
Clinical and Biochemical Evaluation of the Use of Alb-PRF versus L-PRF in Mandibular Third Molar Extractions: A Split-Mouth Randomized Clinical Trial
 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Eligibility Criteria
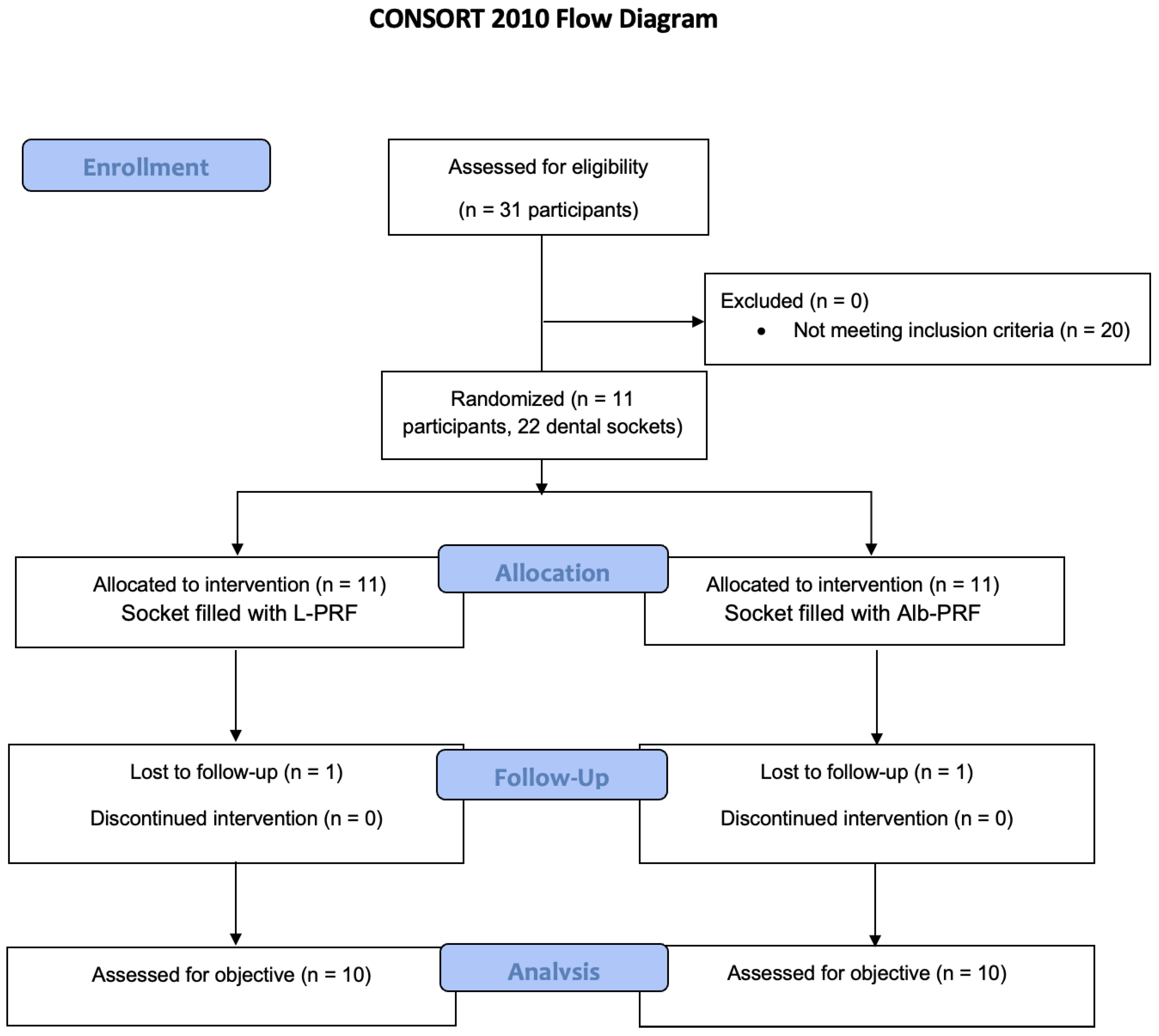
2.3. Sample Size Calculation, Randomization, and Blinding
2.4. Preparation of Platelet Concentrates
2.4.1. L-PRF Preparation (Control Group)
2.4.2. Alb-PRF Preparation
2.5. Surgical Procedures
2.6. Postoperative Evaluation
2.7. Assessment of the In Vitro Release of Biological Mediators by Alb-PRF and L-PRF Membranes
2.8. Evaluation of Cytokines and Growth Factors in the Surgical Sites
2.9. Statistical Analysis
3. Results
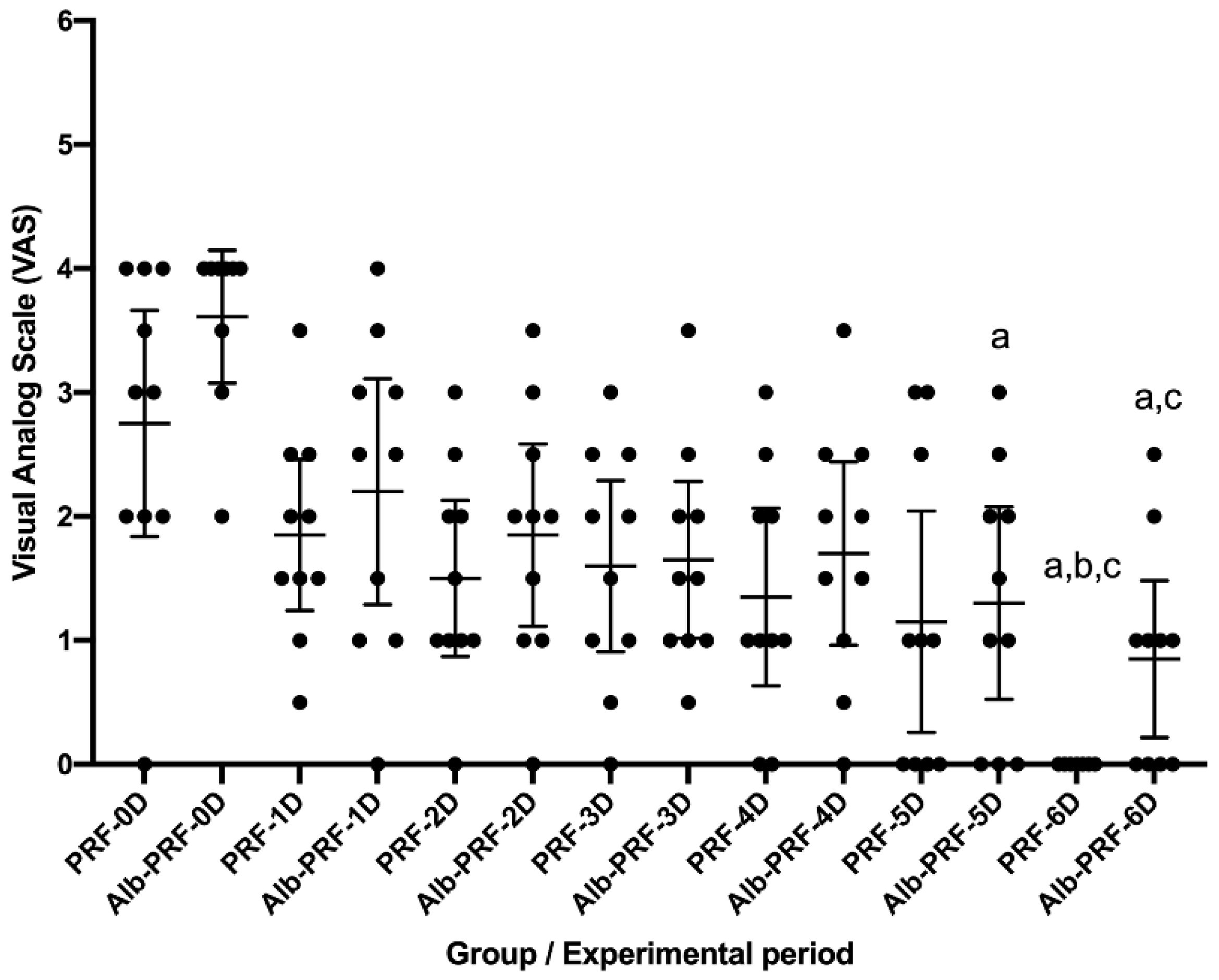
3.1. Pain
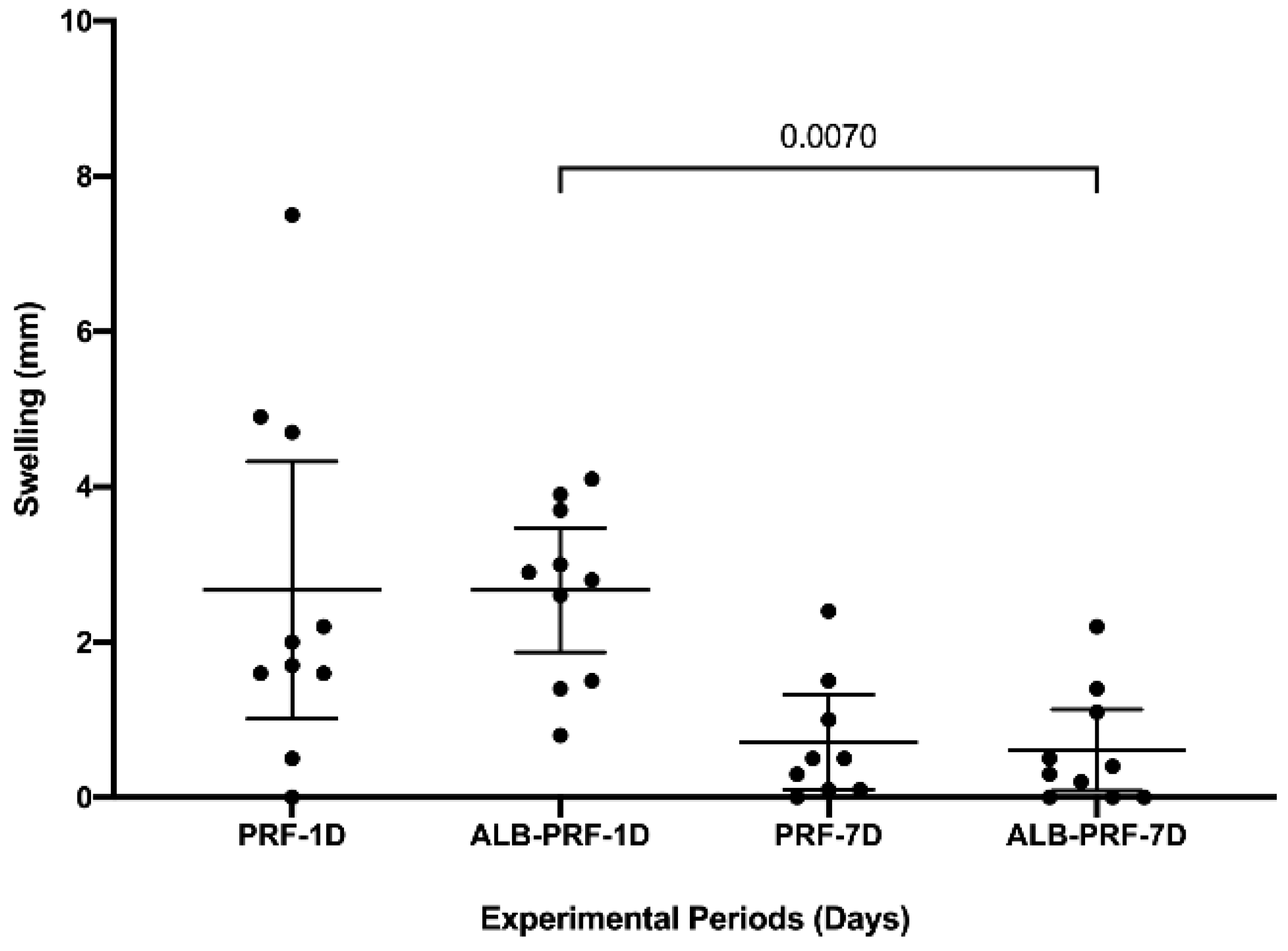
3.2. Swelling
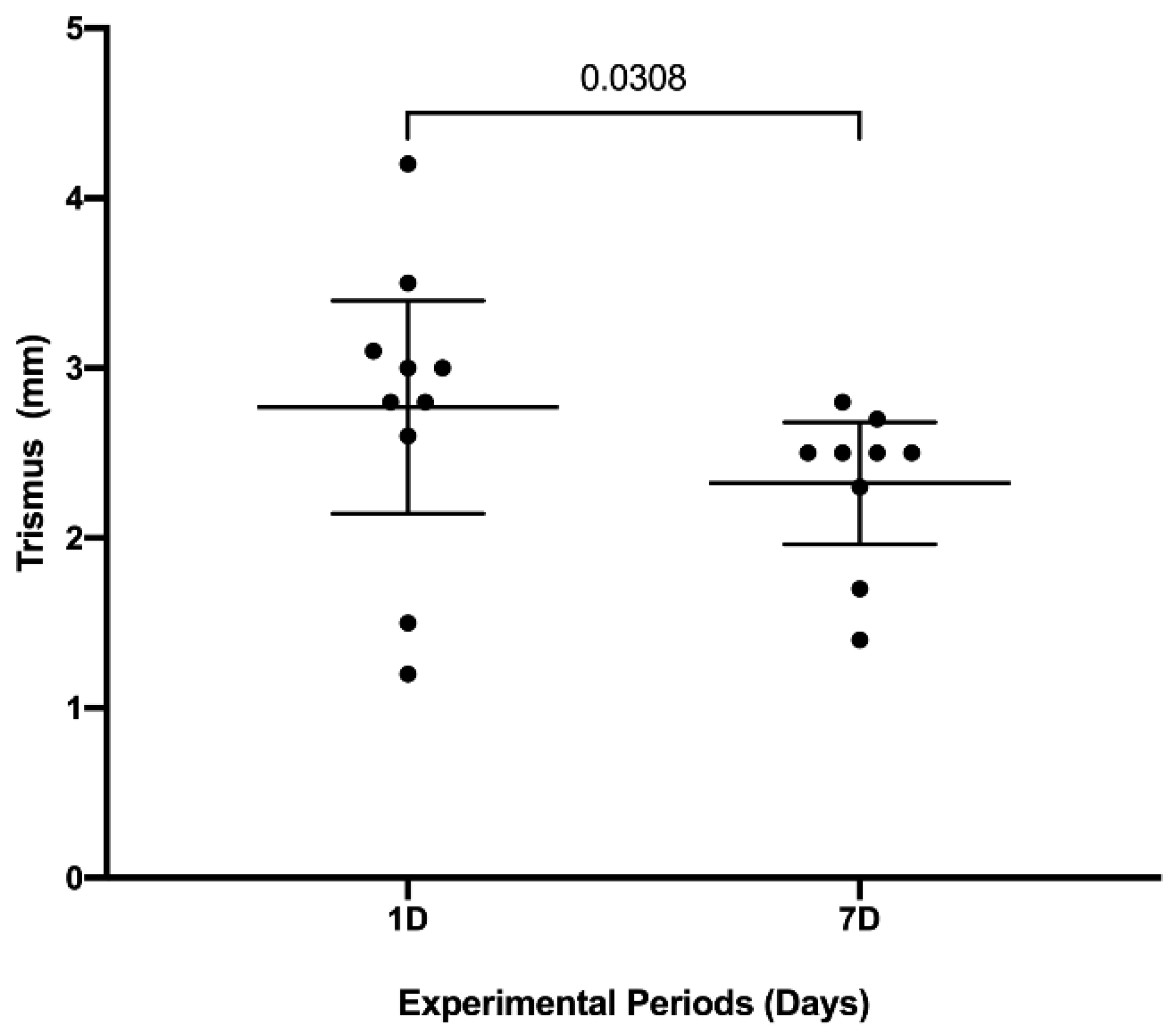
3.3. Trismus
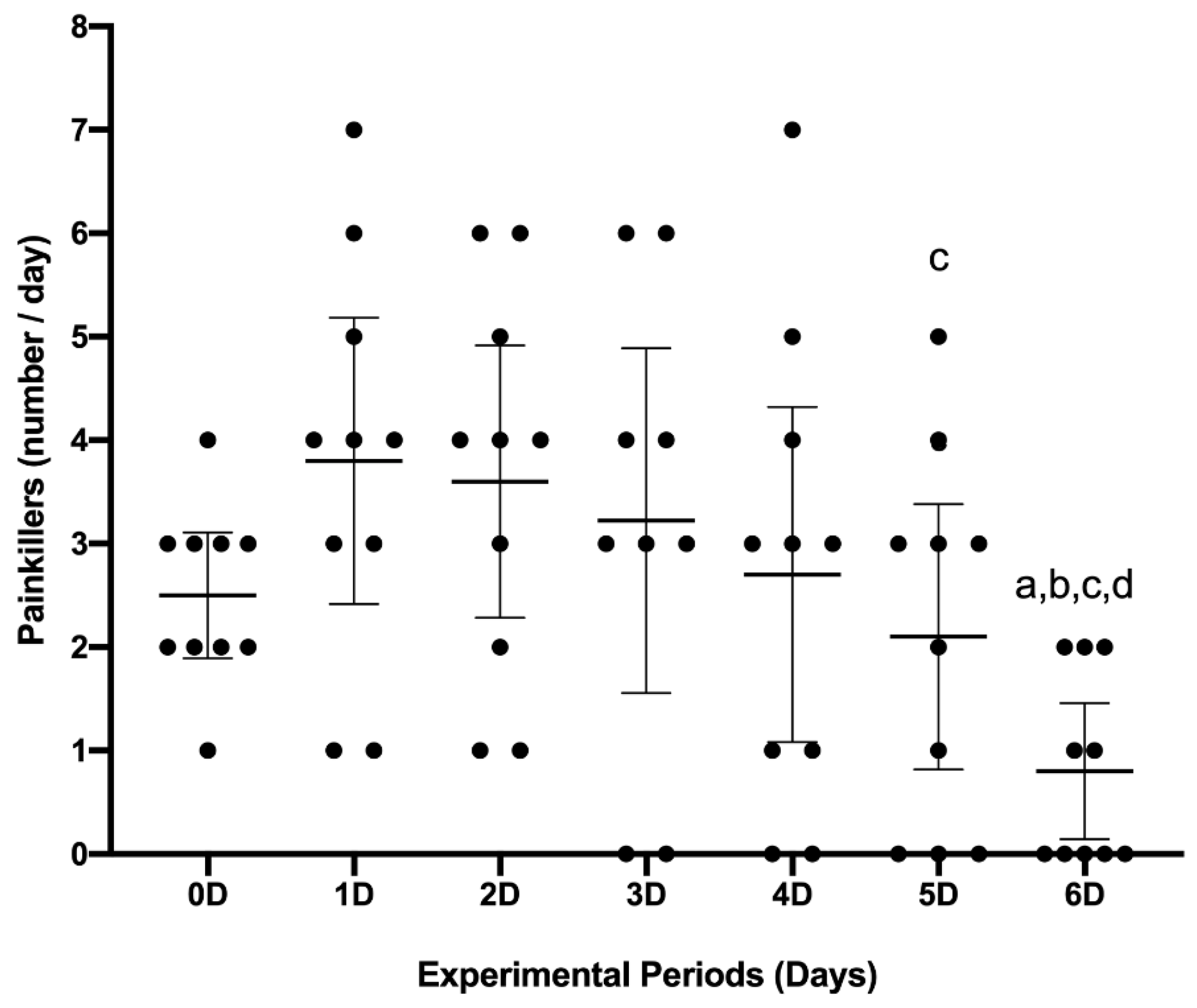
3.4. Analgesic Consumption
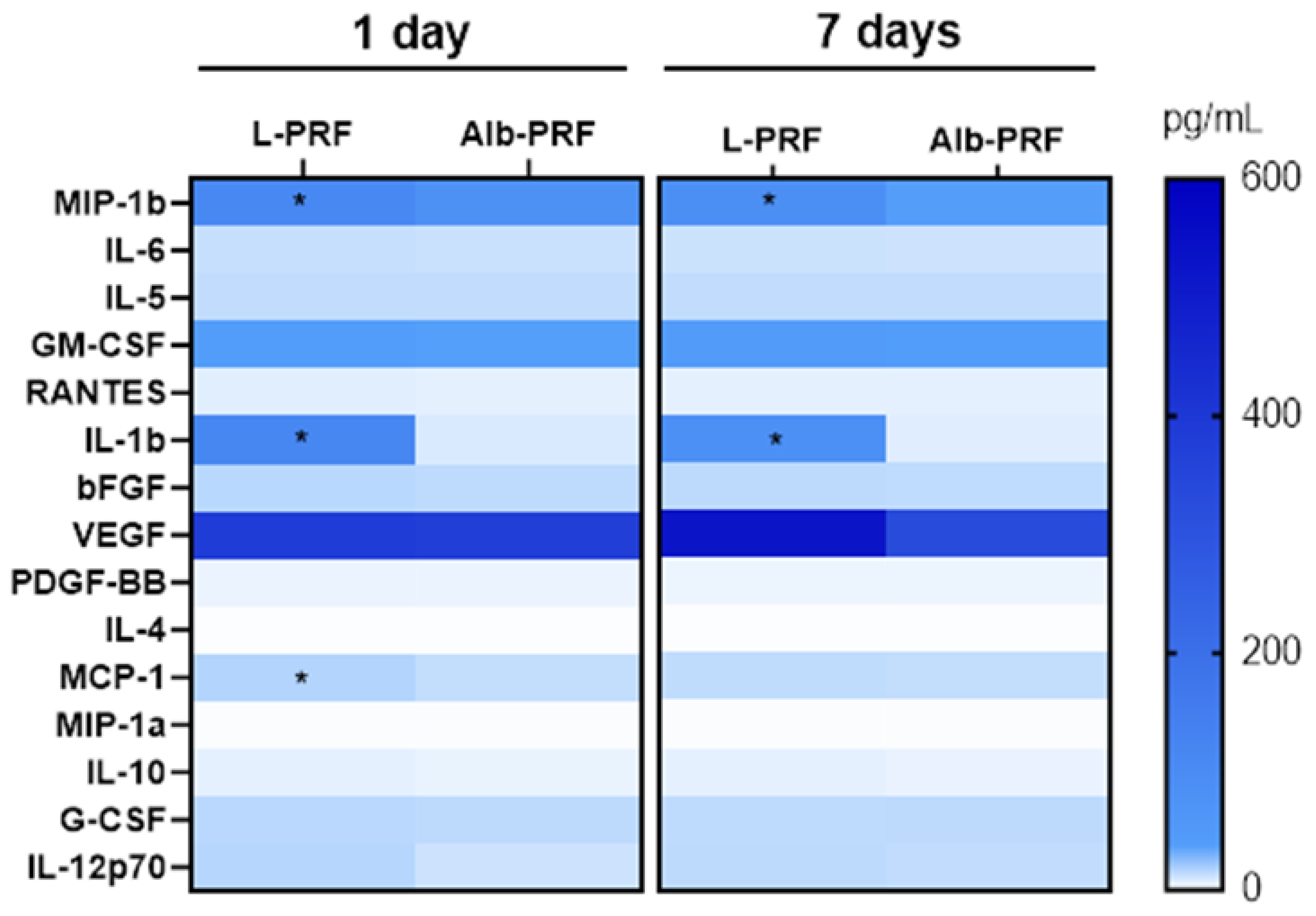
3.5. Biochemical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Green, D.; Walsh, D.; Mann, S.; Oreffo, R.O. The potential of biomimesis in bone tissue engineering: Lessons from the design and synthesis of invertebrate skeletons. Bone 2002, 30, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Behonick, D.J.; Xing, Z.; Lieu, S.; Buckley, J.M.; Lotz, J.C.; Marcucio, R.S.; Werb, Z.; Miclau, T.; Colnot, C. Role of matrix metalloproteinase 13 in both endochondral and intramembranous ossification during skeletal regeneration. PLoS ONE 2007, 2, e1150. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, C.; Alpern, E.; Miclau, T.; Helms, J.A. Does adult fracture repair recapitulate embryonic skeletal formation? Mech. Dev. 1999, 87, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Seal, B.; Otero, T.; Panitch, A. Polymeric biomaterials for tissue and organ regeneration. Mater. Sci. Eng. R Rep. 2001, 34, 147–230. [Google Scholar] [CrossRef]
- Miguel, F.B.; Cardoso, A.K.M.; Barbosa, A.A., Jr.; Marcantonio, E., Jr.; Goissis, G.; Rosa, F.P. Morphological assessment of the behavior of three-dimensional anionic collagen matrices in bone regeneration in rats. J. Biomed. Mater. Res. Part B Appl. Biomater. 2006, 78, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Miguel, F.B.; de Almeida Barbosa Júnior, A.; de Paula, F.L.; Barreto, I.C.; Goissis, G.; Rosa, F.P. Regeneration of critical bone defects with anionic collagen matrix as scaffolds. J. Mater. Sci. Mater. Med. 2013, 24, 2567–2575. [Google Scholar] [CrossRef]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 85, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e51–e55. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e45–e50. [Google Scholar] [CrossRef]
