
Functional Biomaterials for Local Control of Orthodontic Tooth Movement

Abstract
:1. Introduction
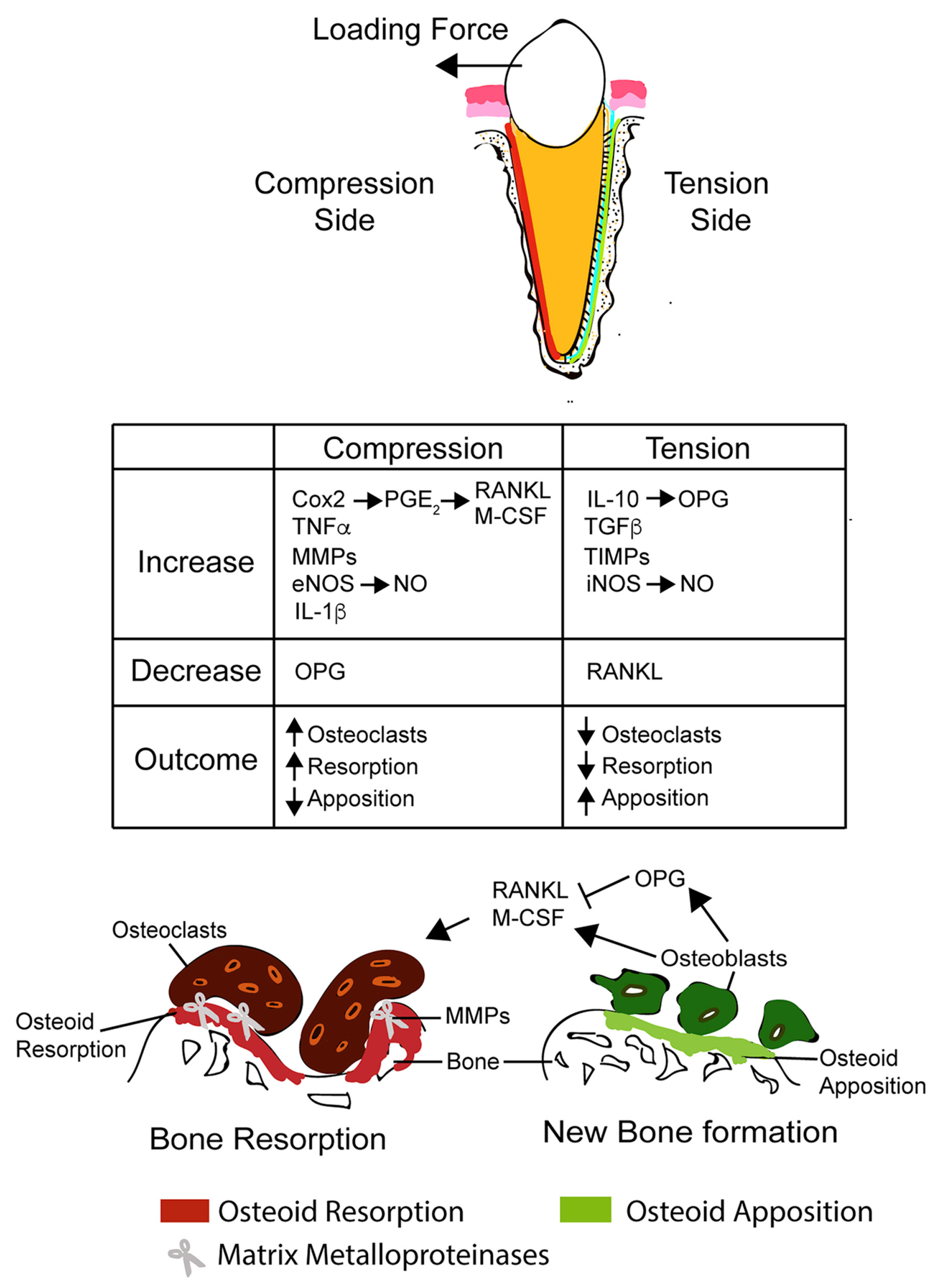
2. Mechanism of Orthodontic Tooth Movement
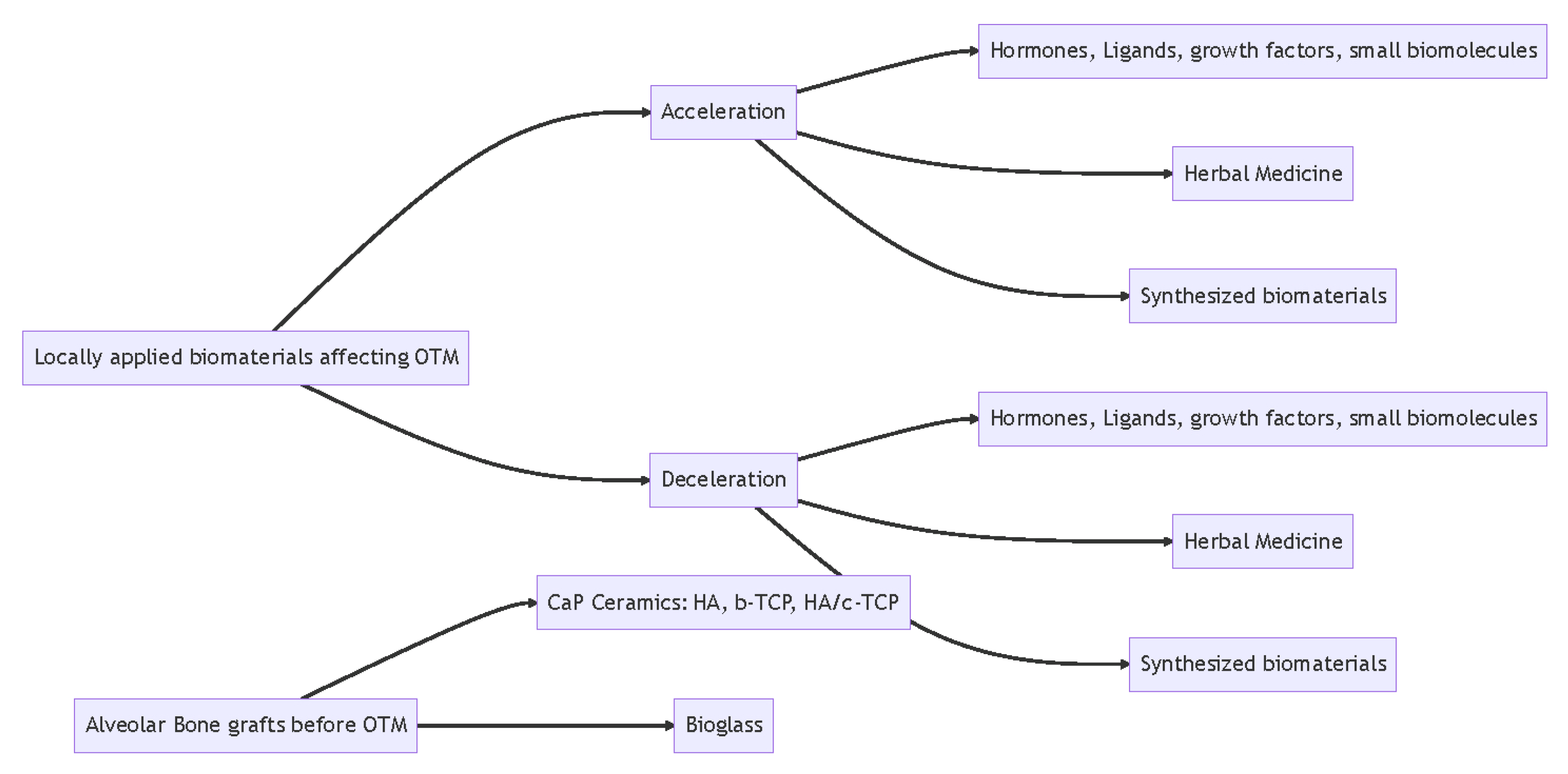
3. Accelerating Orthodontic Tooth Movement
3.1. Hormones, Ligands, Growth Factors, and Biomaterials
3.1.1. Prostaglandin E2
3.1.2. Epidermal Growth Factor
3.1.3. Fibroblast Growth Factor
3.1.4. RANKL
3.1.5. Other Hormones and Growth Factors
3.2. Herbal Medicine Biomaterials
Asperosaponin VI
3.3. Synthetic Biomaterials
Graphene Oxide
4. Decelerating Orthodontic Tooth Movement
4.1. Hormones, Ligands, and Growth Factors
4.1.1. Adiponectin
4.1.2. Osteoprotegerin
4.1.3. Nitric Oxide
4.1.4. Matrix Metalloproteinase Inhibitor: Ilomastat
4.1.5. Hydroxyapatite-Incorporated Advanced Platelet-Rich Fibrin
4.2. Small Molecules or Herbal Medicine
4.2.1. Triptolide
4.2.2. Resveratrol
4.2.3. Sinomenine
4.2.4. Exosomes-Encapsulated Simvastatin
5. Orthodontic Tooth Movement after Bone Grafting
5.1. Calcium Phosphate (CaP) Ceramics: HA, b-TCP, HA/c-TCP
5.1.1. Hydroxyapatite
5.1.2. Beta-Tricalcium Phosphate Ceramic
5.1.3. Biphasic Calcium Phosphate
5.2. Bioglass
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Talic, N.F. Adverse effects of orthodontic treatment: A clinical perspective. Saudi Dent. J. 2011, 23, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Tsichlaki, A.; Chin, S.Y.; Pandis, N.; Fleming, P.S. How long does treatment with fixed orthodontic appliances last? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 308–318. [Google Scholar] [CrossRef]
- Andrade, I., Jr.; dos Santos Sousa, A.B.; da Silva, G.G. New therapeutic modalities to modulate orthodontic tooth movement. Dent. Press J. Orthod. 2014, 19, 123–133. [Google Scholar] [CrossRef]
- Cağlaroğlu, M.; Erdem, A. Histopathologic investigation of the effects of prostaglandin E2 administered by different methods on tooth movement and bone metabolism. Korean J. Orthod. 2012, 42, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.-J.; Wang, X.-X.; Wang, Y.; Chen, P.-P.; Ma, D.; Zhang, J. Effect of akebiasaponin D with different concentrations on orthodontic tooth movement in rats. Shanghai Kou Qiang Yi Xue Shanghai J. Stomatol. 2018, 27, 129–134. [Google Scholar]
- Leiker, B.J.; Nanda, R.S.; Currier, G.F.; Howes, R.I.; Sinha, P.K. The effects of exogenous prostaglandins on orthodontic tooth movement in rats. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Seifi, M.; Eslami, B.; Saffar, A.S. The effect of prostaglandin E2 and calcium gluconate on orthodontic tooth movement and root resorption in rats. Eur. J. Orthod. 2003, 25, 199–204. [Google Scholar] [CrossRef]
- Seifi, M.; Hamedi, R.; Khavandegar, Z. The Effect of Thyroid Hormone, Prostaglandin E2, and Calcium Gluconate on Orthodontic Tooth Movement and Root Resorption in Rats. J. Dent. Shiraz Univ. Med. Sci. 2015, 16 (Suppl. S1), 35–42. [Google Scholar]
- Parcianello, R.G.; Amerio, E.; Giner Tarrida, L.; Nart, J.; Flores Mir, C.; Puigdollers Pérez, A. Local hormones and growth factors to enhance orthodontic tooth movement: A systematic review of animal studies. Orthod. Craniofac. Res. 2022, 25, 281–303. [Google Scholar] [CrossRef]
- Saddi, K.R.G.C.; Alves, G.D.; Paulino, T.P.; Ciancaglini, P.; Alves, J.B. Epidermal Growth Factor in Liposomes May Enhance Osteoclast Recruitment during Tooth Movement in Rats. Angle Orthod. 2008, 78, 604–609. [Google Scholar] [CrossRef]
- Chang, J.H.; Chen, P.-J.; Arul, M.R.; Dutra, E.H.; Nanda, R.; Kumbar, S.G.; Yadav, S. Injectable RANKL sustained release formulations to accelerate orthodontic tooth movement. Eur. J. Orthod. 2020, 42, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.B.; Ferreira, C.L.; Martins, A.F.; Silva, G.A.; Alves, G.D.; Paulino, T.P.; Ciancaglini, P.; Thedei, G., Jr.; Napimoga, M. Local delivery of EGF–liposome mediated bone modeling in orthodontic tooth movement by increasing RANKL expression. Life Sci. 2009, 85, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Seifi, M.; Badiee, M.R.; Abdolazimi, Z.; Amdjadi, P. Effect of basic fibroblast growth factor on orthodontic tooth movement in rats. Cell J. 2013, 15, 230–237. [Google Scholar] [PubMed]
