
Magnesium-Based Temporary Implants: Potential, Current Status, Applications, and Challenges

Abstract
:1. Introduction
2. Desired Characteristics of Implants
- Similar Density and Young’s Modulus as Surrounding Tissues: Implants should have similar or comparable density and Young’s modulus as that of the surrounding tissues. Any significant differences will create stress concentrations leading to potential implant failure, inflammation, tissue damage, and bone loss. For example, the dental implant will experience excessive stress during chewing when it has a higher Young’s modulus than the surrounding bone. Hence, the careful selection of implant materials with comparable density, and Young’s modulus is crucial to ensure the proper and safe functioning of implants without stress field effects.
- Adequate mechanical strength: It is a crucial property for load bearing implants like orthopedic and dental implants, as they are designed to replace or augment bones or joints. In general, the implants are expected to be strong enough to withstand the forces and stresses that it will encounter within the body, without compromising its structural integrity. For example, the dental implants are specifically designed to handle mechanical loads from biting and chewing of foods. Normally, the mechanical strength requirements are specified in terms of tensile, compressive, or bending strength, and their typical values range from 50 to 2000 MPa for tensile strength, 100 to 2000 MPa for compressive strength, and 50 to 1000 MPa for bending strength.
- Corrosion resistant: It is particularly important for metallic implants that are in contact with body fluids as some metals tend to corrode upon exposure to body fluids like blood, plasma, or intestinal fluid, which may then lead to the loss of structural integrity, failure, toxicity, or other complications. Hence, it is essential to control the corrosion of permanent implants by choosing the right material that remains inert in body fluids (e.g., titanium or stainless steel) or by using protective coatings. The typical values for corrosion resistance for body implants range from 0.1 to 10 mpy (mils per year) as measured by corrosion tests such as ASTM F2129.
- Biocompatible: One of the major requirements for body implants is biocompatibility as incompatible implants can cause infection, inflammation, rejection, and other complications. Hence, the implant materials are specifically designed to coexist with the living tissues without causing any adverse reactions or immune response in the body. The biocompatibility of implants can be evaluated by test procedures like MTT (3-(4,5-dimethylthazolk-2-yl)-2,5-diphenyl tetrazolium bromide) assay, cell adhesion, cell proliferation, alkaline phosphatase (ALP) activity, and compatibility tests as per ISO 10993 [27].
- Radiopacity: This is the ability of the implant to be visible on medical imaging devices such as X-rays and CT scans. It is a crucial factor while selecting materials for implants as it enables easy detection on X-rays and accurate diagnosis for treatment planning.
- Ability to withstand sterilization: Implants must be sterilized before implantation to ensure that it is free from harmful microorganisms to prevent infections and other complications. Therefore, it is essential for implants to withstand sterilization methods such as autoclaving, gamma radiation, ethylene oxide gas, or other chemical treatments.
- Biodegradability and bioresorbable nature: Implants can also be designed to gradually break down and be absorbed by the body over time, as in the case of biodegradable implants, with the degradation products being either metabolized or excreted. Such implants can be made from materials that the body can absorb and integrate into surrounding tissue, e.g., synthetic or natural polymers, such as polylactic acid (PLA) or collagen. They offer potential advantages, such as reduced risk of complications and improved healing times, as well as a potential reduction to treatment cost.