- Ehrenfest, D.M.D.; Andia, I.; Zumstein, M.A.; Zhang, C.-Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Current consensus, clinical implications and perspectives. Muscles Ligaments Tendons J. 2014, 4, 3. [Google Scholar] [CrossRef]
- de Almeida Barros Mourão, C.F.; Miron, R.J.; de Mello Machado, R.C.; Ghanaati, S.; Alves, G.G.; Calasans-Maia, M.D. Usefulness of platelet-rich fibrin as a hemostatic agent after dental extractions in patients receiving anticoagulant therapy with factor Xa inhibitors: A case series. Oral Maxillofac. Surg. 2019, 23, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Sari, H.; Karaketir, S.; Kumral, T.L.; Akgun, M.F.; Gurpinar, B.; Hanci, D.; Berkiten, G.; Uyar, Y. The effect of platelet-rich fibrin (PRF) on wound healing, adhesion, and hemostasis after endoscopic sinus surgery in patients with nasal polyposis. Am. J. Otolaryngol. 2021, 42, 103010. [Google Scholar] [CrossRef]
- de Almeida Barros Mourão, C.F.; Calasans-Maia, M.; Del Fabbro, M.; Vieira, F.L.D.; de Mello Machado, R.C.; Capella, R.; Miron, R.J.; Alves, G.G. The use of Platelet-rich Fibrin in the management of medication-related osteonecrosis of the jaw: A case series. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 84–89. [Google Scholar]
- Cano-Durán, J.A.; Peña-Cardelles, J.F.; Ortega-Concepción, D.; Paredes-Rodríguez, V.M.; García-Riart, M.; López-Quiles, J. The role of Leucocyte-rich and platelet-rich fibrin (L-PRF) in the treatment of the medication-related osteonecrosis of the jaws (MRONJ). J. Clin. Exp. Dent. 2017, 9, e1051–e1059. [Google Scholar] [CrossRef]
- Bolukbasi, N.; Ersanlı, S.; Keklikoglu, N.; Basegmez, C.; Ozdemir, T. Sinus augmentation with platelet-rich fibrin in combination with bovine bone graft versus bovine bone graft in combination with collagen membrane. J. Oral Implantol. 2015, 41, 586–595. [Google Scholar] [CrossRef]
- Pathak, H.; Mohanty, S.; Urs, A.B.; Dabas, J. Treatment of oral mucosal lesions by scalpel excision and platelet-rich fibrin membrane grafting: A review of 26 sites. J. Oral Maxillofac. Surg. 2015, 73, 1865–1874. [Google Scholar] [CrossRef]
