
Electron Microscopy (EM) Analysis of Collagen Fibers in the Peri-Implant Soft Tissues around Two Different Abutments
 , , ,
, , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
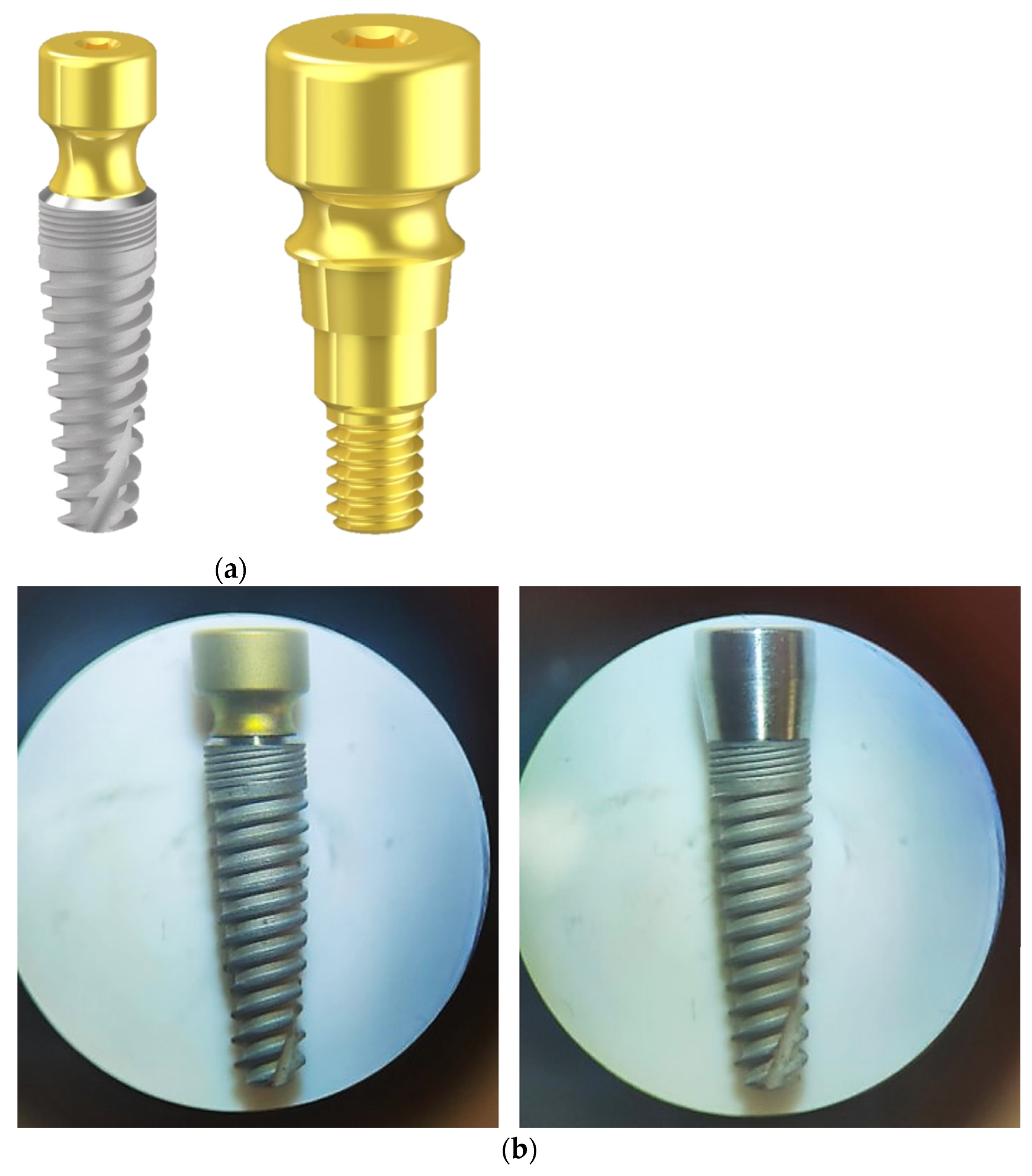
2.1. Implant Characteristics
2.2. Ethical Statement
2.3. Experimental Animals and Housing
2.4. Experimental Design
2.5. Surgical and Terminal Procedures
2.6. Samples Preparation
2.7. Electron Microscopy (EM)
2.7.1. Preparation and Analysis of Samples for EM
2.7.2. EM Ultrastructural Analysis of Collagen Bundles
2.7.3. EM Quantitative Analysis of Collagen Bundles
- (i)
- In each micrograph, the total area covered by collagen bundles was evaluated by drawing the outline of each bundle using the Soft Imaging System (GmbH, Muenster, Germany). All measured bundle values were then mathematically summarized. Only cross-sectioned bundles with a minimum size of 0.5 µm2, where collagen fibers were distinguishable and not longitudinally oriented, were considered for the analysis. Considering that each micrograph at 7100× of magnification covers 142.6 µm2 of sample, the relative presence of collagen bundles (%) in each sample was obtained by dividing the number of total outlined collagen fibers (in µm2) by the total area of analyzed samples (i.e., 142.6 µm2 × 15 micrographs).