3. Magnesium for Temporary Implants
- (i)
- Mechanical Properties
- Tensile strength: Magnesium-based materials have a lower tensile strength than titanium and stainless steel, but their strength-to-weight ratio is higher, which makes them an attractive option for lightweight implant applications. In this regard, it is also worth noting that the newly developed Mg alloys and composites have strength and ductility comfortably exceeding that of cortical bone.
- Elastic modulus: The elastic modulus of Mg alloys and composites is relatively low compared to titanium and stainless steel, which helps to minimize stress-shielding effects and prevent bone resorption that can occur with stiffer implant materials.
- Ductility: Magnesium alloys have relatively poor ductility compared to many metallic biomaterials, including titanium and stainless steel. For these reasons, novel Mg alloys are being developed with superior plastic deformation capabilities for load-bearing applications.
- Fatigue strength: The fatigue strength of magnesium-based materials is typically lower than that of titanium and stainless steel, which may limit their use in applications with higher cyclic loading.
- Corrosion resistance: While Mg has a lower corrosion resistance than titanium and stainless steel, its biodegradability can be an advantage in temporary implant applications. Similarly, compared to polymer and ceramic implant materials, Mg exhibits higher strength, better ductility, and a lower modulus of elasticity. These properties make Mg highly suitable for load-bearing applications.
- (ii)
- Biocompatibility
- Manganese and lithium are shown to be beneficial for anti-inflammatory properties.
- Reinforcement: Naturally occurring calcium phosphate mineral ceramics like tricalcium phosphate and hydroxyapatite have been used as reinforcement to develop Mg composites for biomedical applications. Being a major component of bone and teeth, they are biocompatible and well-tolerated by the human body. Similar benefits were also reported when synthetic silica-based bioglass ceramic was used as a reinforcement in Mg. Biodegradable polymers, such as polylactic acid (PLA) and polyglycolic acid (PGA), are also used as biodegradable reinforcements as they can be metabolized into lactic and glycolic acids that are naturally occurring in the body [38,39,40].
- (iii)
- Biodegradation
- (iv) Bioactivity and Apatite Formation
In Vitro/In Vivo Studies and Clinical Trials on Mg-Based Implants
4. Applications of Magnesium-Based Biodegradable Temporary Implants
5. Commercially Available Magnesium-Based Temporary Implants
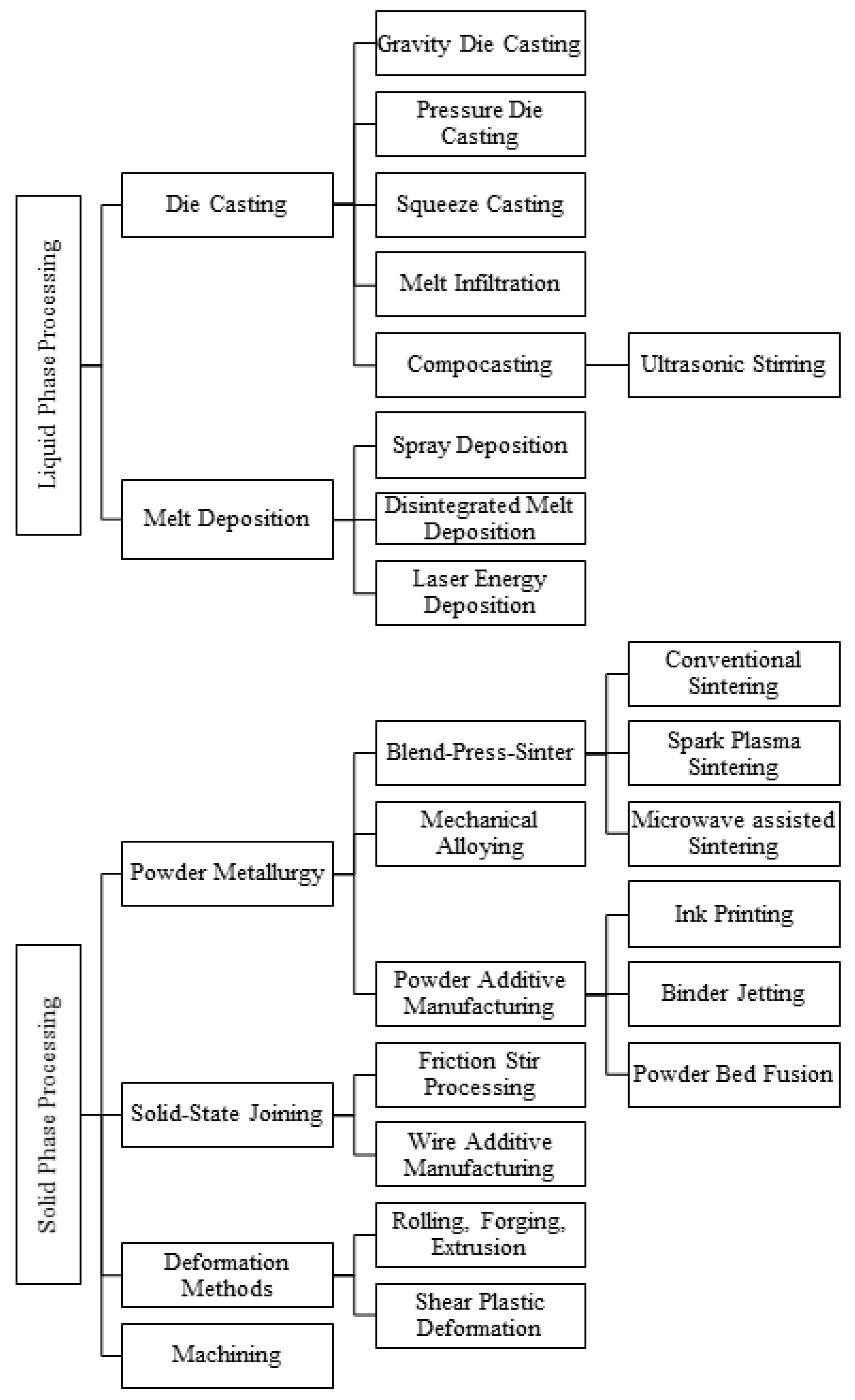
6. Fabrication Methods Applicable for Mg-Based Temporary Implants
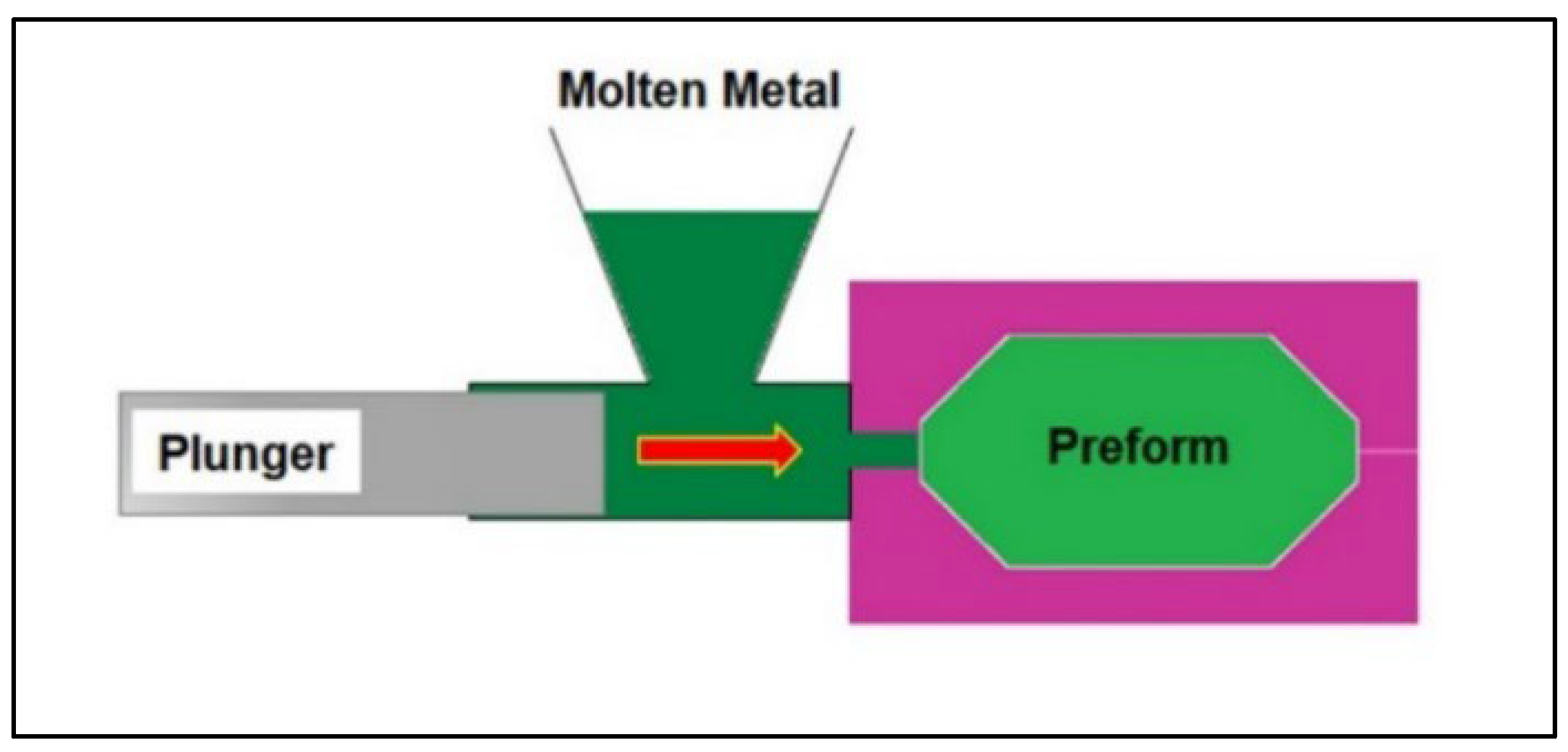
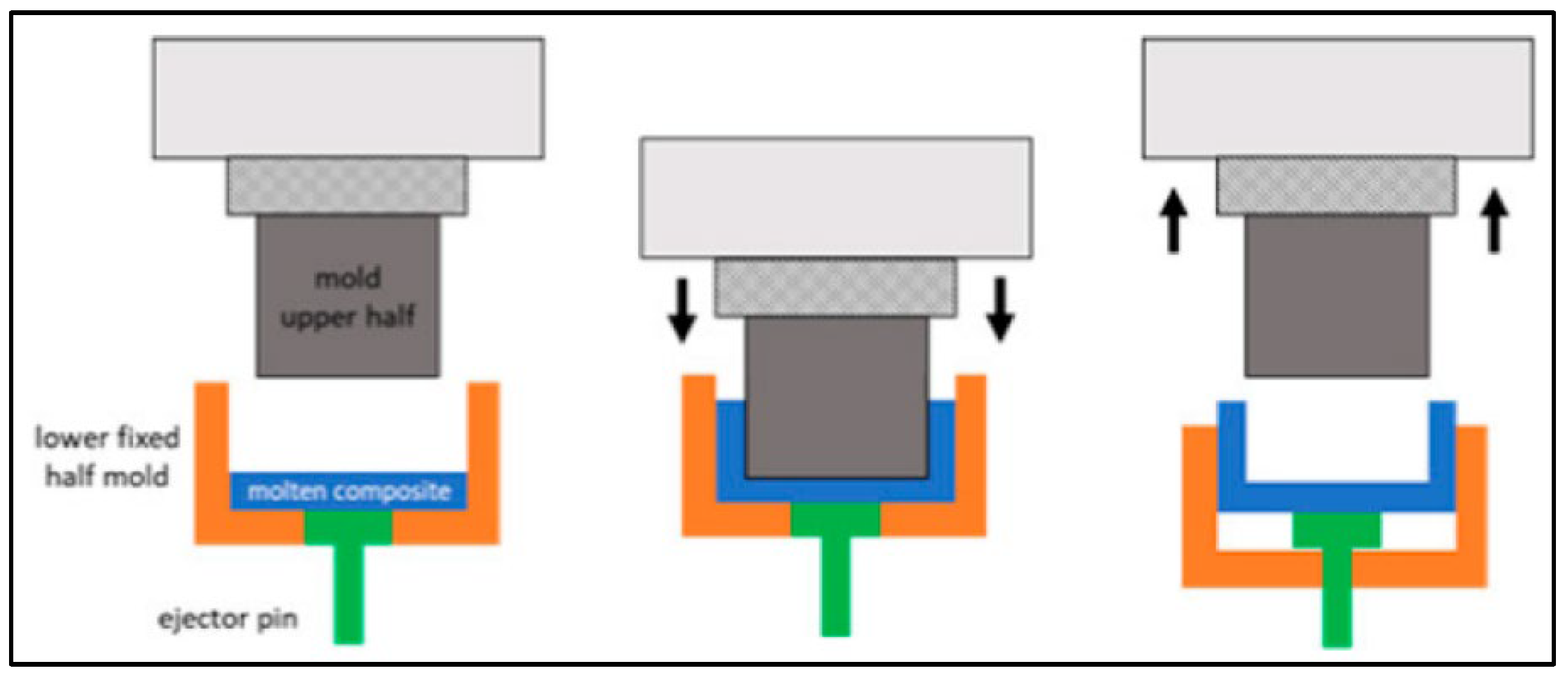
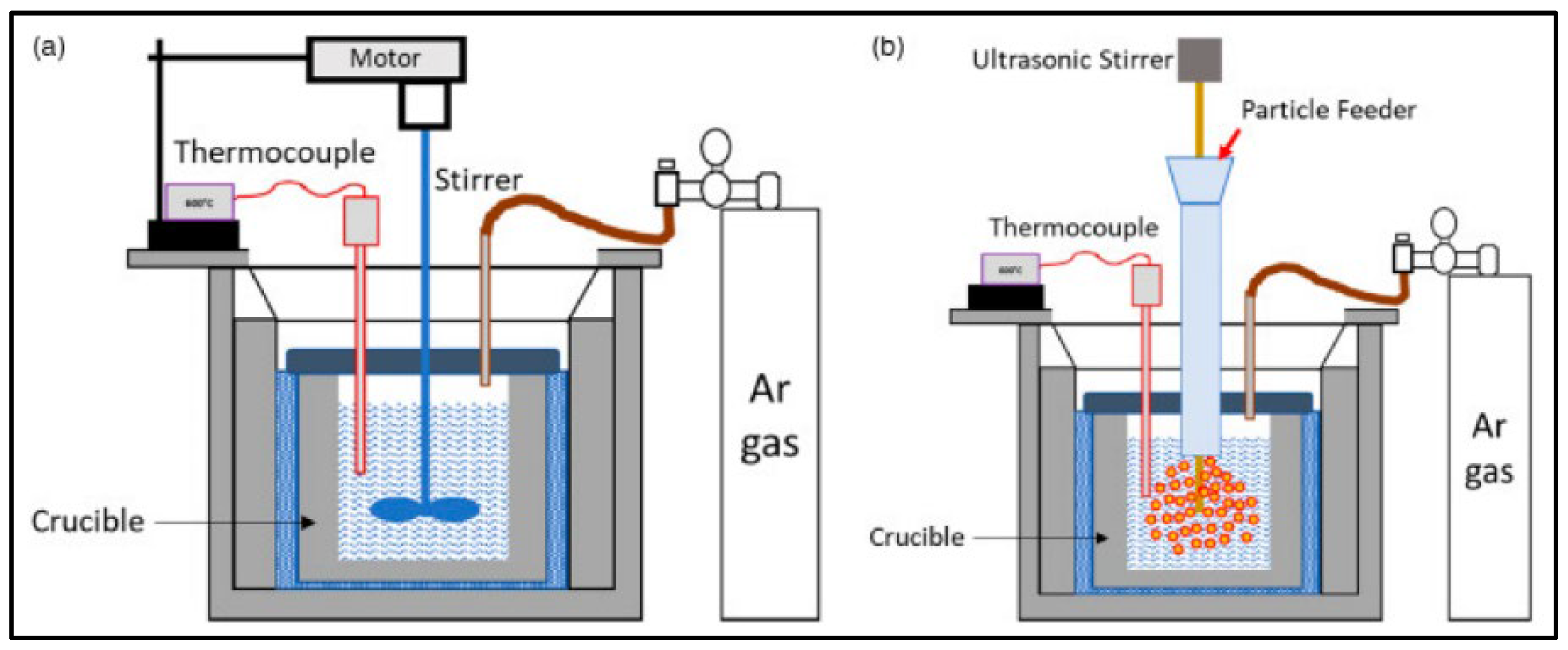
- (a)
- Die Casting
- (b)
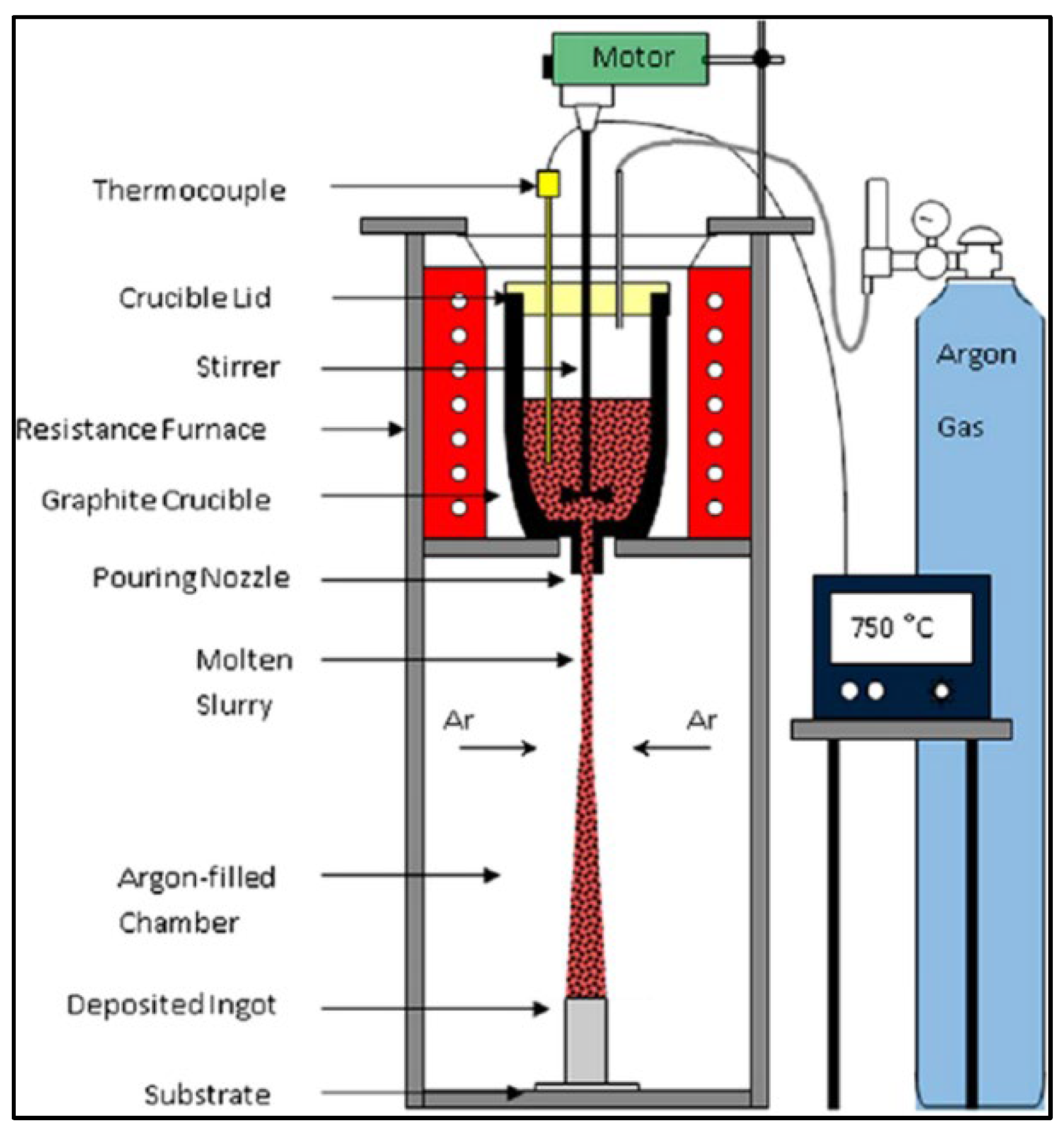
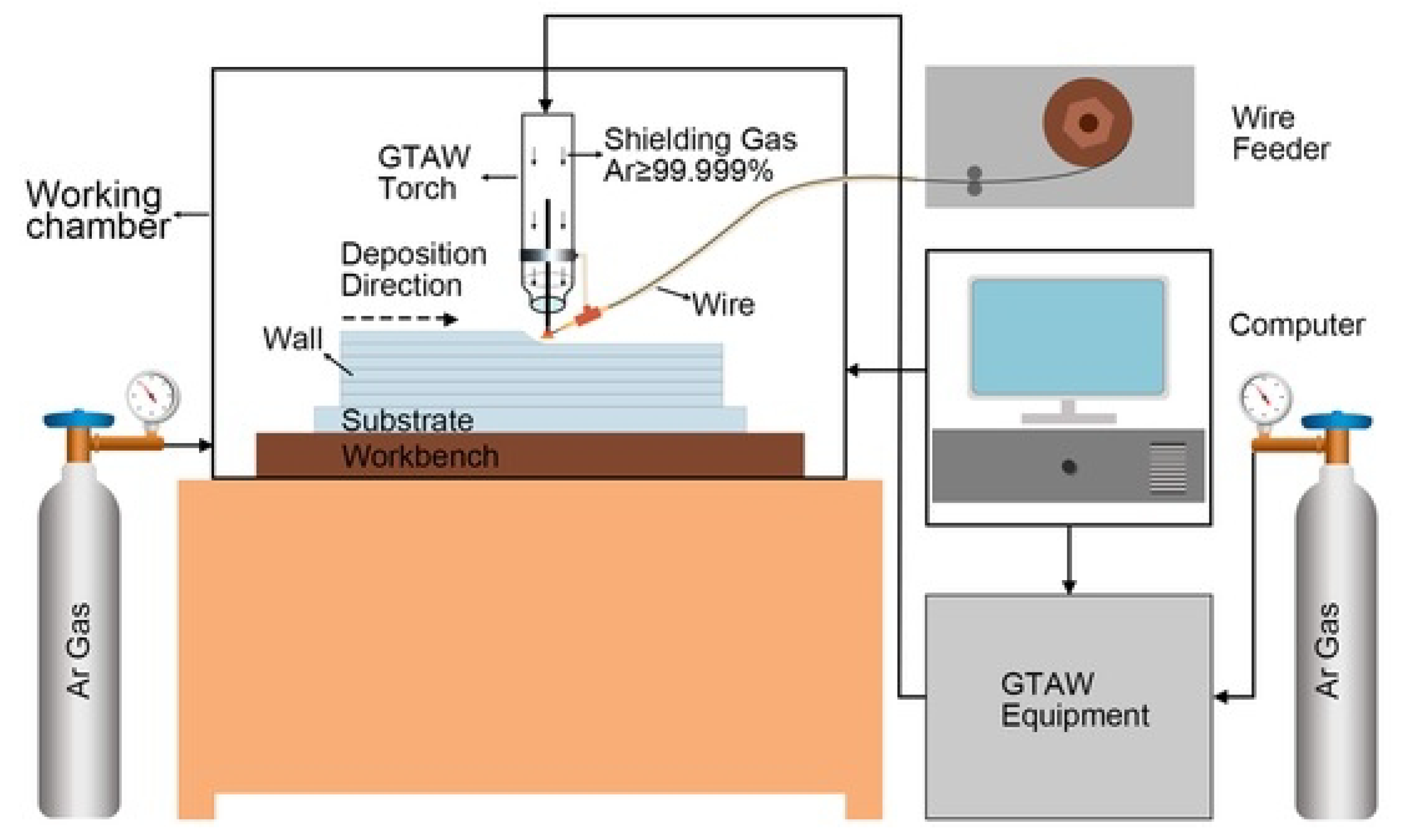
- Melt Deposition
- (c)
- Powder Metallurgy Methods
- (d)
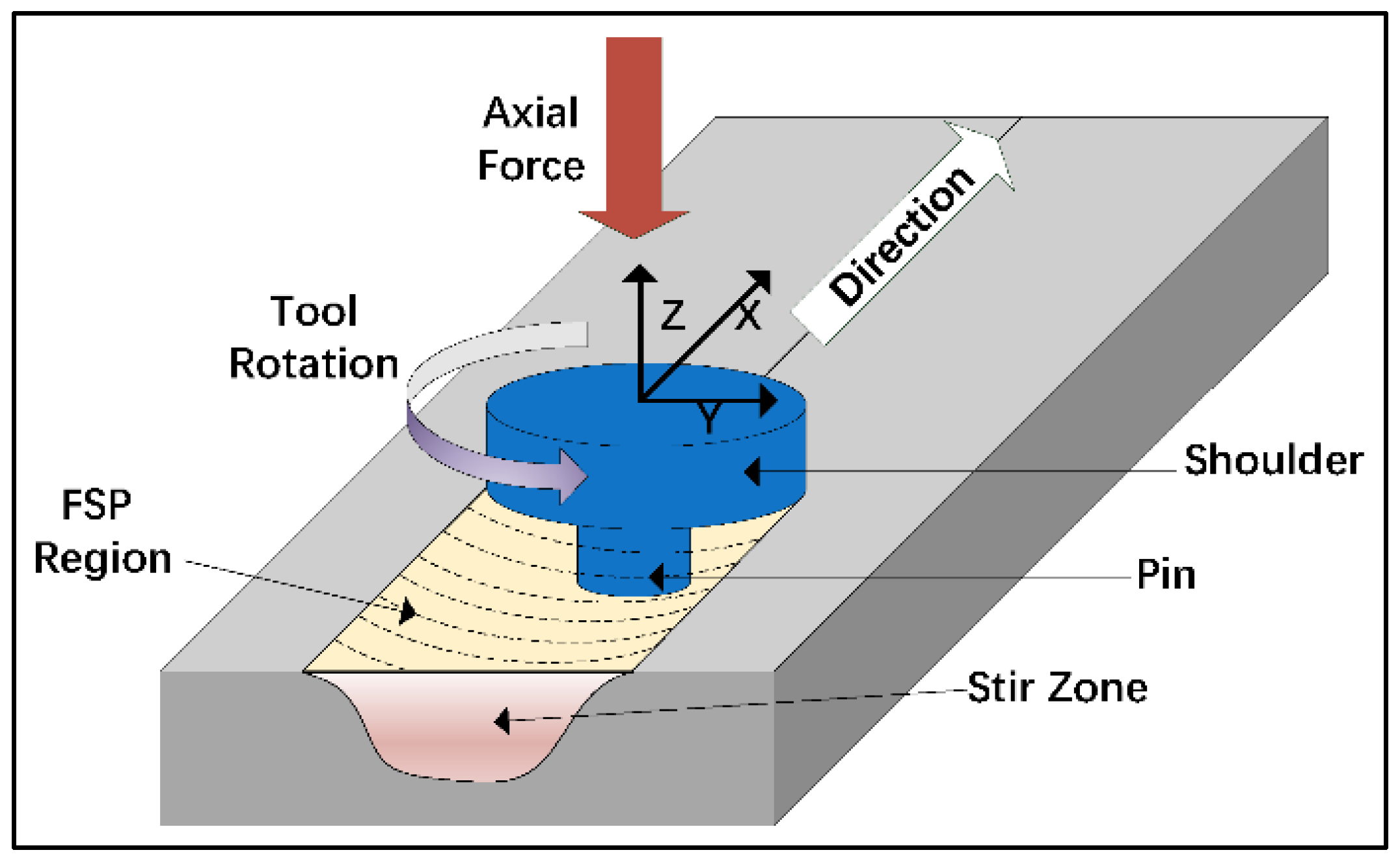
- Solid-State Joining Methods
- (e)
- Deformation Processing Methods Applicable to Magnesium Alloys
- (f)
- Machining of Magnesium
7. Current Challenges and Recommendations
- Rapid corrosion: It is the major challenge associated with Mg-based biodegradable implants. Being highly reactive, Mg corrodes rapidly in the presence of bodily fluids, making it difficult to control the degradation rate of the implant. Balancing the corrosion rate is crucial, as a high rate could lead to premature failure.