- Lourenco, E.S.; de Almeida Barros Mourão, C.F.; Leite, P.E.C.; Granjeiro, J.M.; Calasans-Maia, M.D.; Alves, G.G. The in vitro release of cytokines and growth factors from fibrin membranes produced through horizontal centrifugation. J. Biomed. Mater. Res. Part A 2018, 106, 1373–1380. [Google Scholar] [CrossRef]
- de Almeida Barros Mourão, C.F.; Gheno, E.; Lourenço, E.S.; de Lima Barbosa, R.; Kurtzman, G.M.; Javid, K.; Mavropoulos, E.; Benedicenti, S.; Calasans-Maia, M.D.; de Mello Machado, R.C. Characterization of a new membrane from concentrated growth factors associated with denaturized Albumin (Alb-CGF) for clinical applications: A preliminary study. Int. J. Growth Factors Stem Cells Dent. 2018, 1, 64. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Schaller, B.; de Almeida Barros Mourão, C.F.; Zhang, Y.; Sculean, A.; Miron, R.J. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets 2021, 32, 74–81. [Google Scholar] [CrossRef]
- Gheno, E.; de Almeida Barros Mourão, C.F.; De Mello-Machado, R.C.; Stellet Lourenco, E.; Miron, R.J.; Catarino, K.F.F.; Alves, A.T.; Alves, G.G.; Calasans-Maia, M.D. In vivo evaluation of the biocompatibility and biodegradation of a new denatured plasma membrane combined with liquid PRF (Alb-PRF). Platelets 2021, 32, 542–554. [Google Scholar] [CrossRef]
- Horváthy, D.B.; Simon, M.; Schwarz, C.M.; Masteling, M.; Vácz, G.; Hornyák, I.; Lacza, Z. Serum albumin as a local therapeutic agent in cell therapy and tissue engineering. BioFactors 2017, 43, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Zhang, Y. Autologous liquid platelet rich fibrin: A novel drug delivery system. Acta Biomater. 2018, 75, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Mourão, C.F.; Lowenstein, A. The Use of Alb-PRF as a Drug Delivery System for Malignant Lesion Treatment. Rev. Bras. Cancerol. 2023, 69, 2. [Google Scholar] [CrossRef]
- Li, P.-S.; Liang Lee, I.; Yu, W.-L.; Sun, J.-S.; Jane, W.-N.; Shen, H.-H. A novel albumin-based tissue scaffold for autogenic tissue engineering applications. Sci. Rep. 2014, 4, 5600. [Google Scholar] [CrossRef] [PubMed]
- Li, W.J.; Laurencin, C.T.; Caterson, E.J.; Tuan, R.S.; Ko, F.K. Electrospun nanofibrous structure: A novel scaffold for tissue engineering. J. Biomed. Mater. Res. Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2002, 60, 613–621. [Google Scholar] [CrossRef]
