1. Introduction
Skin cancer is one of the most common types of malignancy in the US and globally. One important strategy in controlling skin cancer is avoiding excessive sun exposure and applying sunscreen products. However, up to now, there is inadequate evidence as to whether sunscreen use can reduce the risk of skin cancer. Additionally, sunscreen has its own side effects and limitations [
1]. Chemoprevention, which is defined as the use of natural products or pharmacological agents, to inhibit, block, or reverse cancer development, was proposed to reduce skin cancer [
2]. There is an increasing interest in chemoprevention for individuals with increased risk for skin cancer.
The cardiovascular drug carvedilol was reported with skin cancer preventive activity [
3,
4]. Carvedilol is a β-adrenergic receptor (β-AR) antagonist and an FDA-approved drug used for cardiovascular diseases. Carvedilol has two oral formulations: the immediate-release formulation, which is taken twice a day and the controlled-release formulation, which is taken once a day [
5]. Carvedilol is a chiral drug; it is marketed as a racemic mixture consisting of S- and R- enantiomers in a 1:1 ratio. Although S- and R-carvedilol have the same chemical formula, the two enantiomers exhibit distinct pharmacokinetic and pharmacodynamic profiles [
6,
7,
8,
9]. Noticeably, S-carvedilol is a potent, competitive antagonist for β-adrenergic receptors, while R-carvedilol is not; it is not considered a β-blocker [
10,
11]. Our previous studies demonstrate that skin cancer preventive activity of carvedilol is independent of β-AR antagonism [
12]. The racemic carvedilol, S-carvedilol, and R-carvedilol similarly prevent ultraviolet (UV) radiation-induced skin DNA damage, reactive oxidative species (ROS) formation, inflammation, and carcinogenesis [
13]. Using R-carvedilol can avoid unwanted cardiovascular effects for a chemopreventive agent because they lack β-AR antagonism. In a previous study using an oral dose of 1.6 mg/kg/day, R-carvedilol did not affect heart rate and blood pressure in mice [
6]. Thus, the optically pure R-carvedilol enantiomer may be a better candidate for development as a skin cancer chemopreventive agent.
One limitation in repurposing R-carvedilol for skin cancer prevention is related to its delivery. Carvedilol belongs to the biopharmaceutical classification system (BCS) class II drugs; a highly lipophilic compound with low solubility and poor oral bioavailability [
14]. A larger dose and higher dosing frequency are required to achieve the effective concentration. Topical drug delivery shows significant advantages for drugs targeting the skin because it avoids first-pass metabolism and reduces systemic effects [
15]. Topical administration is important for skin cancer prevention because the drug will have a greater likelihood of reaching the site of damage and provides a relatively easy method of self-treatment.
Carvedilol may be encapsulated in surfactant systems or nanocarriers for enhanced dermal targeting [
16]. Previously, it was demonstrated that racemic carvedilol can be encapsulated into transfersomal formulations for topical application [
17,
18]. Transfersome, also named flexible liposome or deformable liposome, is an altered version of conventional liposomes prepared with phospholipids with the addition of surfactants, i.e., edge activators. Transfersomes exhibit an ability to enhance drug penetration into the intercellular lipid matrix by blending with the
stratum corneum (SC) and modifying the lipid lamellae [
19,
20,
21]. Previous studies showed that transfersome-encapsulated drugs were able to penetrate into deeper layers of skin without systemic absorption [
19,
21,
22]. In contrast, classic liposomes have little value for topical drug delivery because they do not deeply penetrate the skin, but rather remain confined to the SC layer [
20].
Therefore, we hypothesized that transfersomes can deliver R-carvedilol into the skin and that R-carvedilol-loaded transfersomes can be developed into a topical formulation for skin cancer prevention. Although a skin targeting transfersome delivery system for the racemic carvedilol was reported [
17,
18], due to the different stereochemistry of R- and S-carvedilol, it is necessary to examine whether transfersomes can be optimized to effectively deliver the optically pure R-carvedilol. Thus, the goal of the present study is to prepare several R-carvedilol-loaded transfersomal formulations, examine their drug penetration through the skin, deposition into the skin, as well as efficacy and safety. The data presented in this report collectively support a hypothesis that transfersomes are a valid system for R-carvedilol skin delivery.
2. Materials and Methods
2.1. Chemicals and Reagents
R-carvedilol was synthesized by Chem-Impex International, Inc. (Wood Dale, IL, USA). The purity was determined by the manufacturer using Chiral HPLC as 98.97%. After the compound was received, the accuracy and purity were confirmed by chiral HPLC using Phenomenex Lux® 5 µm Cellulose-4 LC Column 250 × 4.6 mm (Phenomenex, Torrance, CA, USA). Tween-80, sodium cholate, and polyethylene glycol 400 (PEG 400) were purchased from VWR (Radnor, PA, USA). L-α-phosphatidylcholine (Soy PC or SPC), L-α-phosphatidylcholine hydrogenated (Hydro Egg PC, HEPC), and 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC) were purchased from Avanti Polar Lipids, Inc. (Alabaster, AL, USA). Carbopol® 934 was purchased from SERVA Electrophoresis GmbH (Heidelberg, Germany). Triethanolamine (TEA) was purchased from Sigma-Aldrich (St. Louis, MO, USA).
2.2. Preparation of R-carvedilol-Loaded Transfersomes and Carbopol Gel
Transfersomes were prepared by a thin film hydration method as described previously [
18]. In brief, the lipids, surfactants and R-carvedilol (5 mg) were dissolved in chloroform:methanol (2:1,
v/
v). To form a thin film, the organic solvent was gradually evaporated under reduced pressure in a rotary evaporator at 45 °C for 30 min. Next, the thin film was hydrated in 10 mL PBS (pH 7.4) at 51 °C. Then, the formulation was sonicated in a water bath for 5 or 30 min before passing through a 100 nm pore size membrane (Avanti Polar Lipids, Alabaster, AL, USA) through an extruder (Liposofast LF-50, Avestin, Ottawa, ON, Canada) to reduce the particle size and obtain stable transfersomes. The plain transfersome (PT), used as no drug control, was prepared in the same way, except that no drug was added. Carbopol gel was prepared because it was previously reported in mouse studies that it increases skin retention [
17]. The transfersomal formulations were mixed with 0.5% Carbopol
® 934 and triethanolamine (TEA) (1:1.5,
w/
w) and then vortexed until a clear gel was formed.
