
Effect of Interbody Implants on the Biomechanical Behavior of Lateral Lumbar Interbody Fusion: A Finite Element Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Finite Element Model of the Lumbar Spine
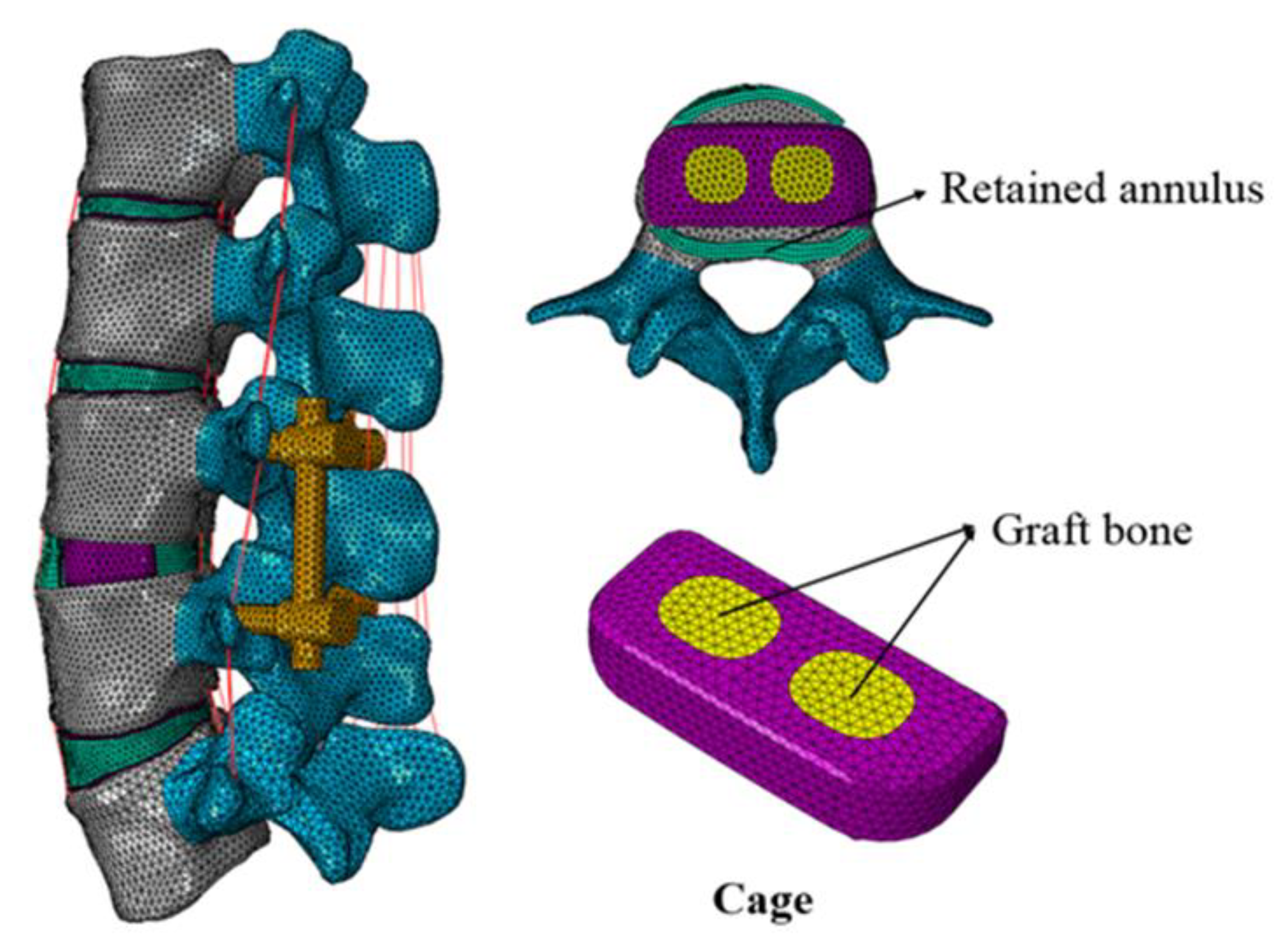
2.2. Finite Element Models of L3-4 Lateral Interbody Fusion Construct
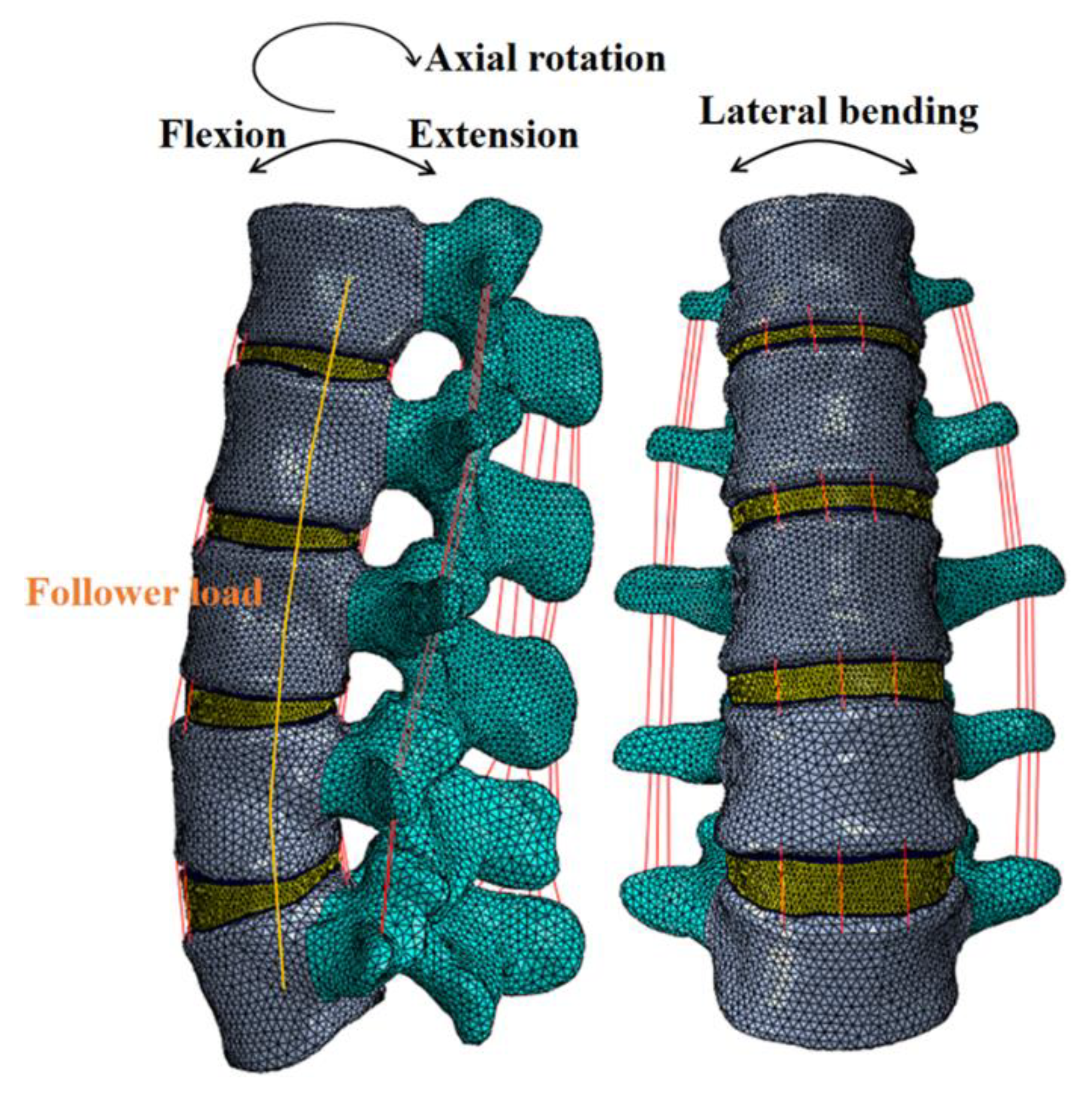
2.3. Boundary and Loading Conditions
3. Results
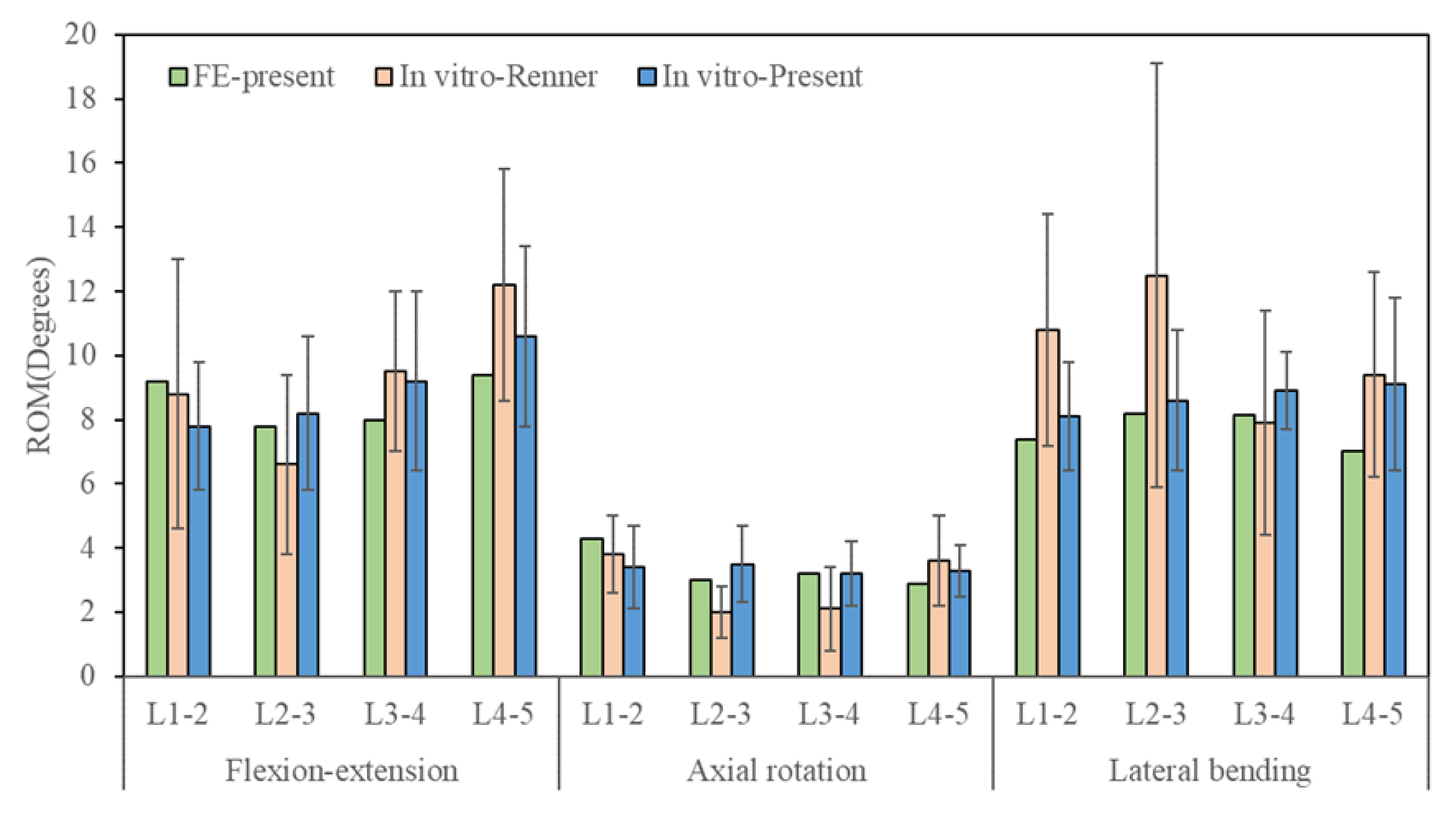
3.1. Model Validation
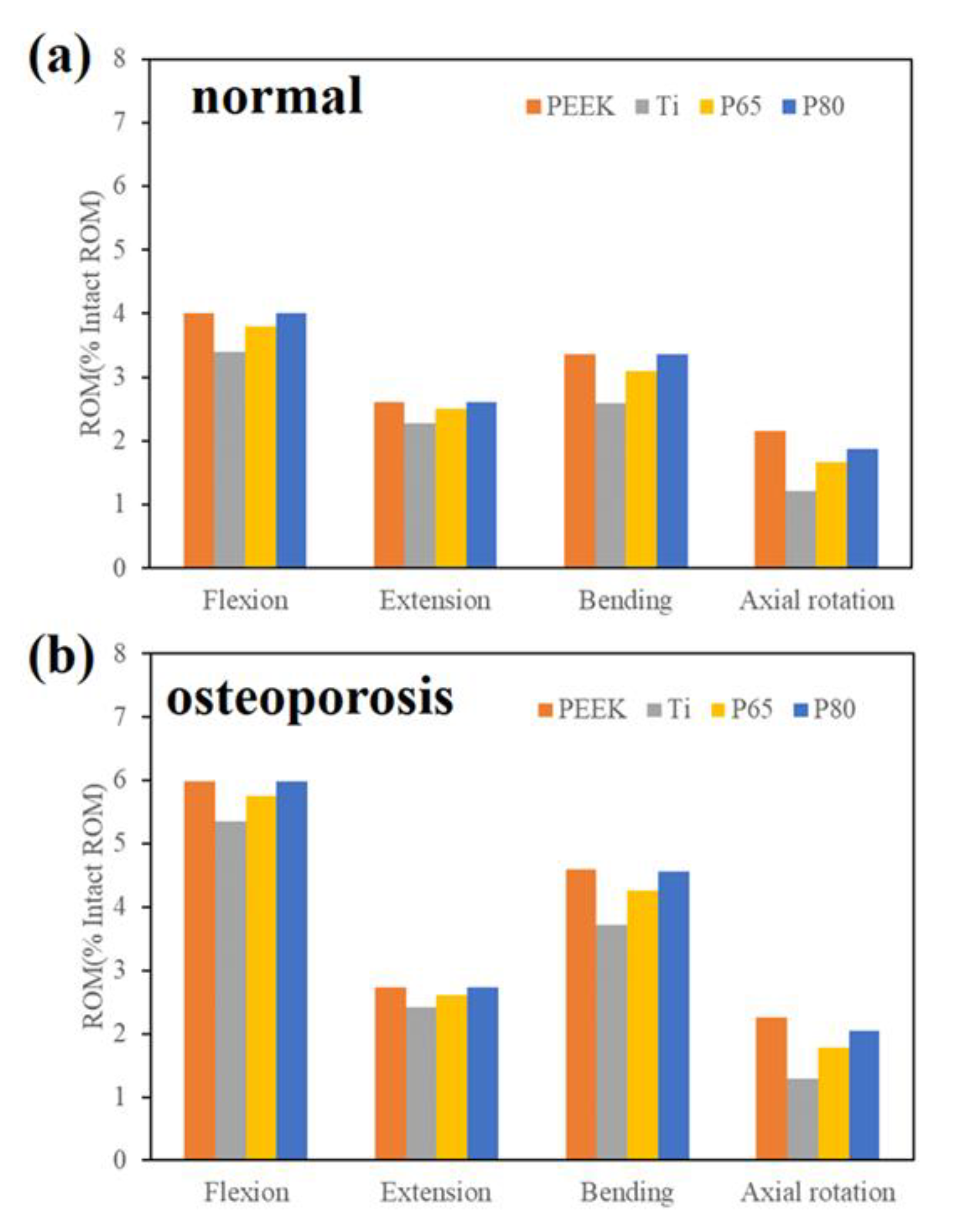
3.2. ROM of the Surgical Segment
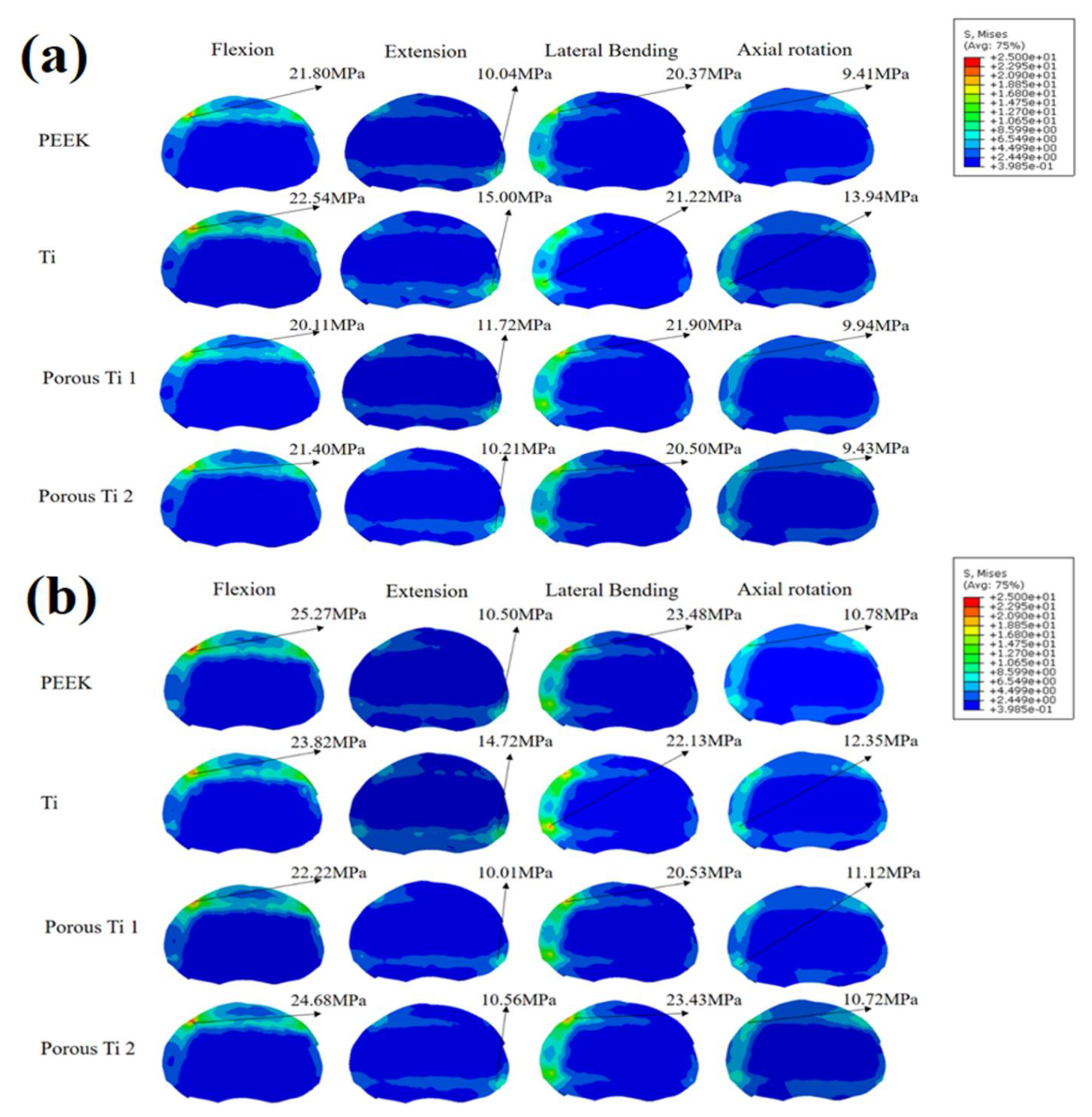
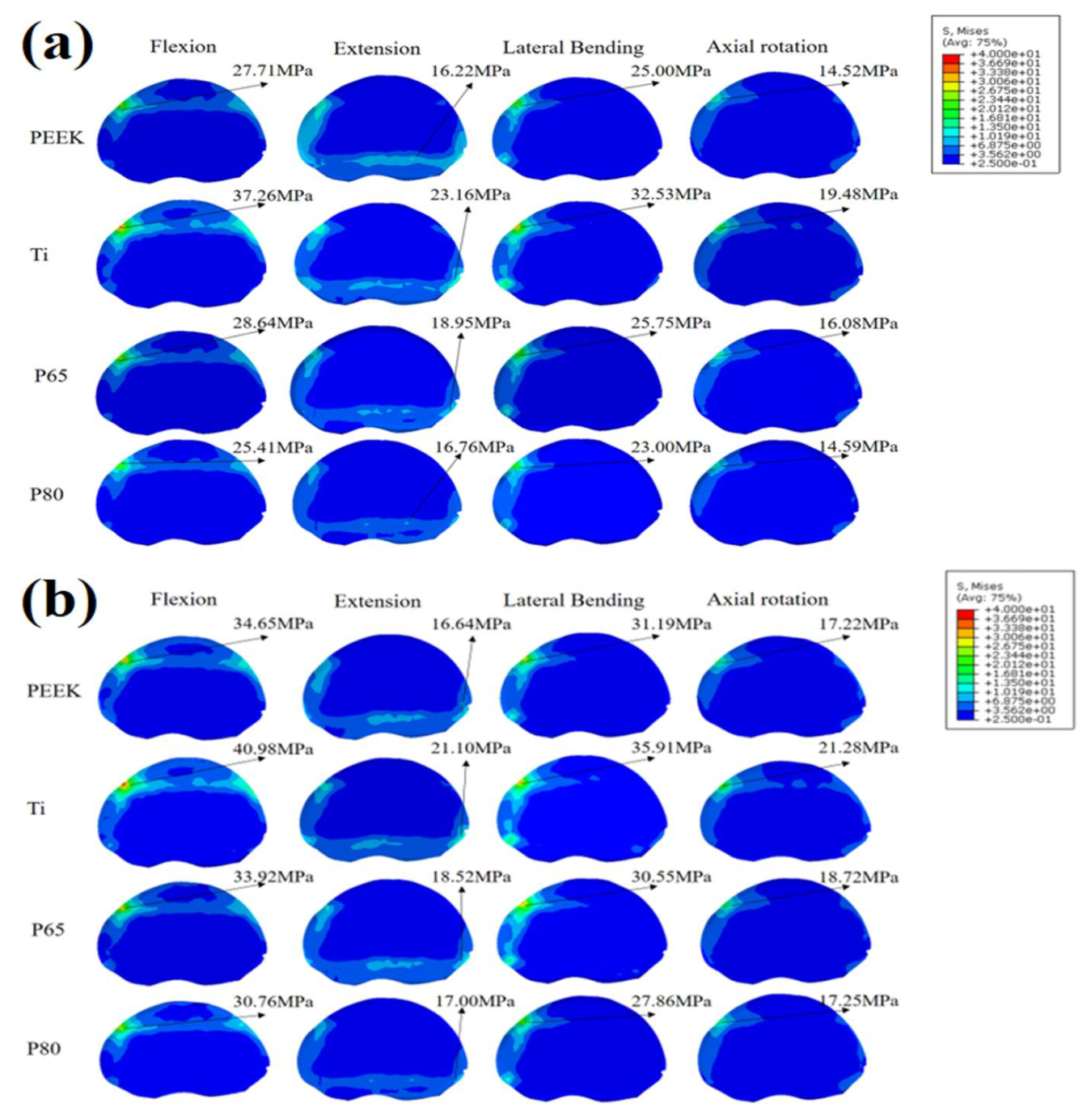
3.3. Endplate Stress
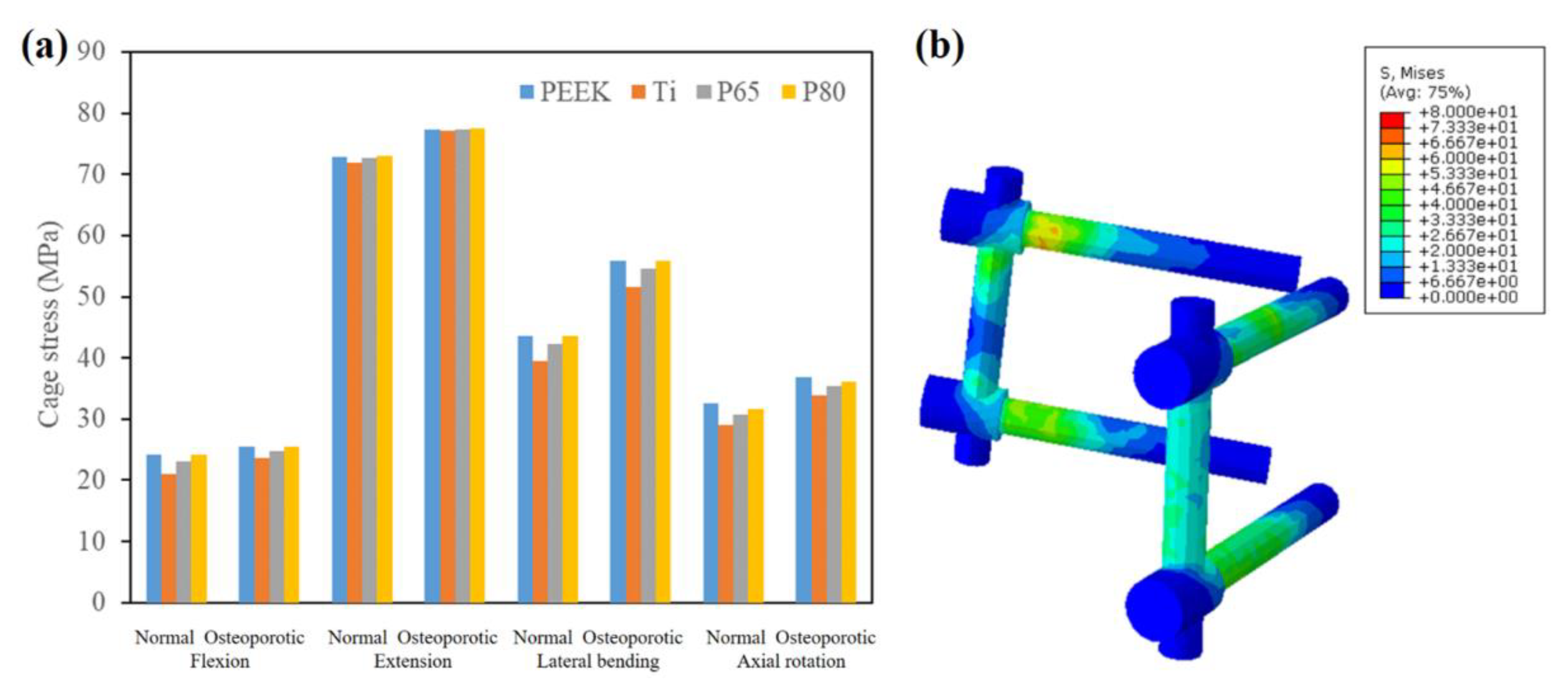
3.4. Scaffold Stress
3.5. Pedicle Screw Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tan, J.-H.; Cheong, C.K.; Hey, H.W.D. Titanium (Ti) scaffolds may be superior to polyetheretherketone (PEEK) scaffolds in lumbar interbody fusion: A systematic review and meta-analysis of clinical and radiological outcomes of spinal interbody fusions using Ti versus PEEK scaffolds. Eur. Spine J. 2021, 30, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- Perez-Orribo, L.; Kalb, S.; Reyes, P.M.; Chang, S.W.; Crawford, N.R. Biomechanics of Lumbar Cortical Screw-Rod Fixation Versus Pedicle Screw-Rod Fixation with and Without Interbody Support. Spine 2013, 38, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Massaad, E.; Fatima, N.; Kiapour, A.; Hadzipasic, M.; Shankar, G.M.; Shin, J.H. Polyetheretherketone Versus Titanium Scaffolds for Posterior Lumbar Interbody Fusion: Meta-Analysis and Review of the Literature. Neurospine 2020, 17, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Lu, T.; Ren, J.; Sun, Z.; Zhang, J.; Xu, K.; Sun, L.; Yang, P.; Wang, D.; Lian, Y.; Zhai, J.; et