- Crawford, D.; Lau, T.C.; Frost, M.C.; Hatch, N.E. Control of Orthodontic Tooth Movement by Nitric Oxide Releasing Nanoparticles in Sprague-Dawley Rats. Front. Mater. 2022, 9, 811251. [Google Scholar] [CrossRef]
- Sydorak, I.; Dang, M.; Baxter, S.J.; Halcomb, M.; Ma, P.; Kapila, S.; Hatch, N. Microsphere controlled drug delivery for local control of tooth movement. Eur. J. Orthod. 2019, 41, 1–8. [Google Scholar] [CrossRef]
- Liu, X.; Muhammed, F.K.; Liu, Y. Simvastatin encapsulated in exosomes can enhance its inhibition of relapse after orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 881–889. [Google Scholar] [CrossRef]
- Holliday, L.S.; Vakani, A.; Archer, L.; Dolce, C. Effects of Matrix Metalloproteinase Inhibitors on Bone Resorption and Orthodontic Tooth Movement. J. Dent. Res. 2003, 82, 687–691. [Google Scholar] [CrossRef]
- Dunn, M.D.; Park, C.H.; Kostenuik, P.J.; Kapila, S.; Giannobile, W.V. Local delivery of osteoprotegerin inhibits mechanically mediated bone modeling in orthodontic tooth movement. Bone 2007, 41, 446–455. [Google Scholar] [CrossRef]
- Hudson, J.B.; Hatch, N.; Hayami, T.; Shin, J.M.; Stolina, M.; Kostenuik, P.J.; Kapila, S. Local Delivery of Recombinant Osteoprotegerin Enhances Postorthodontic Tooth Stability. Calcif. Tissue Int. 2012, 90, 330–342. [Google Scholar] [CrossRef]
- Schneider, D.A.; Smith, S.M.; Campbell, C.; Hayami, T.; Kapila, S.; Hatch, N.E. Locally limited inhibition of bone resorption and orthodontic relapse by recombinant osteoprotegerin protein. Orthod. Craniofac. Res. 2015, 18, 187–195. [Google Scholar] [CrossRef]
- Yan, T.; Xie, Y.; He, H.; Fan, W.; Huang, F. Role of nitric oxide in orthodontic tooth movement (Review). Int. J. Mol. Med. 2021, 48, 168. [Google Scholar] [CrossRef] [PubMed]
- Alhasyimi, A.A.; Pudyani, P.P.; Asmara, W.; Ana, I.D. Enhancement of post-orthodontic tooth stability by carbonated hydroxyapatite-incorporated advanced platelet-rich fibrin in rabbits. Orthod. Craniofac. Res. 2018, 21, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Wang, X.; Ren, X.; Bu, J.; Zheng, D.; Zhang, J. Asperosaponin VI Injection Enhances Orthodontic Tooth Movement in Rats. Med. Sci. Monit. 2020, 26, e922372. [Google Scholar] [CrossRef]
- Yang, F.; Wang, X.X.; Ma, D.; Cui, Q.; Zheng, D.H.; Liu, X.C.; Zhang, J. Effects of Triptolide on Tooth Movement and Root Resorption in Rats. Drug Des. Dev. Ther. 2019, 13, 3963–3975. [Google Scholar] [CrossRef]
- Liu, X.-C.; Wang, X.-X.; Zhang, L.-N.; Yang, F.; Nie, F.-J.; Zhang, J. Inhibitory effects of resveratrol on orthodontic tooth movement and associated root resorption in rats. Arch. Oral Biol. 2020, 111, 104642. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, Y.; Zou, J.; Yang, Y.; Han, R.; Zhang, J. Sinomenine Inhibits Orthodontic Tooth Movement and Root Resorption in Rats and Enhances Osteogenic Differentiation of PDLSCs. Drug Des. Dev. Ther. 2022, 16, 2949–2965. [Google Scholar] [CrossRef]
- AlSwafeeri, H.; ElKenany, W.; Mowafy, M.; Karam, S. Effect of local administration of simvastatin on orthodontic tooth movement in rabbits. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 75–86. [Google Scholar] [CrossRef]
- Jiao, D.; Wang, J.; Yu, W.; Zhang, K.; Zhang, N.; Cao, L.; Jiang, X.; Bai, Y. Biocompatible reduced graphene oxide stimulated BMSCs induce acceleration of bone remodeling and orthodontic tooth movement through promotion on osteoclastogenesis and angiogenesis. Bioact. Mater. 2022, 15, 409–425. [Google Scholar] [CrossRef]
- Proff, P.; Bayerlein, T.; Fanghänel, J.; Gerike, W.; Bienengräber, V.; Gedrange, T. The application of bone graft substitutes for alveolar ridge preservation after orthodontic extractions and for augmentation of residual cleft defects. Folia Morphol. 2006, 65, 81–83. [Google Scholar]
- Möhlhenrich, S.C.; Kniha, K.; Magnuska, Z.; Hermanns-Sachweh, B.; Gremse, F.; Hölzle, F.; Danesh, G.; Modabber, A. Evaluation of different grafting materials for alveolar cleft repair in the context of orthodontic tooth movement in rats. Sci. Rep. 2021, 11, 13586. [Google Scholar] [CrossRef]