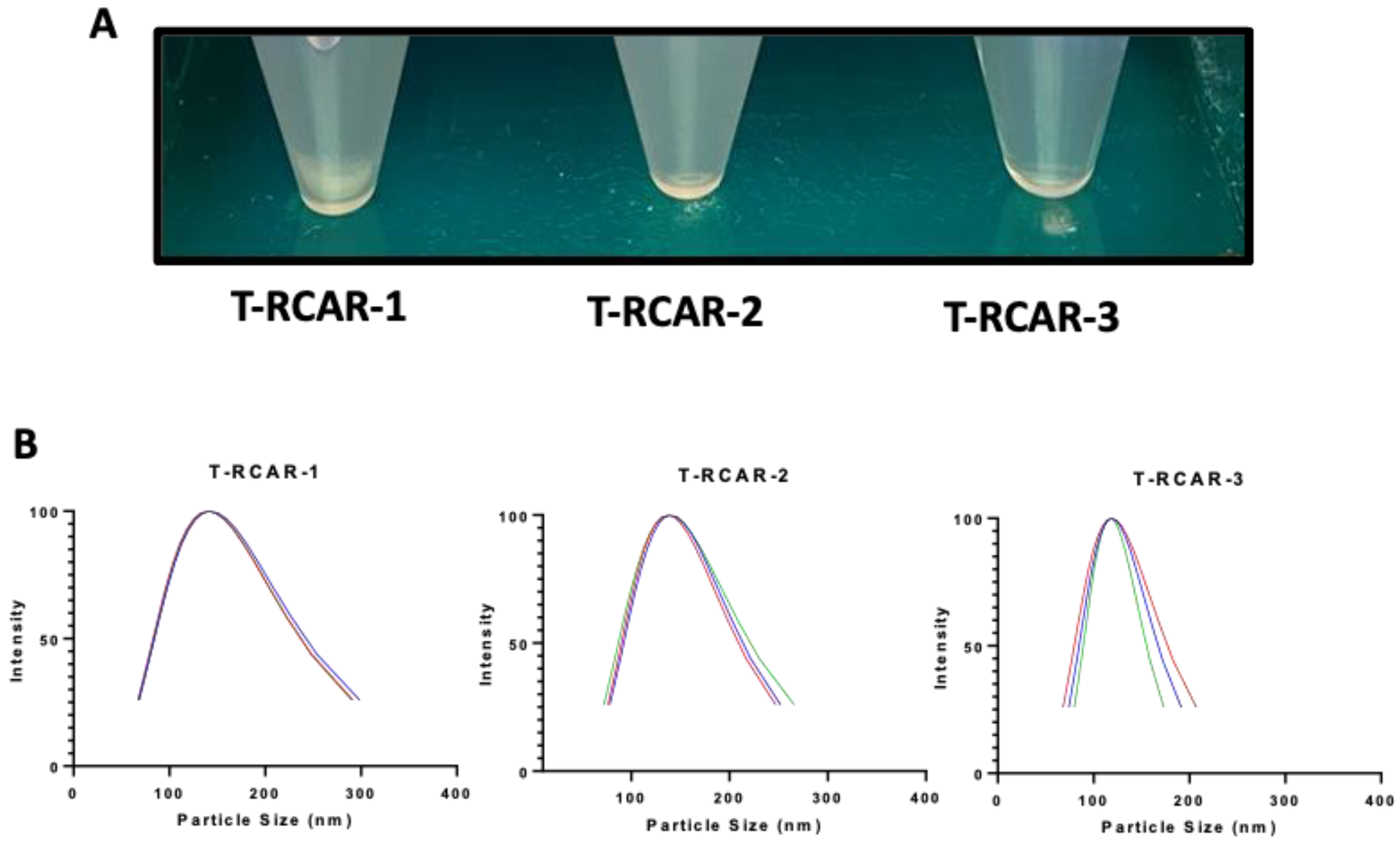
2.3. Determination of Particle Size, Zeta Potential and Encapsulation Efficiency
Particle sizes and polydispersity index (PDI) were determined using the Nanobrook Omni particle sizer (Brookhaven Instruments Corporation, Holtsville, NY, USA). Zeta potential was determined using Malvern zeta-sizer (Malvern Panalytical, Malvern, UK). The encapsulation efficiency (EE) was determined according to reported methods [
18]. In brief, the transfersomes were centrifuged inside the 30,000-dalton cutoff Nanosep
® tubes (Pall Life Sciences, Ann Arbor, MI, USA) at 14,000 rpm for 1 h at 4 °C. The drug level in the filtrate, which represents the free drug was analyzed via HPLC. To determine the total drug concentration, the transfersome suspension (10 μL) was mixed with 990 μL of methanol and vortexed for 1 h to disrupt the transfersomes. The encapsulation efficiency was calculated by the following formula.
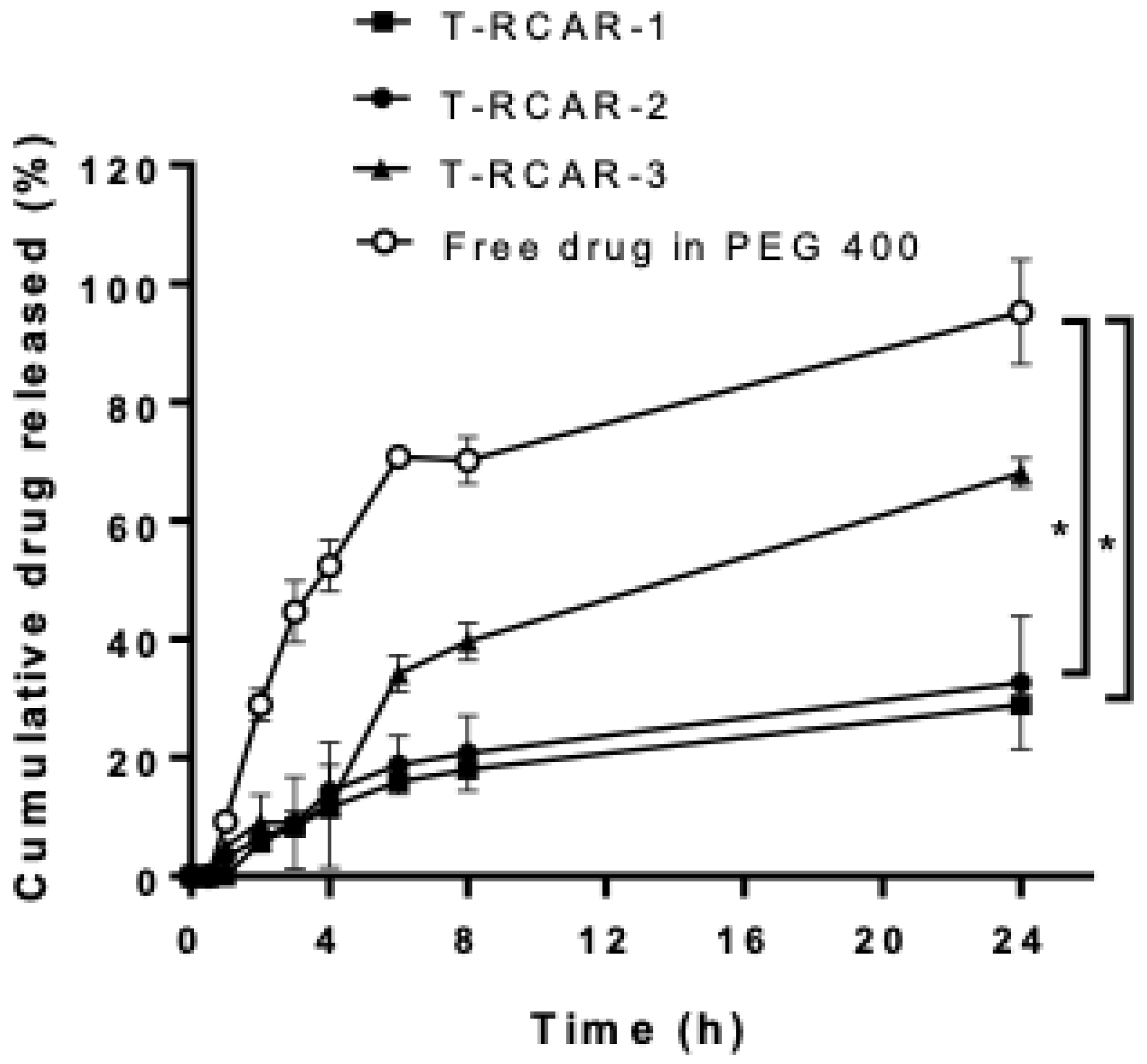
2.4. In Vitro Drug Release Analysis
The in vitro drug release was analyzed using a Pur-A-Lyzer Mini Dialysis Kit with 3.5 kDa as the molecular weight cut off (MWCO) (Sigma-Aldrich, St. Louis, MO, USA). The release was conducted in a shaking incubator at 100 rpm and 37 °C. The transfersomes containing 0.1 mg R-carvedilol or the same amount of free drug dissolved in PEG 400 (volume 2.5 mL) were added into the dialysis tubes. PBS was used as the release medium and the tubes were immersed in 100 mL of PBS (pH 7.4). At various time intervals (0.5, 1, 2, 3, 4, 6, 8, and 24 h), 1 mL samples were withdrawn from the release medium and replaced with 1 mL of fresh PBS. The samples were analyzed via HPLC.