- Pretorius, E.; Lipinski, B.; Bester, J.; Vermeulen, N.; Soma, P. Albumin stabilizes fibrin fiber ultrastructure in low serum albumin type 2 diabetes. Ultrastruct. Pathol. 2013, 37, 254–257. [Google Scholar] [CrossRef]
- Da Silva, M.T.; de Almeida Barros Mourao, C.F.; Mello-Machado, R.C.; Montemezzi, P.; de Lima Barbosa, R.; Sartoretto, S.C.; Leite, P.E.C.; Javid, K.; Kawase, T.; Alves, G.G. Effects of Leukocyte-Platelet-Rich Fibrin (L–PRF) on Pain, Soft Tissue Healing, Growth Factors, and Cytokines after Third Molar Extraction: A Randomized, Split-Mouth, Double-Blinded Clinical Trial. Appl. Sci. 2021, 11, 1666. [Google Scholar] [CrossRef]
- Ritto, F.G.; Pimentel, T.; Canellas, J.V.S.; Junger, B.; Cruz, M.; Medeiros, P.J. Randomized double-blind clinical trial evaluation of bone healing after third molar surgery with the use of leukocyte- and platelet-rich fibrin. Int. J. Oral Maxillofac. Surg. 2019, 48, 1088–1093. [Google Scholar] [CrossRef]
- Asif, M.; Ullah, A.; Mujtaba, H.; Umer, M.F.; Khurshid, Z. Comparative Study of Frequency of Alveolar Osteitis, with and without using Platelet-Rich Fibrin in Mandibular Third Molar Surgery. Int. J. Dent. 2023, 2023, 2256113. [Google Scholar] [CrossRef]
- Ustaoğlu, G.; Göller Bulut, D.; Gümüş, K. Evaluation of different platelet-rich concentrates effects on early soft tissue healing and socket preservation after tooth extraction. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Ishihama, K.; Kimura, T.; Yasui, Y.; Komaki, M.; Ota, Y. Azithromycin as prophylaxis for the prevention of postoperative infection in impacted mandibular third-molar surgery. J. Infect. Chemother. 2006, 12, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Bouloux, G.F.; Steed, M.B.; Perciaccante, V.J. Complications of third molar surgery. Oral Maxillofac. Surg. Clin. 2007, 19, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Barone, S.; Bennardo, F.; Giudice, A. Three-dimensional facial swelling evaluation of pre-operative single-dose of prednisone in third molar surgery: A split-mouth randomized controlled trial. BMC Oral Health 2023, 23, 614. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Alvira-González, J.; Figueiredo, R.; Valmaseda-Castellón, E.; Quesada-Gómez, C.; Gay-Escoda, C. Predictive factors of difficulty in lower third molar extraction: A prospective cohort study. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e108–e114. [Google Scholar] [CrossRef]
