

Collagen Membranes Functionalized with 150 Cycles of Atomic Layer Deposited Titania Improve Osteopromotive Property in Critical-Size Defects Created on Rat Calvaria
 ,
,  , ,
, ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
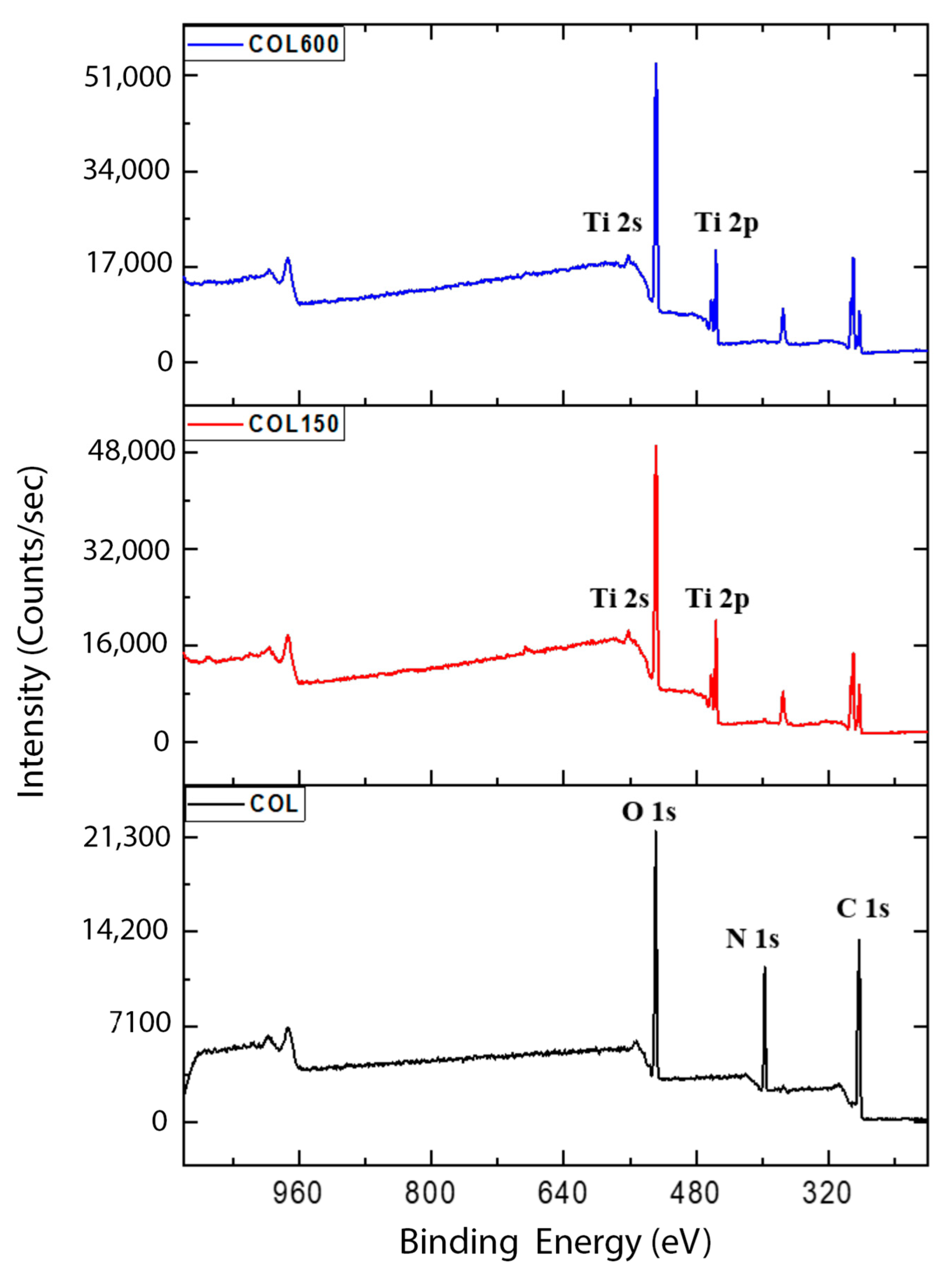
2.1. Sample Preparation and Characterization
2.2. Animal Study
2.2.1. Ethics Statement
2.2.2. Sample Size
2.3. Surgical Procedures
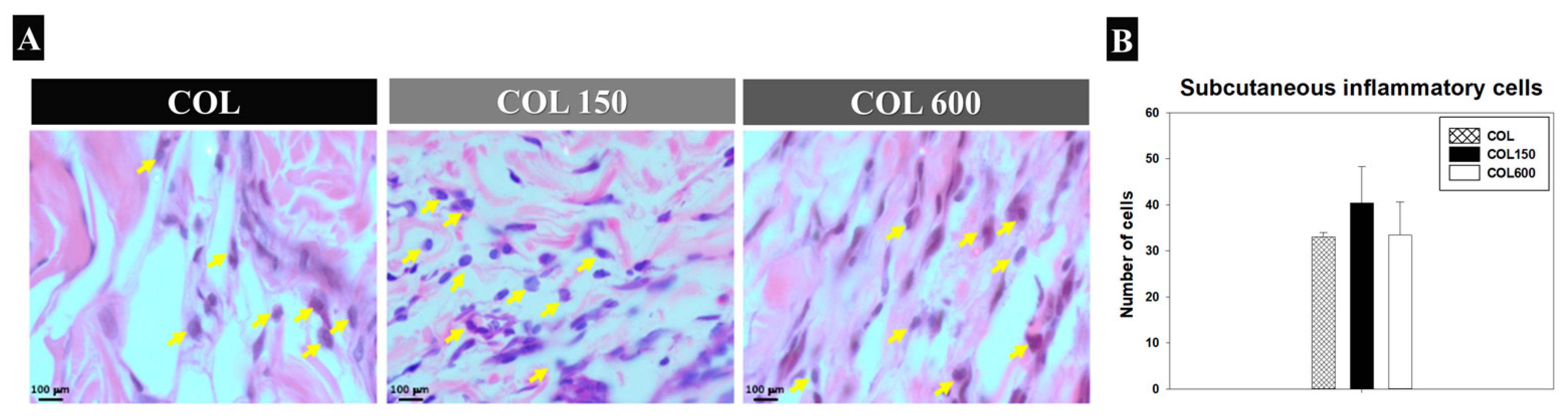
2.3.1. Biocompatibility Assay (Subcutaneous Tissue Behavior around Membranes)
2.3.2. Calvaria Defect
- Blood Clot—BC (Negative group)—n = 9 rats: the bone defects were filled only by the blood clot; 3 rats were euthanized in each period of analysis (7, 14, and 28 days after surgery);
- Collagen Membrane—COL (control group)—n = 9 rats: the bone defects were covered by collagen membrane; 3 rats were euthanized in each period of analysis (7, 14, and 28 days after surgery);
- Collagen Membrane with 150 atomic layer deposition cycles of TiO2—COL150 (test group 1)—n = 9 rats: the bone defects were covered by membrane with 150 atomic layer deposition cycles of TiO2; 3 rats were euthanized in each period of analysis (7, 14, and 28 days after surgery);
- Collagen Membrane with 600 atomic layer deposition cycles of TiO2—COL600 (test group 2):—n = 9 rats: the bone defects were covered by membrane with 600 atomic layer deposition cycles of TiO2; 3 rats were euthanized in each period of analysis (7, 14, and 28 days after surgery).