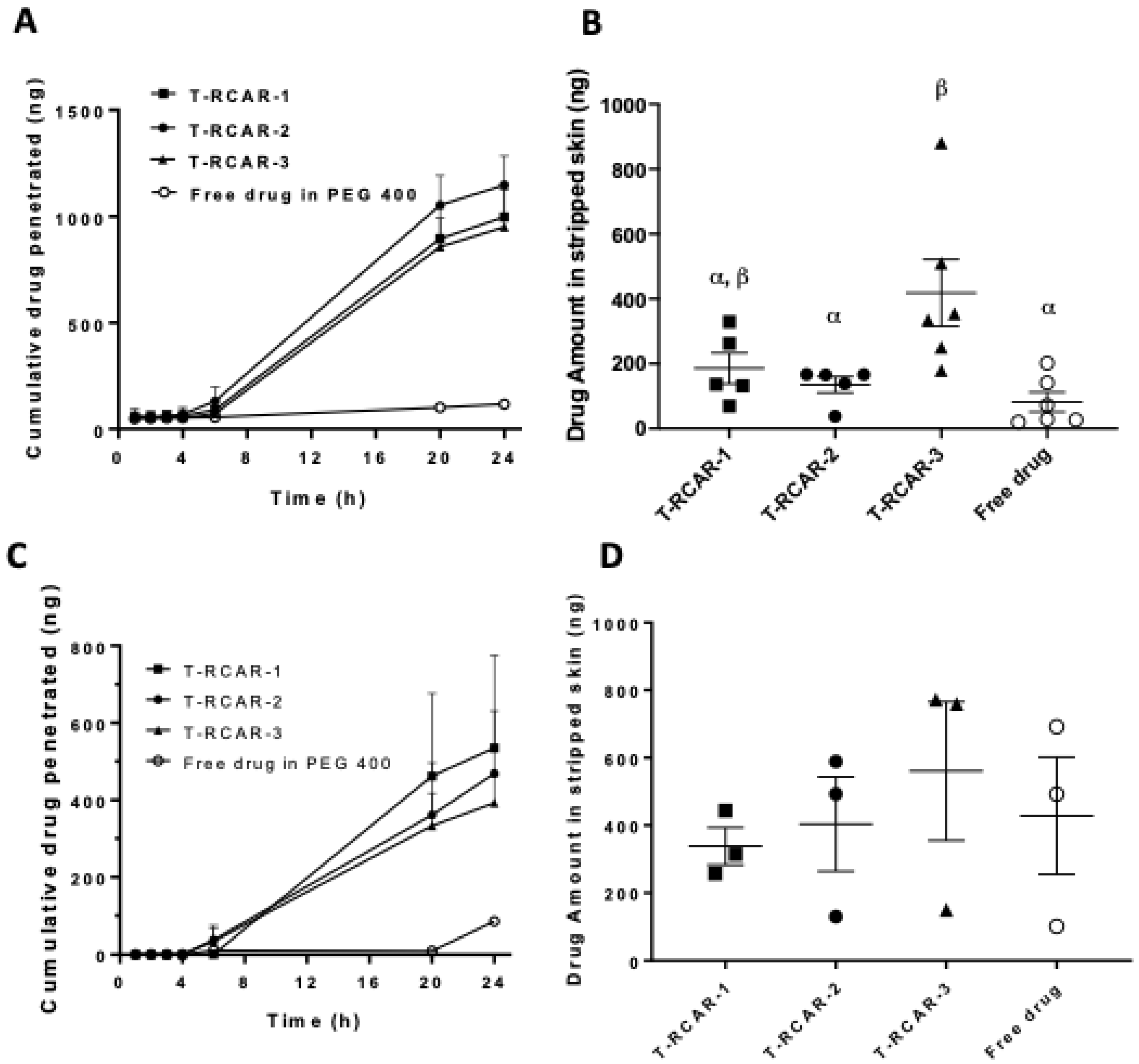
2.5. Ex Vivo Skin Permeation Analysis
The ex vivo skin permeation and retention studies were performed using the Franz diffusion system (Crown Glass Company, Somerville, NJ, USA) (surface area of 1.13 cm
2), loaded with porcine ear skin (Sierra for Medical Science, Whittier, CA, USA). The methods were previously reported [
17,
18]. In brief, the receiver compartment was filled with 5.5 mL of 40%
v/
v PEG 400 in PBS (pH 7.4) or 4% bovine serum albumin (BSA) in PBS and maintained at 37 °C under magnetic stirring. PEG 400 or BSA was added to increase the solubility of permeated R-carvedilol. T-RCAR transfersomes or the free drug dissolved in PEG 400 containing 4 µg R-carvedilol (200 mL) were applied onto the porcine skin in the donor compartment. At the time intervals of 0.5, 1, 2, 3, 4, 6, 20, and 24 h, 0.2 mL solvent in the receiver compartment was collected and replaced with 0.2 mL solvent.