al. Relationship between the elastic modulus of the scaffold material and the biomechanical properties of transforaminal lumbar interbody fusion: A logarithmic regression analysis based on parametric finite element simulations. Comput. Methods Programs Biomed. 2022, 214, 106570. [Google Scholar] [CrossRef] [PubMed]
- Seaman, S.; Kerezoudis, P.; Bydon, M.; Torner, J.C.; Hitchon, P.W. Titanium vs. polyetheretherketone (PEEK) interbody fusion: Meta-analysis and review of the literature. J. Clin. Neurosci. 2017, 44, 23–29. [Google Scholar] [CrossRef]
- Schnake, K.J.; Fleiter, N.; Hoffmann, C.; Pingel, A.; Scholz, M.; Langheinrich, A.; Kandziora, F. P LIF surgery with titanium-coated PEEK or uncoated PEEK scaffolds: A prospective randomised clinical and radiological study. Eur. Spine J. 2021, 30, 114–121. [Google Scholar] [CrossRef]
- Olivares-Navarrete, R.; Gittens, R.A.; Schneider, J.M.; Hyzy, S.L.; Haithcock, D.A.; Ullrich, P.F.; Schwartz, Z.; Boyan, B.D. Osteoblasts exhibit a more differentiated phenotype and increased bone morphogenetic protein production on titanium alloy substrates than on poly-ether-ether-ketone. Spine J. 2012, 12, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-N.; Chang, C.-W. Computational comparison of three different scaffold porosities in posterior lumbar interbody fusion with porous scaffold. Comput. Biol. Med. 2021, 139, 105036. [Google Scholar] [CrossRef]