- Krishnan, V.; Davidovitch, Z. On a Path to Unfolding the Biological Mechanisms of Orthodontic Tooth Movement. J. Dent. Res. 2009, 88, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Zainal Ariffin, S.H.; Yamamoto, Z.; Zainol Abidin lntan, Z.; Megat Abdul Wahab, R.; Zainal Ariffin, Z. Cellular and Molecular Changes in Orthodontic Tooth Movement. Sci. World J. 2011, 11, 1788–1803. [Google Scholar] [CrossRef] [PubMed]
- Goulet, G.C.; Cooper, D.M.L.; Coombe, D.; Zernicke, R.F. Influence of cortical canal architecture on lacunocanalicular pore pressure and fluid flow. Comput. Methods Biomech. Biomed. Eng. 2008, 11, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Verborgt, O.; Tatton, N.A.; Majeska, R.J.; Schaffler, M.B. Spatial distribution of Bax and Bcl-2 in osteocytes after bone fatigue: Complementary roles in bone remodeling regulation? J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2002, 17, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Bonewald, L.F. Osteocytes as dynamic multifunctional cells. Ann. N. Y. Acad. Sci. 2007, 1116, 281–290. [Google Scholar] [CrossRef]
- Li, J.; Zhao, Z.; Wang, J.; Chen, G.; Yang, J.; Luo, S. The role of extracellular matrix, integrins, and cytoskeleton in mechanotransduction of centrifugal loading. Mol. Cell. Biochem. 2008, 309, 41–48. [Google Scholar] [CrossRef]
- Schwartz, M.A.; DeSimone, D.W. Cell adhesion receptors in mechanotransduction. Curr. Opin. Cell Biol. 2008, 20, 551–556. [Google Scholar] [CrossRef]
- Takahashi, I.; Nishimura, M.; Onodera, K.; Bae, J.-W.; Mitani, H.; Okazaki, M.; Sasano, Y. Expression of MMP-8 and MMP-13 genes in the periodontal ligament during tooth movement in rats. J. Dent. Res. 2003, 82, 646–651. [Google Scholar] [CrossRef]
- Krishnan, V.; Davidovitch, Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board. Orthod. 2006, 129, 469.e1–469.e32. [Google Scholar] [CrossRef]
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C.-C. Orthodontic tooth movement: The biology and clinical implications. Kaohsiung J. Med Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef]
- Long, H.; Pyakurel, U.; Wang, Y.; Liao, L.; Zhou, Y.; Lai, W. Interventions for accelerating orthodontic tooth movement. Angle Orthod. 2013, 83, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Wise, G.E.; Lin, F.; Fan, W. Localization of epidermal growth factor and its receptor in mandibular molars of the rat prior to and during prefunctional tooth eruption. Dev. Dyn. 1992, 195, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.Z.; Lu, L.; Unsworth, L.D.; Major, P.W.; Doschak, M.R.; Kaipatur, N.R. RANKL release from self-assembling nanofiber hydrogels for inducing osteoclastogenesis in vitro. Acta Biomater. 2017, 49, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.W.K.; Rabie, A.B.M.; Hägg, E.U.O. The effect of crude extract from Radix Dipsaci on bone in mice. Phytother. Res. 2007, 21, 596–598. [Google Scholar] [CrossRef]
- Jiao, D.; Cao, L.; Liu, Y.; Wu, J.; Zheng, A.; Jiang, X. Synergistic Osteogenesis of Biocompatible Reduced Graphene Oxide with Methyl Vanillate in BMSCs. ACS Biomater. Sci. Eng. 2019, 5, 1920–1936. [Google Scholar] [CrossRef]
- Arita, Y.; Kihara, S.; Ouchi, N.; Takahashi, M.; Maeda, K.; Ichiromiyagawa, J.; Hotta, K.; Shimomura, I.; Nakamura, T.; Miyaoka, K.; et al. Paradoxical Decrease of an Adipose-Specific Protein, Adiponectin, in Obesity. Biochem. Biophys. Res. Commun. 1999, 257, 79–83. [Google Scholar] [CrossRef]
- Iwayama, T.; Yanagita, M.; Mori, K.; Sawada, K.; Ozasa, M.; Kubota, M.; Miki, K.; Kojima, Y.; Takedachi, M.; Kitamura, M.; et al. Adiponectin regulates functions of gingival fibroblasts and periodontal ligament cells. J. Periodontal Res. 2012, 47, 563–571. [Google Scholar] [CrossRef]
- Berner, H.S.; Lyngstadaas, S.P.; Spahr, A.; Monjo, M.; Thommesen, L.; Drevon, C.A.; Syversen, U.; Reseland, J.E. Adiponectin and its receptors are expressed in bone-forming cells. Bone 2004, 35, 842–849. [Google Scholar] [CrossRef]
- Lin, Y.Y.; Chen, C.Y.; Chuang, T.Y.; Lin, Y.; Liu, H.Y.; Mersmann, H.J.; Wu, S.C.; Ding, S.T. Adiponectin receptor 1 regulates bone formation and osteoblast differentiation by GSK-3β/β-Catenin signaling in mice. Bone 2014, 64, 147–154. [Google Scholar] [CrossRef]