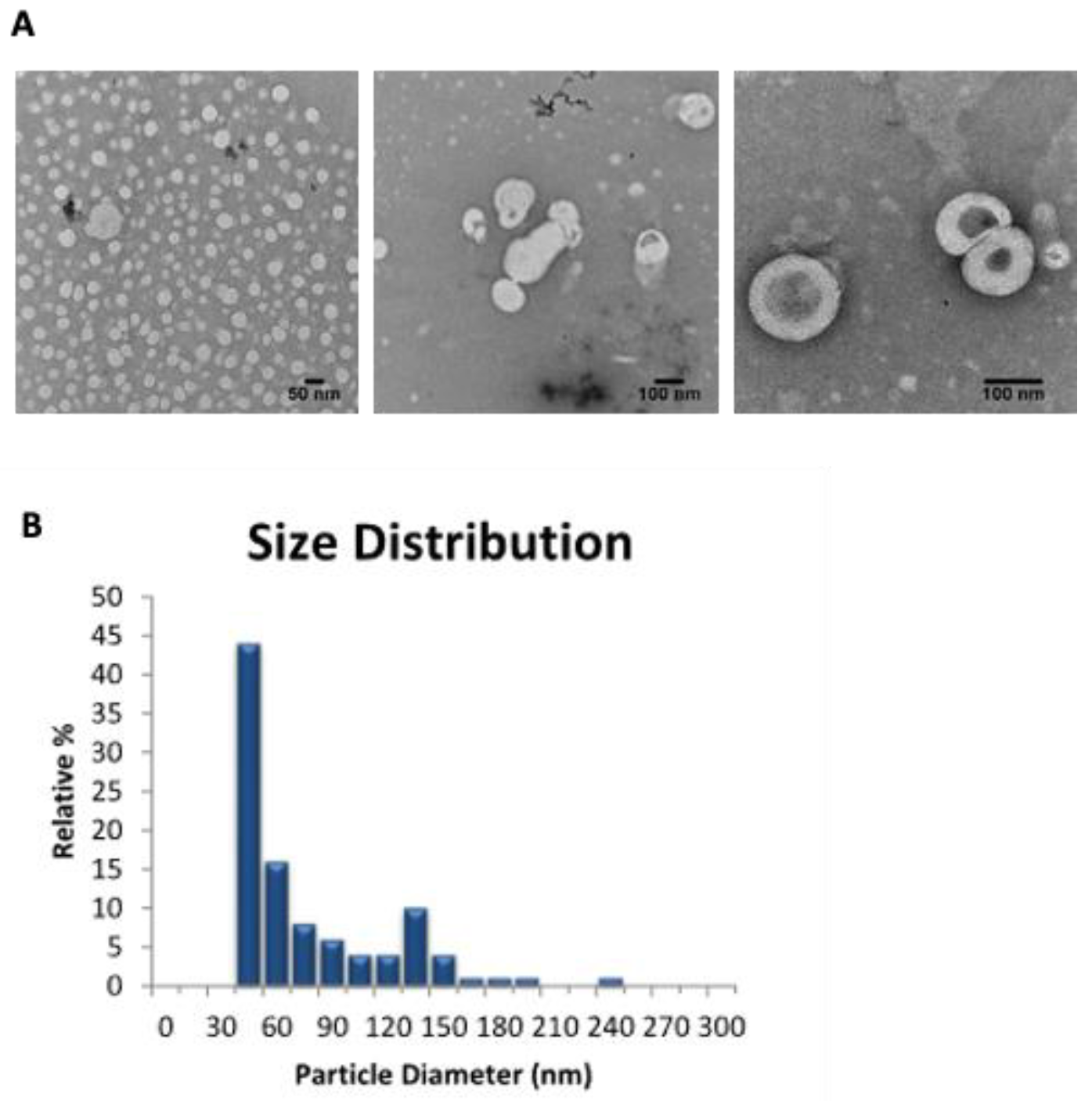
2.6. Transmission Electron Microscopic (TEM) Analysis
TEM is a visualization tool for nanoparticles and was used to obtain a quantitative measure of particle size and size distribution [
23]. Vesicles that are suspended in PBS were examined by TEM with the negative staining method at Fortis Life Sciences/nanoComposix (San Diego, CA, USA). In brief, samples were prepared for imaging by drying the nanoparticles on a copper grid coated with a thin layer of carbon. Images were obtained by the use of a JEOL 1010 transmission electron microscope (JEOL USA, Peabody, MA, USA), operating at an accelerating voltage of 100 keV and an AMT XR41-B 4-megapixel (2048 × 2048) bottom mount camera. The camera’s finite conjugate optical coupler provides high resolution and flat focus with less than 0.1% distortion for magnifications as high as 150,000×.
2.7. HPLC Analysis
After R-carvedilol was received, chiral HPLC analysis was used to determine the purity and accuracy of R-Carvedilol, with Phenomenex Lux® 5 µm Cellulose-4 LC Column 250 × 4.6 mm (Part No. 00G-4491-E0, Serial Number H21-389311, Batch No. 5599-0063) (Phenomenex, Torrance, CA, USA). The drug level was detected using an Agilent 1260 HPLC system (Agilent Technologies Inc., Santa Clara, CA, USA), equipped with a quaternary pump (G1311B), an autosampler (G7129A), an automatic thermostatic column compartment, a diode array detector (DAD) detector (G1315D), and a computer with Agilent OpenLAB CDS Chemstation Edition for LC&LC/MS Systems (Rev C.01.07). The drug was separated on a BDS Hypersil C18 reverse-phase column (2.1 × 150 mm; 2.4 um) (Thermo Scientific, Waltham, MA, USA) coupled with a C18 guard column (10 mm × 2.1, 3 um) (Thermo Scientific). The mobile phase was a mixture of acetonitrile:buffer (38:62); the buffer was made of 20 mM ammonium acetate, 0.1% triethylamine, and adjusted to pH 4.5 with phosphoric acid. The flow rate was 0.2 mL/min. R-carvedilol was analyzed at the wavelength of 240 nm. Propranolol (1 µg/mL) was used as an internal standard.