- Complex geometry of implants: The degradation behavior of Mg-based implants varies depending on the implant’s surface area-to-volume ratio and location in the body. Although controlling these variables can be challenging, it is necessary to ensure that the implant degrades in a controlled and safe manner.
- Inflammation due to corrosion products: While Mg is biocompatible, its degradation products can cause inflammation and tissue damage. Thus, developing better biocompatible magnesium-based materials is crucial to avoid negative side effects.
- Another key challenge associated with Mg implants is its susceptibility to stress corrosion cracking (SCC). In general, Mg implants can experience SCC when subjected to stress in a corrosive environment, leading to localized corrosion and cracking, resulting in premature failure. As the mechanism of SCC and its severity heavily depends on the alloy microstructure, incorporation of alloying elements (e.g., Al, Mn, and RE) and the control of grain size and texture are found to be beneficial in improving the resistance to SCC. Similarly, the application of protective coatings and surface treatments also act as barriers against corrosion to delay or prevent SCC. In this regard, the design of implants can also be optimized to reduce stress concentration and applied stress to reduce the risk of SCC.
- Enhance mechanical properties: Mg-based implants must have adequate mechanical properties to provide sufficient support and stability during the implantation period. Hence, novel Mg alloys with improved mechanical properties are required for the development of high-performance Mg-based implants.
- Improve corrosion resistance: Since Mg-based implants exhibit a faster degradation rate in body fluids, coatings are recommended to control the corrosion rate and hence improve the corrosion resistance of Mg-based implants.
- Optimize biodegradation rate: As biodegradation is an essential factor for the successful application of Mg-based implants, the use of alloying elements, grain size refinement, and surface treatments must be explored to control the biodegradation rate of Mg-based implants.
- Develop appropriate manufacturing techniques: Appropriate manufacturing techniques are essential for the development of Mg-based implants with controlled microstructure and mechanical properties. Researchers should explore different manufacturing techniques, such as additive manufacturing and powder metallurgy, to optimize the microstructure and mechanical properties of Mg-based implants.
- Conducting long-term clinical studies: Long-term studies should be conducted to evaluate the biodegradation rate, biocompatibility, and mechanical stability of Mg-based implants over extended periods. This will help to boost the confidence on Mg-based temporary implants over permanent implants.
- Standardizing test protocols: The testing protocols for Mg implants must be standardized to assess key aspects such as biodegradation rate, biocompatibility, and mechanical properties.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gotman, I. Characteristics of Metals Used in Implants. J. Endourol. 1997, 11, 383–389. [Google Scholar] [CrossRef]
- Batchelor, A.W.; Chandrasekaran, M. Service Characteristics of Biomedical Materials and Implants; Imperial College Press: London, UK, 2004; Volume 3, ISBN 1860945368. [Google Scholar]
- Park, J.B.; Bronzino, J.D. Biomaterials: Principles and Applications; CRC: Boca Raton, FL, USA, 2002. [Google Scholar]
- Park, J.; Lakes, R.S. Biomaterials: An Introduction; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2007; ISBN 0387378804. [Google Scholar]
- Kaplan, E.G.; Kaplan, G.S.; Kaplan, D.M.; Kaplan, R.K. History of Implants. Clin. Podiatry 1984, 1, 3–10. [Google Scholar] [PubMed]
- Witte, F. The History of Biodegradable Magnesium Implants: A Review. Acta Biomater. 2010, 6, 1680–1692. [Google Scholar] [CrossRef]
- Prakasam, M.; Locs, J.; Salma-Ancane, K.; Loca, D.; Largeteau, A.; Berzina-Cimdina, L. Biodegradable Materials and Metallic Implants-A Review. J. Funct. Biomater. 2017, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, J.S.; Richards, R.G. The Use of Titanium and Stainless Steel in Fracture Fixation. Expert Rev. Med. Devices 2010, 7, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Bairagi, D.; Mandal, S. A Comprehensive Review on Biocompatible Mg-Based Alloys as Temporary Orthopaedic Implants: Current Status, Challenges, and Future Prospects. J. Magnes. Alloy. 2022, 10, 627–669. [Google Scholar] [CrossRef]
- Zhou, H.; Liang, B.; Jiang, H.; Deng, Z.; Yu, K. Magnesium-Based Biomaterials as Emerging Agents for Bone Repair and Regeneration: From Mechanism to Application. J. Magnes. Alloy. 2021, 9, 779–804. [Google Scholar] [CrossRef]
- Staiger, M.P.; Pietak, A.M.; Huadmai, J.; Dias, G. Magnesium and Its Alloys as Orthopedic Biomaterials: A Review. Biomaterials 2006, 27, 1728–1734. [Google Scholar] [CrossRef]
- Savio, D.; Bagno, A. When the Total Hip Replacement Fails: A Review on the Stress-Shielding Effect. Processes 2022, 10, 612. [Google Scholar] [CrossRef]
- Sumner, D.R. Long-Term Implant Fixation and Stress-Shielding in Total Hip Replacement. J. Biomech. 2015, 48, 797–800. [Google Scholar] [CrossRef]
- Chakraborty Banerjee, P.; Al-Saadi, S.; Choudhary, L.; Harandi, S.E.; Singh, R. Magnesium Implants: Prospects and Challenges. Materials 2019, 12, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Liu, X.; Wu, S.; Yeung, K.W.K.; Zheng, Y.; Chu, P.K. Design of Magnesium Alloys with Controllable Degradation for Biomedical Implants: From Bulk to Surface. Acta Biomater. 2016, 45, 2–30. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, Y.; Wang, Y.L.; Tian, Y.Q.; Chen, L.S. Research Progress on Surface Protective Coatings of Biomedical Degradable Magnesium Alloys. J. Alloys Compd. 2021, 885, 161001. [Google Scholar] [CrossRef]
- Agarwal, S.; Curtin, J.; Duffy, B.; Jaiswal, S. Biodegradable Magnesium Alloys for Orthopaedic Applications: A Review on Corrosion, Biocompatibility and Surface Modifications. Mater. Sci. Eng. C 2016, 68, 948–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Zhang, M.; Li, Y.; Zhao, J.; Qin, L.; Lai, Y. Corrosion and Biocompatibility Improvement of Magnesium-Based Alloys as Bone Implant Materials: A Review. Regen. Biomater. 2017, 4, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Xing, F.; Li, S.; Yin, D.; Xie, J.; Rommens, P.M.; Xiang, Z.; Liu, M.; Ritz, U. Recent Progress in Mg-Based Alloys as a Novel Bioabsorbable Biomaterials for Orthopedic Applications. J. Magnes. Alloy. 2022, 10, 1428–1456. [Google Scholar] [CrossRef]
- Gutiérrez Púa, L.D.C.; Rincón Montenegro, J.C.; Fonseca Reyes, A.M.; Zambrano Rodríguez, H.; Paredes Méndez, V.N. Biomaterials for Orthopedic Applications and Techniques to Improve Corrosion Resistance and Mechanical Properties for Magnesium Alloy: A Review. J. Mater. Sci. 2023, 58, 3879–3908. [Google Scholar] [CrossRef]
- Nasr Azadani, M.; Zahedi, A.; Bowoto, O.K.; Oladapo, B.I. A Review of Current Challenges and Prospects of Magnesium and Its Alloy for Bone Implant Applications. Prog. Biomater. 2022, 11, 1–26. [Google Scholar] [CrossRef]
- Tipan, N.; Pandey, A.; Mishra, P. Selection and Preparation Strategies of Mg-Alloys and Other Biodegradable Materials for Orthopaedic Applications: A Review. Mater. Today Commun. 2022, 31, 103658. [Google Scholar] [CrossRef]
- Zaman, H.A.; Sharif, S.; Idris, M.H.; Kamarudin, A. Metallic Biomaterials for Medical Implant Applications: A Review. Appl. Mech. Mater. 2015, 735, 19–25. [Google Scholar] [CrossRef]
- Tathe, A.; Ghodke, M.; Nikalje, A.P. A Brief Review: Biomaterials and Their Application. Int. J. Pharm. Pharm. Sci. 2010, 2, 19–23. [Google Scholar]
- Von Recum, A.F.; Jacobi, J.E. Handbook of Biomaterials Evaluation: Scientific, Technical and Clinical Testing of Implant Materials; CRC Press: Boca Raton, FL, USA, 1998; ISBN 1560324791. [Google Scholar]
- Bonfante, E.A.; Coelho, P.G. A Critical Perspective on Mechanical Testing of Implants and Prostheses. Adv. Dent. Res. 2016, 28, 18–27. [Google Scholar] [CrossRef]
- Ratner, B.D. The Biocompatibility of Implant Materials. In Host Response to Biomaterials; Elsevier: Amsterdam, The Netherlands, 2015; pp. 37–51. [Google Scholar]
- Hofmann, G.O. Biodegradable Implants in Traumatology: A Review on the State-of-the-Art. Arch. Orthop. Trauma Surg. 1995, 114, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Ortiz, O.; Goyal, R.; Kohn, J. Biodegradable Polymers. Handb. Polym. Appl. Med. Med. Devices 2014, 13, 303–335. [Google Scholar]
- Vainionpää, S.; Rokkanen, P.; Törmälä, P. Surgical Applications of Biodegradable Polymers in Human Tissues. Prog. Polym. Sci. 1989, 14, 679–716. [Google Scholar] [CrossRef]
- Tsakiris, V.; Tardei, C.; Clicinschi, F.M. Biodegradable Mg Alloys for Orthopedic Implants—A Review. J. Magnes. Alloy. 2021, 9, 1884–1905. [Google Scholar] [CrossRef]
- Zan, R.; Shen, S.; Huang, Y.; Yu, H.; Liu, Y.; Yang, S.; Zheng, B.; Gong, Z.; Wang, W.; Zhang, X.; et al. Research Hotspots and Trends of Biodegradable Magnesium and Its Alloys. Smart Mater. Med. 2023, 4, 468–479. [Google Scholar] [CrossRef]
- Czerwinski, F. Magnesium Alloys: Design, Processing and Properties; BoD–Books on Demand: Norderstedt, Germany, 2011; ISBN 9533075201. [Google Scholar]
- Avedesian, M.M.; Baker, H. ASM Specialty Handbook: Magnesium and Magnesium Alloys; ASM International: Almere, The Netherlands, 1999; ISBN 0871706571. [Google Scholar]