- Oshima, K.; Nampei, A.; Matsuda, M.; Iwaki, M.; Fukuhara, A.; Hashimoto, J.; Yoshikawa, H.; Shimomura, I. Adiponectin increases bone mass by suppressing osteoclast and activating osteoblast. Biochem. Biophys. Res. Commun. 2005, 331, 520–526. [Google Scholar] [CrossRef]
- Lee, H.W.; Kim, S.Y.; Kim, A.Y.; Lee, E.J.; Choi, J.-Y.; Kim, J.B. Adiponectin Stimulates Osteoblast Differentiation Through Induction of COX2 in Mesenchymal Progenitor Cells. Stem Cells 2009, 27, 2254–2262. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.-P.; Li, X.-P.; Wang, M.; Zhao, L.-L.; Li, H.; Xie, H.; Lu, Z.-Y. Adiponectin exerts its negative effect on bone metabolism via OPG/RANKL pathway: An in vivo study. Endocrine 2014, 47, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.A.; Wang, Y.; Callon, K.E.; Watson, M.; Lin, J.; Lam, J.B.B.; Costa, J.L.; Orpe, A.; Broom, N.; Naot, D.; et al. In Vitro and in Vivo Effects of Adiponectin on Bone. Endocrinology 2009, 150, 3603–3610. [Google Scholar] [CrossRef] [PubMed]
- Haugen, S.; Aasarød, K.M.; Stunes, A.K.; Mosti, M.P.; Franzen, T.; Vandevska-Radunovic, V.; Syversen, U.; Reseland, J.E. Adiponectin prevents orthodontic tooth movement in rats. Arch. Oral Biol. 2017, 83, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M. RANK/RANKL/OPG during orthodontic tooth movement. Orthod. Craniofac. Res. 2009, 12, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Förstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef]
- Yoo, S.-K.; Warita, H.; Soma, K. Duration of orthodontic force affecting initial response of nitric oxide synthase in rat periodontal ligaments. J. Med. Dent. Sci. 2004, 51, 83–88. [Google Scholar]
- Nomura, S.; Tsuru, K.; Maruta, M.; Matsuya, S.; Takahashi, I.; Ishikawa, K. Fabrication of carbonate apatite blocks from set gypsum based on dissolutionprecipitation reaction in phosphate-carbonate mixed solution. Dent. Mater. J. 2014, 33, 166–172. [Google Scholar] [CrossRef]
- Burnouf, T.; Lee, C.-Y.; Luo, C.-W.; Kuo, Y.-P.; Chou, M.-L.; Wu, Y.-W.; Tseng, Y.-H.; Su, C.-Y. Human blood-derived fibrin releasates: Composition and use for the culture of cell lines and human primary cells. Biologicals 2012, 40, 21–30. [Google Scholar] [CrossRef]
- Chen, S.-R.; Dai, Y.; Zhao, J.; Lin, L.; Wang, Y.; Wang, Y. A Mechanistic Overview of Triptolide and Celastrol, Natural Products from Tripterygium wilfordii Hook F. Front. Pharmacol. 2018, 9, 104. [Google Scholar] [CrossRef]
- Li, W.; Gong, K.; Ding, Y.; Chaurasiya, B.; Ni, Y.; Wu, Y.; Zhao, P.; Shen, Y.; Zhang, Z.; Webster, T.J. Effects of triptolide and methotrexate nanosuspensions on left ventricular remodeling in autoimmune myocarditis rats. Int. J. Nanomed. 2019, 14, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Fan, D.; Guo, Q.; Shen, J.; Zheng, K.; Lu, C.; Zhang, G.; Lu, A.; He, X. The Effect of Triptolide in Rheumatoid Arthritis: From Basic Research towards Clinical Translation. Int. J. Mol. Sci. 2018, 19, 376. [Google Scholar] [CrossRef]
- Pangeni, R.; Sahni, J.K.; Ali, J.; Sharma, S.; Baboota, S. Resveratrol: Review on therapeutic potential and recent advances in drug delivery. Expert Opin. Drug Deliv. 2014, 11, 1285–1298. [Google Scholar] [CrossRef] [PubMed]
- Xia, N.; Daiber, A.; Förstermann, U.; Li, H. Antioxidant effects of resveratrol in the cardiovascular system. Br. J. Pharmacol. 2017, 174, 1633–1646. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.L.d.B.; Monteiro, V.V.S.; Navegantes-Lima, K.C.; Reis, J.F.; Gomes, R.D.S.; Rodrigues, D.V.S.; Gaspar, S.L.d.F.; Monteiro, M.C. Resveratrol Role in Autoimmune Disease—A Mini-Review. Nutrients 2017, 9, 1306. [Google Scholar] [CrossRef]
- Jia, R.; Li, Y.; Cao, L.; Du, J.; Zheng, T.; Qian, H.; Gu, Z.; Jeney, G.; Xu, P.; Yin, G. Antioxidative, anti-inflammatory and hepatoprotective effects of resveratrol on oxidative stress-induced liver damage in tilapia (Oreochromis niloticus). Comp. Biochem. Physiol. Part C Toxicol. Pharmacol. 2019, 215, 56–66. [Google Scholar] [CrossRef]
- Zhang, M.-W.; Wang, X.-H.; Shi, J.; Yu, J.-G. Sinomenine in Cardio-Cerebrovascular Diseases: Potential Therapeutic Effects and Pharmacological Evidences. Front. Cardiovasc. Med. 2021, 8, 749113. [Google Scholar] [CrossRef]
