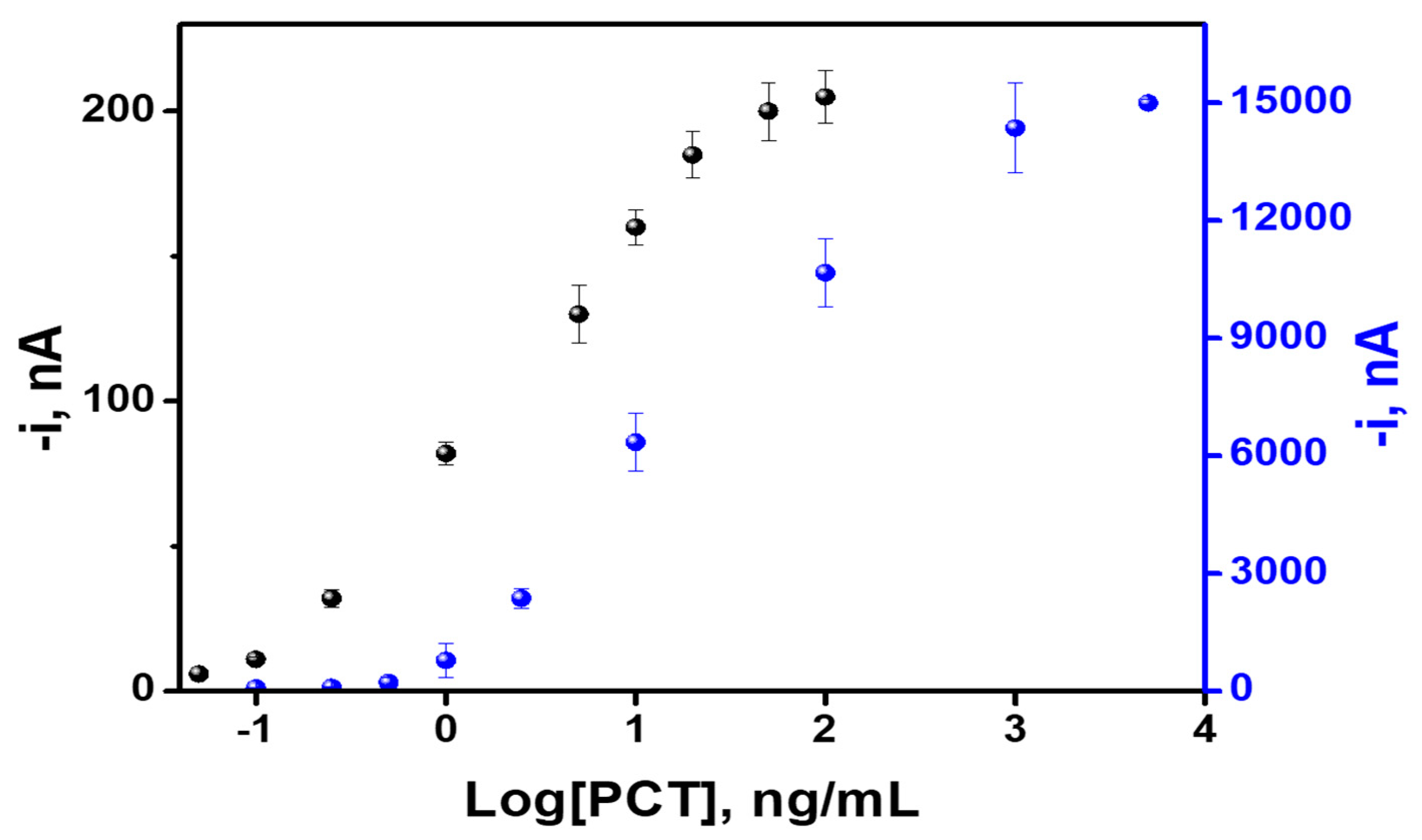
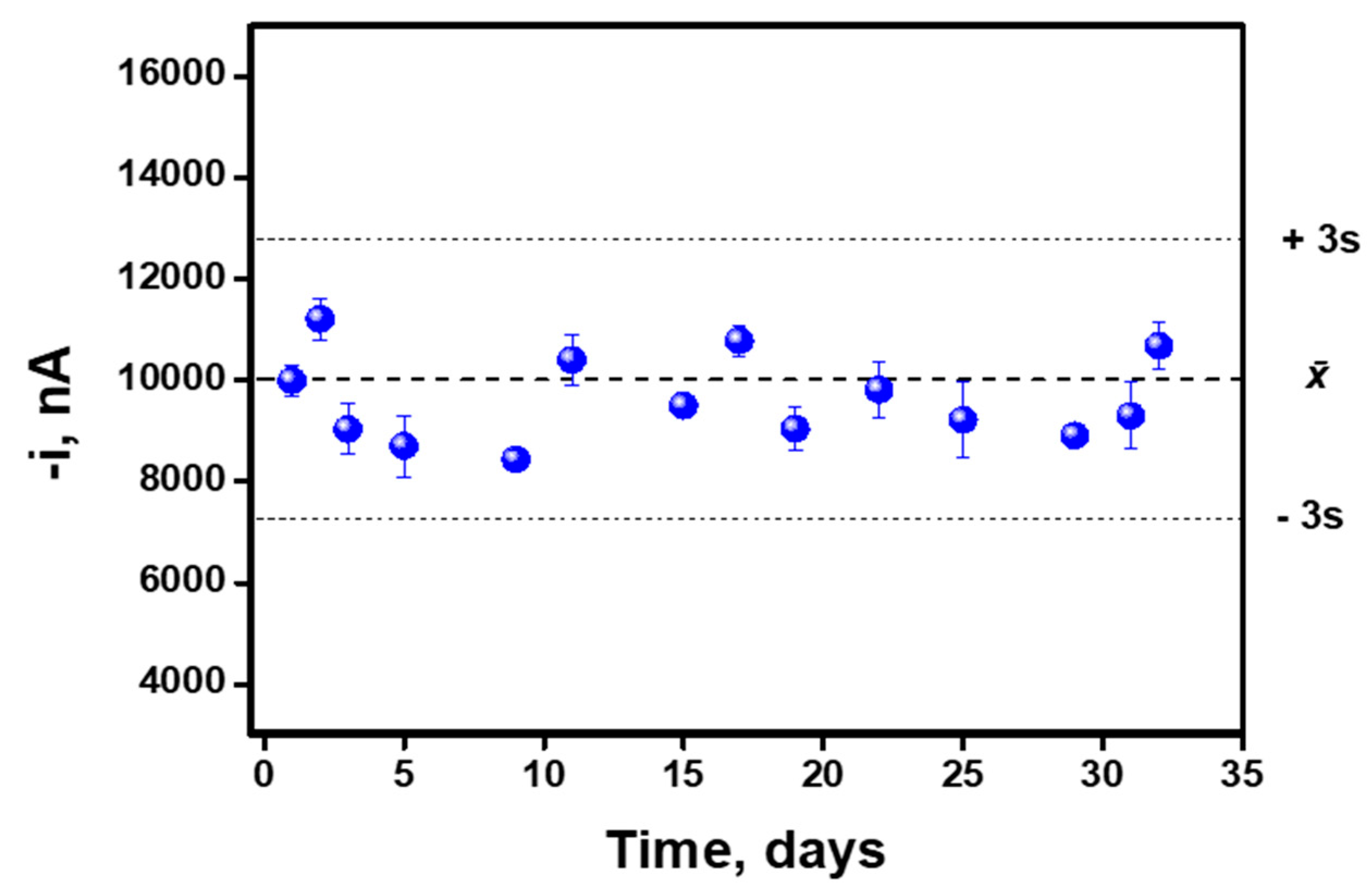
3.2. Analytical Characteristics
3.3. Analysis of Human Serum and Plasma Samples
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Paoli, C.J.; Reynolds, M.A.; Sinha, M.; Gitlin, M.; Crouser, E. Epidemiology and costs of sepsis in the United States—An analysis based on timing of diagnosis and severity level. Crit. Care Med. 2018, 46, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third International consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentrations in patients with sepsis and infections. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Bouadma, L.; Luyt, C.E.; Tubach, F.; Cracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Meisner, M.; Tschaikowsky, K.; Schnabel, S.; Schmidt, J.; Katalinic, A.; Schuttler, J. Procalcitonine influence of temperature, storage, anticoagulation and arterial or venous asservation of blood samples on procalcitonin concentrations. Eur. Clin. Chem. Lab. Med. 1997, 35, 597–601. [Google Scholar] [CrossRef] [Green Version]
- Sager, R.; Kutz, A.; Mueller, B.; Schuetz, P. Procalcitoninguided diagnosis andantibiotic stewardship revisited. BMC Med. 2017, 15, 15. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, P.; Birkhahn, R.; Sherwin, R.; Jones, A.E.; Singer, A.; Kline, J.A.; Runyon, M.S.; Self, W.H.; Courtney, D.M.; Nowak, R.M.; et al. Serial procalcitonin predicts mortality in severe sepsis patients: Results from the multicenter procalcitonin monitoring—SEpsis (MOSES) study. Crit. Care Med. 2017, 45, 781–789. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. PCT approved blood infection marker for guiding antibiotic therapy. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Dipalo, M.; Guido, L.; Micca, G.; Pittalis, S.; Locatelli, M.; Motta, A.; Bianchi, V.; Callegari, T.; Aloe, R.; Rin, G.; et al. Multicenter comparison of automated procalcitonin immunoassays. Pract. Lab. Med. 2015, 2, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Xue, J.; Yang, L.; Jia, Y.; Wang, H.; Zhang, N.; Ren, X.; Ma, H.; Wei, Q.; Ju, H. Electrochemiluminescence double quenching system based on novel emitter GdPO4: Eu with low-excited positive potential for ultrasensitive procalcitonin detection. ACS Sens. 2019, 4, 2825–2831. [Google Scholar] [CrossRef]