2.8. Cell Culture and MTT Assay (2D)
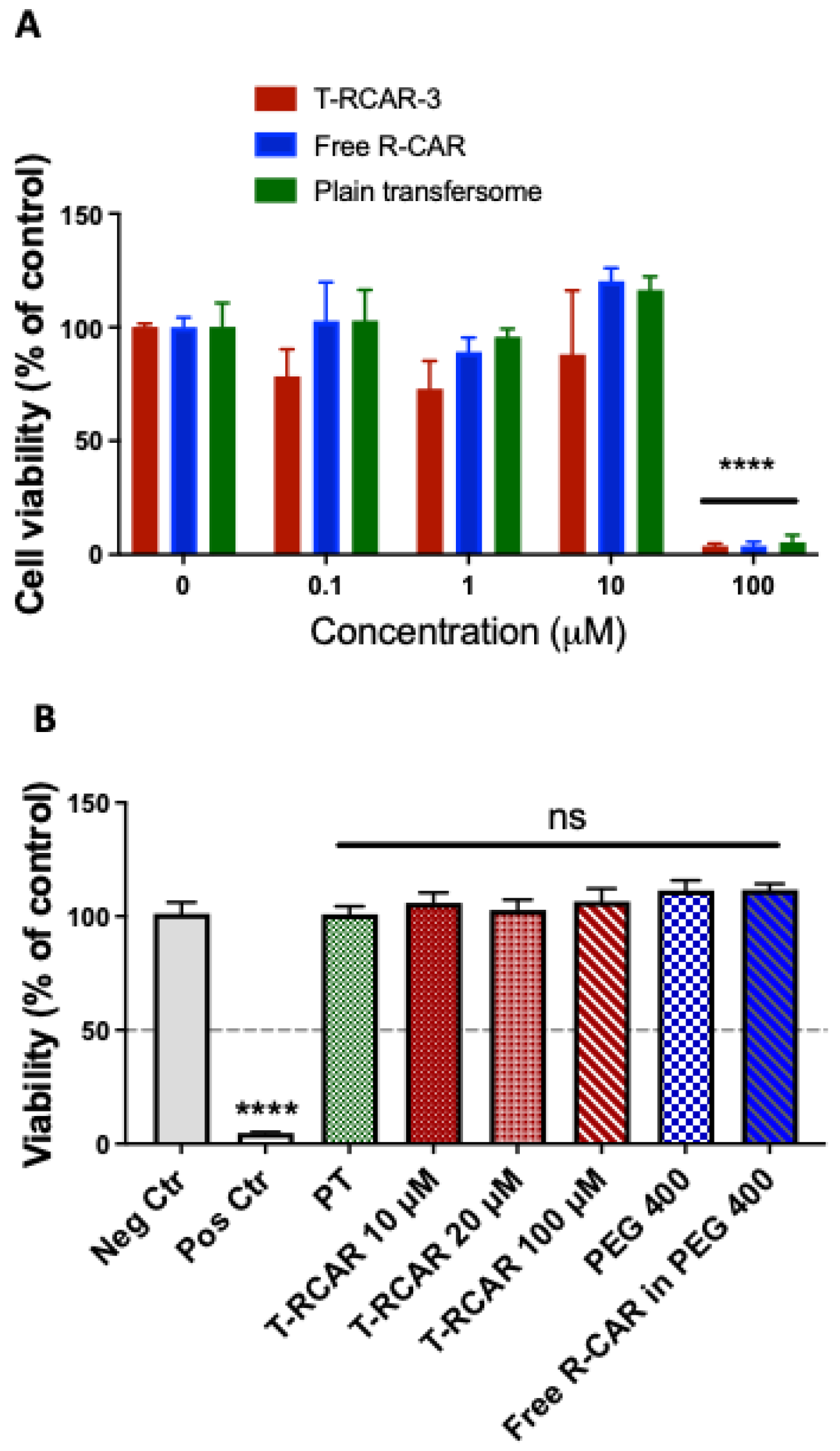
The in vitro cytotoxicity was evaluated in the monolayer culture of the non-tumorous murine epidermal cell line JB6 CI 41-5a (JB6 P+) (ATCC, Manassas, VA, USA) using MTT (3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyl tetrazolium bromide) assay, because this cell line was shown as a commonly used model to predict in vivo skin toxicity of chemicals [
23]. JB6 P+ cells were maintained in Eagle’s minimum essential medium (EMEM) containing 4% heat-inactivated fetal bovine serum and 1% penicillin/streptomycin. The cells were seeded in a 96-well plate at a density of 1 × 10
4 cells/100 μL medium/well and incubated overnight or until 70–80% confluence. The cells were treated with T-RCAR-3, free R-carvedilol, or plain transforsome (PT). The drug concentrations were 0.1, 1, 10, and 100 µM. The PT was diluted the same way as the T-RCAR. MTT assay was conducted 48 h after incubation. The stock solution (5 mg/mL) of thiazolyl blue tetrazolium bromide (MTT; Sigma, M2128) was prepared in DPBS (pH 7.4) and filtered to remove crystals and to sterilize. The MTT solution was added to each well in an amount equal to 10% of the cell culture volume and the plate was incubated at 37 °C for 4 h. Isopropanol with 0.1 N HCl (100 µL) was added to each well to replace the media before using a spectrophotometer at 570 nm wavelength to read the optic density of the formazan salt produced (reference 630 nm).
2.9. EpiDerm Skin Irritation Test (3D)
The in vitro skin irritation test for T-RCAR was conducted according to the protocol developed by MatTek Corporation (Ashland, MA, USA) of “EPI-200-STI”, a reconstructed human epidermal model EpiDerm [
24]. The EpiDerm skin culture was purchased from MatTek. In brief, eight treatment groups including the negative and positive controls were established on the EpiDerm culture (sample size n = 3). The negative control was DPBS and the positive control was 5% SDS. The test groups consisted of the plain transfersome (same dilution as the 100 μM of T-RCAR), T-RCAR-3 at three doses (10 μM, 20 μM, and 100 μM), PEG 400 as the vehicle for free drug, and 100 μM of a R-carvedilol-free drug dissolved in PEG 400. The EpiDerm culture was exposed to test agents for 60 min and incubated at 37 °C without treatments for 2 days. Then a MTT assay was used to determine cell viability and irritation. After, the same procedure was conducted as the 2D MTT assay. A 96-well plate was used to read the optic density of the formazan salt produced in the Epiderm samples that included two of each treatment group. Then the mean was taken.
2.10. Acute and Repeat Dose Dermal Toxicity Study in Mice
All animal studies were carried out under the recommendations and guidelines established by the Western University of Health Sciences’ Institutional Animal Care and Use Committee, which approved these studies. Mice had access to water and food ad libitum and housed on a 12 h light/dark cycle with 35% humidity. All SKH-1 hairless mice were obtained from our internal breeding protocol with breeding pairs purchased from Charles River (Wilmington, MA, USA).
The acute dermal toxicity study (single dose testing) was carried out in accordance with the OECD guidelines No. 402 (2017) with modification. In brief, six female adult healthy SKH-1 hairless mice (6~8 weeks old) were randomly divided into two groups (control and T-RCAR treatment). Although 10 µM of R-carvedilol was effective in our previous studies [
13], the toxicity study started at a higher dose, 100 µM in 0.5% Carbopol gel (200 µL). According to our previous study, the gel form and suspension form of transfersomes of carvedilol showed the same skin permeation profile [
17]. On day 0, a single dose of T-RCAR gel was applied topically with a uniform distribution over the back area of ~6 cm
2. Body weight was measured on days 0, 1, 2, 3, and 14. The skin phenotypes were assessed using the multi-probe adapter system (Courage and Khazaka Electronic GmbH, Cologne, Germany), a non-invasive method commonly used to evaluate skin irritation and barrier function, which includes other methods used to evaluate skin dryness, erythema, and trans-epidermal water loss (TEWL). This was conducted at days 0, 1, 2, and 3.