Critical Size Defect Assay
2.4. Analysis
2.4.1. Biocompatibility Analysis (Subcutaneous Tissue Behavior around Membranes)
2.4.2. Critical Size Defect Assay
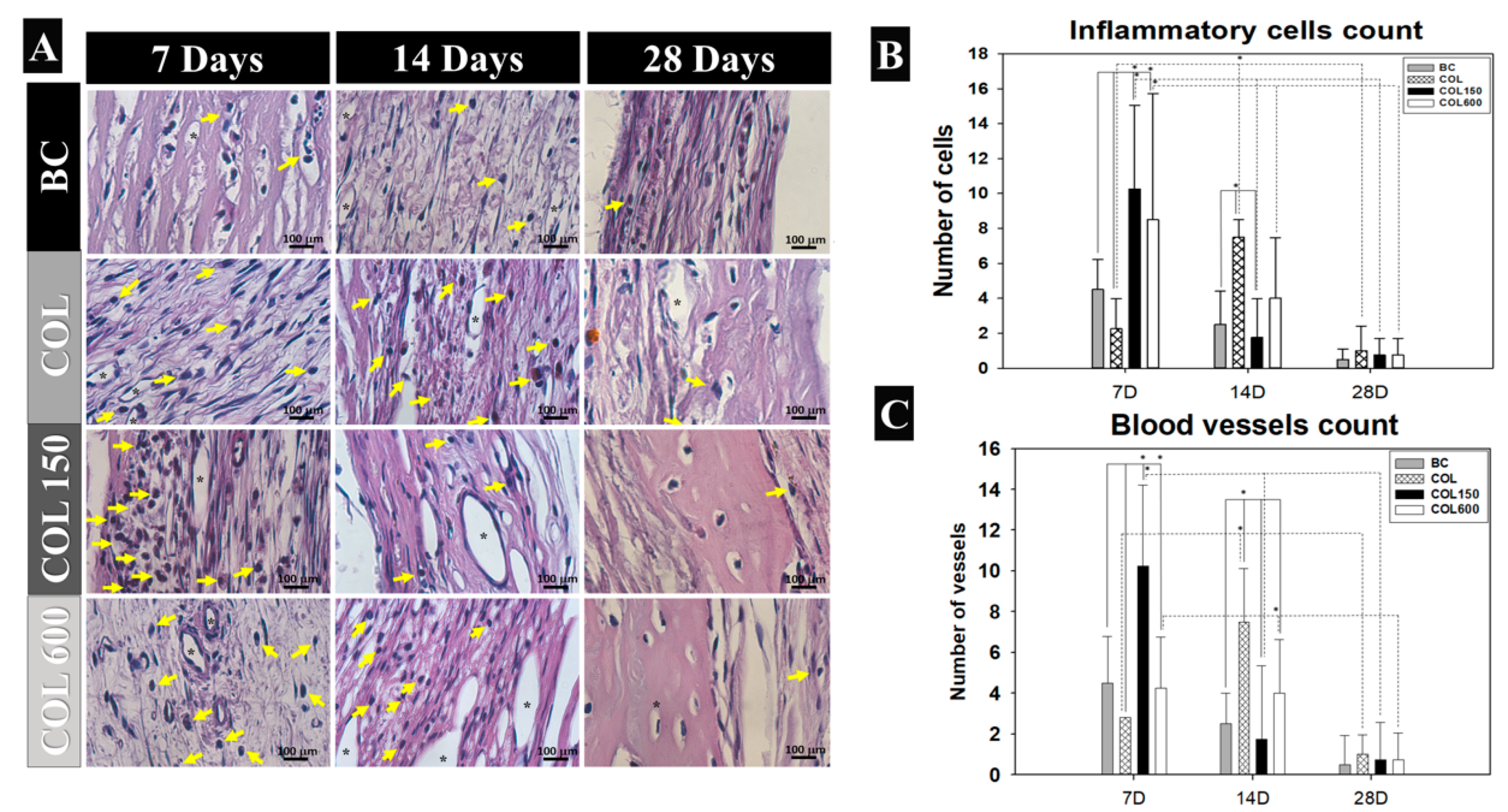
Inflammatory Cells and Blood Cells Count
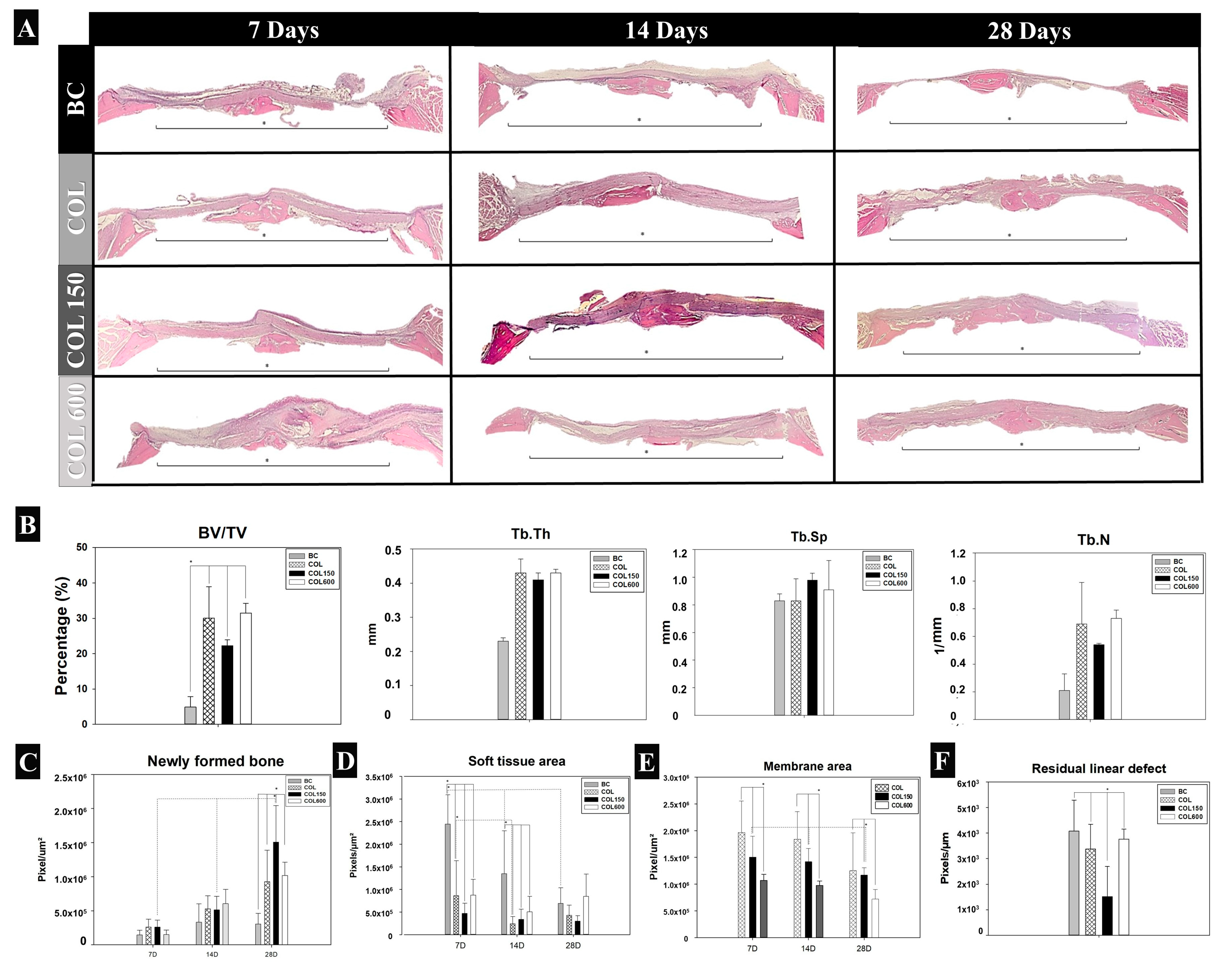
Computed Microtomographic (Micro-CT)
2.4.3. Histometric Analysis
New Bone Formed (NBF)
Soft Tissue Area
Membrane Area
Residual Linear Defect
Statistical Analysis
3. Results
3.1. Biocompatibility Analysis (Subcutaneous Tissue Behavior Around Membranes)
3.2. Inflammatory Cells and Blood Cells Count (Calvaria Defect)
3.3. Panoramic Histological View and Tridimensional Microtomography Assessment (Calvaria)
3.4. New Bone Formed (NBF) (Calvaria)
3.5. Soft Tissue Area (Calvaria)
3.6. Membrane Area (Calvaria)
3.7. Residual Linear Defect (Calvaria)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noia, C.F.; Netto, H.D.M.C.; Lopes, R.O.; Chessa, J.R.; Mazzonetto, R. Use of Autogenous Bone Graft in Oral Cavity Recon-structions. Retrospective Analysis of 07 Years. Rev. Port. Estomatol. Cir. Maxilofac. 2009, 50, 221–225. [Google Scholar] [CrossRef] [Green Version]
- Wernle, J.D.; Damron, T.A.; Allen, M.J. Local irradiation alters bone morphology and increases bone fragility in a mouse model. J. Biomech. 2010, 43, 2738–2746. [Google Scholar] [CrossRef] [PubMed]
- Fliefel, J.R.; Tröltzsch, M.; Kühnisch, J.; Ehrenfeld, M.; Otto, S. Treatment strategies and outcomes of bisphospho-nate-related osteonecrosis of the jaw (BRONJ) with characterization of patients: A systematic review. Int. J. Oral. Maxillofac. Surg. 2015, 44, 568–585. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Helmi, M.F.; Huang, H.; Goodson, J.M.; Hasturk, H.; Tavares, M.; Natto, Z.S. Prevalence of periodontitis and alveolar bone loss in a patient population at Harvard School of Dental Medicine. BMC Oral Health 2019, 19, 254. [Google Scholar] [CrossRef] [Green Version]
- Güll, F.D.; Deppe, H.; Kesting, M.; Schwarzer, C. Periodontal disease-like bone loss after adjuvant radiotherapy in the head and neck region: A case report and review of the literature. Quintessence Int. 2017, 48, 451–457. [Google Scholar] [CrossRef]