- Chen, P.; Xia, F.; Tian, D.; Zhou, C. A dual-coreactants electrochemiluminescent immunosensor for procalcitonin detection based on CdS-MoS2 nanocomposites. J. Electrochem. Soc. 2018, 165, B196–B201. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Yang, L.; Xue, J.; Zhang, N.; Fan, D.; Ma, H.; Ren, X.; Hu, L.; Wei, Q. Bioactivity-protected electrochemiluminescence biosensor using gold nanoclusters as the low-potential luminophor and Cu2S snowflake as co-reaction accelerator for procalcitonin analysis. ACS Sens. 2019, 4, 1909–1916. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Qiao, X.; Liu, J.; Xia, F.; Tian, D.; Zhou, C. A dual-signals response electrochemiluminescence immunosensor based on PTC-DEPA/KCC-1 NCs for detection of procalcitonin. Sens. Actuators B Chem. 2018, 267, 525–532. [Google Scholar] [CrossRef]
- Xu, X.; Song, X.; Nie, R.; Yang, Y.; Chen, Y.; Yang, L. Ultra-sensitive capillary immunosensor combining porous-layer surface modification and biotin-streptavidin nano-complex signal amplification: Application for sensing of procalcitonin in serum. Talanta 2019, 205. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Sun, Y.; Elseviers, J.; Muyldermans, S.; Liu, S.; Wan, Y. A nanobody-based electrochemiluminescent immunosensor for sensitive detection of human procalcitonin. Analyst 2014, 139, 3718–3721. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Li, Q.; Rao, W.; Liu, X.; Yin, L.; Zhang, H. Determining the concentration of procalcitonin using a magnetic particles-based chemiluminescence assay for the clinical diagnosis of sepsis. Anal. Sci. 2013, 29, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Xianyu, Y.; Wu, J.; Dong, M.; Zheng, W.; Sun, J.; Jiang, X. Double-Enzymes-Mediated Bioluminescent Sensor for Quantitative and Ultrasensitive Point-of-Care Testing. Anal. Chem. 2017, 89, 5422–5427. [Google Scholar] [CrossRef]
- Taranova, N.A.; Urusov, A.E.; Sadykhov, E.G.; Zherdev, A.V.; Dzantiev, B.B. Bifunctional gold nanoparticles as an agglomeration-enhancing tool for highly sensitive lateral flow tests: A case study with procalcitonin. Microchim. Acta 2017, 184, 4189–4195. [Google Scholar] [CrossRef]
- Wang, H.; Wang, H.; Chen, S.; Dzakah, E.E.; Kang, K.; Wang, J.; Wang, J. Development of a fluorescent immnunochromatographic assay for the procalcitonin detection of clinical patients in China. Clin. Chim. Acta 2015, 444, 37–42. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhou, C.; Wu, R.; Li, L.; Shen, H.; Li, L.S. Preparation of multi-shell structured fluorescent composite nanoparticles for ultrasensitive human procalcitonin detection. RSC Adv. 2015, 5, 5988–5995. [Google Scholar] [CrossRef]