- Hassan, S.F.; Islam, M.T.; Saheb, N.; Baig, M.M.A. Magnesium for Implants: A Review on the Effect of Alloying Elements on Biocompatibility and Properties. Materials 2022, 15, 5669. [Google Scholar] [CrossRef]
- Ding, Y.; Wen, C.; Hodgson, P.; Li, Y. Effects of Alloying Elements on the Corrosion Behavior and Biocompatibility of Biodegradable Magnesium Alloys: A Review. J. Mater. Chem. B 2014, 2, 1912–1933. [Google Scholar] [CrossRef]
- Kumar, R.; Katyal, P. Effects of Alloying Elements on Performance of Biodegradable Magnesium Alloy. Mater. Today Proc. 2022, 56, 2443–2450. [Google Scholar] [CrossRef]
- Bommala, V.K.; Krishna, M.G.; Rao, C.T. Magnesium Matrix Composites for Biomedical Applications: A Review. J. Magnes. Alloy. 2019, 7, 72–79. [Google Scholar] [CrossRef]
- Jhamb, S.; Matai, J.; Marwaha, J.; Goyal, A.; Pandey, A. A Comprehensive Analysis on Magnesium-Based Alloys and Metal Matrix Composites for Their in-Vitro Biocompatibility. Adv. Mater. Process. Technol. 2022, 44, 1–34. [Google Scholar] [CrossRef]
- Kumar, K.; Das, A.; Prasad, S.B. Recent Developments in Biodegradable Magnesium Matrix Composites for Orthopaedic Applications: A Review Based on Biodegradability, Mechanical and Biocompatibility Perspective. Mater. Today Proc. 2021, 44, 2038–2042. [Google Scholar] [CrossRef]
- Kasaeian-Naeini, M.; Sedighi, M.; Hashemi, R. Severe Plastic Deformation (SPD) of Biodegradable Magnesium Alloys and Composites: A Review of Developments and Prospects. J. Magnes. Alloy. 2022, 10, 938–955. [Google Scholar] [CrossRef]
- Shaikh, S.; Qayoom, I.; Sarvesha, R.; Kumar, A. Bioresorbable Magnesium-Based Alloys Containing Strontium Doped Nanohydroxyapatite Promotes Bone Healing in Critical Sized Bone Defect in Rat Femur Shaft. J. Magnes. Alloy. 2023, 11, 270–286. [Google Scholar] [CrossRef]
- Shahin, M.; Munir, K.; Wen, C.; Li, Y. Magnesium Matrix Nanocomposites for Orthopedic Applications: A Review from Mechanical, Corrosion, and Biological Perspectives. Acta Biomater. 2019, 96, 1–19. [Google Scholar] [CrossRef]
- Seetharaman, S.; Tekumalla, S.; Gupta, M. Magnesium-Based Nanocomposites: Advances and Applications; IOP Publishing: Bristol, UK, 2020; ISBN 0750335351. [Google Scholar]
- Song, X.; Bayati, P.; Gupta, M.; Elahinia, M.; Haghshenas, M. Fracture of Magnesium Matrix Nanocomposites—A Review. Int. J. Lightweight Mater. Manuf. 2021, 4, 67–98. [Google Scholar] [CrossRef]
- Alexander, M. Biodegradation and Bioremediation; Gulf Professional Publishing: Houston, TX, USA, 1999; ISBN 0120498618. [Google Scholar]
- Mozafari, M.; Bordbar-Khiabani, A.; Yarmand, B. Emerging Magnesium-Based Biomaterials for Orthopedic Implantation. Emerg. Mater. Res. 2020, 8, 305–319. [Google Scholar] [CrossRef] [Green Version]
- Sezer, N.; Evis, Z.; Kayhan, S.M.; Tahmasebifar, A.; Koç, M. Review of Magnesium-Based Biomaterials and Their Applications. J. Magnes. Alloy. 2018, 6, 23–43. [Google Scholar] [CrossRef]
- Zhang, A.M.; Lenin, P.; Zeng, R.C.; Kannan, M.B. Advances in Hydroxyapatite Coatings on Biodegradable Magnesium and Its Alloys. J. Magnes. Alloy. 2022, 10, 1154–1170. [Google Scholar] [CrossRef]
- Shadanbaz, S.; Dias, G.J. Calcium Phosphate Coatings on Magnesium Alloys for Biomedical Applications: A Review. Acta Biomater. 2012, 8, 20–30. [Google Scholar] [CrossRef]
- Chalisgaonkar, R. Insight in Applications, Manufacturing and Corrosion Behaviour of Magnesium and Its Alloys—A Review. Mater. Today Proc. 2020, 26, 1060–1071. [Google Scholar] [CrossRef]
- Nguyen, T.L.; Blanquet, A.; Staiger, M.P.; Dias, G.J.; Woodfield, T.B.F. On the Role of Surface Roughness in the Corrosion of Pure Magnesium In Vitro. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.L.; Liu, Y.; Song, X.Y. Plasma-Sprayed Hydroxyapatite Coating for Improved Corrosion Resistance and Bioactivity of Magnesium Alloy. J. Therm. Spray Technol. 2018, 27, 1381–1387. [Google Scholar] [CrossRef]
- Song, G.L. Control of Degradation of Biocompatible Magnesium in a Pseudo-Physiological Environment by a Ceramic like Anodized Coating. In Advanced Materials Research; Trans Tech Publ: Stafa-Zurich, Switzerland, 2007; Volume 29, pp. 95–98. [Google Scholar]
- Stürznickel, J.; Delsmann, M.M.; Jungesblut, O.D.; Stücker, R.; Knorr, C.; Rolvien, T.; Kertai, M.; Rupprecht, M. Safety and Performance of Biodegradable Magnesium-Based Implants in Children and Adolescents. Injury 2021, 52, 2265–2271. [Google Scholar] [CrossRef]
- Espiritu, J.; Meier, M.; Seitz, J.M. The Current Performance of Biodegradable Magnesium-Based Implants in Magnetic Resonance Imaging: A Review. Bioact Mater. 2021, 6, 4360–4367. [Google Scholar] [CrossRef]
- Jana, A.; Das, M.; Balla, V.K. In Vitro and In Vivo Degradation Assessment and Preventive Measures of Biodegradable Mg Alloys for Biomedical Applications. J. Biomed. Mater. Res. A 2022, 110, 462–487. [Google Scholar] [CrossRef] [PubMed]
- Gray-Munro, J.E.; Seguin, C.; Strong, M. Influence of Surface Modification on the In Vitro Corrosion Rate of Magnesium Alloy AZ31. J. Biomed. Mater. Res. Part A Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2009, 91, 221–230. [Google Scholar]
- Wang, Y.; Zhu, Z.; Xu, X.; He, Y.; Zhang, B. Improved Corrosion Resistance and Biocompatibility of a Calcium Phosphate Coating on a Magnesium Alloy for Orthopedic Applications. Eur. J. Inflamm. 2016, 14, 169–183. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Gu, X.; Lou, S.; Zheng, Y. The Development of Binary Mg–Ca Alloys for Use as Biodegradable Materials within Bone. Biomaterials 2008, 29, 1329–1344. [Google Scholar] [CrossRef]
- Zhang, E.; Yin, D.; Xu, L.; Yang, L.; Yang, K. Microstructure, Mechanical and Corrosion Properties and Biocompatibility of Mg–Zn–Mn Alloys for Biomedical Application. Mater. Sci. Eng. C 2009, 29, 987–993. [Google Scholar] [CrossRef]
- Gu, X.; Zheng, Y.; Cheng, Y.; Zhong, S.; Xi, T. In Vitro Corrosion and Biocompatibility of Binary Magnesium Alloys. Biomaterials 2009, 30, 484–498. [Google Scholar] [CrossRef]
- Chen, Y.; Yan, J.; Zhao, C.; Zhang, S.; Yu, S.; Wang, Z.; Wang, X.; Zhang, X.; Zheng, Q. In Vitro and In Vivo Assessment of the Biocompatibility of an Mg–6Zn Alloy in the Bile. J. Mater. Sci. Mater. Med. 2014, 25, 471–480. [Google Scholar] [CrossRef]
- Gu, X.N.; Xie, X.H.; Li, N.; Zheng, Y.F.; Qin, L. In Vitro and In Vivo Studies on a Mg–Sr Binary Alloy System Developed as a New Kind of Biodegradable Metal. Acta Biomater. 2012, 8, 2360–2374. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, M.E.; Aslani, A.; Liu, H. The Effects of Nanostructured Hydroxyapatite Coating on the Biodegradation and Cytocompatibility of Magnesium Implants. J. Biomed. Mater. Res. A 2013, 101A, 2340–2354. [Google Scholar] [CrossRef]
- Abdal-hay, A.; Barakat, N.A.M.; Lim, J.K. Hydroxyapatite-Doped Poly(Lactic Acid) Porous Film Coating for Enhanced Bioactivity and Corrosion Behavior of AZ31 Mg Alloy for Orthopedic Applications. Ceram. Int. 2013, 39, 183–195. [Google Scholar] [CrossRef]
- Nishita, M.; Park, S.-Y.; Nishio, T.; Kamizaki, K.; Wang, Z.; Tamada, K.; Takumi, T.; Hashimoto, R.; Otani, H.; Pazour, G.J.; et al. Ror2 Signaling Regulates Golgi Structure and Transport through IFT20 for Tumor Invasiveness. Sci. Rep. 2017, 7, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavitha, R.J.; Ravichandran, K.; Sankara Narayanan, T.S.N. Deposition of Strontium Phosphate Coatings on Magnesium by Hydrothermal Treatment: Characteristics, Corrosion Resistance and Bioactivity. J. Alloys Compd. 2018, 745, 725–743. [Google Scholar] [CrossRef]
- Li, J.; Han, P.; Ji, W.; Song, Y.; Zhang, S.; Chen, Y.; Zhao, C.; Zhang, F.; Zhang, X.; Jiang, Y. The In Vitro Indirect Cytotoxicity Test and In Vivo Interface Bioactivity Evaluation of Biodegradable FHA Coated Mg–Zn Alloys. Mater. Sci. Eng. B 2011, 176, 1785–1788. [Google Scholar] [CrossRef]
- Mao, L.; Shen, L.; Chen, J.; Wu, Y.; Kwak, M.; Lu, Y.; Xue, Q.; Pei, J.; Zhang, L.; Yuan, G.; et al. Enhanced Bioactivity of Mg–Nd–Zn–Zr Alloy Achieved with Nanoscale MgF2 Surface for Vascular Stent Application. ACS Appl. Mater. Interfaces 2015, 7, 5320–5330. [Google Scholar] [CrossRef]
- Lock, J.Y.; Wyatt, E.; Upadhyayula, S.; Whall, A.; Nuñez, V.; Vullev, V.I.; Liu, H. Degradation and Antibacterial Properties of Magnesium Alloys in Artificial Urine for Potential Resorbable Ureteral Stent Applications. J. Biomed. Mater. Res. A 2014, 102, 781–792. [Google Scholar] [CrossRef]
- Liu, Z.; Schade, R.; Luthringer, B.; Hort, N.; Rothe, H.; Müller, S.; Liefeith, K.; Willumeit-Römer, R.; Feyerabend, F. Influence of the Microstructure and Silver Content on Degradation, Cytocompatibility, and Antibacterial Properties of Magnesium-Silver Alloys In Vitro. Oxid. Med. Cell Longev. 2017, 2017, 8091265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, H.; Zhao, Y.; An, Z.; Cheng, M.; Wang, Q.; Cheng, T.; Wang, Q.; Wang, J.; Jiang, Y.; Zhang, X.; et al. Enhanced Antibacterial Properties, Biocompatibility, and Corrosion Resistance of Degradable Mg-Nd-Zn-Zr Alloy. Biomaterials 2015, 53, 211–220. [Google Scholar] [CrossRef]
- Chen, J.; Peng, W.; Zhu, L.; Tan, L.; Etim, I.P.; Wang, X.; Yang, K. Effect of Copper Content on the Corrosion Behaviors and Antibacterial Properties of Binary Mg–Cu Alloys. Mater. Technol. 2018, 33, 145–152. [Google Scholar] [CrossRef]
- Song, Y.; Shan, D.; Chen, R.; Zhang, F.; Han, E.-H. Biodegradable Behaviors of AZ31 Magnesium Alloy in Simulated Body Fluid. Mater. Sci. Eng. C 2009, 29, 1039–1045. [Google Scholar] [CrossRef]