- Wang, H.; Wan, Y.; Li, Q.; Xia, Y.; Liu, X.; Liu, Z.; Li, X. Porous fusion scaffold design via integrated global-local topology optimization and biomechanical analysis of performance. J. Mech. Behav. Biomed. Mater. 2020, 112, 103982. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Chung, C.-J.; Wang, C.-W.; Peng, Y.-T.; Chang, C.-H.; Chen, C.-H.; Chen, Y.-N.; Li, C.-T. Computational comparison of three posterior lumbar interbody fusion techniques by using porous titanium interbody scaffolds with 50% porosity. Comput. Biol. Med. 2016, 71, 35–45. [Google Scholar] [CrossRef]
- Zhang, N.-Z.; Xiong, Q.-S.; Yao, J.; Liu, B.-L.; Zhang, M.; Cheng, C.-K. Biomechanical changes at the adjacent segments induced by a lordotic porous interbody fusion scaffold. Comput. Biol. Med. 2022, 143, 105320. [Google Scholar] [CrossRef] [PubMed]
- Makino, T.; Takaneka, S.; Sakai, Y.; Yoshikawa, H.; Kaito, T. Impact of mechanical stability on the progress of bone ongrowth on the frame surfaces of a titanium-coated PEEK scaffold and a 3D porous titanium alloy scaffold: In vivo analysis using CT color mapping. Eur. Spine J. 2021, 30, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Meena, V.K.; Kalra, P.; Sinha, R.K. Finite element study on the influence of pore size and structure on stress shielding effect of additive manufactured spinal scaffold. Comput. Methods Biomech. Biomed. Eng. 2022, 25, 566–577. [Google Scholar] [CrossRef]
- Tsuruga, E.; Takita, H.; Itoh, H.; Wakisaka, Y.; Kuboki, Y. Pore size of porous hydroxyapatite as the cell-substratum controls BMP-induced osteogenesis. J. Biochem. 1997, 121, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, P.-I.; Hsu, C.-C.; Chen, S.-Y.; Wu, T.-H.; Huang, C.-C. Biomechanical investigation into the structural design of porous additive manufactured scaffolds using numerical and experimental approaches. Comput. Biol. Med. 2016, 76, 14–23. [Google Scholar] [CrossRef]