- Tang, J.; Lei, L.; Feng, H.; Zhang, H.; Han, Y. Preparation of K+-Doped core-shell NaYF4: Yb, Er upconversion nanoparticles and its application for fluorescence immunochromatographic assay of human procalcitonin. J. Fluoresc. 2016, 26, 2237. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.Y.; Wang, C.R.; Xie, C.M.; Wang, X.G.; Liang, R.L.; Xu, W.W. Rapid and sensitive lateral flow immunoassay method for procalcitonin (PCT) based on time-resolved immunochromatography. Sensors 2017, 17, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, R.; Xu, X.; Cui, X.; Chen, Y.; Yang, L. A highly sensitive capillary-based immunosensor by combining with peroxidase nanocomplex-mediated signal amplification for detection of procalcitonin in human serum. ACS Omega 2019, 4, 6210–6217. [Google Scholar] [CrossRef] [Green Version]
- Vashist, S.K.; Schneider, E.M.; Barth, E.; Luong, J.H.T. Surface plasmon resonance-based immunoassay for procalcitonin. Anal. Chim. Acta 2016, 938, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Jing, W.; Wang, Y.; Yang, Y.; Wang, Y.; Ma, G.; Wang, S.; Tao, N. Time-resolved digital immunoassay for rapid and sensitive quantitation of procalcitonin with plasmonic imaging. ACS Nano 2019, 13, 8609–8617. [Google Scholar] [CrossRef] [PubMed]
- Baldini, F.; Bolzoni, L.; Giannetti, A.; Kess, M.; Krämer, P.M.; Kremmer, E.; Senesi, F.; Trono, C. A new procalcitonin optical immunosensor for POCT applications. Anal. Bioanal. Chem. 2009, 393, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Buchegger, P.; Preininger, C. Four assay designs and on-chip calibration: Gadgets for a sepsis protein array. Anal. Chem. 2014, 86, 3174–3180. [Google Scholar] [CrossRef]
- Kemmler, M.; Sauer, U.; Schleicher, E.; Preininger, C.; Brandenburg, A. Biochip point-of-care device for sepsis diagnostics. Sens. Actuators B Chem. 2014, 192, 205–215. [Google Scholar] [CrossRef]
- Kramer, P.M.; Kess, M.; Kremmer, E.; Schulte-Hostede, S. Multi-parameter determination of TNFα, PCT and CRP for point-of-care testing. Analyst 2011, 136, 692–695. [Google Scholar] [CrossRef]
- Rascher, D.; Geerlo, A.; Kremmer, E.; Krämer, P.; Schmid, M.; Hartmann, A.; Rieger, M. Total internal reflection (TIRF)-based quantification of procalcitonin for sepsis diagnosis—A point-of-care testing application. Biosens. Bioelectron. 2014, 59, 251–258. [Google Scholar] [CrossRef]