- Liu, M.; Wang, J.; Zhu, S.; Zhang, Y.; Sun, Y.; Wang, L.; Guan, S. Corrosion Fatigue of the Extruded Mg–Zn–Y–Nd Alloy in Simulated Body Fluid. J. Magnes. Alloy. 2020, 8, 231–240. [Google Scholar] [CrossRef]
- Reza Kashyzadeh, K.; Amiri, N.; Maleki, E.; Unal, O. A Critical Review on Improving the Fatigue Life and Corrosion Properties of Magnesium Alloys via the Technique of Adding Different Elements. J. Mar. Sci. Eng. 2023, 11, 527. [Google Scholar] [CrossRef]
- Nascimento, L.; Yi, S.; Bohlen, J.; Fuskova, L.; Letzig, D.; Kainer, K.U. High Cycle Fatigue Behaviour of Magnesium Alloys. Procedia Eng. 2010, 2, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Bowen, P.K.; Drelich, J.; Goldman, J. Magnesium in the Murine Artery: Probing the Products of Corrosion. Acta Biomater. 2014, 10, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Bowen, P.K.; Drelich, J.; Goldman, J. A New In Vitro-In Vivo Correlation for Bioabsorbable Magnesium Stents from Mechanical Behavior. Mater. Sci. Eng. C 2013, 33, 5064–5070. [Google Scholar] [CrossRef] [PubMed]
- Bowen, P.K.; Gelbaugh, J.A.; Mercier, P.J.; Goldman, J.; Drelich, J. Tensile Testing as a Novel Method for Quantitatively Evaluating Bioabsorbable Material Degradation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 2101–2113. [Google Scholar] [CrossRef] [PubMed]
- Witte, F.; Kaese, V.; Haferkamp, H.; Switzer, E.; Meyer-Lindenberg, A.; Wirth, C.J.; Windhagen, H. In Vivo Corrosion of Four Magnesium Alloys and the Associated Bone Response. Biomaterials 2005, 26, 3557–3563. [Google Scholar] [CrossRef]
- Waksman, R.; Pakala, R.; Kuchulakanti, P.K.; Baffour, R.; Hellinga, D.; Seabron, R.; Tio, F.O.; Wittchow, E.; Hartwig, S.; Harder, C. Safety and Efficacy of Bioabsorbable Magnesium Alloy Stents in Porcine Coronary Arteries. Catheter. Cardiovasc. Interv. 2006, 68, 607–617. [Google Scholar] [CrossRef]
- Witte, F.; Fischer, J.; Nellesen, J.; Vogt, C.; Vogt, J.; Donath, T.; Beckmann, F. In Vivo Corrosion and Corrosion Protection of Magnesium Alloy LAE442. Acta Biomater. 2010, 6, 1792–1799. [Google Scholar] [CrossRef]
- Wang, Y.; He, Y.; Zhu, Z.; Jiang, Y.; Zhang, J.; Niu, J.; Mao, L.; Yuan, G. In Vitro Degradation and Biocompatibility of Mg-Nd-Zn-Zr Alloy. Chin. Sci. Bull. 2012, 57, 2163–2170. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Shimizu, Y.; Odashima, K.; Sano, Y.; Yamamoto, A.; Mukai, T.; Ikeo, N.; Takahashi, T.; Kumamoto, H. In Vitro and In Vivo Analysis of the Biodegradable Behavior of a Magnesium Alloy for Biomedical Applications. Dent. Mater. J. 2019, 38, 11–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratna Sunil, B.; Sampath Kumar, T.S.; Chakkingal, U.; Nandakumar, V.; Doble, M.; Devi Prasad, V.; Raghunath, M. In Vitro and In Vivo Studies of Biodegradable Fine Grained AZ31 Magnesium Alloy Produced by Equal Channel Angular Pressing. Mater. Sci. Eng. C 2016, 59, 356–367. [Google Scholar] [CrossRef]
- Dziuba, D.; Meyer-Lindenberg, A.; Seitz, J.M.; Waizy, H.; Angrisani, N.; Reifenrath, J. Long-Term In Vivo Degradation Behaviour and Biocompatibility of the Magnesium Alloy ZEK100 for Use as a Biodegradable Bone Implant. Acta Biomater. 2013, 9, 8548–8560. [Google Scholar] [CrossRef]
- Makkar, P.; Sarkar, S.K.; Padalhin, A.R.; Moon, B.-G.; Lee, Y.S.; Lee, B.T. In Vitro and In Vivo Assessment of Biomedical Mg–Ca Alloys for Bone Implant Applications. J. Appl. Biomater. Funct. Mater. 2018, 16, 126–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, D.; Zhou, W.; Liu, Y.; Li, N.; Zheng, Y.; Sun, Z. Fatigue Behaviors of HP-Mg, Mg–Ca and Mg–Zn–Ca Biodegradable Metals in Air and Simulated Body Fluid. Acta Biomater. 2016, 41, 351–360. [Google Scholar] [CrossRef]
- Zhao, D.; Witte, F.; Lu, F.; Wang, J.; Li, J.; Qin, L. Current Status on Clinical Applications of Magnesium-Based Orthopaedic Implants: A Review from Clinical Translational Perspective. Biomaterials 2017, 112, 287–302. [Google Scholar] [CrossRef]
- Feyerabend, F.; Fischer, J.; Holtz, J.; Witte, F.; Willumeit, R.; Drücker, H.; Vogt, C.; Hort, N. Evaluation of Short-Term Effects of Rare Earth and Other Elements Used in Magnesium Alloys on Primary Cells and Cell Lines. Acta Biomater. 2010, 6, 1834–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.-N.; Zheng, Y.-F. A Review on Magnesium Alloys as Biodegradable Materials. Front. Mater. Sci. China 2010, 4, 111–115. [Google Scholar] [CrossRef]
- Mao, L.; Zhou, H.; Chen, L.; Niu, J.; Zhang, L.; Yuan, G.; Song, C. Enhanced Biocompatibility and Long-Term Durability In Vivo of Mg-Nd-Zn-Zr Alloy for Vascular Stent Application. J. Alloys Compd. 2017, 720, 245–253. [Google Scholar] [CrossRef]
- Mao, L.; Shen, L.; Niu, J.; Zhang, J.; Ding, W.; Wu, Y.; Fan, R.; Yuan, G. Nanophasic Biodegradation Enhances the Durability and Biocompatibility of Magnesium Alloys for the Next-Generation Vascular Stents. Nanoscale 2013, 5, 9517–9522. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zheng, B.; Wang, P.; Wang, X.; Zhang, B.; Shi, Q.; Xi, T.; Chen, M.; Guan, S. Enhanced In Vitro and In Vivo Performance of Mg-Zn-Y-Nd Alloy Achieved with APTES Pretreatment for Drug-Eluting Vascular Stent Application. ACS Appl. Mater. Interfaces 2016, 8, 17842–17858. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Xia, K.; Wang, T.; Niu, J.; Song, Y.; Xiong, Z.; Zheng, K.; Wei, S.; Lu, W. Growth, In Vitro Biodegradation and Cytocompatibility Properties of Nano-Hydroxyapatite Coatings on Biodegradable Magnesium Alloys. J. Alloys Compd. 2016, 672, 366–373. [Google Scholar] [CrossRef]
- Husak, Y.; Solodovnyk, O.; Yanovska, A.; Kozik, Y.; Liubchak, I.; Ivchenko, V.; Mishchenko, O.; Zinchenko, Y.; Kuznetsov, V.; Pogorielov, M. Degradation and In Vivo Response of Hydroxyapatite-Coated Mg Alloy. Coatings 2018, 8, 375. [Google Scholar] [CrossRef] [Green Version]
- Saremi, M.; Mohajernia, S.; Hejazi, S. Controlling the Degradation Rate of AZ31 Magnesium Alloy and Purity of Nano-Hydroxyapatite Coating by Pulse Electrodeposition. Mater. Lett. 2014, 129, 111–113. [Google Scholar] [CrossRef]
- Plaass, C.; Ettinger, S.; Sonnow, L.; Koenneker, S.; Noll, Y.; Weizbauer, A.; Reifenrath, J.; Claassen, L.; Daniilidis, K.; Stukenborg-Colsman, C.; et al. Early Results Using a Biodegradable Magnesium Screw for Modified Chevron Osteotomies. J. Orthop. Res. 2016, 34, 2207–2214. [Google Scholar] [CrossRef] [Green Version]
- Biber, R.; Pauser, J.; Geßlein, M.; Bail, H.J. Magnesium-Based Absorbable Metal Screws for Intra-Articular Fracture Fixation. Case Rep. Orthop. 2016, 2016, 9673174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wichelhaus, A.; Emmerich, J.; Mittlmeier, T. A Case of Implant Failure in Partial Wrist Fusion Applying Magnesium-Based Headless Bone Screws. Case Rep. Orthop. 2016, 2016, 7049130. [Google Scholar] [CrossRef] [Green Version]
- Leonhardt, H.; Franke, A.; McLeod, N.M.H.; Lauer, G.; Nowak, A. Fixation of Fractures of the Condylar Head of the Mandible with a New Magnesium-Alloy Biodegradable Cannulated Headless Bone Screw. Br. J. Oral Maxillofac. Surg. 2017, 55, 623–625. [Google Scholar] [CrossRef] [PubMed]
- Biber, R.; Pauser, J.; Brem, M.; Bail, H.J. Bioabsorbable Metal Screws in Traumatology: A Promising Innovation. Trauma Case Rep. 2017, 8, 11–15. [Google Scholar] [CrossRef]
- Gigante, A.; Setaro, N.; Rotini, M.; Finzi, S.S.; Marinelli, M. Intercondylar Eminence Fracture Treated by Resorbable Magnesium Screws Osteosynthesis: A Case Series. Injury 2018, 49, S48–S53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acar, B.; Kose, O.; Unal, M.; Turan, A.; Kati, Y.A.; Guler, F. Comparison of Magnesium versus Titanium Screw Fixation for Biplane Chevron Medial Malleolar Osteotomy in the Treatment of Osteochondral Lesions of the Talus. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 163–173. [Google Scholar] [CrossRef]
- Choo, J.T.; Lai, S.H.S.; Tang, C.Q.Y.; Thevendran, G. Magnesium-Based Bioabsorbable Screw Fixation for Hallux Valgus Surgery—A Suitable Alternative to Metallic Implants. Foot Ankle Surg. 2019, 25, 727–732. [Google Scholar] [CrossRef]
- Kose, O.; Turan, A.; Unal, M.; Acar, B.; Guler, F. Fixation of Medial Malleolar Fractures with Magnesium Bioabsorbable Headless Compression Screws: Short-Term Clinical and Radiological Outcomes in Eleven Patients. Arch. Orthop. Trauma Surg. 2018, 138, 1069–1075. [Google Scholar] [CrossRef]
- Atkinson, H.D.; Khan, S.; Lashgari, Y.; Ziegler, A. Hallux Valgus Correction Utilising a Modified Short Scarf Osteotomy with a Magnesium Biodegradable or Titanium Compression Screws—A Comparative Study of Clinical Outcomes. BMC Musculoskelet. Disord. 2019, 20, 334. [Google Scholar] [CrossRef] [Green Version]
- Klauser, H. Internal Fixation of Three-Dimensional Distal Metatarsal I Osteotomies in the Treatment of Hallux Valgus Deformities Using Biodegradable Magnesium Screws in Comparison to Titanium Screws. Foot Ankle Surg. 2019, 25, 398–405. [Google Scholar] [CrossRef]
- Zhao, D.; Huang, S.; Lu, F.; Wang, B.; Yang, L.; Qin, L.; Yang, K.; Li, Y.; Li, W.; Wang, W.; et al. Vascularized Bone Grafting Fixed by Biodegradable Magnesium Screw for Treating Osteonecrosis of the Femoral Head. Biomaterials 2016, 81, 84–92. [Google Scholar] [CrossRef]