- Miron, R.J.; Pinto, N.R.; Quirynen, M.; Ghanaati, S. Standardization of relative centrifugal forces in studies related to platelet-rich fibrin. J. Periodontol. 2019, 90, 817–820. [Google Scholar] [CrossRef]
- Ghanaati, S.; Mourão, C.; Adam, E.; Sader, R.; Zadeh, H.; Al-Maawi, S. The role of centrifugation process in the preparation of therapeutic blood concentrates: Standardization of the protocols to improve reproducibility. Int. J. Growth Factors Stem Cells Dent. 2019, 2, 41–44. [Google Scholar] [CrossRef]
- Camps-Font, O.; Sábado-Bundó, H.; Toledano-Serrabona, J.; Valmaseda-de-la-Rosa, N.; Figueiredo, R.; Valmaseda-Castellón, E. Antibiotic prophylaxis in the prevention of dry socket and surgical site infection after lower third molar extraction: A network meta-analysis. Int. J. Oral Maxillofac. Surg. 2023. [Google Scholar] [CrossRef]
- Ustun, Y.; Erdogan, O.; Esen, E.; Karsli, E.D. Comparison of the effects of 2 doses of methylprednisolone on pain, swelling, and trismus after third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 535–539. [Google Scholar] [CrossRef]
- Gabka, J.; Matsumura, T. Measuring techniques and clinical testing of an anti-inflammatory agent (tantum). Munch. Med. Wochenschr. 1971, 113, 198–203. [Google Scholar] [PubMed]
- Keyhan, S.; Fallahi, H.R.; Cheshmi, B.; Mokhtari, S.; Zandian, D.; Yousefi, P. Use of piezoelectric surgery and Er:YAG laser: Which one is more effective during impacted third molar surgery? Maxillofac. Plast. Reconstr. Surg. 2019, 41, 29. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, X.; Zhou, Z.; Hao, Y.; Li, H.; Cheng, Y.; Ren, X.; Wang, X. Effects of Impacted Lower Third Molar Extraction on Periodontal Tissue of the Adjacent Second Molar. Ther. Clin. Risk Manag. 2021, 17, 235–247. [Google Scholar] [CrossRef] [PubMed]
- de Almeida Barros Mourão, C.F.; de Mello-Machado, R.C.; Javid, K.; Moraschini, V. The use of leukocyte- and platelet-rich fibrin in the management of soft tissue healing and pain in post-extraction sockets: A randomized clinical trial. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2020, 48, 452–457. [Google Scholar] [CrossRef]
- Annunziata, M.; Guida, L.; Nastri, L.; Piccirillo, A.; Sommese, L.; Napoli, C. The role of autologous platelet concentrates in alveolar socket preservation: A systematic review. Transfus. Med. Hemother. 2018, 45, 195–203. [Google Scholar] [CrossRef]