- Sauer, U.; Domnanich, P.; Preininger, C. Protein chip for the parallel quantification of high and low abundant biomarkers for sepsis. Anal. Biochem. 2011, 419, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Molinero-Fernández, Á.; Moreno-Guzmán, M.; Arruza, L.; López, M.Á.; Escarpa, A. Polymer-based micromotors fluorescence immunoassay for on the move sensitive procalcitonin determination in very low birth weight infants’ plasma. ACS Sens. 2015. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, W.; Jin, G.; Niu, Y.; Chen, Y.; Xie, M. Label-free sandwich imaging ellipsometry immunosensor for serological detection of procalcitonin. Anal. Chem. 2018, 90, 8002–8010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremmer, E.; Meyer, K.; Grässer, F.A.; Flatley, A.; Kösters, M.; Luppa, P.B.; Krämer, P.M. A new strategy for the development of monoclonal antibodies for the determination of human procalcitonin in serum samples. Anal. Bioanal. Chem. 2012, 402, 989–995. [Google Scholar] [CrossRef]
- Zhang, Y.; Si, X.; Zhang, M.; Yang, X.; Yuan, H.; Wang, X.; Zhang, Y.; Wang, H. Rapid colorimetric determination of procalcitonin using magnetic separation and enzymatic catalysis. Anal. Lett. 2019, 52, 602–612. [Google Scholar] [CrossRef]
- Liao, T.; Yuan, F.; Yu, H.; Li, Z. An ultrasensitive ELISA method for the detection of procalcitonin based on magnetic beads and enzyme-antibody labeled gold nanoparticles. Anal. Methods 2016, 8, 1577–1585. [Google Scholar] [CrossRef]
- Sener, G.; Ozgur, E.; Rad, A.Y.; Uzun, L.; Say, R.; Denizli, A. Rapid real-time detection of procalcitonin using a microcontact imprinted surface plasmon resonance biosensor. Analyst 2013, 138, 6422–6428. [Google Scholar] [CrossRef]
- Yang, Z.-H.; Ren, S.; Zhou, Y.; Yuan, R.; Chai, Y.-Q. Cu/Mn double-doped CeO2 nanocomposites as signal tags and signal amplifiers for sensitive electrochemical detection of procalcitonin. Anal. Chem. 2017, 89, 13349–13356. [Google Scholar] [CrossRef]
- Chiang, C.Y.; Huang, T.T.; Wang, C.H.; Huang, C.J.; Tsai, T.H.; Yu, S.N.; Chen, Y.T.; Hong, S.W.; Hsu, C.W.; Chang, T.C.; et al. Fiber optic nanogold-linked immunosorbent assay for rapid detection of procalcitonin at femtomolar concentration level. Biosens. Bioelectron. 2019, 151, 111871. [Google Scholar] [CrossRef] [PubMed]