- Li, X.-M.; Li, M.-T.; Jiang, N.; Si, Y.-C.; Zhu, M.-M.; Wu, Q.-Y.; Shi, D.-C.; Shi, H.; Luo, Q.; Yu, B. Network Pharmacology-Based Approach to Investigate the Molecular Targets of Sinomenine for Treating Breast Cancer. Cancer Manag. Res. 2021, 13, 1189–1204. [Google Scholar] [CrossRef]
- Zhou, B.; Lu, X.; Tang, Z.; Liu, D.; Zhou, Y.; Zeng, P.; Xiong, H. Influence of sinomenine upon mesenchymal stem cells in osteoclastogenesis. Biomed. Pharmacother. 2017, 90, 835–841. [Google Scholar] [CrossRef]
- Yuana, Y.; Balachandran, B.; van der Wurff-Jacobs, K.M.G.; Schiffelers, R.M.; Moonen, C.T. Potential Use of Extracellular Vesicles Generated by Microbubble-Assisted Ultrasound as Drug Nanocarriers for Cancer Treatment. Int. J. Mol. Sci. 2020, 21, 3024. [Google Scholar] [CrossRef]
- Lu, M.J.J.; Wang, Z.; Zhang, H.; Xu, W.; Zhang, C.; Yang, Y.; Zheng, X.; Xu, J. Bone Graft Materials for Alveolar Bone Defects in Orthodontic Tooth Movement. Tissue Eng. Part B Rev. 2022, 28, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Carmagnola, D.; Berglundh, T.; Thilander, B.; Lindhe, J. Orthodontic movement in bone defects augmented with Bio-OssR. An experimental study in dogs. J. Clin. Periodontol. 2001, 28, 73–80. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Properties of Osteoconductive Biomaterials: Calcium Phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Gedrange, T.; Gredes, T.; Spassow, A.; Mai, R.; Alegrini, S.; Dominiak, M.; Kunert-Keil, C.; Heinemann, F. Orthodontic tooth movement into jaw regions treated with synthetic bone substitute. Ann. Acad. Med. Stetin. 2010, 56, 80–84. [Google Scholar] [PubMed]
- Reichert, C.; Wenghöfer, M.; Götz, W.; Jäger, A. Pilot study on orthodontic space closure after guided bone regeneration. J. Orofac. Orthop. Fortschr. Kieferorthopädie 2011, 72, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Seifi, M.; Arayesh, A.; Shamloo, N.; Hamedi, R. Effect of Nanocrystalline Hydroxyapatite Socket Preservation on Orthodontically Induced Inflammatory Root Resorption. Cell J. 2015, 16, 514–527. [Google Scholar] [CrossRef]
- Hossain, M.Z.; Yamada, T.; Yamauchi, K. Biodegradable ceramic as a bone graft substitute followed by orthodontic tooth movement. Nihon Kyosei Shika Gakkai Zasshi J. Jpn. Orthod. Soc. 1989, 48, 483–495. [Google Scholar]
- Sheats, R.D.; Strauss, R.A.; Rubenstein, L.K. Effect of a resorbable bone graft material on orthodontic tooth movement through surgical defects in the cat mandible. J. Oral Maxillofac. Surg. 1991, 49, 1299–1303. [Google Scholar] [CrossRef]
- Hossain, M.Z.; Kyomen, S.; Tanne, K. Biologic Responses of Autogenous Bone and Beta-tricalcium Phosphate Ceramics Transplanted into Bone Defects to Orthodontic Forces. Cleft Palate Craniofac. J. 1996, 33, 277–283. [Google Scholar] [CrossRef]
- Zhang, F.-F.; Bao, S.-J.; Ye, S.-J.; Wei, B.; Gong, Y. Study of the timing of tooth movement after repair of alveolar bone defects by rabbit BMSCs combined with beta-TCP. Shanghai Kou Qiang Yi Xue Shanghai J. Stomatol. 2019, 28, 231–236. [Google Scholar]
- Zhang, D.; Chu, F.; Yang, Y.; Xia, L.; Zeng, D.; Uludağ, H.; Zhang, X.; Qian, Y.; Jiang, X. Orthodontic Tooth Movement in Alveolar Cleft Repaired with a Tissue Engineering Bone: An Experimental Study in Dogs. Tissue Eng. Part A 2011, 17, 1313–1325. [Google Scholar] [CrossRef]
- Ru, N.; Liu, S.S.-Y.; Bai, Y.; Li, S.; Liu, Y.; Wei, X. BoneCeramic graft regenerates alveolar defects but slows orthodontic tooth movement with less root resorption. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 523–532. [Google Scholar] [CrossRef]
- Attia, M.S.; Shoreibah, E.A.; Ibrahim, S.A.; Nassar, H.A. Regenerative therapy of osseous defects combined with orthodontic tooth movement. J. Int. Acad. Periodontol. 2012, 14, 17–25. [Google Scholar]
- Tanimoto, K.; Sumi, K.; Yoshioka, M.; Oki, N.; Tanne, Y.; Awada, T.; Kato, Y.; Sugiyama, M.; Tanne, K. Experimental Tooth Movement into New Bone Area Regenerated by Use of Bone Marrow–Derived Mesenchymal Stem Cells. Cleft Palate Craniofac. J. 2015, 52, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Möhlhenrich, S.C.; Kniha, K.; Magnuska, Z.; Chhatwani, S.; Hermanns-Sachweh, B.; Gremse, F.; Hölzle, F.; Danesh, G.; Modabber, A. Development of root resorption during orthodontic tooth movement after cleft repair using different grafting materials in rats. Clin. Oral Investig. 2022, 26, 5809–5821. [Google Scholar] [CrossRef] [PubMed]