- Canellas, J.; Medeiros, P.J.D.; Figueredo, C.; Fischer, R.G.; Ritto, F.G. Platelet-rich fibrin in oral surgical procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 395–414. [Google Scholar] [CrossRef]
- Canellas, J.d.S.; Ritto, F.; Medeiros, P. Evaluation of postoperative complications after mandibular third molar surgery with the use of platelet-rich fibrin: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1138–1146. [Google Scholar] [CrossRef]
- Bennardo, F.; Gallelli, L.; Palleria, C.; Colosimo, M.; Fortunato, L.; De Sarro, G.; Giudice, A. Can platelet-rich fibrin act as a natural carrier for antibiotics delivery? A proof-of-concept study for oral surgical procedures. BMC Oral Health 2023, 23, 134. [Google Scholar] [CrossRef]
- Moraschini, V.; Miron, R.J.; Mourão, C.; Louro, R.S.; Sculean, A.; da Fonseca, L.A.M.; Calasans Maia, M.D.; Shibli, J.A. Antimicrobial effect of platelet-rich fibrin: A systematic review of in vitro evidence-based studies. Periodontology 2000 2023. [Google Scholar] [CrossRef]
- Yang, B.; Zhang, Z.; Yang, Z.; Ruan, J.; Luo, L.; Long, F.; Tang, D. Chanling Gao Attenuates Bone Cancer Pain in Rats by the IKKβ/NF-κB Signaling Pathway. Front. Pharmacol. 2020, 11, 525. [Google Scholar] [CrossRef]
- Francisco-Cruz, A.; Aguilar-Santelises, M.; Ramos-Espinosa, O.; Mata-Espinosa, D.; Marquina-Castillo, B.; Barrios-Payan, J.; Hernandez-Pando, R. Granulocyte-macrophage colony-stimulating factor: Not just another haematopoietic growth factor. Med. Oncol. 2014, 31, 774. [Google Scholar] [CrossRef] [PubMed]
- Önnheim, K.; Huang, S.; Strid Holmertz, A.; Andersson, S.; Lönnblom, E.; Jonsson, C.; Holmdahl, R.; Gjertsson, I. Rheumatoid arthritis chondrocytes produce increased levels of pro-inflammatory proteins. Osteoarthr. Cart. Open 2022, 4, 100235. [Google Scholar] [CrossRef] [PubMed]
- Herder, C.; Peeters, W.; Illig, T.; Baumert, J.; de Kleijn, D.P.; Moll, F.L.; Poschen, U.; Klopp, N.; Müller-Nurasyid, M.; Roden, M.; et al. RANTES/CCL5 and risk for coronary events: Results from the MONICA/KORA Augsburg case-cohort, Athero-Express and CARDIoGRAM studies. PLoS ONE 2011, 6, e25734. [Google Scholar] [CrossRef] [PubMed]
- Luzina, I.G.; Keegan, A.D.; Heller, N.M.; Rook, G.A.; Shea-Donohue, T.; Atamas, S.P. Regulation of inflammation by interleukin-4: A review of “alternatives”. J. Leukoc. Biol. 2012, 92, 753–764. [Google Scholar] [CrossRef]