- Jensen, S.S. Timing of implant placement after traumatic dental injury. Dent. Traumatol. 2019, 35, 376–379. [Google Scholar] [CrossRef] [Green Version]
- Geckili, O.; Bilhan, H.; Geckili, E.; Cilingir, A.; Mumcu, E.; Bural, C. Evaluation of possible prognostic factors for the success, survival, and failure of dental implants. Implant. Dent. 2014, 23, 44–50. [Google Scholar] [CrossRef]
- Couso-Queiruga, E.; Stuhr, S.; Tattan, M.; Chambrone, L.; Avila-Ortiz, G. Post-extraction dimensional changes: A systematic review and meta-analysis. J. Clin. Periodontol. 2021, 48, 126–144. [Google Scholar] [CrossRef]
- Guilherm, A.S.; Zavanelli, R.A.; Fernandes, J.M.A.; Castro, A.T.; Barros, C.A.; Souza, J.E.A.; Cozac, C.D.; Santos, V.A. Osse-ointegrated implants in areas with maxillary sinus lift and bone grafts. Rev. Gaúcha de Odontol. 2009, 57, 157–163. [Google Scholar]
- Lemos, S.F. Autogenous bone graft with teeth: A literature review. Braz. J. Implantol. Health Sci. 2019, 1, 101–118. [Google Scholar]
- Kim, Y.K. Clinical application and classification of bone graft material according to component. J. Korean Dent. Assoc. 2010, 48, 263–274. [Google Scholar]
- Maciel, J.; Momesso, G.A.; Ramalho-Ferreira, G.; Consolaro, R.B.; de Carvalho, P.S.P.; Faverani, L.P.; Bassi, A.P.F. Bone Healing Evaluation in Critical-Size Defects Treated with Xenogenous Bone Plus Porcine Collagen. Implant Dent. 2017, 26, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Bishal, A.K.; Sukotjo, C.; Jokisaari, J.R.; Klie, R.F.; Takoudis, C.G. Enhanced Bioactivity of Collagen Fiber Functionalized with Room Temperature Atomic Layer Deposited Titania. ACS Appl. Materials Interfaces 2018, 10, 34443–34454. [Google Scholar] [CrossRef]
- Magnusson, S.P.; Heinemeier, K.M.; Kjaer, M. Collagen Homeostasis and Metabolism. Adv. Exp. Med. Biol. 2016, 920, 11–25. [Google Scholar] [CrossRef]
- Meyer, M. Processing of collagen-based biomaterials and the resulting materials properties. Biomed. Eng. Online 2019, 18, 24. [Google Scholar] [CrossRef] [Green Version]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef] [Green Version]