- Yu, X.; Zhao, D.; Huang, S.; Wang, B.; Zhang, X.; Wang, W.; Wei, X. Biodegradable Magnesium Screws and Vascularized Iliac Grafting for Displaced Femoral Neck Fracture in Young Adults. BMC Musculoskelet. Disord. 2015, 16, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-W.; Han, H.-S.; Han, K.-J.; Park, J.; Jeon, H.; Ok, M.-R.; Seok, H.-K.; Ahn, J.-P.; Lee, K.E.; Lee, D.-H. Long-Term Clinical Study and Multiscale Analysis of In Vivo Biodegradation Mechanism of Mg Alloy. Proc. Natl. Acad. Sci. USA 2016, 113, 716–721. [Google Scholar] [CrossRef] [Green Version]
- Windhagen, H.; Radtke, K.; Weizbauer, A.; Diekmann, J.; Noll, Y.; Kreimeyer, U.; Schavan, R.; Stukenborg-Colsman, C.; Waizy, H. Biodegradable Magnesium-Based Screw Clinically Equivalent to Titanium Screw in Hallux Valgus Surgery: Short Term Results of the First Prospective, Randomized, Controlled Clinical Pilot Study. Biomed. Eng. Online 2013, 12, 62. [Google Scholar] [CrossRef] [Green Version]
- Zartner, P.; Buettner, M.; Singer, H.; Sigler, M. First Biodegradable Metal Stent in a Child with Congenital Heart Disease: Evaluation of Macro and Histopathology. Catheter. Cardiovasc. Interv. 2007, 69, 443–446. [Google Scholar] [CrossRef]
- Zartner, P.; Cesnjevar, R.; Singer, H.; Weyand, M. First Successful Implantation of a Biodegradable Metal Stent into the Left Pulmonary Artery of a Preterm Baby. Catheter. Cardiovasc. Interv. 2005, 66, 590–594. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.J.; Oslizlok, P.; Walsh, K.P. Early Restenosis Following Biodegradable Stent Implantation in an Aortopulmonary Collateral of a Patient with Pulmonary Atresia and Hypoplastic Pulmonary Arteries. Catheter. Cardiovasc. Interv. 2007, 69, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Schranz, D.; Zartner, P.; Michel-Behnke, I.; Akintürk, H. Bioabsorbable Metal Stents for Percutaneous Treatment of Critical Recoarctation of the Aorta in a Newborn. Catheter. Cardiovasc. Interv. 2006, 67, 671–673. [Google Scholar] [CrossRef]
- Maeng, M.; Jensen, L.O.; Falk, E.; Andersen, H.R.; Thuesen, L. Negative Vascular Remodelling after Implantation of Bioabsorbable Magnesium Alloy Stents in Porcine Coronary Arteries: A Randomised Comparison with Bare-Metal and Sirolimus-Eluting Stents. Heart 2009, 95, 241–246. [Google Scholar] [CrossRef]
- Waksman, R.; Erbel, R.; Di Mario, C.; Bartunek, J.; de Bruyne, B.; Eberli, F.R.; Erne, P.; Haude, M.; Horrigan, M.; Ilsley, C.; et al. Early- and Long-Term Intravascular Ultrasound and Angiographic Findings After Bioabsorbable Magnesium Stent Implantation in Human Coronary Arteries. JACC Cardiovasc. Interv. 2009, 2, 312–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gersh, B.J. Temporary Scaffolding of Coronary Arteries with Bioabsorbable Magnesium Stents: A Prospective, Non-Randomised Multicentre Trial. Yearb. Cardiol. 2008, 2008, 241–243. [Google Scholar] [CrossRef]
- Haude, M.; Erbel, R.; Erne, P.; Verheye, S.; Degen, H.; Böse, D.; Vermeersch, P.; Wijnbergen, I.; Weissman, N.; Prati, F.; et al. Safety and Performance of the Drug-Eluting Absorbable Metal Scaffold (DREAMS) in Patients with de-Novo Coronary Lesions: 12 Month Results of the Prospective, Multicentre, First-in-Man BIOSOLVE-I Trial. Lancet 2013, 381, 836–844. [Google Scholar] [CrossRef]
- Haude, M.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; Von Birgelen, C.; Christiansen, E.H.; Wijns, W.; Neumann, F.J.; Kaiser, C.; et al. Safety and Performance of the Second-Generation Drug-Eluting Absorbable Metal Scaffold in Patients with de-Novo Coronary Artery Lesions (BIOSOLVE-II): 6 Month Results of a Prospective, Multicentre, Non-Randomised, First-in-Man Trial. Lancet 2016, 387, 31–39. [Google Scholar] [CrossRef]
- Haude, M.; Wlodarczak, A.; van der Schaaf, R.J.; Torzewski, J.; Ferdinande, B.; Escaned, J.; Iglesias, J.F.; Bennett, J.; Toth, G.; Joner, M.; et al. Safety and Performance of the Third-Generation Drug-Eluting Resorbable Coronary Magnesium Scaffold System in the Treatment of Subjects with de Novo Coronary Artery Lesions: 6-Month Results of the Prospective, Multicenter BIOMAG-I First-in-Human Study. EClinicalMedicine 2023, 59, 101940. [Google Scholar] [CrossRef] [PubMed]
- Towers, W.S.; Kurtom, K. Rare Systemic Response to Titanium Spinal Fusion Implant: Case Report. Cureus 2020, 12, e7109. [Google Scholar] [CrossRef] [Green Version]
- K Singh, N.; Kumar Singh, N.; Pandit, D.; Saxena, K.K. Recent Trends in Bio-Materials and Advances in Design of Spinal Fusion Implants. Adv. Mater. Process. Technol. 2022, 8, 2122–2141. [Google Scholar]
- Novikova, L.N.; Novikov, L.N.; Kellerth, J.-O. Biopolymers and Biodegradable Smart Implants for Tissue Regeneration after Spinal Cord Injury. Curr. Opin. Neurol. 2003, 16, 711–715. [Google Scholar] [PubMed]
- Winicki, N.; Lin, J.; Holt-Torres, P.; Vyas, R.; Aslani, A.; Tobin, E.; Liu, H. Magnesium-Based Bioresorbable Implants for Craniomaxillofacial and Orthopaedic Operations: In Vivo Studies in Rats. J. Am. Coll. Surg. 2021, 233, S208. [Google Scholar] [CrossRef]
- Shankar, S.; Nithyaprakash, R.; Abbas, G.; Naveenkumar, R.; Prakash, C.; Pramanik, A.; Basak, A.K. Tribological Behavior of AZ31 Alloy Against Si3N4 Using In-Vitro and In-Silico Submodeling Approach for Human Hip Prosthesis. Silicon 2023, 15, 983–991. [Google Scholar] [CrossRef]
- Heublein, B.; Rohde, R.; Kaese, V.; Niemeyer, M.; Hartung, W.; Haverich, A. Biocorrosion of Magnesium Alloys: A New Principle in Cardiovascular Implant Technology? Heart 2003, 89, 651. [Google Scholar] [CrossRef] [Green Version]
- Antuña, P.; Cuesta, J.; García-Guimaraes, M.; Alfonso, F. Coronary Aneurysms After Magnesium Resorbable Vascular Scaffolds: “The Dissolving Scaffold Follows the Vessel Wall”. Cardiovasc. Revascularization Med. 2020, 21, 162–164. [Google Scholar] [CrossRef]
- Radwan-Pragłowska, J.; Janus, Ł.; Szajna, E.; Galek, T.; Sierakowska, A.; Piątkowski, M.; Tupaj, M.; Radomski, P.; Michalec, M.; Bogdał, D. Biodegradable Mg-Based Implants Obtained via Anodic Oxidation Applicable in Dentistry: Preparation and Characterization. J. Mater. Res. Technol. 2022, 20, 1736–1754. [Google Scholar] [CrossRef]
- Mei, D.; Wang, C.; Nienaber, M.; Pacheco, M.; Barros, A.; Neves, S.; Reis, R.L.; Zhu, S.; Bohlen, J.; Letzig, D. Corrosion Behavior of Mg Wires for Ureteral Stent in Artificial Urine Solution. Corros. Sci. 2021, 189, 109567. [Google Scholar] [CrossRef]
- Zhang, S.; Zheng, Y.; Zhang, L.; Bi, Y.; Li, J.; Liu, J.; Yu, Y.; Guo, H.; Li, Y. In Vitro and In Vivo Corrosion and Histocompatibility of Pure Mg and a Mg-6Zn Alloy as Urinary Implants in Rat Model. Mater. Sci. Eng. C 2016, 68, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Yao, L.; Yuan, F.; Dai, G.; Xue, B. Evaluation of a Novel Biodegradable Ureteral Stent Produced from Polyurethane and Magnesium Alloys. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Seetharaman, S.; Subramanian, J.; Singh, R.A.; Wong, W.L.E.; Nai, M.L.S.; Gupta, M. Mechanical Properties of Sustainable Metal Matrix Composites: A Review on the Role of Green Reinforcements and Processing Methods. Technology 2022, 10, 32. [Google Scholar] [CrossRef]
- Heimann, R.B. The Nature of Plasma Spraying. Coatings 2023, 13, 622. [Google Scholar] [CrossRef]
- Malaki, M.; Xu, W.; Kasar, A.K.; Menezes, P.L.; Dieringa, H.; Varma, R.S.; Gupta, M. Advanced Metal Matrix Nanocomposites. Metals 2019, 9, 330. [Google Scholar] [CrossRef] [Green Version]
- Pappas, J.M.; Dong, X. Characterization of Laser Direct Deposited Magnesium Aluminate Spinel Ceramics. In Proceedings of the 2019 International Solid Freeform Fabrication Symposium, Austin, TX, USA, 12–14 August 2019; University of Texas at Austin: Austin, TX, USA, 2019. [Google Scholar]
- Exner, H.E.; Arzt, E. Sintering Processes; Springer: Berlin/Heidelberg, Germany, 1990; ISBN 9401068186. [Google Scholar]
- Prashantha Kumar, H.G.; Anthony Xavior, M. Processing of Graphene/CNT-Metal Powder. In Powder Technology; Cavalheiro, A.A., Ed.; IntechOpen: Rijeka, Croatia, 2018; Chapter 3; ISBN 978-1-78923-661-3. [Google Scholar]
- Matli, P.R.; Shakoor, R.A.; Amer Mohamed, A.M.; Gupta, M. Microwave Rapid Sintering of Al-Metal Matrix Composites: A Review on the Effect of Reinforcements, Microstructure and Mechanical Properties. Metals 2016, 6, 143. [Google Scholar] [CrossRef] [Green Version]
- Suryanarayana, C.; Ivanov, E.; Boldyrev, V. V The Science and Technology of Mechanical Alloying. Mater. Sci. Eng. A 2001, 304, 151–158. [Google Scholar] [CrossRef]
- Suryanarayana, C. Mechanical Alloying: A Novel Technique to Synthesize Advanced Materials. Research 2019, 2019, 4219812. [Google Scholar] [CrossRef] [Green Version]
- Mamedov, V. Spark Plasma Sintering as Advanced PM Sintering Method. Powder Metall. 2002, 45, 322–328. [Google Scholar] [CrossRef]
- Franceschin, G.; Flores-Martínez, N.; Vázquez- Victorio, G.; Ammar, S.; Valenzuela, R. Sintering and Reactive Sintering by Spark Plasma Sintering (SPS). In Sintering of Functional Materials; Shishkovsky, I., Ed.; IntechOpen: Rijeka, Croatia, 2017; Chapter 6; ISBN 978-953-51-3757-3. [Google Scholar]
- Kantaros, A. 3D Printing in Regenerative Medicine: Technologies and Resources Utilized. Int. J. Mol. Sci. 2022, 23, 14621. [Google Scholar] [CrossRef] [PubMed]
- Mirzababaei, S.; Pasebani, S. A Review on Binder Jet Additive Manufacturing of 316L Stainless Steel. J. Manuf. Mater. Process. 2019, 3, 82. [Google Scholar] [CrossRef] [Green Version]