- (ii)
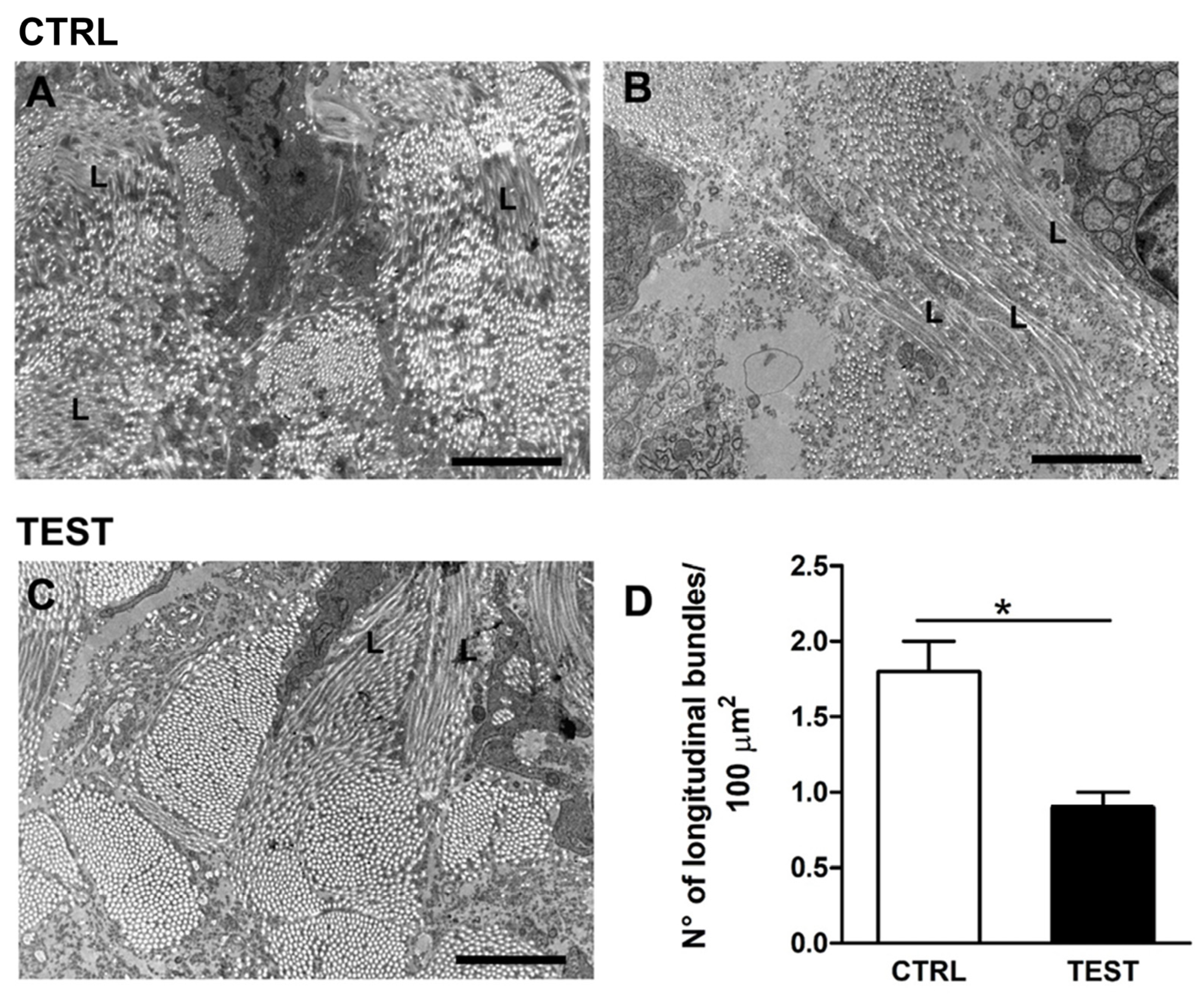
- In each micrograph, the number of longitudinally oriented bundles of collagen (of different sizes) was counted and reported as mean ± standard error of the mean (SEM) in 100 µm2.