- Khan, R.; Khan, M.H. Use of collagen as a biomaterial: An update. J. Indian Soc. Periodontol. 2013, 17, 539–542. [Google Scholar] [CrossRef]
- Marelli, B.; Ghezzi, C.E.; Barralet, J.E.; Boccaccini, A.R.; Nazhat, S.N. Three- dimensional mineralization of dense nanofibrillar collagen-bioglass hybrid scaffolds. Biomacromolecules 2010, 11, 1470–1479. [Google Scholar] [CrossRef]
- Wahl, D.; Czenuszka, J. Collagen-hydroxyapatite composites or hard tissue repair. Eur. Cell. Mater. 2006, 11, 43–56. [Google Scholar] [CrossRef]
- Ibara, A.; Miyajo, H.; Fugetsu, B.; Nishida, E.; Takita, H.; Tanaka, S.; Sugaya, T.; Kawanami, M. Osteoconductivity and bio-degradability of collagen scaffold coated with nano-β-TCP and fibroblast growth factor 2. J. Nanomater. 2013, 2013, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Biesalski, H.K.; Dragsted, L.O.; Elmadfa, I.; Grossklaus, R.; Muller, M.; Schrenk, D.; Walter, P.; Weber, P. Bioactive compounds: Definition and assessment of activity. Nutrition 2009, 25, 1202–1205. [Google Scholar] [CrossRef] [PubMed]
- Bishal, A.K.; Sukotjo, C.; Takoudis, C.G. Room temperature TiO atomic layer deposition on collagen membrane from a titanium 2 alkylamide precursor. J. Vac. Sci. Technol. 2017, 35, 01B134. [Google Scholar] [CrossRef]
- Liu, L.; Bhatia, R.; Webster, T.J. Atomic layer deposition of nano-TiO2 thin films with enhanced biocompatibility and an-timicrobial activity for orthopedic implants. Int. J. Nanomed. 2017, 12, 8711–8723. [Google Scholar] [CrossRef] [Green Version]
- Grigal, I.P.; Markeey, A.M.; Gudkoya, S.A.; Chernikoya, A.G.; Mityaev, A.S.; Alekhin, A.P. Correlation between bioactivity and structural properties of titanium dioxide coatings grown by atomic layer deposition. Appl. Surf. Sci. 2012, 258, 3415–3419. [Google Scholar] [CrossRef]
- Hashemi Astaneh, S.; Jursich, G.; Sukotjo, C.; Takoudis, C.G. Surface and subsurface film growth of titanium dioxide on polydimethylsiloxane by atomic layer deposition. Appl. Surf. Sci. 2019, 493, 779–786. [Google Scholar] [CrossRef]