- Kurzynowski, T.; Pawlak, A.; Smolina, I. The Potential of SLM Technology for Processing Magnesium Alloys in Aerospace Industry. Arch. Civ. Mech. Eng. 2020, 20, 23. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Liu, X.; Zhao, Y. Research Status and Prospect of Friction Stir Processing Technology. Coatings 2019, 9, 129. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Zhou, Y.; Liu, C.; Wu, Q.; Chen, X.; Lu, J. Wire Arc Additive Manufacturing of AZ31 Magnesium Alloy: Grain Refinement by Adjusting Pulse Frequency. Materials 2016, 9, 823. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Zhang, J.; Wang, J.; Li, Z.; Xie, J.; Liu, S.; Guan, K.; Wu, R. Toward the Development of Mg Alloys with Simultaneously Improved Strength and Ductility by Refining Grain Size via the Deformation Process. Int. J. Miner. Metall. Mater. 2021, 28, 30–45. [Google Scholar] [CrossRef]
- Nazeer, F.; Long, J.; Yang, Z.; Li, C. Superplastic Deformation Behavior of Mg Alloys: A-Review. J. Magnes. Alloy. 2022, 10, 97–109. [Google Scholar] [CrossRef]
- Danish, M.; Yasir, M.; Mia, M.; Nazir, K.; Ahmed, T.; Rani, A.M.A. High Speed Machining of Magnesium and Its Alloys. In High Speed Machining; Elsevier: Amsterdam, The Netherlands, 2020; pp. 263–282. [Google Scholar]
- Carou, D.; Rubio, E.M.; Davim, J.P. Machinability of Magnesium and Its Alloys: A Review. Tradit. Mach. Process. Res. Adv. 2015, 2015, 133–152. [Google Scholar]
- Venkatesh, R.; SivaChandran, S.; Maridurai, T.; Baskar, S.; Sivashankar, N.; Arivazhagan, R. Magnesium Alloy Machining and Its Methodology: A Systematic Review and Analyses. In Proceedings of the AIP Conference Proceedings; AIP Publishing LLC: Long Island, NY, USA, 2022; Volume 2473, p. 020003. [Google Scholar]
- Kuczmaszewski, J.; Zagorski, I.; Dziubinska, A. Investigation of Ignition Temperature, Time to Ignition and Chip Morphology after the High-Speed Dry Milling of Magnesium Alloys. Aircr. Eng. Aerosp. Technol. Int. J. 2016, 88, 389–396. [Google Scholar] [CrossRef]
- Dinesh, S.; Senthilkumar, V.; Asokan, P.; Arulkirubakaran, D. Effect of Cryogenic Cooling on Machinability and Surface Quality of Bio-Degradable ZK60 Mg Alloy. Mater. Des. 2015, 87, 1030–1036. [Google Scholar] [CrossRef]
- Bhowmick, S.; Alpas, A.T. The Role of Diamond-like Carbon Coated Drills on Minimum Quantity Lubrication Drilling of Magnesium Alloys. Surf. Coat. Technol. 2011, 205, 5302–5311. [Google Scholar] [CrossRef]
- Carou, D.; Rubio, E.M.; Lauro, C.H.; Davim, J.P. Experimental Investigation on Surface Finish during Intermittent Turning of UNS M11917 Magnesium Alloy under Dry and near Dry Machining Conditions. Measurement 2014, 56, 136–154. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Permanent Implants | Temporary Implants |
|---|---|---|
| Intended use | Designed to replace or enhance a body part or function that has been lost or compromised, such as a hip replacement, dental implant, or pacemaker. | Designed for short-term applications such as stabilizing bone fractures, providing support during tissue healing, or delivering medication to a specific site in the body. |
| Examples | Hip replacements, dental implants, pacemakers, breast implants, and joint replacements. | Sutures, splints, stents, temporary dental crowns, drug delivery systems. |
| Duration of placement | Designed to remain in the body for an extended period of time, often for the patient’s lifetime. | Intended to be removed after a certain period of time, ranging from a few days to several years. |
| Design considerations | Requires more complex design considerations to ensure their longevity, durability, and compatibility with the body. They are typically made from materials that are biocompatible and can withstand the stresses and strains of daily use, such as titanium, stainless steel, or ceramic. | Design and choice of material depends on the application. Can be made using materials that can be absorbed by the body or easily removed. For example, sutures are made from absorbable materials that break down over time and are absorbed by the body’s tissues. Splints and casts are made from materials such as plaster or fiberglass that can be easily removed once the injury has healed. |
| Surgical procedure | Requires invasive surgical procedures, such as the insertion of a hip replacement or the placement of a dental implant. | Temporary implants require multiple invasive surgical procedures. However, the rectification surgery for implant removal can be avoided if biodegradable materials are employed as temporary implants |
| Biocompatibility and corrosion | The material should be non-toxic and not cause an immune response or rejection by the body. The material should not corrode or degrade in the body’s harsh environment. | The material should be non-toxic and not cause an immune response or rejection by the body. Temporary implant must be designed in such a way that it either remains inert (for removable implants) or degrade over time in a controlled fashion (in the case of biodegradable implants). |
| Mechanical Properties | The material should be able to withstand the body’s natural wear and tear for a long period of time without degrading or breaking down. They should have high strength, stiffness, and durability for long-term support. | Sufficient strength to provide temporary support. The material should be flexible and able to conform to the shape of the body part where it is inserted. |
| Materials |
|
|
| Alloy | Tensile Strength (MPa) | Yield Strength (MPa) | Modulus of Elasticity (GPa) | Elongation (%) | Corrosion Rate (mm/year) |
|---|---|---|---|---|---|
| AE42 | 230 | 145 | 45–55 | 6 | - |
| AE44 | 245 | 142 | 52–57 | 10 | −0.2 |
| AM100A | 150–275 | 83–110 | 45–60 | 2–4 | - |
| AM20 | 210 | 90 | - | 20 | - |
| AM50 | 230 | 125 | 45 | 8 | - |
| AM60 | 220 | 130 | 45–50 | 6 | - |
| AZ31 | 240–290 | 150–220 | 45 | 9–21 | 0.1–0.3 |
| AZ61 | 195–310 | 180–240 | 44–50 | 12–16 | 0.1–0.3 |
| AZ63 | 200–275 | 97–130 | 45 | 6–12 | - |
| AZ80 | 315–380 | 215–275 | 45 | 5–11 | - |
| AZ81 | 275 | 85 | 45–65 | 15 | - |
| AZ91 | 165–275 | 80–195 | 44–47 | 2.3–4.5 | 0.1–0.3 |
| EQ21 | 234 | 172 | - | 2 | - |
| EQ22 | 275 | 205 | - | 4 | - |
| EZ33 | 160 | 105 | - | 3 | - |
| WE43 | 235 | 190 | 45–55 | 4–10 | 0.05–0.1 |
| WE54 | 270 | 190 | 45–60 | 4 | - |
| ZE41 | 205 | 140 | 50 | 3.5 | - |
| ZE63 | 295 | 190 | - | 7 | - |
| ZEK100 | 250–280 | 140–200 | 45–50 | 10–15 | 0.02–0.05 |
| ZK51 | 276 | 165 | - | 3 | - |
| ZK60 | 305–365 | 200–305 | - | 11–16 | - |
| MgCa0.4 | 190–230 | 72–166 | - | 21–34 | - |
| MgCa0.8 | 145–185 | 70–100 | 45–55 | 10–20 | 0.2–0.3 |
| MgCa | 165–315 | 81–230 | - | 1.6–19 | 0.02–0.31 |
| MgSn0.25–3Ca0.2–1.5 | 240 | - | - | 8–9 | - |
| MgSr0.5 | 98 | 44 | - | 4.0 | - |
| MgSr0.3Ca0.3 | 107 | 52 | - | 8.8 | - |
| MgZn1Mn1Sr0.25–1 | 255–280 | 206–241 | - | 7–18 | 0.5–2.0 |
| MgSrY | 75–115 | 45–71 | - | 5–8 | 0.7–12 |
| MgZn6 | 280 | 169 | 42.3 | 18.8 | 2.32 |
| MgZn1Ca0.5 | 210 | - | - | 44 | 3.91 |
| MgZn4Ca0.2 | 185–297 | 60–240 | - | 12.5–21.3 | 1.98–2.05 |
| MgZn4RE0.5 | 142 | 110 | - | 8.9 | 0.105 |
| ZX21 | 190–240 | 150–200 | 40–50 | 5–15 | 0.05–0.1 |
| ZQ63 | 170–320 | 100–300 | 42–45 | 4–14 | 0.005–0.02 |
| QX120 | 170–240 | 125–320 | 45–50 | 10–24 | 0.005–0.008 |
| Mg/(10–30)Al2O3 | 200–240 | 160–180 | 50–60 | 5–10 | 0.005–0.03 |
| Mg/(10–30)ZrO2 | 190–230 | 140–170 | 40–60 | 5–10 | 0.01–0.05 |
| Mg/(5–20)TiO2 | 190–220 | 130–150 | 20–30 | 5–10 | 0.001–0.02 |
| Mg/(10–30)HA | 160–220 | 130–200 | 40–60 | 8–15 | 0.01–0.1 |
| Mg/(10–30)TCP | 170–220 | 100–150 | 40–50 | 8–12 | 0.02–0.08 |
| Mg/(5–20)PLA | 160–200 | 120–150 | 4–6 | 5–10 | 0.005–0.02 |
| Mg/(5–20)PGA | 200–240 | 170–200 | 5–6 | 3–6 | 0.001–0.01 |
| Traditional Implant Materials | |||||
| Ti6Al4V | 880–900 | 790–800 | 114 | 10–20 | negligible |
| CoCrMo | 1050–1300 | 800–1000 | 230 | 20–30 | negligible |
| Stainless steel (316L) | 520–700 | 190–260 | 200 | 40–50 | negligible |
| Polyetheretherketone (PEEK) | 90–120 | 70–100 | 3–4 | 50–100 | negligible |
| Polylactic acid (PLA) | 50–70 | 20–50 | 3–4 | 5–10 | negligible |
| Polyglycolic acid (PGA) | 30–50 | 10–30 | 1.5–2.5 | 10–20 | negligible |
| Alloying Element | Biocompatibility | Presence in Human Body | Presence in Blood Serum |
| Zinc | Essential micronutrient and biocompatible. Acts as antimicrobial agent and prevents the growth of bacteria on the implant surface. Promotes osteogenesis and angiogenesis. | 2 g | 46 μmol/L |
| Calcium | Plays a crucial role in bone formation. The release of Ca2+ ions can stimulate cell growth and differentiation. | 1100 g | 0.919–0.993 mg/L |
| Rare earth elements (REEs) | REEs in general (for example, like cerium, neodymium, and yttrium) modulate the immune response to reduce inflammatory reaction and enhance the biocompatibility of the alloy. The specific influence of REEs differs with respect to individual element type and concentration. | - | - |
| Strontium | Promotes osteogenesis and angiogenesis and reduces bone resorption. The release of Sr2+ ions (with similar properties as Ca2+) can stimulate cell growth and differentiation. | 0.3 g | 0.17 mg |
| Silver | Induces antibacterial effect. | - | 11–26 mg/L |
| Iron | Essential nutrient for life. However, the biocorrosion aspects needs to be carefully controlled. Can be metabolically regulated and stored. | 4–5 g | 5.0–17.6 g/L |
| Lithium | Assists in bone formation. Reduces kidney function and leads to central nervous system disorder. | 2–4 ng/g | |
| Manganese | Helps in bone formation and protects against infection. | 12 mg | 0.8 µg/L |
| Silicon | Cross-linking agent of connective tissue-based membrane structures. Necessary for growth as bone calcification. | 18 mg | - |