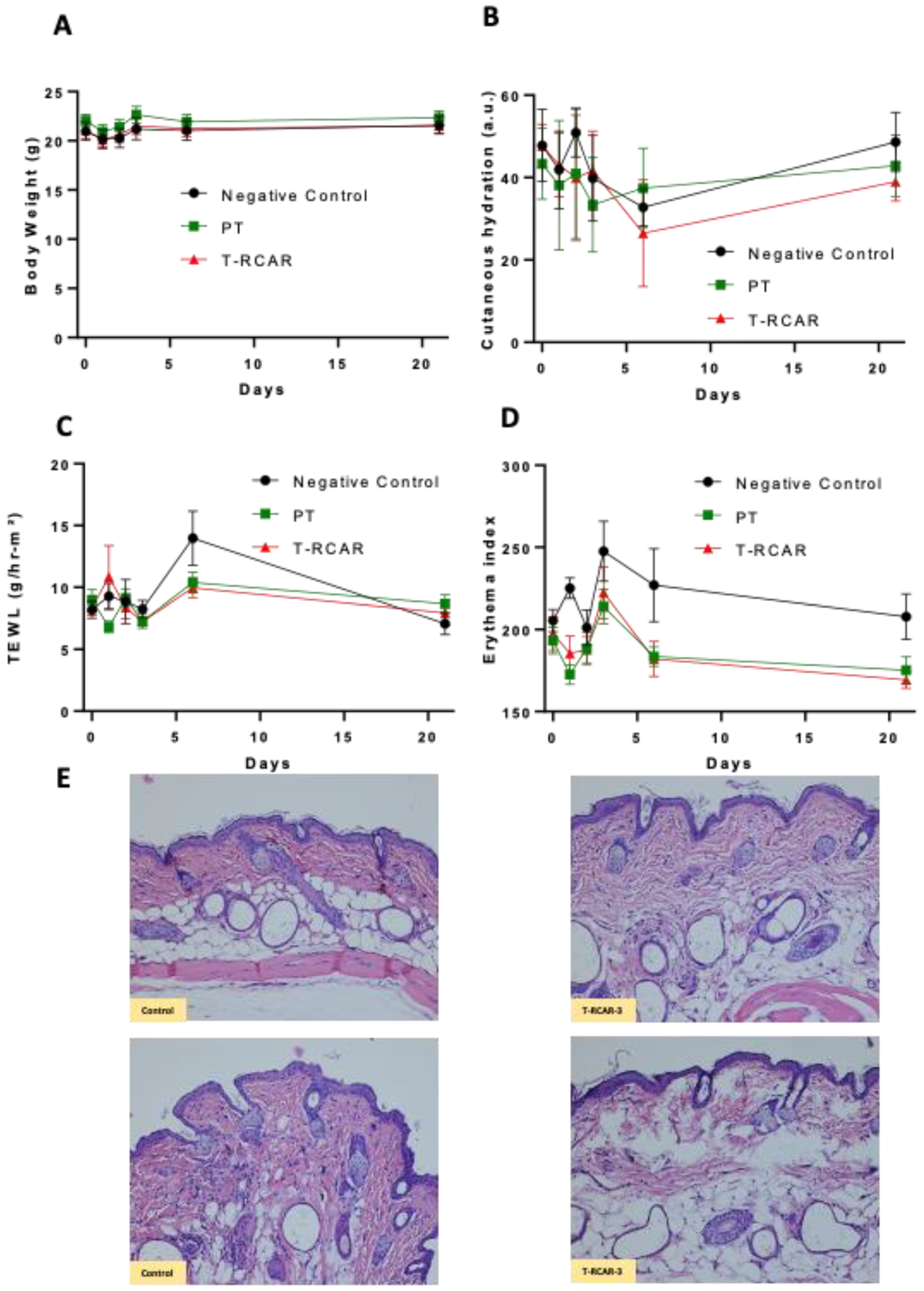
The repeated dose acute dermal toxicity study was carried out in accordance with the OECD guidelines No. 410 (1981) with modification. In brief, adult healthy mice (6~8 weeks old, females) were used. Animals were randomized into three groups: negative control, plain transfersome (PT), and T-RCAR. Four animals were used as negative control without any treatment. Six animals were used in the PT and in the T-RCAR group, which were then treated with T-RCAR containing 100 μM (200 μL) of drug or the plain transfersomes of the same volume. This was applied topically once every day for 21 days corresponding to the two groups. The treatment started on day 0. On days 0, 1, 2, 3, 6, and 21, the body weight and skin parameters were measured. Animals were euthanized at the end of the study, 24 h after the last dose. Major organs including skin, liver, kidneys, lung, heart, and spleen were excised and stored in formalin for histological evaluation.
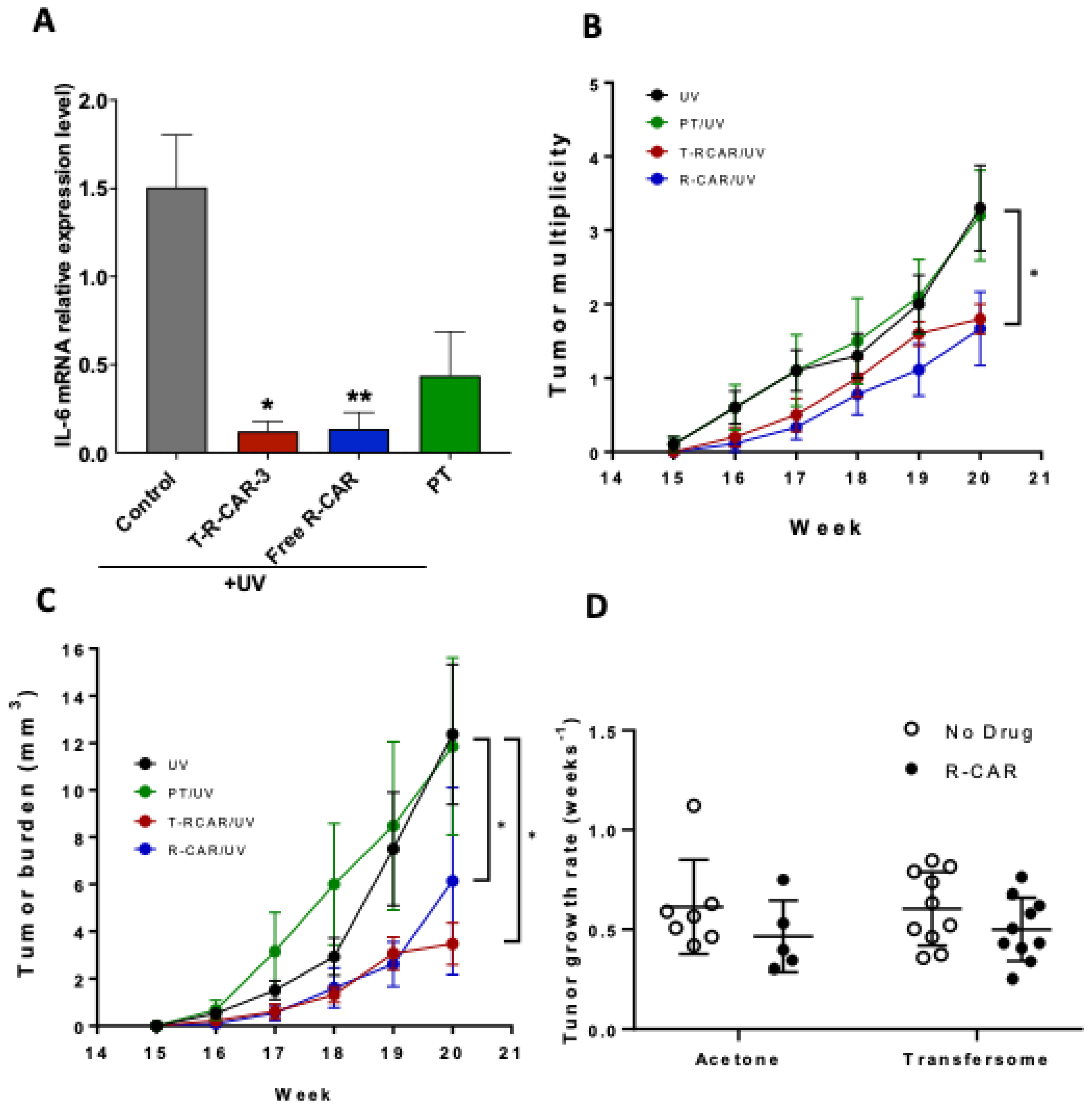
2.11. UV-Induced Acute Skin Inflammation
Female SKH-1 hairless mice, seven-eight weeks of age, were randomly divided into four groups (n = 3~4): (1) UV + PEG 400 vehicle, (2) UV + T-RCAR-3 gel containing 10 μM R-carvedilol, (3) UV + free R-carvedilol 10 μM in PEG 400 solution, and (4) UV + plain transfersomes gel. The UV lamps used in these studies were previously described [
17]. Topical treatment of drug or vehicle was given on day −2, −1, and day 0 immediately after a single dose of UV radiation (336 mJ/cm
2). For all topical treatments, a 200 μL volume of test agents were applied to the back of the mouse. The area of treatment for each mouse was approximately 6 cm