- Song, S.; Guo, Y.; Yang, Y.; Fu, D. Advances in pathogenesis and therapeutic strategies for osteoporosis. Pharmacol. Ther. 2022, 237, 108168. [Google Scholar] [CrossRef]
- Kang, S.; Park, C.-H.; Jung, H.; Lee, S.; Min, Y.-S.; Kim, C.-H.; Cho, M.; Jung, G.-H.; Kim, D.-H.; Kim, K.-T.; et al. Analysis of the physiological load on lumbar vertebrae in patients with osteoporosis: A finite-element study. Sci. Rep. 2022, 12, 11001. [Google Scholar] [CrossRef]
- Wang, Z.; Ma, R.; Cai, Z.; Wang, Z.; Yang, S.; Ge, Z. Biomechanical Evaluation of Stand-Alone Oblique Lateral Lumbar Interbody Fusion Under 3 Different Bone Mineral Density Conditions: A Finite Element Analysis. World Neurosurg. 2021, 155, E285–E293. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Shahnazari, M.; Orwoll, E.S.; Lane, N.E. Osteoporosis in men: Findings from the Osteoporotic Fractures in Men Study (MrOS). Ther. Adv. Musculoskelet. Dis. 2016, 8, 15–27. [Google Scholar] [CrossRef]
- Zhu, J.; Shen, H.; Cui, Y.; Fogel, G.R.; Liao, Z.; Liu, W. Biomechanical Evaluation of Transforaminal Lumbar Interbody Fusion with Coflex-F and Pedicle Screw Fixation: Finite Element Analysis of Static and Vibration Conditions. Orthop. Surg. 2022, 14, 2339–2349. [Google Scholar] [CrossRef]
- Choi, J.; Shin, D.-A.; Kim, S. Biomechanical Effects of the Geometry of Ball-and-Socket Artificial Disc on Lumbar Spine. Spine 2017, 42, E332–E339. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Guo, L.-X.; Zhao, D. Posterior Lumbar Interbody Fusion Versus Transforaminal Lumbar Interbody Fusion: Finite Element Analysis of the Vibration Characteristics of Fused Lumbar Spine. World Neurosurg. 2021, 150, E81–E88. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, H.; Fogel, G.R.; Liao, Z.; Li, Y.; Liu, W. Biomechanical Analysis of Porous Additive Manufactured Scaffolds for Lateral Lumbar Interbody Fusion: A Finite Element Analysis. World Neurosurg. 2018, 111, E581–E591. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, H.; Fogel, G.R.; Xiang, D.; Liao, Z.; Liu, W. Finite element model predicts the biomechanical performance of transforaminal lumbar interbody fusion with various porous additive manufactured scaffolds. Comput. Biol. Med. 2018, 95, 167–174. [Google Scholar] [CrossRef]
- Fan, W.; Guo, L.-X.; Zhang, M. Biomechanical analysis of lumbar interbody fusion supplemented with various posterior stabilization systems. Eur. Spine J. 2021, 30, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Renner, S.M.; Natarajan, R.N.; Patwardhan, A.G.; Havey, R.M.; Voronov, L.I.; Guo, B.Y.; Andersson, G.B.J.; An, H.S. Novel model to analyze the effect of a large compressive follower pre-load on range of motions in a lumbar spine. J. Biomech. 2007, 40, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.-D.; Guo, L.-X. Biomechanical role of cement augmentation in the vibration characteristics of the osteoporotic lumbar spine after lumbar interbody fusion. J. Mater. Sci. -Mater. Med. 2022, 33, 52. [Google Scholar] [CrossRef]
- Li, J.; Xu, W.; Zhang, X.; Xi, Z.; Xie, L. Biomechanical role of osteoporosis affects the incidence of adjacent segment disease after percutaneous transforaminal endoscopic discectomy. J. Orthop. Surg. Res. 2019, 14, 131. [Google Scholar] [CrossRef]
- Liu, Z.-X.; Gao, Z.-W.; Chen, C.; Liu, Z.-Y.; Cai, X.-Y.; Ren, Y.-N.; Sun, X.; Ma, X.-L.; Du, C.-F.; Yang, Q. Effects of osteoporosis on the biomechanics of various supplemental fixations co-applied with oblique lumbar interbody fusion (OLIF): A finite element analysis. BMC Musculoskelet. Disord. 2022, 23, 794. [Google Scholar] [CrossRef]