- Hyde, G.K.; McCullen, S.D.; Jeon, S.; Stewart, S.M.; Jeon, H.; Loboa, E.G.; Parsons, G.N. Atomic layer deposition and bio-compatibility of titanium nitride nano-coatings on cellulose fiber substrates. Biomed. Mater. 2009, 4, 025001. [Google Scholar] [CrossRef] [PubMed]
- Bishal, A.K.; Anderson, N.D.; Hung, S.K.H.; Jokisaari, J.R.; Klie, R.F.; Koh, A.; Abdussalam, W.; Sukotjo, C.; Takoudis, C.G. Highly Conductive Collagen by Low-Temperature Atomic Layer Deposition of Platinum. ACS Appl. Mater. Interfaces 2020, 12, 44371–44380. [Google Scholar] [CrossRef]
- Shahmohammadi, M.; Yang, B.; Takoudis, C.G. Applications of Titania Atomic Layer Deposition in the Biomedical Field and Recent Updates. Am. J. Biomed. Sci. Res. 2020, 8, 465–468. [Google Scholar]
- Selvaraj, S.K.; Jursich, G.; Takoudis, C.G. Design and implementation of a novel portable atomic layer deposition/chemical vapor deposition hybrid reactor. Rev. Sci. Instrum. 2013, 84, 095109. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. PLoS Biol. 2010, 6, e1000412. [Google Scholar] [CrossRef] [Green Version]
- Zellin, G.; Linde, A. Effects of different osteopromotive membrane porosities on experimental bone neogenesis in rats. Biomaterials 1996, 17, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Farnezi Bassi, A.P.; Ferreira Bizelli, V.; Mello Francatti, T.; Rezende de Moares Ferreira, A.C.; Carvalho Pereira, J.; Al-Sharani, H.M.; de Almeida Lucas, F.; Faverani, L.P. Bone Regeneration Assessment of Polycaprolactone Membrane on Critical-Size Defects in Rat Calvaria. Membranes 2021, 11, 124. [Google Scholar] [CrossRef] [PubMed]
- Ramires, G.A.D.; Helena, J.T.; Oliveira, J.C.S.; Faverani, L.P.; Bassi, A.P.F. Evaluation of Guided Bone Regeneration in Critical Defects Using Bovine and Porcine Collagen Membranes: Histomorphometric and Immunohistochemical Analyses. Int. J. Biomater. 2021, 2021, 8828194. [Google Scholar] [CrossRef] [PubMed]