- Machibya, F.M.; Zhuang, Y.; Guo, W.; You, D.; Lin, S.; Wu, D.; Chen, J. Effects of bone regeneration materials and tooth movement timing on canine experimental orthodontic treatment. Angle Orthod. 2018, 88, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, T.; Wu, G.; Li, W.; Feng, X.; Pathak, J.L.; Shi, J. BMP2-Functionalized Biomimetic Calcium Phosphate Graft Promotes Alveolar Defect Healing During Orthodontic Tooth Movement in Beagle Dogs. Front. Bioeng. Biotechnol. 2020, 8, 517. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Fan, F.Y.; Wang, X.X.; Xing, D.Y.; Wang, S.L. Effect of bioactive glass filling defective alveolar bone on tooth movement. Zhonghua Kou Qiang Yi Xue Za Zhi 2006, 41, 92–93. [Google Scholar]



{kind=link}
{kind=link}
| Author Ref./Year | Sample Size | OTM Model Animal/Force | Biomaterials (Dosage/Route of Administration) | Outcomes |
|---|---|---|---|---|
| Cağlaroğlu M, 2012 [4] | 45 | Rabbit/ 20 g reciprocal force on the maxillary incisor | PGE2 (10 μg/mL /Intravenous, submucosal, or intraligamentous) | 1. Increase in OTM in rabbits receiving submucosal and intraligamentous PGE2 injection, with increased OTM observed in rabbits receiving the intraligamentous injection in comparison to the submucosal injection 2. Root resorption not found to be a statistically significant risk but may still be a risk. |
| Cui J, 2018 [5] | 40 | Wistar rats/40 g mesial force on maxillary first molar | PGE2 (25 μg/kg), akebiasaponin D (5 mg/kg) and (10 mg/kg) | PGE2 injection yielded increased OTM when compared to injection of akebiasaponin D of 5 mg/kg and similar results to injection of akebiasaponin D 10 mg/kg |
| Leiker B, 1995 [6] | 132 | Sprague-Dawley rats/60 g force mesial on the maxillary first molar | PGE2 (0.1, 1, 5, and 10 μg/submucosa | 1. Increased OTM with injection of PGE2 with no statistical significance between groups. 2. Increased root resorption associated with increased number of injections and higher concentrations |
| Seifi M, 2003 [7] | 24 | Wistar rats/60 g force mesial to the maxillary first molar | PGE2 (0.1 mL of 1 mg/mL)/submucosal + 10% Ca (200 mg/kg)/intraperitoneal | 1. PGE2 injection showed increased OTM but PGE2 with Ca showed a higher OTM than the control but less than PGE2 alone 2. No significant difference in root resorption between control, PGE2 or PGE2 and Ca. |
| Seifi M, 2015 [8] | 64 | Wistar rats/60 g force mesial to the maxillary first molar | Thyroxine (20 μg/kg)/intraperitoneal PGE2 (0.1 mL of 1 mg/mL)/submucosal 10% Calcium gluconate (200 mg/kg/intraperitoneal) | 1. Highest OTM observed in thyroxine and PGE2 groups 2. Root resorption observed with statistical difference in PGE2 groups in comparison to others |
| Saddi KR, 2008 [10] | 32 | Holtzman rats/mesial force on the maxillary first molar | EGF within liposome (2 ng/μL) Soluble EGF (2 ng/μL) Liposomes only /submucosal | 1. Highest OTM observed in rats injected with EGF or EGF in liposomes. 2. Statistically significant higher number of osteoclasts recruited in group injected with EGF in liposomes |
| Chang JH, 2020 [11] | 24 | Wistar rats/5–8 g force mesial to maxillary first molar | RANKL (1 μg): microsphere(1 mg) in 3 μL 10% HEC gel/intraosseous through osteoperforation | 1. Increased OTM associated with RANKL injection 2. Decreased tissue density observed but no significant root resorption difference between groups observed |
| Alves JB, 2009 [12] | 96 | Holtzman rats/20 g force mesial to maxillary first molar | Empty liposomes EGF (20 ng) EGF-Liposome(20 ng) /submucosal | EGF-liposome injection was associated with statistically significant increased OTM and osteoclast numbers and RANKL expression |
| Seifi M, 2013 [13] | 50 | Wistar rats/60 g mesial force to maxillary first molar | bFGF (10 ng, 100 ng, and 1000 ng)/ submucosal | Increased OTM associated with bFGF injections and is dose dependent, with 1000 ng bFGF being the most effective |
| Author Ref./Year | Sample Size | OTM Model Animal/Force | Biomaterials (Dosage/Route of Administration) | Outcomes |
|---|---|---|---|---|