- Liu, X.; Ma, J.; Park, P.; Huang, X.; Xie, N.; Ye, X. Biomechanical comparison of multilevel lateral interbody fusion with and without supplementary instrumentation: A three-dimensional finite element study. BMC Musculoskelet. Disord. 2017, 18, 63. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Griffith, J.F.; Leung, P.C.; Lee, R. Effect of Osteoporosis on Morphology and Mobility of the Lumbar Spine. Spine 2009, 34, E115–E121. [Google Scholar] [CrossRef] [PubMed]
- Rastegar, S.; Arnoux, P.-J.; Wang, X.; Aubin, C.-E. Biomechanical analysis of segmental lumbar lordosis and risk of scaffold subsidence with different scaffold heights and alternative placements in transforaminal lumbar interbody fusion. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, Y.; Chon, T.E.; Baker, J.S.; Gu, Y. Analysis of stress and stabilization in adolescent with osteoporotic idiopathic scoliosis: Finite element method. Comput. Methods Biomech. Biomed. Eng. 2022, 26, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Guo, L.-X.; Zhao, D. Stress analysis of the implants in transforaminal lumbar interbody fusion under static and vibration loadings: A comparison between pedicle screw fixation system with rigid and flexible rods. J. Mater. Sci.-Mater. Med. 2019, 30, 118. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.S.; Lee, K.J.; Kwon, Y.B.; Kang, K.C. Characteristics and Efficacy of a New 3-Dimensional Printed Mesh Structure Titanium Alloy Spacer for Posterior Lumbar Interbody Fusion. Orthopedics 2017, 40, 880–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amini, D.A.; Moser, M.; Oezel, L.; Zhu, J.; Okano, I.; Shue, J.; Sama, A.A.; Cammisa, F.P.; Girardi, F.P.; Hughes, A.P. Early