- Susin, C.; Lee, J.; Fiorini, T.; Koo, K.T.; Schüpbach, P.; Finger Stadler, A.; Wikesjö, U.M. Screening of Hydroxyapatite Biomaterials for Alveolar Augmentation Using a Rat Calvaria Critical-Size Defect Model: Bone Formation/Maturation and Biomaterials Resolution. Biomolecules 2022, 12, 1677. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.A.; Fernandes, K.R.; Parisi, J.R.; Vale, G.C.A.; Junior, S.R.A.; Freitas, F.R.; Sales, A.F.S.; Fortulan, C.A.; Peitl, O.; Zanotto, E.; et al. Marine collagen scaffolds and photobiomodulation on bone healing process in a model of calvaria defects. J. Bone Miner. Metab. 2020, 38, 639–647. [Google Scholar] [CrossRef]
- Reyes, R.; Rodríguez, J.A.; Orbe, J.; Arnau, M.R.; Évora, C.; Delgado, A. Combined sustained release of BMP2 and MMP10 accelerates bone formation and mineralization of calvaria critical size defect in mice. Drug Deliv. 2018, 25, 750–756. [Google Scholar] [CrossRef] [Green Version]
- Silva-Bermudez, P.; Rodil, S.E. An overview of protein adsorption on metal oxide coatings for biomedical implants. Surf. Coat. Technol. 2010, 233, 147–158. [Google Scholar] [CrossRef]
- Al-Maawi, S.; Orlowska, A.; Sander, R.; James Kirkpatrick, C.; Ghanaati, S. In vivo cellular reactions to different biomaterials—Physiological and pathological aspects and their consequences. Semin. Immunol. 2017, 29, 49–61. [Google Scholar] [CrossRef]
- Ziats, N.P.; Miller, K.M.; Anderson, J.M. In vitro and in vivo interactions of cells with biomaterials. Biomaterials 1988, 9, 5–13. [Google Scholar] [CrossRef]
- Hashemi Astaneh, S.; Faverani, L.P.; Sukotjo, C.; Takudis, C.G. Atomic layer deposition on dental materials: Processing conditions and surface functionalization to improve physical, chemical, and clinical properties—A review. Acta Biomater. 2021, 121, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Bizelli, V.F.; Ramos, E.U.; Veras, A.S.C.; Teixeira, G.R.; Faverani, L.P.; Bassi, A.P.F. Calvaria Critical Size Defects Regeneration Using Collagen Membranes to Assess the Osteopromotive Principle: An Animal Study. Membranes 2022, 12, 461. [Google Scholar] [CrossRef] [PubMed]