| Crawford D, 2022 [14] | 32 | Sprague Dawley rats/ 50 g reciprocal force between maxillary 1st molar and incisors for 18 days | S-nitrosothiol (2.2 mg/kg of S-nitrosothoil containing nanoparticles, in saline/intraperitoneal injection immediately prior to orthodontic appliance activation) | Nitric oxide (NO) released from S-nitrosothiol containing nanoparticles inhibited movement of teeth for 1 week. |
| Sydorak I, 2019 [15] | 42 | Sprague Dawley rats/ 25 g reciprocal force between maxillary 1st molar and incisors for 28 days | OPG (1 mg/kg non-encapsulated or microsphere encapsulated/intraperitoneal injection/single dose injected mesial to maxillary 1st molar one day prior to OTM) | A single injection of microsphere encapsulated OPG significantly enhanced orthodontic anchorage, while a single injection of non-encapsulated OPG did not. |
| Liu X, 2022 [16] | 32 | Sprague Dawley rats/ 50 g reciprocal force between maxillary 1st molar and incisors for 14 days | Simvastatin encapsulated in exosome, simvastatin in saline/submucosal and intraligementary injection | Encapsulating simvastatin into the exosomes derived from PDLSCs improved simvastatin solubility and enhanced the inhibition effect of relapse. |
| Holliday L, 2003 [17] | N/A | Sprague Dawley rats/ 40 g reciprocal force between maxillary 1st molar and incisors for 10 days | Polymer ELVAX40 impregnated with Ilomastat/intraperitoneal injection | In the presence of Ilomastat, tooth movement on day 10 was significantly inhibited. Initial tipping and the lag phase were not significantly different. |
| Alhasyimi A, 2018 [22] | 45 | Rabbits/ 50 cN reciprocal force between lower incisors for 14 days | Carbonated hydroxyapatite-incorporated advanced platelet-rich fibrin (CHA-aPRF)/intrasulcular injection every 7 days | Intrasulcular injection of hydrogel CHA incorporated aPRF locally reduced the orthodontic relapse in rabbits. |
| Yang F, 2019 [24] | 48 | Wistar rats/ 50 g reciprocal force between maxillary 1st molar and incisors for 14 days | Triptolide (30 or 15 µg/kg/day/ intraperitoneal injection) | The amount of tooth movement and the ratio of root resorption area were significantly decreased in the triptolide-treated rats. |
| Liu X, 2020 [25] | 36 | Wistar rats/ 50 g reciprocal force between maxillary 1st molar and incisors for 14 days | Resveratrol (10 or 5 mg/kg/day, dissolved in CMC/gavage) | The RSV groups showed a significant decrease in the distance of OTM and orthodontic induced root resorption ratio. |
| Li H, 2022 [26] | 54 | Wistar rats/ 50 g reciprocal force between maxillary 1st molar and incisors for 14 days | Sinomenine (40 or 20 mg/kg/day/intraperitoneal injection) | The tooth movement and root resorption of sinomenine groups were reduced. |
| Haugen S, 2017 [54] | 24 | Wistar rats/ 0.5 N reciprocal force between maxillary 1st molar and incisors for 14 days | Adiponectin (2 or 0.2 µg every third day for 14 days/intraperitoneal injection) | Submucosal injections of adiponectin prevented experimental tooth movement in rats. The effect was dosage-dependent and local. |
| Author Ref./Year | Sample Size | OTM Model Animal/Force | Grafting Materials | Outcomes |
|---|---|---|---|---|
| Möhlhenrich SC, 2021 [30] | 21 | Wistar Rat/NiTi coil springs (0.14 N) | β-TCP/HA (beta-tricalcium phosphate/hydroxyapatite) vs. Autograft & Human Xenograft | 1. Autograft has the best bone integration and the β-TCP/HA the least 2. OTM has a secondary role in the remodeling process of grafted bone |
| Araujo MG, 2001 [72] | 5 | Beagle Dog/closed coil spring of 30 to 50 cN | Bio-Oss | 1. OTM occurred in grafted site without complication 2. Zone of the ridge with OTM shows degradation of Bio-Oss 3. Zone without OTM inactive filler material remains after 12 months |
| Gedrange T, 2010 [74] | 1 | Pig (Sus scrofa domesticus)/ 1–2 N on each adjacent tooth to the right mandibular premolar | HA (Nano-Bone® of Artoss GmbH, Germany) | 1. OTM through grafted sites could increase the risk of root resorption 2. Different resorption changes at apical, medial, and coronal root sections |