- Molinero-Fernández, Á.; Moreno-Guzmán, M.; Arruza, L.; López, M.Á.; Escarpa, A. Toward early diagnosis of late-onset sepsis in preterm neonates: Dual magnetoimmunosensor for simultaneous procalcitonin and co-reactive protein determination in diagnosed clinical samples. ACS Sens. 2019, 4, 2117–2123. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.M.; Ryu, M.Y.; Kim, J.H.; Cho, C.H.; Park, T.J.; Park, J.P. An electrochemical biosensor for detection of the sepsis-related biomarker procalcitonin. RSC Adv. 2017, 7, 36562–36565. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Hu, Q.; Yu, X.; Wang, L. Ultrasensitive electrochemical immunosensor for procalcitonin with signal enhancement based on zinc nanoparticles functionalized ordered mesoporous carbon-silica nanocomposites. Sens. Actuators B Chem. 2018, 258, 238–245. [Google Scholar] [CrossRef]
- Seshadri, P.; Manoli, K.; Schneiderhan-Marra, N.; Anthes, U.; Wierzchowiec, P.; Bonrad, K.; Di Franco, C.; Torsi, L. Low-picomolar, label-free procalcitonin analytical detection with an electrolyte-gated organic field-effect transistor based electronic immunosensor. Biosens. Bioelectron. 2018, 104, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Wang, X. Amperometric immunosensor of procalcitonin based on amplification strategy of ferrocene-modified gold nanoparticles. Int. J. Electrochem. Sci. 2015, 10, 9342–9350. [Google Scholar]
- Sui, Y.; Xu, A.; Jin, X.; Zheng, J.; He, X.; Cheng, Y.; Xie, Q.; Liu, R. In situ enzymatic generation of gold for ultrasensitive amperometric sandwich immunoassay of procalcitonin. Biosens. Bioelectron. 2018, 117, 422–428. [Google Scholar] [CrossRef]
- Zhang, T.; Ren, X.; Fan, D.; Kuang, X.; Wang, H.; Wu, D.; Wei, Q. Electrochemical procalcitonin immunoassay based on Au@Ag heterojunction nanorods as labels and CeO2-CuO nanorods as enhancer. Sens. Actuators B Chem. 2019, 297, 126800. [Google Scholar] [CrossRef]
- Gao, Z.; Li, Y.; Zhang, C.; Zhang, S.; Jia, Y.; Dong, Y. An enzyme-free immunosensor for sensitive determination of procalcitonin using NiFe PBA nanocubes@TB as the sensing matrix. Anal. Chim. Acta 2019. [Google Scholar] [CrossRef]
- Ghrera, A.S. Quantum dot modified interface for electrochemical immunosensing of procalcitonin for the detection of urinary tract infection. Anal. Chim. Acta 2019, 1056, 26–33. [Google Scholar] [CrossRef]
- Qian, Y.; Feng, J.; Wang, H.; Fan, D.; Jiang, N.; Wei, Q.; Ju, H. Sandwich-type signal-off photoelectrochemical immunosensor based on dual suppression effect of PbS quantum dots/CO3O4 polyhedron as signal amplification for procalcitonin detection. Sens. Actuators B Chem. 2019, 300, 127001. [Google Scholar] [CrossRef]
- Mahe, L.S.A.; Green, S.J.; Winlove, C.P.; Jenkins, A.T.A. Pyrene-wired antibodies on highly oriented pyrolytic graphite as a label-free impedance biosensor for the sepsis biomarker procalcitonin. J. Solid State Electrochem. 2014, 18, 3245–3249. [Google Scholar] [CrossRef]