- Gurgone, D.; McShane, L.; McSharry, C.; Guzik, T.J.; Maffia, P. Cytokines at the Interplay Between Asthma and Atherosclerosis? Front. Pharmacol. 2020, 11, 166. [Google Scholar] [CrossRef]
- Klementiev, B.; Enevoldsen, M.N.; Li, S.; Carlsson, R.; Liu, Y.; Issazadeh-Navikas, S.; Bock, E.; Berezin, V. Antiinflammatory properties of a peptide derived from interleukin-4. Cytokine 2013, 64, 112–121. [Google Scholar] [CrossRef]
- Trybek, G.; Jarzęcka, J.; Preuss, O.; Jaroń, A. Effect of Intraoral Drainage after Impacted Mandibular Third Molar Extraction on Non-Infectious Postoperative Complications. J. Clin. Med. 2021, 10, 4705. [Google Scholar] [CrossRef]
- Bernal Rodriguez, C.G.; Kraul, L.F.; Cardoso, T.W.; Eduardo, C.P.; Aranha, A.C.C.; de Freitas, P.M. Photobiomodulation in the Postoperative of Bichectomy Surgeries: Case Series. Photomed. Laser Surg. 2018, 36, 391–394. [Google Scholar] [CrossRef]
- Mahat, A.K.; Yadav, R.; Yadav, A.K.; Acharya, P.; Dongol, A.; Sagtani, A.; Jaisani, M.R. A Comparative Study of the Effect of Sutureless versus Multiple Sutures Technique on Complications following Third Molar Surgery in Nepalese Subpopulation. Int. J. Dent. 2020, 2020, 9314762. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | Alb-PRF | L-PRF |
|---|---|---|
| VEGF | 810 ± 153 | 1104 ± 298 |
| PDGF-BB | 551 ± 39 | 426 ± 24 * |
| bFGF | 28 ± 6 | 27 ± 12 |
| G-CSF | 381 ± 58 | 278 ± 74 |
| GM-CSF | 12 ± 6 | 57 ± 22 * |
| IL-1β | 2 ± 2 | 162,7 ± 78 * |
| IL-6 | 268 ± 45 | 4564 ± 946 * |
| TNFα | 39 ± 9 | 98 ± 24 * |
| IFNy | 85 ± 29 | 246 ± 37 * |
| IL-8 | 6954 ± 782 | 120,589 ± 756 * |
| IL-13 | 2 ± 1.4 | 1.9 ± 0.8 |
| IL-15 | 12 ± 8.9 | 96 ± 26 * |
| IL-7 | 0.46 ± 0.46 | 0.634 ± 0.46 |
| IL-12p70 | 5 ± 4 | 9 ± 2 |
| IL-17A | 29 ± 8 | 37 ± 7 |
| IL-9 | 4 ± 2 | 5 ± 0.1 |
| IL-5 | 0.31 ± 0.1 | 0.3 ± 0.38 |
| IL-2 | 2 ± 1 | 3 ± 2 |
| IL-1RA | 267 ± 70 | 262 ± 64 |
| IL-4 | 0.9 ± 0 | 8.7 ± 0.7 * |
| IL-10 | 5 ± 4 | 19 ± 13 |
| RANTES | 593 ± 55 | 1084 ± 162 * |
| Eotaxin | 133 ± 3 | 136 ± 9 |
| IP-10 | 20 ± 7 | 49 ± 22 |
| MIP-1b | 170 ± 57 | 155 ± 59 |
| MIP-1a | 0 ± 0 | 39 ± 5 * |
| MCP-1 | 356 ± 22 | 155 ± 38 * |
| MIP-1b | IL-6 | IL-5 | GM-CSF | Rantes | IL-1b | bFGF | VEGF | PDGF | IL-4 | MCP-1 | MIP-1a | IL-10 | G-CSF | IL-12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L-PRF | |||||||||||||||
| VAS 0 | 0.0741 | 0.0124 | 0.1125 | 0.3488 | 0.1243 | 0.1359 | 0.2347 | 0.2718 | 0.1367 | 0.0124 | 0.1989 | −0.1359 | 0.1359 | 0.0000 | 0.1235 |