- Seweryn, A.; Pielok, A.; Lawniczak-Jablonska, K.; Pietruszka, R.; Marcinkowska, K.; Sikora, M.; Witkowski, B.S.; Godlewski, M.; Marycz, K.; Smieszek, A. Zirconium Oxide Thin Films Obtained by Atomic Layer Deposition Technology Abolish the Anti-Osteogenic Effect Resulting from miR-21 Inhibition in the Pre-Osteoblastic MC3T3 Cell Line. Int. J. Nanomed. 2020, 15, 1595–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smieszek, A.; Seweryn, A.; Marcinkowska, K.; Sikora, M.; Lawniczak-Jablonska, K.; Witkowski, B.S.; Kuzmiuk, P.; Godlewski, M.; Marycz, K. Titanium Dioxide Thin Films Obtained by Atomic Layer Deposition Promotes Osteoblasts’ Viability and Differentiation Potential while Inhibiting Osteoclast Activity-Potential Application for Osteo-porotic Bone Regeneration. Materials 2020, 13, 4817. [Google Scholar] [CrossRef]
- Shahmohammadi, M.; Mukherjee, R.; Sukotjo, C.; Diwekar, U.M.; Takoudis, C.G. Recent Advances in Theoretical Development of Thermal Atomic Layer Deposition: A Review. Nanomaterials 2022, 12, 831. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faverani, L.P.; Astaneh, S.H.; Costa, M.G.d.; Delanora, L.A.; Lima-Neto, T.J.; Barbosa, S.; Ariani, M.D.; Takoudis, C.; Sukotjo, C. Collagen Membranes Functionalized with 150 Cycles of Atomic Layer Deposited Titania Improve Osteopromotive Property in Critical-Size Defects Created on Rat Calvaria. J. Funct. Biomater. 2023, 14, 120. https://doi.org/10.3390/jfb14030120
Faverani LP, Astaneh SH, Costa MGd, Delanora LA, Lima-Neto TJ, Barbosa S, Ariani MD, Takoudis C, Sukotjo C. Collagen Membranes Functionalized with 150 Cycles of Atomic Layer Deposited Titania Improve Osteopromotive Property in Critical-Size Defects Created on Rat Calvaria. Journal of Functional Biomaterials. 2023; 14(3):120. https://doi.org/10.3390/jfb14030120
Chicago/Turabian StyleFaverani, Leonardo P., Sarah Hashemi Astaneh, Monique Gonçalves da Costa, Leonardo A. Delanora, Tiburtino J. Lima-Neto, Stéfany Barbosa, Maretaningtias Dwi Ariani, Christos Takoudis, and Cortino Sukotjo. 2023. "Collagen Membranes Functionalized with 150 Cycles of Atomic Layer Deposited Titania Improve Osteopromotive Property in Critical-Size Defects Created on Rat Calvaria" Journal of Functional Biomaterials 14, no. 3: 120. https://doi.org/10.3390/jfb14030120