| Reichert C, 2011 [75] | 3 | Human/ NiTi closed coil springs (200 g) | HA (Nano-Bone® of Artoss GmbH, Germany) | 1. Gingival invagination causes delayed OTM in control sites 2. OTM was possible and faster in grafted area without adverse effect (e.g., Root resorption or inflammation) |
| Seifi M, 2015 [76] | 4 | Beagle Dog/NiTi closed coil springs (159 g) | HA (NanoBone® non-sintered porous nano-crystalline hydroxyapatite) | 1. No difference between grafted site compared to non-grafted site on OTM 2. The use of synthetic bone substitute can induce neovascularization and osteogenesis 3. Grafting with HA does not have a major impact on the amount of root resorption post-OTM |
| Hossain MZ, 1989 [77] | 20 | Beagle Dog/Coil spring adjusted to achieve OTM of of 2 mm per month | β-TCP (beta-tricalcium phosphate ceramic; Synthograft®) vs. autogenous PMCB (particulate marrow and cancellous bone) | 1. No significant difference compared to PMCB 2. No adverse effect on OTM |
| Sheats RD, 1991 [78] | 12 | Cat/NiTi close coil spring (100 g) | β-TCP (beta-tricalcium phosphate ceramic; Synthograft®) | 1. No difference between grafted site compared to non-grafted site on OTM |
| Hossain MZ, 1996 [79] | 9 | Beagle Dog/Open coil spring activated to achieve 2 mm OTM per month | β-TCP vs. autogenous PMCB (particulate marrow and cancellous bone) | 1. TCPC exhibits more biodegradability and remodeling ability, resulting in less root resorption compared to PMCB |
| Zhang FF, 2019 [80] | 40 | New Zealand Rabbit/NiTi closed coil springs (80 g) | bMSCs/β-TCP | 1. 8 weeks post -surgery is the best initiation time for OTM |
| Zhang D, 2011 [81] | 6 | Beagle Dog/NiTi closed coil springs (50 g) | bMSCs/β-TCP vs. β-TCP vs. Autograft | 1. Synthetic bone grafts have no effect on OTM bMSCs/β-TCP promotes new bone formation and mineralization compared to β-TCP alone |
| Ru N, 2016 [82] | 40 | Sprague Dawley Rat/NiTi coil springs (10 g) | β-TCP/HA (BoneCeramic Straumann, Basel, Switzerland) vs. natural bovine cancellous bone particles (Bio-Oss; Geistlich Pharma, Wolhusen, Switzerland) | 1. BoneCeramic produces the slowest OTM 2. BonCeramic causes the least root resorption compared to Bio-Oss |
| Attia MS, 2012 [83] | 15 | Human/10–15 g per tooth | Bio-Glass | 1. Combined orthodontic/regenerative therapy promotes periodontal regeneration |
| Tanimoto K, 2015 [84] | 3 | Beagle Dog/Elastic chain (100 g) | MSC+ CAP (bone marrow-derived mesenchymal stem cells + carbonated hydroxyapatite) vs. CAP | 1. MSC+ CAP allows for OTM at a constant rate compared to the CAP grafted site that resulted in OTM at various rate |
| Möhlhenrich SC, 2022 [85] | 21 | Wistar Rat/NiTi coil springs (0.14 N) | β-TCP/HA (beta-tricalcium phosphate/hydroxyapatite) vs. Autograft & Human Xenograft | 1. All three graft materials have a similar effect on OTM and root resorption |
| Machibya SC, 2018 [86] | 24 | Beagle Dog/NiTi closed coil springs (150 g) | β-TCP vs. Bio-Oss | 1. Initiation after 1 month: Bio-Oss has better radiologic features but slower OTM 2. Initiation after 2 months: β-TCP has better radiographic features and faster OTM compared to early OTM in the β-TCP group. |
| Jiang S, 2020 [87] | 9 | Beagle Dog/NiTi closed coil springs (150 g) | BioCaP BMP2-functionalized biomimetic calcium phosphate (BioCaP) vs. deproteinized bovine bone (DBB) | 1. BioCaP graft promotes alveolar bone healing and reduces root resorption during OTM compared to DBB |
| Zhang J, 2006 [88] | 40 | Wistar Rat/NiTi coil springs (0.39 N) | Bio-Glass | 1. Good integration of the bone graft material 2. No difference between grafted site compared to non-grafted site on OTM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.; Fu, M.L.; Harb, I.; Ma, L.X.; Tran, S.D. Functional Biomaterials for Local Control of Orthodontic Tooth Movement. J. Funct. Biomater. 2023, 14, 294. https://doi.org/10.3390/jfb14060294
Lin Y, Fu ML, Harb I, Ma LX, Tran SD. Functional Biomaterials for Local Control of Orthodontic Tooth Movement. Journal of Functional Biomaterials. 2023; 14(6):294. https://doi.org/10.3390/jfb14060294
Chicago/Turabian StyleLin, Yi, Moyu Lara Fu, Ingrid Harb, Lisa Xiaolu Ma, and Simon D. Tran. 2023. "Functional Biomaterials for Local Control of Orthodontic Tooth Movement" Journal of Functional Biomaterials 14, no. 6: 294. https://doi.org/10.3390/jfb14060294