- Shen, W.J.; Zhuo, Y.; Chai, Y.Q.; Yang, Z.H.; Han, J.; Yuan, R. Enzyme-free electrochemical immunosensor based on host–guest Nanonets catalyzing amplification for Procalcitonin detection. ACS Appl. Mater. Interfaces 2015, 7, 4127–4134. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.H.; Zhuo, Y.; Yuan, R.; Chai, Y.Q. Electrochemical activity and electrocatalytic property of cobalt phthalocyanine nanoparticles-based immunosensor for sensitive detection of procalcitonin. Sens. Actuators B Chem. 2016, 227, 212–219. [Google Scholar] [CrossRef]
- Liu, F.; Xiang, G.; Yuan, R.; Chen, X.; Luo, F.; Jiang, D.; Huang, S.; Li, Y.; Pu, X. Procalcitonin sensitive detection based on graphene–gold nanocomposite film sensor platform and single-walled carbon nanohorns/hollow Pt chains complex as signal tags. Biosens. Bioelectron. 2014, 60, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Xiang, G.; Chen, X.; Luo, F.; Jiang, D.; Huang, S.; Yi, L.; Pu, X. A novel strategy of procalcitonin detection based on multi-nanomaterials of single-walled carbon nanohorns–hollow Pt nanospheres/PAMAM as signal tags. RSC Adv. 2014, 4, 13934–13940. [Google Scholar] [CrossRef]
- Fang, Y.S.; Wang, H.Y.; Wang, L.S.; Wang, J.F. Electrochemical immunoassay for procalcitonin antigen detection based on signal amplification strategy of multiple nanocomposites. Biosens. Bioelectron. 2014, 51, 310–316. [Google Scholar] [CrossRef]
- Li, P.; Zhang, W.; Zhou, X.; Zhang, L. C60 carboxyfullerene-based functionalised nanohybrids as signal-amplifying tags for the ultrasensitive electrochemical detection of procalcitonin. Clin. Biochem. 2015, 48, 156–161. [Google Scholar] [CrossRef]
- Tan, E.K.W.; Shrestha, P.K.; Pansare, A.V.; Chakrabarti, S.; Li, S.; Chu, D.; Lowe, C.R.; Nagarkar, A.A. Density modulation of embedded nanoparticles via spatial, temporal and chemical control elements. Adv. Mater. 2019, 31, 1901802. [Google Scholar] [CrossRef]
- Yáñez-Sedeño, P.; Campuzano, S.; Pingarrón, J.M. Magnetic particles coupled to disposable screen printed transducers for electrochemical biosensing. Sensors 2016, 16, 1585. [Google Scholar] [CrossRef] [Green Version]
- Fernández-la-Villa, A.; Pozo-Ayuso, D.F.; Castaño-Álvarez, M. Microfluidics and electrochemistry: An emerging tandem for next-generation analytical microsystems. Curr. Opin. Electrochem. 2019, 15, 175–185. [Google Scholar] [CrossRef]