2.8. Statistical Analysis
3. Results
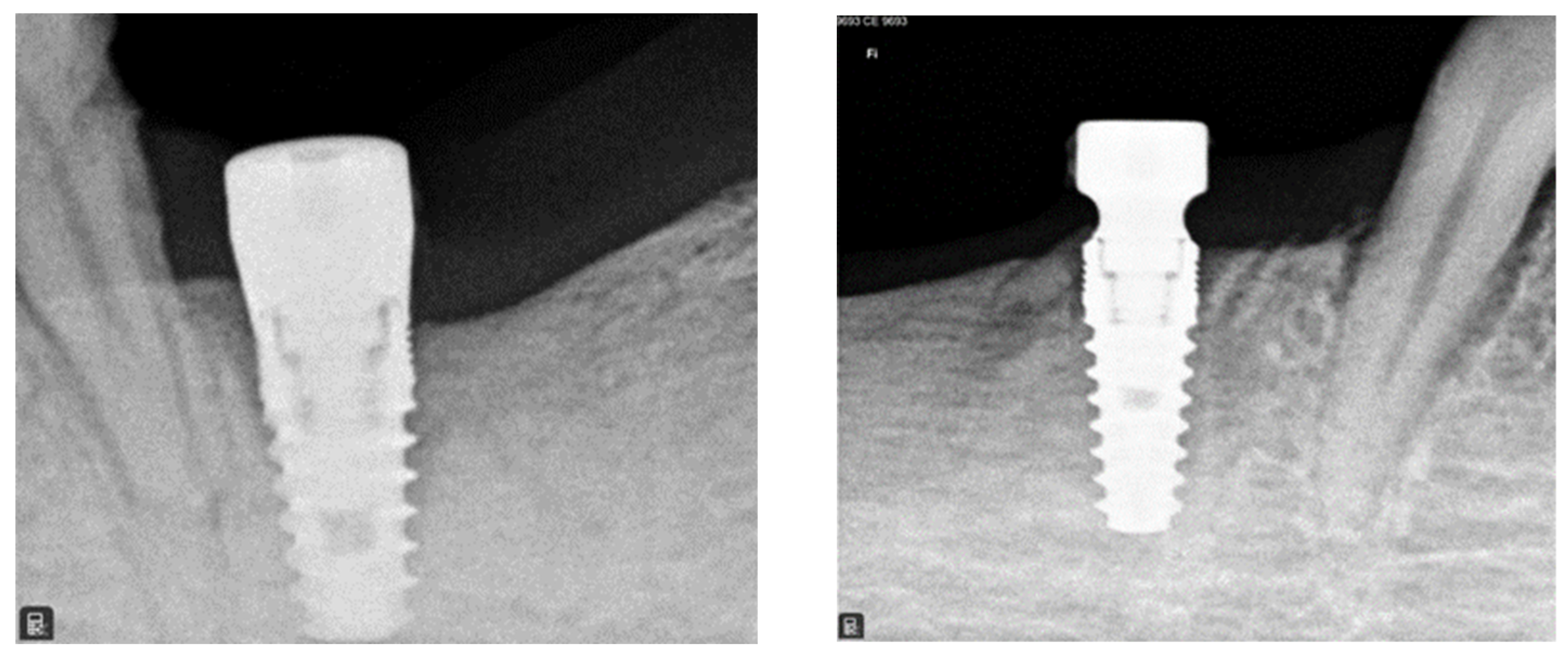
3.1. Radiographic Analysis
3.2. Histological Analysis
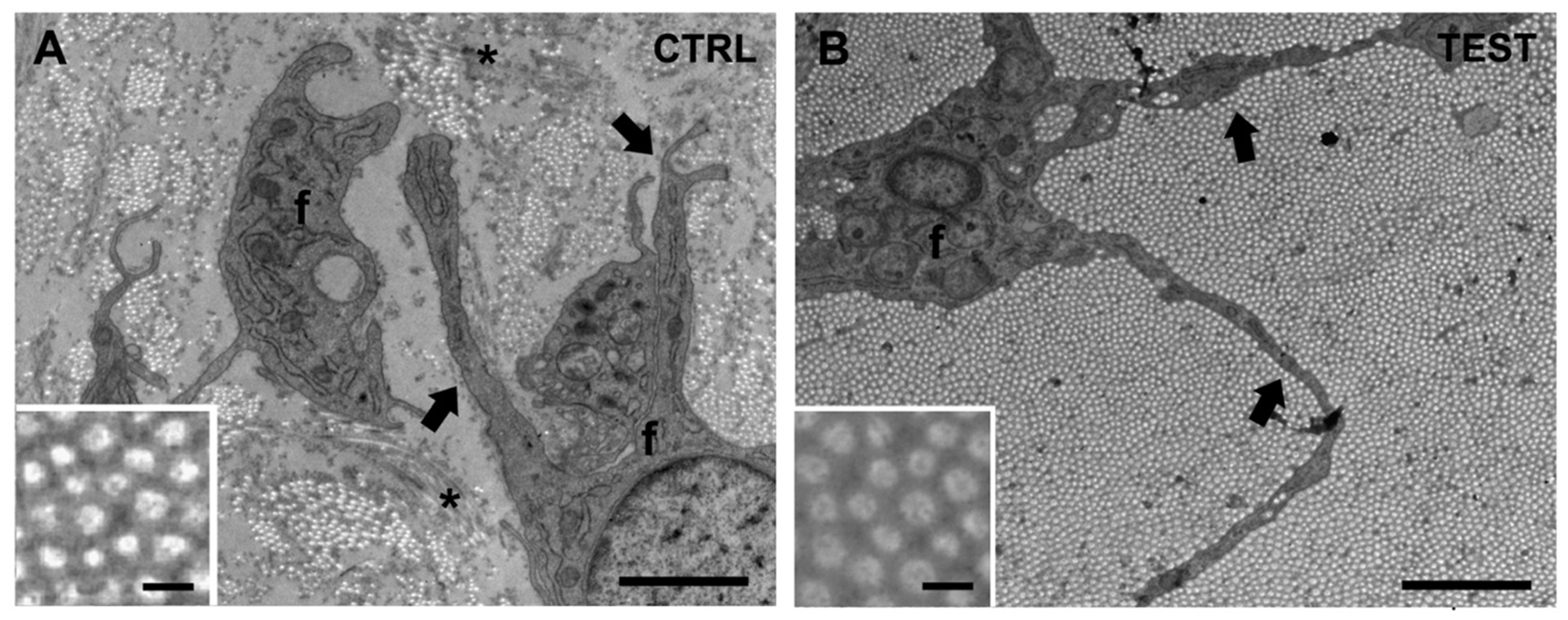
3.3. EM Ultrastructural Analysis of Collagen Fibers in the Peri-Implant Soft Tissue
3.4. EM Quantitative Analysis of Collagen Fiber Bundles
3.5. Additional Ultrastructural Observations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated Titanium Implants. Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Geckili, O.; Bilhan, H.; Geckili, E.; Cilingir, A.; Mumcu, E.; Bural, C. Evaluation of Possible Prognostic Factors for the Success, Survival, and Failure of Dental Implants. Implant Dent. 2014, 23, 44–50. [Google Scholar] [CrossRef]
- Bolle, C.; Gustin, M.P.; Fau, D.; Exbrayat, P.; Boivin, G.; Grosgogeat, B. Early Periimplant Tissue Healing on 1-Piece Implants with a Concave Transmucosal Design: A Histomorphometric Study in Dogs. Implant Dent. 2015, 24, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Meyle, J.; on behalf of Group D of the European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef]
- Schwarz, F.; Ramanauskaite, A. It Is All about Peri-Implant Tissue Health. Periodontology 2000 2022, 88, 9–12. [Google Scholar] [CrossRef]
- Suárez-López del Amo, F.; Lin, G.-H.; Monje, A.; Galindo-Moreno, P.; Wang, H.-L. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, S.; Lee, R. Comparison of Peri-Implant and Periodontal Marginal Soft Tissues in Health and Disease. Periodontology 2000 2018, 76, 116–130. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S237–S248. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J. Dimension of the Periimplant Mucosa. Biological Width Revisited. J. Clin. Periodontol. 1996, 23, 971–973. [Google Scholar] [CrossRef]
- Berglundh, T.; Abrahamsson, I.; Welander, M.; Lang, N.P.; Lindhe, J. Morphogenesis of the Peri-Implant Mucosa: An Experimental Study in Dogs. Clin. Oral Implant. Res. 2007, 18, 1–8. [Google Scholar] [CrossRef]
- Mattheos, N.; Janda, M.; Acharya, A.; Pekarski, S.; Larsson, C. Impact of Design Elements of the Implant Supracrestal Complex (ISC) on the Risk of Peri-Implant Mucositis and Peri-Implantitis: A Critical Review. Clin. Oral Implant. Res. 2021, 32 (Suppl. 21), 181–202. [Google Scholar] [CrossRef] [PubMed]