Outcomes of Three-Dimensional–Printed Porous Titanium versus Polyetheretherketone Cage Implantation for Stand-Alone Lateral Lumbar Interbody Fusion in the Treatment of Symptomatic Adjacent Segment Degeneration. World Neurosurg. 2022, 162, 14–20. [Google Scholar] [CrossRef]
- Tsai, P.I.; Wu, M.H.; Li, Y.Y.; Lin, T.H.; Tsai, J.S.C.; Huang, H.I.; Lai, H.J.; Lee, M.H.; Chen, C.Y. Additive-manufactured Ti-6Al-4V/Polyetheretherketone composite porous cage for Interbody fusion: Bone growth and biocompatibility evaluation in a porcine model. BMC Musculoskelet. Disord. 2021, 22, 171. [Google Scholar] [CrossRef]
- McGilvray, K.C.; Easley, J.; Seim, H.B.; Regan, D.; Berven, S.H.; Hsu, W.K.; Mroz, T.E.; Puttlitz, C.M. Bony ingrowth potential of 3D-printed porous titanium alloy: A direct comparison of interbody cage materials in an in vivo ovine lumbar fusion model. Spine J. 2018, 18, 1250–1260. [Google Scholar] [CrossRef] [Green Version]
- Toop, N.; Gifford, C.; Motiei-Langroudi, R.; Farzadi, A.; Boulter, D.; Forghani, R.; Farhadi, H.F. Can activated titanium interbody cages accelerate or enhance spinal fusion? A review of the literature and a design for clinical trials. J. Mater. Sci.-Mater. Med. 2021, 33, 1. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent segment disease after lumbar or lumbosacral fusion: Review of the literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef]
- Guo, L.X.; Fan, W. Dynamic Response of the Lumbar Spine to Whole-body Vibration Under a Compressive Follower Preload. Spine 2018, 43, 143–153. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Young’s Modulus (MPa) | Poisson Ratio | Cross-Sectional Area (mm2) | References |