- Rackus, D.G.; Shamsi, M.H.; Wheeler, A.R. Electrochemistry, biosensors and microfluidics: A convergence of fields. Chem. Soc. Rev. 2015, 4, 5320–5340. [Google Scholar] [CrossRef]
- Mou, L.; Jiang, X. Materials for microfluidic immunoassays: A review. Adv. Healthc. Mater. 2017, 6, 1601403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Dong, M.; Rigatto, C.; Liu, Y.; Lin, F. Lab-on-chip technology for chronic disease diagnosis. NPJ Digit. Med. 2018, 1, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sackmann, E.K.; Fulton, A.L.; Beebe, D.J. The present and future role of microfluidics in biomedical research. Nature 2014, 507, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.; Han, J.; Choi, J.-W.; Ahn, C.H. Point-of-care testing (POCT) diagnostic systems using microfluidic lab-on-a-chip technologies. Microelectron. Eng. 2015, 132, 46–57. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step | Parameter | Studied Range | Selected Value |
|---|---|---|---|
| Immunocomplex-MB Injection | Immunocomplex-MB dilution (v/v) | 1:10–1:200 | 1:10 |
| Applied Voltage (V) | +1000–2000 | +1500 | |
| Number of pulses | 1–5 | 3 | |
| Pulse time (s) | 10–50 | 25 | |
| Washing | Applied Voltage (V) | +1000–2000 | 1500 |
| Number of pulses | 1–5 | 1 | |
| Pulse time (s) | 10–50 | 25 | |
| Enzyme substrates pumping/driven | Applied Voltage (V) | +1000–2000 | +1500 |
| Time (s) | ---- | 200 s | |
| Detection | E (V) | −0.10–(−0.30) | −0.20 |
| Analytical Characteristic | SPE-C | EMC-Au |
|---|---|---|
| EC50, ng mL−1 | 20.2 | 2.2 |
| Working range, ng mL−1 | 0.5–1000 | 0.1–20 |
| r | 0.990 | 0.990 |
| LOD, ng mL−1 | 0.1 | 0.04 |
| Intra-assay, CV% | <7.5% | 5% |
| Inter-assay, CV% | 8% | 9% |
| PCTadded (ng/mL) | SPE-C | EMC-Au | ||||
|---|---|---|---|---|---|---|
| Serum | Plasma | Serum | ||||
| PCTfound (ng/mL) | Recovery (%) | PCTfound (ng/mL) | Recovery (%) | PCTfound (ng/mL) | Recovery (%) | |
| Before spiked | <0.1 | --- | <0.1 | --- | <0.04 | --- |
| 1.0 | 0.9 | 90 ± 3 | 1.2 | 120 ± 6 | 1.1 | 110 ± 5 |
| 10.0 | 8.9 | 89 ± 14 | 10.4 | 104 ± 7 | 9.6 | 96 ± 2 |
| 100.0 | 99 | 99 ± 7 | 101 | 101 ± 2 | --- * | --- |
| Technique | cAb Immobilization | Assay Format | dAb Label | WR | LOD | Analysis Time * | Sample Volume | Sample | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Chemiluminescence | MB–(anti-FITC–Ab)/FITC–cAb | Double Sandwich | dAb–ABEI | 0.09–600 ng mL−1 | 30 pg mL−1 | 25 min | 40 µL | Serum | 16 |