2 of back skin. During the UV exposure, mice roamed freely in acrylic cages on a rotating platform, ensuring consistent and equal dorsal distribution of UV irradiation. Six hours after UV exposure, all mice were euthanized. Whole skin samples were dissected for RNA isolation.
2.12. RNA Isolation and qPCR Analysis
Total RNA was isolated from whole skin tissue using the RNeasy Mini Kit (Qiagen, Germantown, MD, USA). cDNA was synthesized with the High-Capacity cDNA Reverse Transcriptase Kit (Thermo Fisher). cDNA and SYBR Green Supermix (Thermo Fisher) were mixed with primers for mouse IL-6 gene and β-actin (the primer sequences are available upon request). qPCR was performed on a CFX96 real-time thermal cycler detection system (Bio-rad, Hercules, CA, USA) and analyzed with the 2−ΔΔct with β-actin as the normalization control.
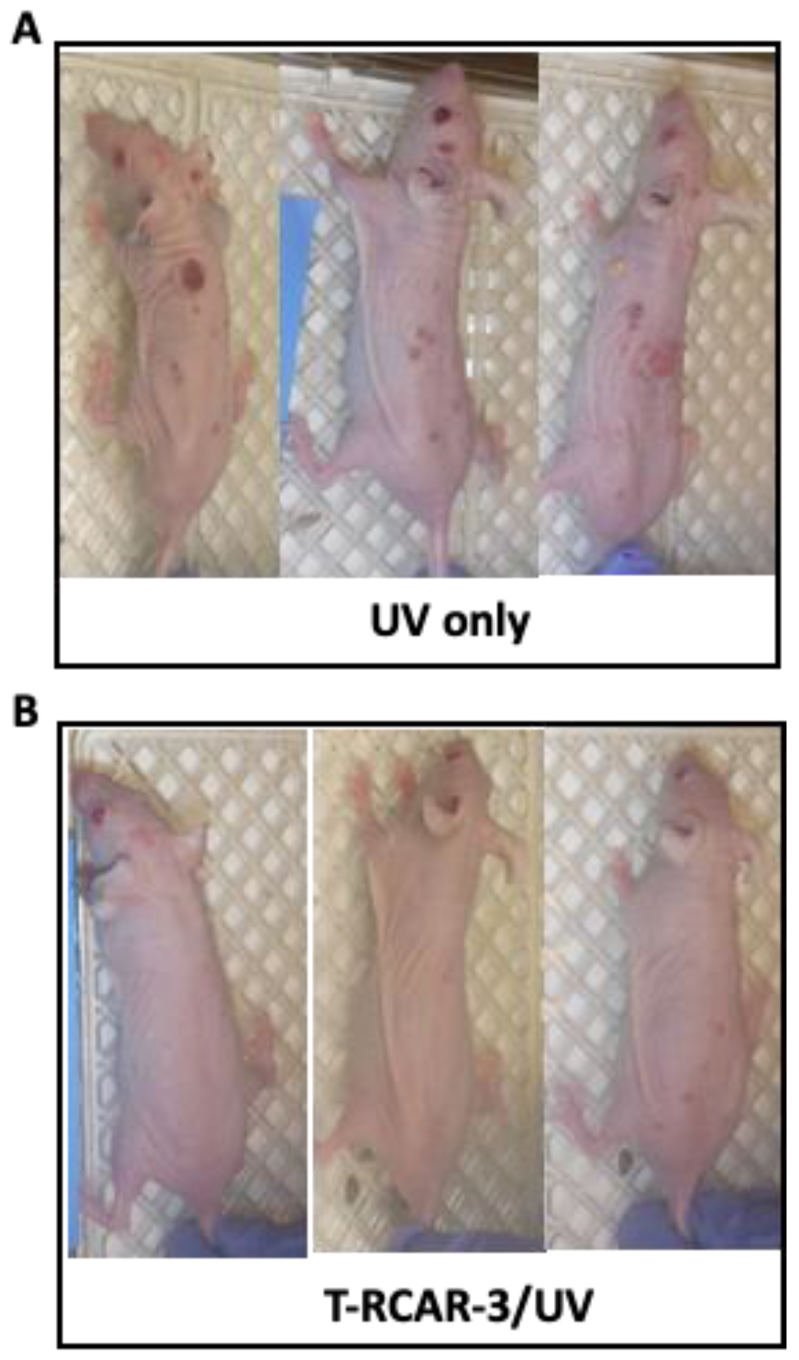
2.13. Chronic UV-Induced Skin Tumorigenesis
Seven-week-old female SKH-1 mice were randomly divided into four groups (n = 10): (1) UV only control, (2) UV-exposed followed by plain transfersome (PT) gel treatment, (3) UV-exposed followed by T-CAR gel treatment (10 µM), and (4) UV-exposed followed by the free drug R-carvedilol. The volume for topical treatment was 300 μL. Mice were pretreated with drugs three times a week for two weeks before starting UV exposure. The mice were then irradiated with gradually increasing levels of UV three times a week for 25 weeks with an initial dose of 50 mJ/cm2. The UV was increased each week by 25 mJ/cm2 to 150 mJ/cm2, which was continued for the duration of the experiment. The drug was applied topically immediately after UV radiation. Tumors of at least 1 mm in diameter were counted and measured with a caliper weekly. The tumor volume was calculated according to the formula: (width)2 × length/2.