- Glauser, R.; Schüpbach, P.; Gottlow, J.; Hämmerle, C.H.F. Periimplant Soft Tissue Barrier at Experimental One-Piece Mini-Implants with Different Surface Topography in Humans: A Light-Microscopic Overview and Histometric Analysis. Clin. Implant Dent. Relat. Res. 2005, 7 (Suppl. 1), s44–s51. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Wennström, J.; Lindhe, J. The Peri-Implant Hard and Soft Tissues at Different Implant Systems. A Comparative Study in the Dog. Clin. Oral Implant. Res. 1996, 7, 212–219. [Google Scholar] [CrossRef]
- Ruggeri, A.; Franchi, M.; Marini, N.; Trisi, P.; Piattelli, A. Supracrestal Circular Collagen Fiber Network around Osseointegrated Nonsubmerged Titanium Implants. Clin. Oral Implant. Res. 1992, 3, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Kim, D.K.; Jun, S.H.; Guze, K.; Schupbach, P.; Nevins, M.L. Histologic evidence of a connective tissue attachment to laser microgrooved abutments: A canine study. Int. J. Periodontics Restor. Dent. 2010, 30, 245–255. [Google Scholar]
- Nevins, M.L.; Camelo, M.; Schupbach, P.; Kim, S.W.; Kim, D.M.; Nevins, M. Human clinical and histologic evaluation of laser-assisted new attachment procedure. Int. J. Periodontics Restor. Dent. 2012, 32, 497–507. [Google Scholar]
- Shapoff, C.A.; Babushkin, J.A.; Wohl, D.J. Clinical Use of Laser-Microtextured Abutments: A Case Series. Int. J. Periodontics Restor. Dent. 2016, 39, 655–662. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Tommasato, G.; Patini, R.; Canullo, L. Influence of modified titanium abutment surface on peri-implant soft tissue behaviour: A systematic review of histological findings. Int. J. Oral Implantol. 2019, 12, 419–429. [Google Scholar]
- Geurs, N.C.; Geisinger, M.L.; Vassilopoulos, P.J.; O’Neal, S.J.; Haigh, S.J.; Reddy, M.S. Optimizing Connective Tissue Integration on Laser-Ablated Implant Abutments. Clin. Adv. Periodontics 2016, 6, 153–159. [Google Scholar] [CrossRef]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Zirconia compared to titanium dental implants in preclinical studies-A systematic review and meta-analysis. Clin. Oral Implant. Res. 2019, 30, 365–395. [Google Scholar] [CrossRef]