|---|---|---|---|---|
| Cortical bone | 12,000 (osteoporosis:8040) | 0.3 | - | [23] |
| Cancellous bone | 100 (osteoporosis:34) | 0.2 | - | [23] |
| Posterior bone | 3500 (osteoporosis:2345) | 0.25 | - | [21] |
| Endplate | 24 (osteoporosis:16.1) | 0.25 | - | [30] |
| Nucleus pulposus | 1 | 0.49 | - | [23] |
| Annulus fibrosus | 4.2 | 0.45 | - | [23] |
| Anterior longitudinal | 20 | 0.3 | 63.7 | [21] |
| Posterior longitudinal | 20 | 0.3 | 20 | |
| Ligament flava | 19.5 | 0.3 | 40 | |
| Interspinal | 11.6 | 0.3 | 40 | |
| Supraspinal | 15 | 0.3 | 30 | |
| Intertransverse | 58.7 | 0.3 | 3.6 | |
| Capsular | 32.9 | 0.3 | 60 | |
| PEEK | 3500 | 0.3 | - | [23] |
| Ti6Al4V | 110,000 | 0.3 | - | [23] |
| 65% porous Ti | 8800 | 0.05 | - | Experiment |
| 80% porous Ti | 5000 | 0.05 | - | Experiment |
| Graft Bone | 3500 | 0.25 | - | [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, H.; Zhu, J.; Huang, C.; Xiang, D.; Liu, W. Effect of Interbody Implants on the Biomechanical Behavior of Lateral Lumbar Interbody Fusion: A Finite Element Study. J. Funct. Biomater. 2023, 14, 113. https://doi.org/10.3390/jfb14020113
Shen H, Zhu J, Huang C, Xiang D, Liu W. Effect of Interbody Implants on the Biomechanical Behavior of Lateral Lumbar Interbody Fusion: A Finite Element Study. Journal of Functional Biomaterials. 2023; 14(2):113. https://doi.org/10.3390/jfb14020113
Chicago/Turabian StyleShen, Hangkai, Jia Zhu, Chenhui Huang, Dingding Xiang, and Weiqiang Liu. 2023. "Effect of Interbody Implants on the Biomechanical Behavior of Lateral Lumbar Interbody Fusion: A Finite Element Study" Journal of Functional Biomaterials 14, no. 2: 113. https://doi.org/10.3390/jfb14020113