2.14. Statistical Analysis
All the data were expressed as a mean ± standard deviation (SD) or standard error (SE) unless stated otherwise. In histograms, all data are shown with a line representing the group mean. All plots were made using GraphPad Prism version 9.2.0 (La Jolla, CA, USA). Statistical analysis of the data was conducted in Prism for one-way ANOVAs, and all other statistical analysis was conducted using NCSS 2019 Statistical Software (Kaysville, UT, USA). The specific statistical tests are detailed in the text and figure legends. For all statistical analyses, means were indicated to be statistically different when p < 0.05.
4. Discussion
The present study developed R-carvedilol-loaded transfersomes, namely “T-RCAR” and characterized these formulations in vitro and in vivo. This study produced essential data to support our hypothesis that T-RCAR formulations could be effective and safe. Several R-carvedilol-uploaded transfersomes were prepared and characterized. Firstly, three phospholipids were used: SPC, DSPC, and HEPC. While DSPC and HEPC failed to make stable transfersomes, SPC-made transfersomes were most stable and used throughout the formulation development. Secondly, two different surfactants were used, Tween-80 and sodium cholate. Both surfactants successfully resulted in stable transfersomes (
Table 1). According to a pilot pig ear skin permeation study (
Table 1), Tween-80 was selected for development of transfersomes. Thirdly, three transfersomes with different drug:lipid:surfactant ratios, named T-RCAR-1, T-RCAR-2, and T-RCAR-3, were compared in terms of stability, in vitro drug release, and ex vivo skin drug retention (
Table 2 and
Table 3) (
Figure 1,
Figure 2 and
Figure 3). T-RCAR-3, which contains the highest level of Tween-80 among the three transfersomes, was selected based on the ex vivo skin retention data (
Figure 2). For the ex vivo skin permeation and retention study, two different types of fluids were used in the receptor chamber. Since R-carvedilol is a lipophilic compound, using PBS alone may result in lower permeability of R-carvedilol. The first fluid we used was PBS containing 40% PEG 400. PEG 400 was added to the receptor chamber to increase the solubility of R-carvedilol. The same experiment was conducted using PBS containing 4% BSA since PEG 400 is not naturally present in the body. According to the literature report [
29], the BSA-containing fluid can better predict transdermal drug delivery for lipophilic compounds. Both fluids consistently showed that T-RCAR-3 had the highest skin retention. Although we do not yet understand the mechanism, Tween 80 level appeared to correlate with stability, in vitro release, and skin retention. Furthermore, the ex vivo skin permeation and retention study was conducted using the Franz diffusion cell system loaded with porcine ear skin. Future studies should confirm this finding on excised human skin.
Although most studies (
Figure 4,
Figure 5,
Figure 6,
Figure 7 and
Figure 8) were conducted only for selected T-RCAR-3, other transfersomes with different content of Tween 80 may be also effective. However, T-RCAR-1, which does not contain any Tween 80 should not be considered, since after long-term storage, a precipitation was observed (
Figure 3). The one-year stability data for the three T-RCAR formulations, although interesting, are limited due to small sample sizes. The long-term stability studies were not planned initially, but focused on T-RCAR-3 for a 5-week stability study, which is shown in
Table 3. Therefore, future studies should be directed to verify the long-term stability of these formulations in different storage conditions. In fact, based on the definition of transfersomes, T-RCAR-1 is not classified as a transferosome as it does not contain surfactant but is a conventional liposome. T-RCAR-2 and T-RCAR-3 performed rather similarly in the comparison studies (
Figure 1,
Figure 2 and
Figure 3); however, T-RCAR-3 matches previously reported carvedilol transfersomal formulations [
17] and performed marginally better in the comparisons. Therefore, T-RCAR-3 was selected for further testing.
The EpiDerm model is a physiologically relevant skin vitro skin models consisting of epidermis and dermis. Although the irritating results from EpiDerm are accepted, due to the robust barrier properties of the EpiDerm model, the non-irritating results may require further verification by other methods [
30]. The in vitro and in vivo skin irritation studies used a higher dose than the effective dose in previous mouse cancer prevention studies [
13]: 100 μM, which is 10 times higher than the effective dose, showed no irritation on the 3D human skin construct and in SKH-1 mice (
Figure 5 and
Figure 6). Further efficacy studies should be conducted to evaluate whether doses as high as 100 μM can be more effective. Further efficacy studies will also need to evaluate whether doses lower than 10 μM can be effective. The future goal is to identify the minimally effective dose for R-carvedilol transfersomes, which is essential information for future clinical drug development.
The current study did not provide comprehensive mechanistic data for the R-carvedilol transfersomes. R-carvedilol and the racemic carvedilol, which contains R- and S-carvedilol, attenuated UV radiation-medicated skin lesions via multiple mechanisms of action. In a previous report [
13], several assays were used to determine the effects of the free drug R-carvedilol on UV-induced oxidative stress, inflammation, and DNA damage, in vitro and in vivo. In the current study, IL-6 expression was used as the representative proinflammatory biomarker (
Figure 7). Future work should investigate the potential mechanisms of action for R-carvedilol’s skin cancer preventive activity.
Although carvedilol-loaded transfersomes were effective and safe in principle [
17], R-carvedilol-loaded transferosomes were preferred over carvedilol-loaded transferosomes for cancer prevention. The reason is that carvedilol is a highly potent β-blocker, with an IC
50 at nanomolar ranges [
31]; skin-targeted formulations may still be absorbed into the systemic circulation, particularly if patients have skin damage due to sunburn or another wound. Additionally, a topical product that is safe if swallowed increases the overall safety profile of the product. Due to the fact that R-carvedilol can effectively prevent UV-induced skin damage at much lower doses (0.1 μM) [
13], it is feasible to develop an over-the-counter topical formulation. The potential clinical applications for such a topical formulation include preventive treatments for a range of skin lesions associated with exposure to UV radiation, including sunburn, actinic keratoses (pre-cancerous skin lesions), and skin cancer, including both non-melanoma and melanoma skin cancer. A T-RCAR formulation could be applied by any individual before sunlight exposure or after a sunburn. However, additional preclinical studies are needed before clinical trials can be started. Specifically, all the efficacy studies presented in the present study have a pre-treatment paradigm (
Figure 7), which needs further evaluation as pre-treatment may not be feasible for all people.

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}