- Blázquez-Hinarejos, M.; Ayuso-Montero, R.; Jané-Salas, E.; López-López, J. Influence of surface modified dental implant abutments on connective tissue attachment: A systematic review. Arch. Oral Biol. 2017, 80, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, X.; Vela, X.; Calvo-Guirado, J.L.; Nart, J.; Stappert, C.F.J. Effect of Platform Switching on Collagen Fiber Orientation and Bone Resorption around Dental Implants: A Preliminary Histologic Animal Study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1116–1122. [Google Scholar]
- Nelson, C.M. Geometric Control of Tissue Morphogenesis. Biochim. Biophys. Acta 2009, 1793, 903–910. [Google Scholar] [CrossRef]
- Mattheos, N.; Vergoullis, I.; Janda, M.; Miseli, A. The Implant Supracrestal Complex and Its Significance for Long-Term Successful Clinical Outcomes. Int. J. Prosthodont. 2021, 34, 88–100. [Google Scholar] [CrossRef]
- Ciurana, X.; Acedo, Á.; Vela, X.; Fortuño, A.; García, J.; Nevins, M. Arrangement of Peri-Implant Connective Tissue Fibers Around Platform-Switching Implants with Conical Abutments and Its Relationship to the Underlying Bone: A Human Histologic Study. Int. J. Periodontics Restor. Dent. 2016, 36, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruiz, R.A.; Calvo-Guirado, J.L.; Abboud, M.; Ramirez-Fernandez, M.P.; Maté-Sánchez de Val, J.E.; Negri, B.; Gomez-Moreno, G.; Markovic, A. Connective Tissue Characteristics around Healing Abutments of Different Geometries: New Methodological Technique under Circularly Polarized Light. Clin. Implant Dent. Relat. Res. 2015, 17, 667–680. [Google Scholar] [CrossRef]
- Kim, S.; Oh, K.C.; Han, D.H.; Heo, S.J.; Ryu, I.C.; Kwon, J.H.; Han, C.H. Influence of transmucosal designs of three one-piece implant systems on early tissue responses: A histometric study in beagle dogs. Int. J. Oral Maxillofac. Implant. 2010, 25, 309–314. [Google Scholar]
- Bishti, S.; Strub, J.R.; Att, W. Effect of the Implant-Abutment Interface on Peri-Implant Tissues: A Systematic Review. Acta Odontol. Scand. 2014, 72, 13–25. [Google Scholar] [CrossRef]
- Gibbs, S.; Roffe, S.; Meyer, M.; Gasser, A. Biology of Soft Tissue Repair: Gingival Epithelium in Wound Healing and Attachment to the Tooth and Abutment Surface. Eur. Cells Mater. 2019, 38, 63–78. [Google Scholar] [CrossRef]