| Aluminum | Releases Al3+ ions that can induce inflammatory response and oxidative stress in cells. Al is not generally recommended in biomedical alloys because of its potential neurotoxicity. | 300 mg | 2.1–4.8 µg/L |
| Nickel | Carcinogenic and toxic. Strong allergen that induces metal sensitivity. | 10 mg | 0.05–0.23 μg/L |
| Copper | Allergen. Trace element in cell. Induces cytotoxicity and inflammatory responses in cells due to the formation of Cu2+ ions. | 200 mg | 74–131 μmol/L |
| Tin | Carcinogenic. When used in larger amounts, leads to tin accumulation in lever. | 3 mg | <0.1 µg/L |
| Zirconium | Toxic if used in higher concentrations. | 250 mg | - |
| Polylactic acid | Biodegradable polymer. Metabolizes into lactic acid that is naturally occurring in the body | ||
| Polyglycolic acid | Biodegradable polymer. Metabolizes into glycolic acid that is naturally occurring in the body | - | |
| Hydroxyapatite | Major component of human bones and teeth. Osteoconductive. | - | 0.06–0.45 mmol/L |
| Tricalcium phosphate | Major component of human bones and teeth. Osteoconductive. Controlled degradation and increased inflammatory response than HA. | 1–2 g/kg of body weight | 0.13–1.38 mmol/L |
| Study | Type of Surgery | Type of Implant | Number of Patients | Average Age in Years | Clinical Follow-Up Timeline | Major Findings |
|---|---|---|---|---|---|---|
| Plaass et al. [100] | Symptomatic hallux valgus with indication for a Chevron-type osteotomy | MAGNEZIX® CS 3.2 (Syntellix AG, Hannover, Germany) | 40/44 | 45.5 | 6 weeks to 1 year |
|
| Biber et al. [101] | Intra-articular osteochondral fracture fixation | Cannulated MAGNEZIX compression screws | 1 | 73 | 1 year |
|
| Wichelhaus et al. [102] | Fracture reduction by palmar approach and retention to address scaphoid fracture. | Cannulated headless Magnezix screws | 1 | 42 | 6 months |
|
| Leonhardt et al. [103] | Fixation of displaced fractures of the condylar head | Magnezix CS 2.7 mm screw similar to the standard headless bone screw | 5 | 73 | - |
|
| Biber et al. [104] | Chevron osteotomies, implant for lateral malleolar fracture fixation in an ankle fracture. | 24 mm long MAGNEZIX® CS 3.2 | 1 | 43 | 6 weeks |
|
| Giganta et al. [105] | ARIF (arthroscopic reduction and internal fixation). | Magnezix | 3 | 63–64 | 1–12 months |
|
| Acar et al. [106] | Biplane chevron medial malleolar osteotomy (MMO) for osteochondral lesions of the talus (OLT) | (MAGNEZIX® CS compression screws from Syntellix - Germany, compared against Ti64 headless compression screws (Acutrak®, Acumed, Hillsboro, OR, USA) | 11 | 18–56 | 12–49 months |
|
| Choo et al. [107] | Forefoot reconstruction surgery with a scarf osteotomy | MAGNEZIX screw (Syntellix AG, Hannover, Germany). | 24/69 (remaining Ti control group) | 54.5 (21–71) years | 12 months |
|
| Kose et al. [108] | Surgery to treat displaced medial malleolar fracture | Magnesium headless compression screws (MAGNEZIX® CS, Syntellix AG, Hanover, Germany) | 11 | 12–24 months |
| |
| Atkinson et al. [109] | Fixation of displacement 1st metatarsal osteotomies in the surgical management of hallux valgus by distal 1st metatarsal “short scarf” osteotomy | Magnesium compression screws (MAGNEZIX® CS (3.2 mm diameter) compression screw) compared with titanium implants | 25 | 12–30 month |
| |
| Klauser et al. [110] | 96 Youngswick and 4 Chevron-Osteotomies | A double-threaded compression screw (MAGNEZIX1 CS 3.2) vs. Fixos screws made of titanium alloy Ti 6Al-4V | 95 Mg vs. 90 Ti | 50.9 vs. 52.3 | 12.2 vs. 11.7 months |
|
| Zhao et al. [111] | Treatment of necrosis | Pure Mg screws | 1 | 17 | 2 years |
|
| Yu et al. [112] | Treatment of displaced femora | Combination of pure Mg implants with vascularized iliac grafting | 19 | 22–45 | 8–24 months |
|
| Lee et al. [113] | Mg-5 wt%Ca-1 wt%Zn alloy | 53 | 20 | 3 |
| |
| Windhagen et al. [114] | Hallux valgus surgery | Magnezix | 26 (Either Ti or Mg, similar design) | 6 months |
| |
| Zartner et al. [115,116] | Hybrid surgical procedure | Cardiovascular stent for balloon angioplasty (Biotronik) | 1 | Newborn | 5 months |
|
| McMahon et al. [117] | Coronary Intervention | Cardiovascular stent for balloon angioplasty (Biotronik) | 1 | Newborn | 4 months |
|
| Schranz et al. [118] | Coronary Intervention | Cardiovascular stent for balloon angioplasty (Biotronik) | 1 | Newborn | 3 months |
|
| Maeng et al. [119] | Coronary Intervention | Cardiovascular stent for balloon angioplasty (Biotronik) compared with traditional stents | AMS (n = 11), sirolimus-eluting stents (Cypher; n = 11) and bare-metal stents (BMS; n = 9) | - | 90 days |
|
| Erbel et al. and Waksman et al. [120,121] | Coronary Intervention | Cardiovascular stent for balloon angioplasty (Biotronik) | 63 patients, (44 men) | 61.3 | 4, 6 and 12 months |
|
| Haude et al. [122] | Coronary Intervention | Balloon-expandable, paclitaxel-eluting scaffold (Biotronik) in symptomatic patients with de-novo coronary lesions. | 46 | - | 1, 6, 12, 24 and 36 months |
|
| Haude et al. [123] | Coronary Intervention | Balloon-expandable, paclitaxel-eluting scaffold (Biotronik) | 123 | - | 1, 6, 12, 24, and 36 months |
|
| Haude et al. [124] | Coronary Intervention | Cardiovascular stent for balloon angioplasty (Biotronik) | 116 | - | 1, 6, 12 months and annually thereafter until 5 years |
|
| Company | Country of Origin | Applications | Implant Type | Unique Features | Year Available | Website |
|---|---|---|---|---|---|---|
| Aap Implantate AG | Germany | Orthopedic | LOQTEQ® plating systems, and cannulated screws | Biodegradable, promotes bone healing, reduces risk of inflammation and infection, custom design available | 2011 | https://www.aap.de/en/ accessed on 22 April 2023 |
| Synthes | Switzerland | Orthopedic | Milagro® screws, plates, and wires | Mg–Y–RE–Zr alloy specifically designed for fractures of the distal radius | 2011 | https://www.synthes.com/ accessed on 22 April 2023 |
| Biotronik | Germany | Cardiovascular | Magmaris® cardiovascular stents | Uses SynerMag® material from magnesium elektron | 2012 | https://www.magmaris.com/ accessed on 22 April 2023 |
| Syntellix AG | Germany | Orthopedic | MAGNEZIX® screws, nails, anchors, and pins | Designed to degrade over time and be replaced by natural bone, range of implants available for orthopedic applications | 2013 | https://www.syntellix.com/ accessed on 22 April 2023 |
| MeKo Laser Material Processing | Germany | Orthopedic | RESOLOY® screws, plates, and nails | Custom implant design and manufacturing available | 2015 | https://www.meko.de/en/ accessed on 22 April 2023 |
| HCM Orthocare | India | Orthopedic | MagOrtho™ screws, plates, and rods | Coated with a bioactive substance that promotes tissue regeneration, reduces risk of inflammation, and promotes bone healing | 2015 | https://www.magortho.com/ accessed on 22 April 2023 |
| Medprin Regenerative Medical Technologies | China | Cardiovascular | MagLumine™ cardiovascular stent | The stent has a unique design that promotes arterial healing and reduces the risk of restenosis. | 2015 | http://en.medprin.com.cn/ accessed on 22 April 2023 |
| Medical magnesium | Germany | Orthopedic | Interference screws, compression screws, and anchor systems | mm.Technology | 2015 | https://www.medical-magnesium.com/en/ accessed on 22 April 2023 |
| MAGNEZIT GROUP | Russia | Orthopedic and cardiovascular | Magnesium screws, plates, and pins for orthopedic applications, as well as magnesium stents for cardiovascular applications | Use high-strength biodegradable magnesium alloy | 2013 | https://magnezit.ru/en/ accessed on 22 April 2023 |
| Technique | Benefits | Limitations |
|---|---|---|
| Liquid state processing | ||
| Gravity Die casting |
|
|
| Pressure Die Casting |
|
|
| Squeeze Casting |
|
|
| Compocasting |
|
|
| Ultrasonic assisted Compocasting | Better dispersion of reinforcement |
|
| Plasma Spray Deposition | Finer microstructure due to faster solidification rates |
|
| Disintegrated Melt Deposition |
|
|
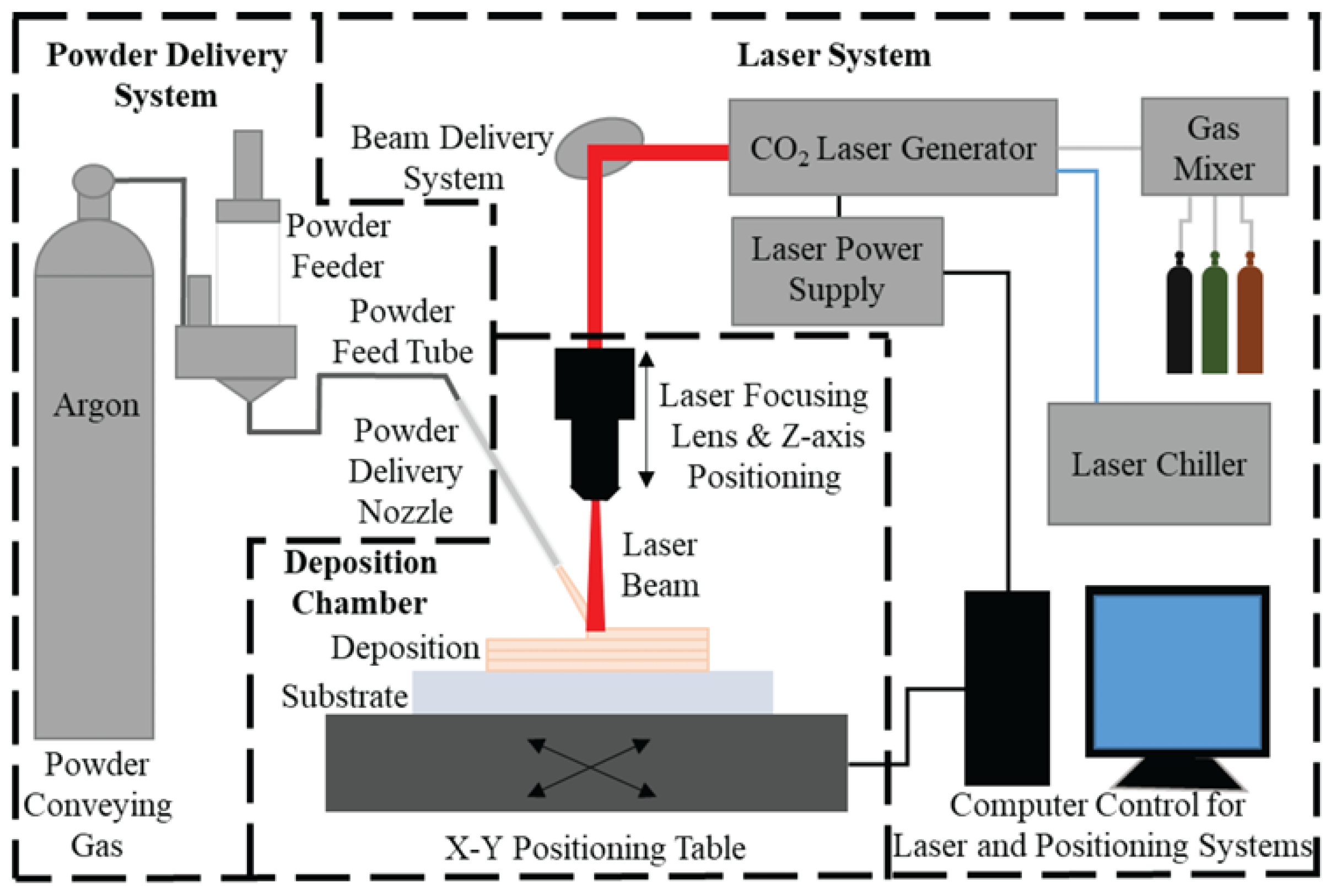
| Laser Energy Deposition |
|
|
| Solid State Processing | ||
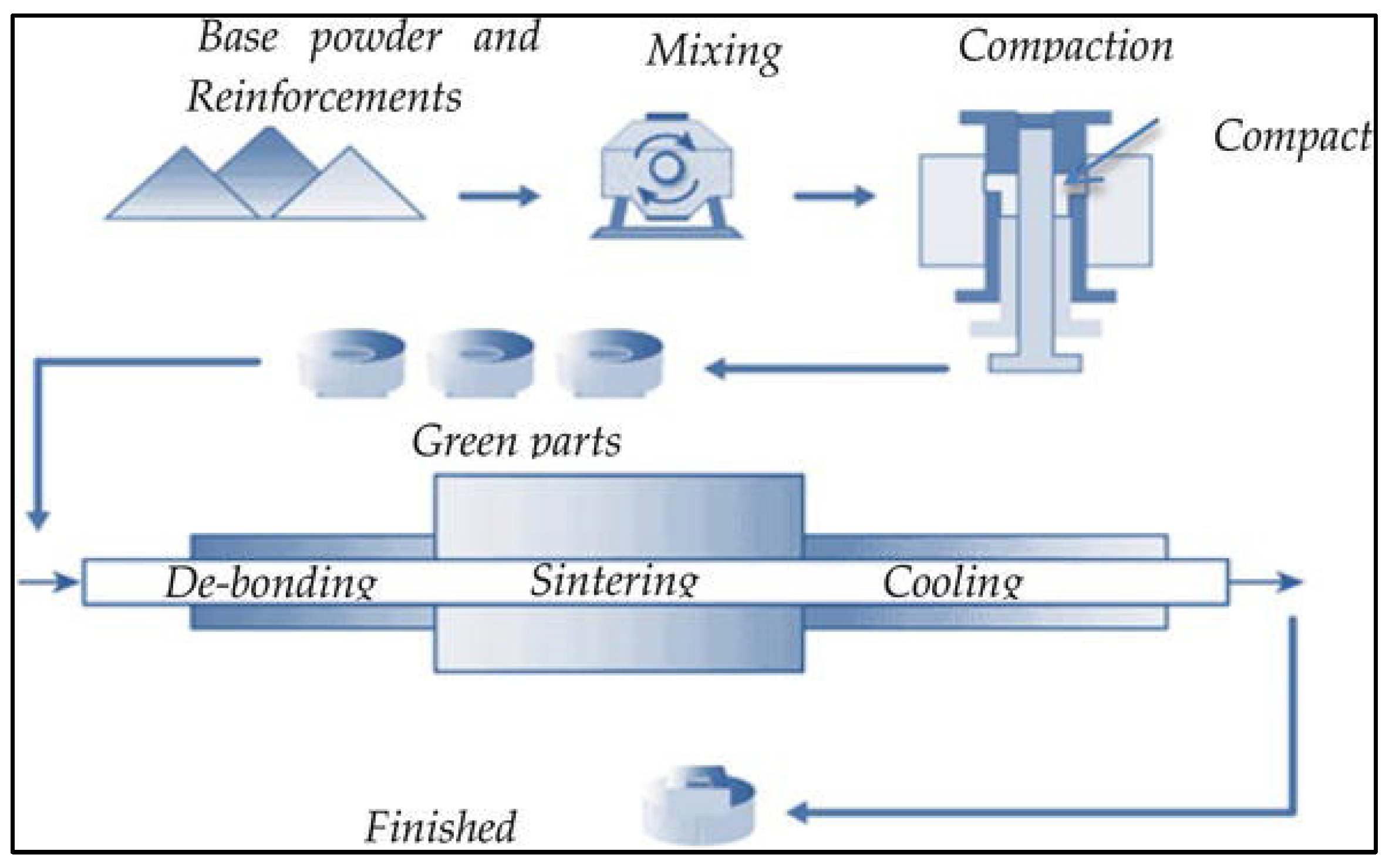
| Simple Blend-Press-Sinter |
|
|
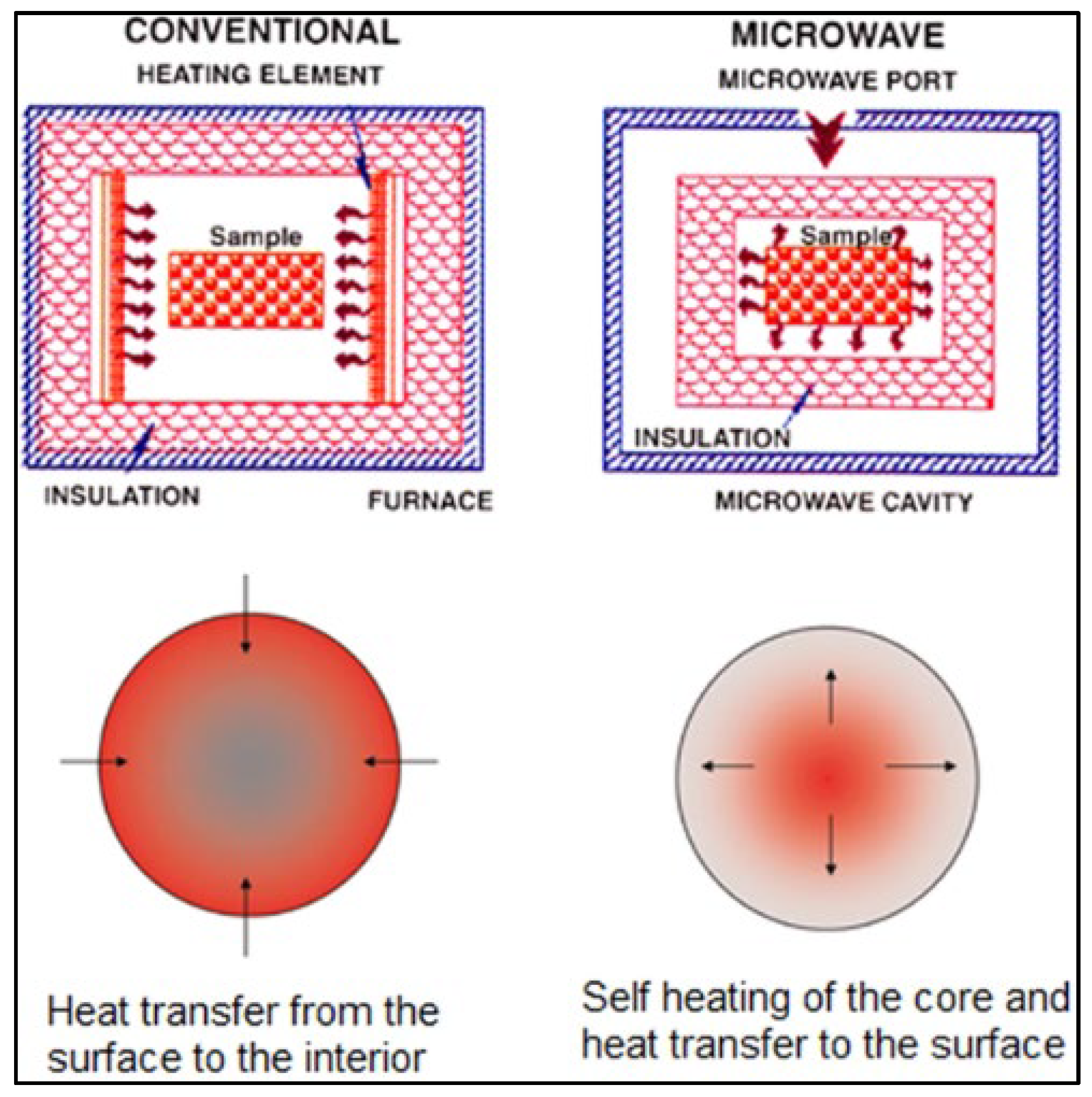
| Microwave Sintering |
|
|
| Mechanical Alloying |
|
|
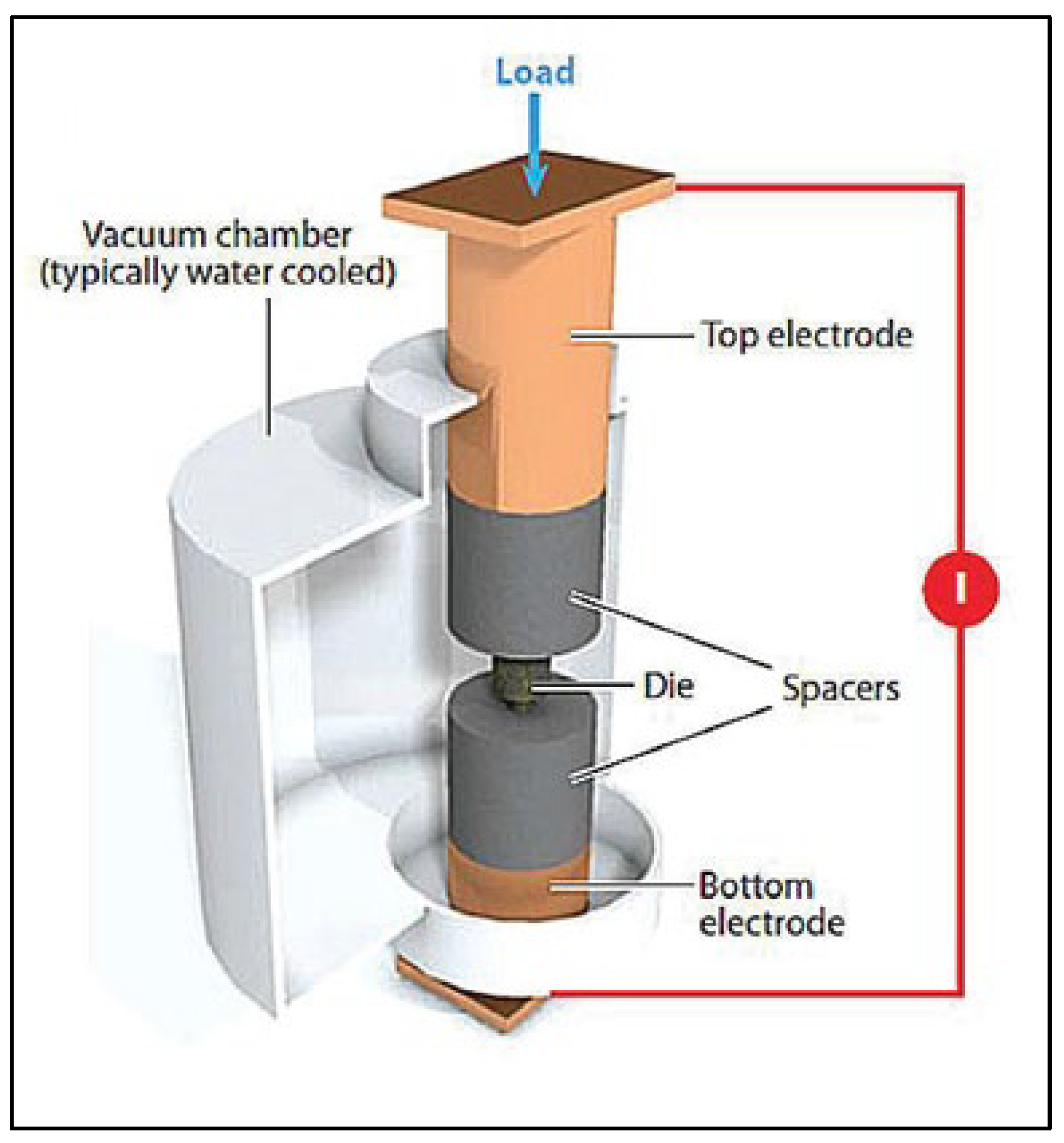
| Spark plasma sintering |
|
|
| Friction Stir Processing |
|
|
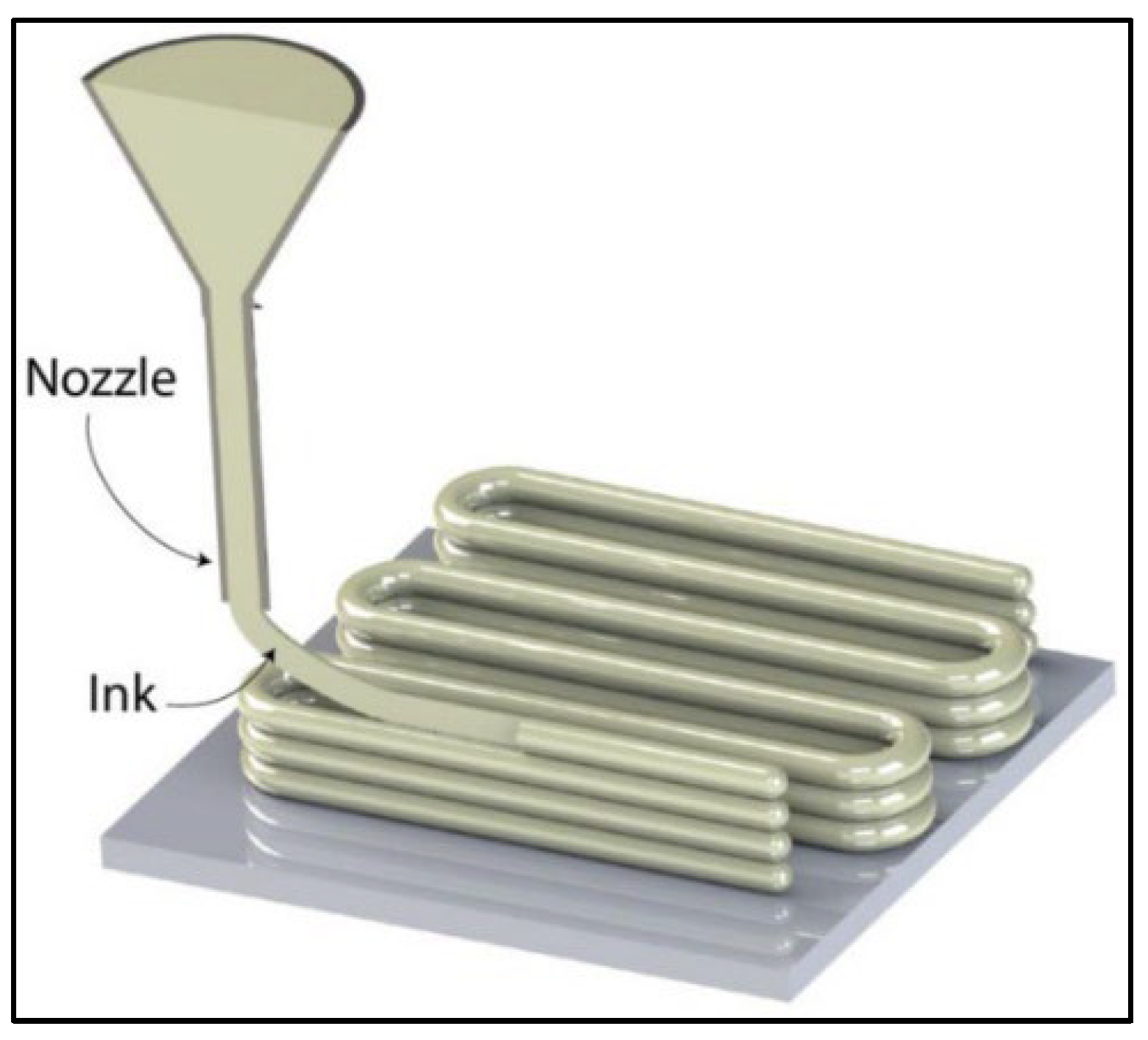
| Direct Ink Writing |
|
|
| Ink Jet Printing |
|
|
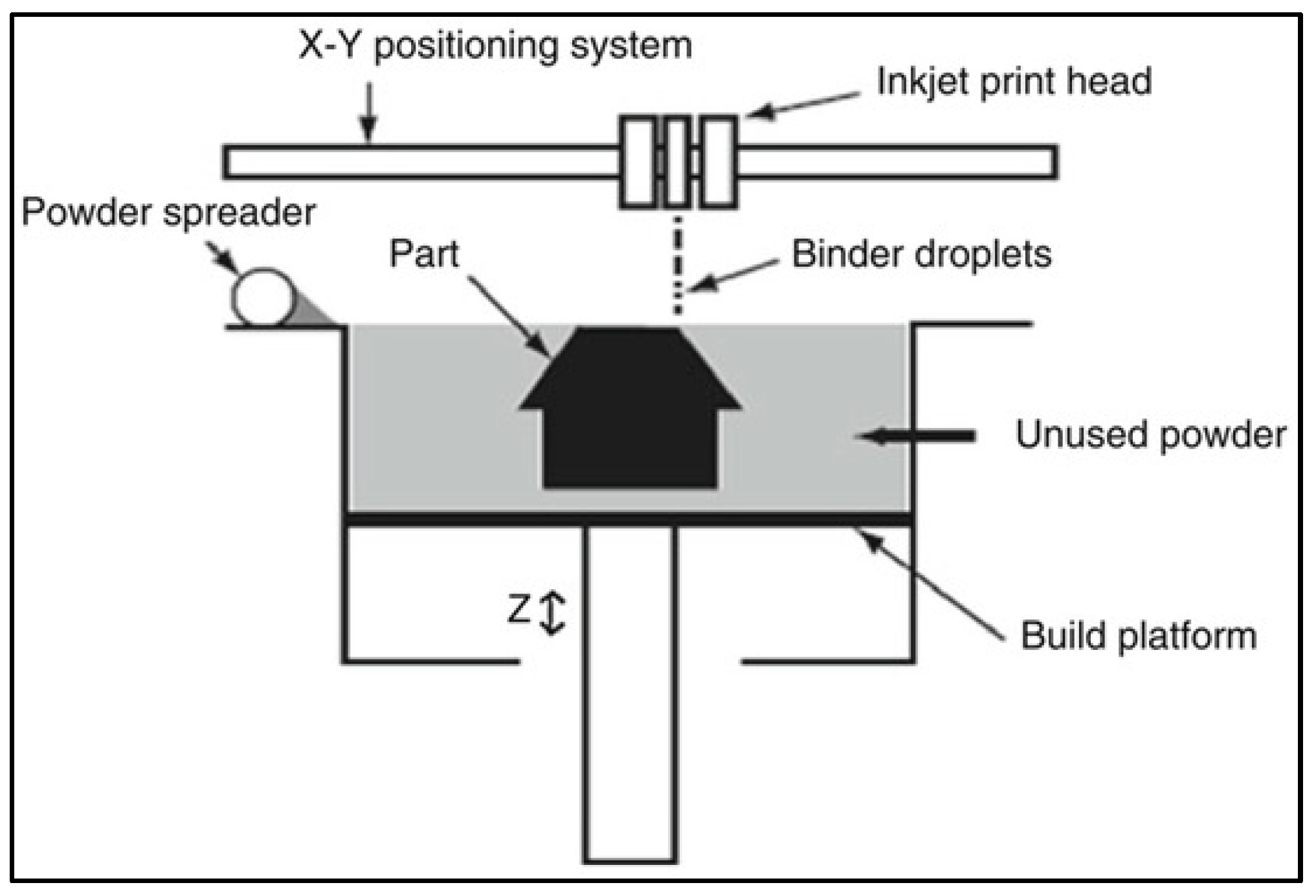
| Binder Jetting |
|
|
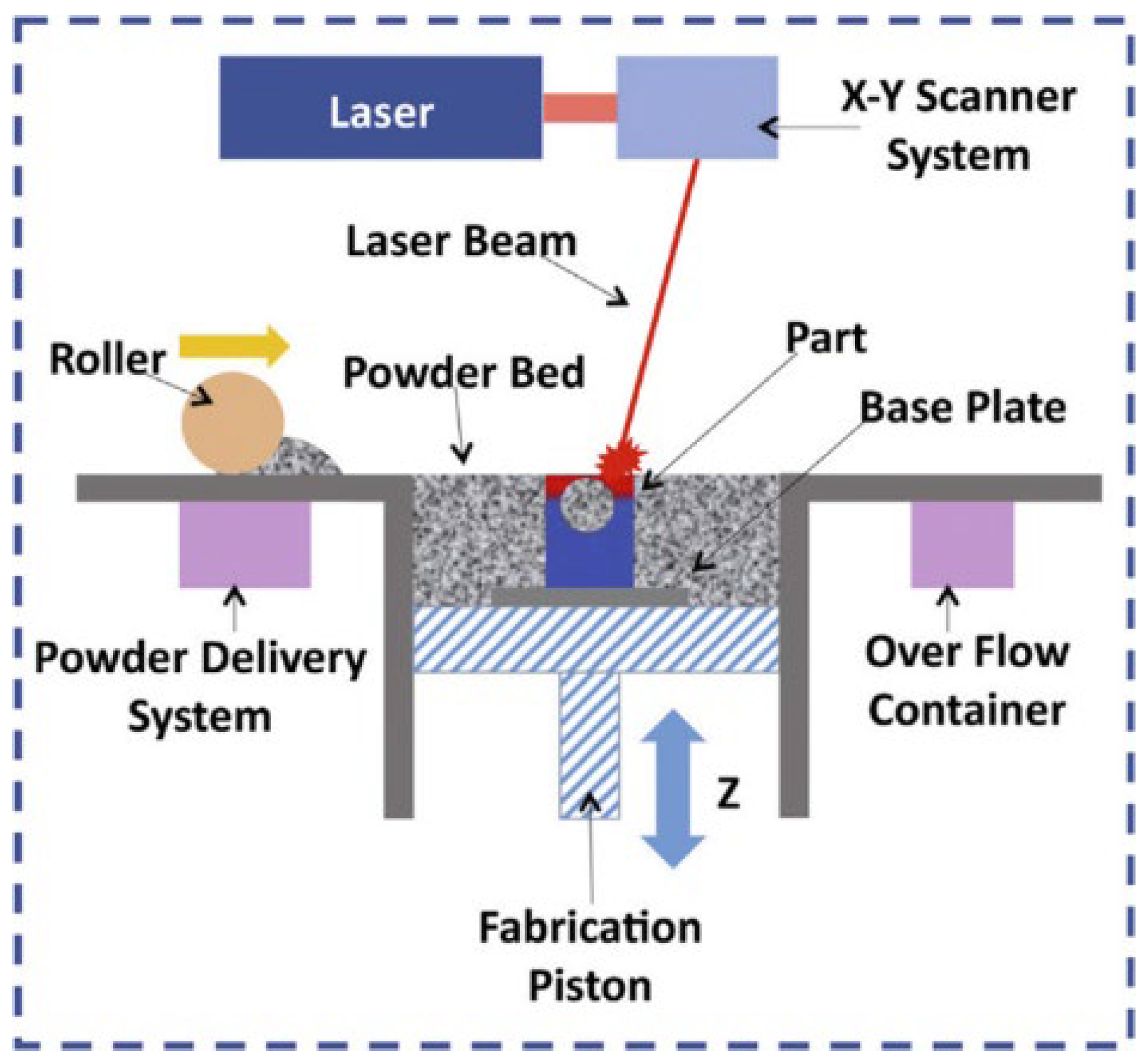
| Laser Powder Bed Fusion |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seetharaman, S.; Sankaranarayanan, D.; Gupta, M. Magnesium-Based Temporary Implants: Potential, Current Status, Applications, and Challenges. J. Funct. Biomater. 2023, 14, 324. https://doi.org/10.3390/jfb14060324
Seetharaman S, Sankaranarayanan D, Gupta M. Magnesium-Based Temporary Implants: Potential, Current Status, Applications, and Challenges. Journal of Functional Biomaterials. 2023; 14(6):324. https://doi.org/10.3390/jfb14060324
Chicago/Turabian StyleSeetharaman, Sankaranarayanan, Dhivya Sankaranarayanan, and Manoj Gupta. 2023. "Magnesium-Based Temporary Implants: Potential, Current Status, Applications, and Challenges" Journal of Functional Biomaterials 14, no. 6: 324. https://doi.org/10.3390/jfb14060324