| Chemiluminescence | MB–COOH/cAb | Sandwich | dAb–(PS-ALP) | 1–104 pg mL−1 | 0.045 pg mL−1 | 1 h | 800 µL | Serum | 17 |
| UV-vis Spectroscopy | MB–COOH/cAb | Sandwich | dAb–HRP | 0.1–10 ng mL−1 | 40 pg mL−1 | 1.5 h | 100 µL | Serum | 35 |
| UV-vis Spectroscopy | MB–COOH/cAb | Sandwich | dAb–(AuNPs-HRP) | 0.02–20 ng mL−1 | 20 pg mL−1 | 1.5 h | 50 µL | Serum | 36 |
| Amperometry | MB–Streptavidin/Biotin–cAb | Sandwich | dAb–HRP | 0.25–100 ng mL−1 | 50 pg mL−1 | 20 min | 25 µL | Neonates plasma | 40 |
| Amperometry | MB–Streptavidin/Biotin–cAb | Sandwich | dAb–HRP | 0.5–1000 ng mL−1 | 100 pg mL−1 | 20 min | 25 µL | Serum Plasma | Our work (SPE-C) |
| Technique | cAb Immobilization | Assay Format | dAb Label | WR | LOD | Analysis Time * | Sample Volume | Sample | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Fluorescence | Covalent cAb | Sandwich | dAb–DY647 | 0.7–25 ng mL−1 | 0.2 ng mL−1 | 23 min | 100 µL | Serum | 26 |
| Reflection Fluorescence | Covalent cAb | Sandwich | dAb–DY647 | 5–500 ng mL−1 | 1 ng mL−1 | 11 min | 10–75 µL | Serum Plasma | 28 |
| Fluorescence | Adsorption cAb | Sandwich | dAb–DY647 | 640–3400 ng mL−1 | 50 ng mL−1 | 22 min | 280 µL | Serum Diluted 1:10 | 29 |
| Reflection Fluorescence | Adsorption cAb | Sandwich | dAb–cyanine | 0.06–7.18 ng mL−1 | 0.02 ng mL−1 | <9 min | 50 µL | Serum Plasma Whole blood | 30 |
| Nanoplasmonic | Covalent cAb | Sandwich | dAb–AuNPs | 1 pg mL−1–100 ng mL−1 | 95 fg mL−1 | <15 min | --- | Serum | 39 |
| Amperometry | MB–Streptavidin/Biotin–cAb | Sandwich | dAb–HRP | 0.1–20 ng mL−1 | 40 pg mL−1 | 20 min | 25 µL | Serum Plasma | Our work (EMC-Au) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molinero-Fernández, Á.; Moreno-Guzmán, M.; López, M.Á.; Escarpa, A. Magnetic Bead-Based Electrochemical Immunoassays On-Drop and On-Chip for Procalcitonin Determination: Disposable Tools for Clinical Sepsis Diagnosis. Biosensors 2020, 10, 66. https://doi.org/10.3390/bios10060066
Molinero-Fernández Á, Moreno-Guzmán M, López MÁ, Escarpa A. Magnetic Bead-Based Electrochemical Immunoassays On-Drop and On-Chip for Procalcitonin Determination: Disposable Tools for Clinical Sepsis Diagnosis. Biosensors. 2020; 10(6):66. https://doi.org/10.3390/bios10060066
Chicago/Turabian StyleMolinero-Fernández, Águeda, María Moreno-Guzmán, Miguel Ángel López, and Alberto Escarpa. 2020. "Magnetic Bead-Based Electrochemical Immunoassays On-Drop and On-Chip for Procalcitonin Determination: Disposable Tools for Clinical Sepsis Diagnosis" Biosensors 10, no. 6: 66. https://doi.org/10.3390/bios10060066