- Valente, N.; Wu, M.; Toti, P.; Derchi, G.; Barone, A. Impact of Concave/Convergent vs Parallel/Divergent Implant Transmucosal Profiles on Hard and Soft Peri-Implant Tissues: A Systematic Review with Meta-Analyses. Int. J. Prosthodont. 2020, 33, 553–564. [Google Scholar] [CrossRef]
- Rompen, E.; Raepsaet, N.; Domken, O.; Touati, B.; Van Dooren, E. Soft Tissue Stability at the Facial Aspect of Gingivally Converging Abutments in the Esthetic Zone: A Pilot Clinical Study. J. Prosthet. Dent. 2007, 97, S119–S125. [Google Scholar] [CrossRef] [PubMed]
- Chien, H.H.; Schroering, R.L.; Prasad, H.S.; Tatakis, D.N. Effects of a New Implant Abutment Design on Peri-Implant Soft Tissues. J. Oral Implantol. 2014, 40, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.B.; Rheu, G.B.; Kim, Y.S.; Jeong, C.M.; Lee, J.Y.; Shin, S.W. Influence of Implant Transmucosal Design on Early Peri-Implant Tissue Responses in Beagle Dogs. Clin. Oral Implant. Res. 2014, 25, 962–968. [Google Scholar] [CrossRef] [PubMed]
- du Sert, N.P.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Iezzi, G.; Di Lillo, F.; Furlani, M.; Degidi, M.; Piattelli, A.; Giuliani, A. The Symmetric 3d Organization of Connective Tissue around Implant Abutment: A Key-Issue to Prevent Bone Resorption. Symmetry 2021, 13, 1126. [Google Scholar] [CrossRef]
- Boncompagni, S.; Rossi, A.E.; Micaroni, M.; Beznoussenko, G.V.; Polishchuk, R.S.; Dirksen, R.T.; Protasi, F. Mitochondria Are Linked to Calcium Stores in Striated Muscle by Developmentally Regulated Tethering Structures. Mol. Biol. Cell 2009, 20, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T.; Moon, I.S.; Lindhe, J. Peri-implant tissues at submerged and non-submerged titanium implants. J. Clin. Periodontol. 1999, 26, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J.; Ericsson, I.; Marinello, C.P.; Liljenberg, B.; Thomsen, P. The soft tissue barrier at implants andteeth. Clin. Oral Implant. Res. 1991, 2, 81–90. [Google Scholar] [CrossRef]
- Giuliani, A.; Cedola, A. Advanced High-Resolution Tomography in Regenerative Medicine; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- Ruggeri, A.; Franchi, M.; Trisi, P.; Piattelli, A. Histologic and Ultrastructural Findings of Gingival Circular Ligament Surrounding Osseointegrated Nonsubmerged Loaded Titanium Implants. Int. J. Oral Maxillofac. Implant. 1994, 9, 636–643. [Google Scholar]
- Bolle, C.; Gustin, M.-P.; Fau, D.; Boivin, G.; Exbrayat, P.; Grosgogeat, B. Soft Tissue and Marginal Bone Adaptation on Platform-Switched Implants with a Morse Cone Connection: A Histomorphometric Study in Dogs. Int. J. Periodontics Restor. Dent. 2016, 36, 221–228. [Google Scholar] [CrossRef]
- Tetè, S.; Mastrangelo, F.; Bianchi, A.; Zizzari, V.; Scarano, A. Collagen Fiber Orientation around Machined Titanium and Zirconia Dental Implant Necks: An Animal Study. Int. J. Oral Maxillofac. Implant. 2009, 24, 52–58. [Google Scholar]
- Mangano, C.; Piattelli, A.; Scarano, A.; Raspanti, M.; Shibli, J.; Mangano, F.; Perrotti, V.; Iezzi, G. A Light and Scanning Electron Microscopy Study of Human Direct Laser Metal Forming Dental Implants. Int. J. Periodontics Restor. Dent. 2014, 34, 9–17. [Google Scholar] [CrossRef]
- Romanos, G.E.; Traini, T.; Johansson, C.B.; Piattelli, A. Biologic Width and Morphologic Characteristics of Soft Tissues around Immediately Loaded Implants: Studies Performed on Human Autopsy Specimens. J. Periodontol. 2010, 81, 70–78. [Google Scholar] [CrossRef]
- Buehler, M.J. Nature Designs Tough Collagen: Explaining the Nanostructure of Collagen Fibrils. Proc. Natl. Acad. Sci. USA 2006, 103, 12285–12290. [Google Scholar] [CrossRef]
- Lin, J.; Shi, Y.; Men, Y.; Wang, X.; Ye, J.; Zhang, C. Mechanical Roles in Formation of Oriented Collagen Fibers. Tissue Eng. Part B Rev. 2020, 26, 116–128. [Google Scholar] [CrossRef]
- Casale, C.; Imparato, G.; Mazio, C.; Netti, P.A.; Urciuolo, F. Geometrical Confinement Controls Cell, ECM and Vascular Network Alignment during the Morphogenesis of 3D Bioengineered Human Connective Tissues. Acta Biomater. 2021, 131, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Sun, B. The Mechanics of Fibrillar Collagen Extracellular Matrix. Cell Rep. Phys. Sci. 2021, 2. [Google Scholar] [CrossRef]
- Schierano, G.; Ramieri, G.; Cortese, M.G.; Aimetti, M.; Preti, G. Organization of the Connective Tissue Barrier around Long-Term Loaded Implant Abutments in Man. Clin. Oral Implant. Res. 2002, 13, 460–464. [Google Scholar] [CrossRef]
- Birk, D.E.; Nurminskaya, M.V.; Zycband, E.I. Collagen Fibrillogenesis in Situ: Fibril Segments Undergo Post-Depositional Modifications Resulting in Linear and Lateral Growth during Matrix Development. Dev. Dyn. 1995, 202, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Mahadik, B.; Choi, J.Y.; Fisher, J.P. Vascularization in Tissue Engineering: Fundamentals and State-of-Art. Prog. Biomed. Eng. 2020, 2, 012002. [Google Scholar] [CrossRef]
- Saeidi, N.; Karmelek, K.P.; Paten, J.A.; Zareian, R.; DiMasi, E.; Ruberti, J.W. Molecular Crowding of Collagen: A Pathway to Produce Highly-Organized Collagenous Structures. Biomaterials 2012, 33, 7366–7374. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample 1 | Sample 2 | Sample 3 | Sample 4 | |
|---|---|---|---|---|
| CTRL | 18 ± 5 | 28 ± 3 | 8 ± 3 | 5 ± 1 |
| TEST | 47 * ± 11 | 46 * ± 6 | 63 * ± 10 | 43 * ± 19 |
| Sample 1 | Sample 2 | Sample 3 | Sample 4 | |
|---|---|---|---|---|
| CTRL | 4.2 ± 5.5 | 4.7 ± 4.4 | 2.6 ± 3.8 | 1.5 ± 1.3 |
| TEST | 20.7 ± 27.7 * | 7.5 ± 9.1 | 23.7 ± 12.6 * | 12.6 ± 16.6 * |
| Sample 1 | Sample 2 | Sample 3 | Sample 4 | |
|---|---|---|---|---|
| CTRL | 1.2 ± 0.3 | 0.9 ± 0.2 | 3.4 ± 0.4 | 1.7 ± 0.2 |
| TEST | 1.1 ± 0.2 | 0.8 ± 0.2 | 1.1 ± 0.3 * | 0.5 ± 0.2 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covani, U.; Giammarinaro, E.; Di Pietro, N.; Boncompagni, S.; Rastelli, G.; Romasco, T.; Velasco-Ortega, E.; Jimenez-Guerra, A.; Iezzi, G.; Piattelli, A.; et al. Electron Microscopy (EM) Analysis of Collagen Fibers in the Peri-Implant Soft Tissues around Two Different Abutments. J. Funct. Biomater. 2023, 14, 445. https://doi.org/10.3390/jfb14090445
Covani U, Giammarinaro E, Di Pietro N, Boncompagni S, Rastelli G, Romasco T, Velasco-Ortega E, Jimenez-Guerra A, Iezzi G, Piattelli A, et al. Electron Microscopy (EM) Analysis of Collagen Fibers in the Peri-Implant Soft Tissues around Two Different Abutments. Journal of Functional Biomaterials. 2023; 14(9):445. https://doi.org/10.3390/jfb14090445
Chicago/Turabian StyleCovani, Ugo, Enrica Giammarinaro, Natalia Di Pietro, Simona Boncompagni, Giorgia Rastelli, Tea Romasco, Eugenio Velasco-Ortega, Alvaro Jimenez-Guerra, Giovanna Iezzi, Adriano Piattelli, and et al. 2023. "Electron Microscopy (EM) Analysis of Collagen Fibers in the Peri-Implant Soft Tissues around Two Different Abutments" Journal of Functional Biomaterials 14, no. 9: 445. https://doi.org/10.3390/jfb14090445