| VAS 1D | 0.3706 | 0.2594 | −0.4751 | −0.1684 | 0.0621 | −0.1853 | −0.3336 | −0.1482 | −0.2610 | −0.2983 | −0.3356 | −0.2594 | −0.1853 | −0.2224 | 0.0000 |
| VAS 2D | 0.7856 | 0.2578 | 0.1180 | 0.4865 | 0.6298 | 0.7365 * | 0.6997 | 0.6138 | 0.4446 | 0.0617 | 0.7039 | 0.7243 | −0.7365 | 0.6752 | 0.6506 |
| VAS 3D | 0.2546 | 0.3516 | −0.1472 | −0.0546 | 0.7013 | 0.4607 | 0.3758 | 0.3031 | 0.1037 | −0.1646 | 0.3964 | 0.2546 | 0.4607 | 0.3395 | 0.5819 |
| VAS 4D | 0.1149 | 0.1916 | −0.4459 | −0.0561 | 0.3854 | 0.3448 | 0.1532 | 0.3065 | 0.0064 | −0.2955 | 0.1542 | 0.0511 | 0.3448 | 0.1660 | 0.4980 |
| VAS 5D | 0.1853 | 0.2347 | −0.0938 | −0.3368 | 0.6649 | 0.3459 | 0.2965 | 0.0988 | 0.0249 | −0.1802 | 0.3294 | 0.2471 | 0.3459 | 0.2965 | 0.4200 |
| VAS 6D | 0.4637 | 0.1364 | 0.0828 | 0.0591 | 0.7683 | 0.4637 | 0.5455 | 0.2455 | 0.1921 | −0.1921 | 0.5488 | 0.4364 | 0.4637 | 0.4364 | 0.3546 |
| Swelling 1D | 0.2275 | 0.3713 | 0.6606 | −0.1802 | 0.5904 | 0.2275 | 0.4311 | −0.0240 | 0.3313 | 0.4096 | 0.4458 | 0.3353 | 0.2275 | 0.3713 | 0.1078 |
| Swelling 7D | 0.4458 | 0.7470 | 0.6585 | 0.5637 | 0.3212 | 0.5543 | 0.5302 | 0.5543 | 0.6303 | 0.8667 * | 0.5515 | 0.4820 | 0.5543 | 0.5543 | 0.6627 |
| Trismus 1D | 0.3615 | 0.5784 | 0.3415 | 0.8469 * | 0.0667 | 0.4097 | 0.3856 | 0.6627 | 0.5576 | 0.5758 | 0.3455 | 0.2410 | 0.4097 | 0.3253 | 0.4579 |
| Trismus 7D | 0.3615 | 0.5784 | 0.3415 | 0.8469 * | 0.0667 | 0.4097 | 0.3856 | 0.6627 | 0.5576 | 0.5758 | 0.3455 | 0.2410 | 0.4097 | 0.3253 | 0.4579 |
| Alb-PRF | |||||||||||||||
| VAS 0 | 0.0507 | 0.1212 | 0.7148 | 0.0761 | −0.4019 | 0.1142 | 0.2297 | 0.2029 | 0.4059 | 0.8230 * | 0.3828 | 0.2599 | 0.4820 | 0.6343 | 0.2029 |
| VAS 1D | −0.6789 | −0.3598 | −0.2857 | −0.3273 | −0.1403 | −0.5577 | −0.4452 | −0.2667 | −0.1576 | −0.4147 | −0.0793 | −0.4969 | −0.1818 | 0.2063 | −0.3637 |
| VAS 2D | −0.4051 | −0.3087 | 0.3145 | 0.0859 | −0.1111 | −0.2455 | −0.1173 | 0.2701 | 0.0982 | 0.0185 | 0.2408 | −0.2138 | 0.0491 | 0.2785 | −0.0737 |
| VAS 3D | −0.3953 | −0.3915 | 0.0380 | −0.1977 | −0.0932 | −0.2841 | −0.0994 | 0.0741 | −0.1730 | 0.0311 | −0.0994 | −0.2279 | 0.0494 | 0.0955 | −0.0247 |
| VAS 4D | 0.1091 | −0.0061 | −0.4596 | 0.1940 | 0.5000 | 0.2182 | 0.2500 | 0.4243 | −0.2303 | −0.4452 | −0.1525 | 0.1242 | 0.0849 | −0.2938 | 0.3273 |
| VAS 5D | −0.4243 | −0.2927 | −0.1491 | −0.1455 | −0.0549 | −0.3031 | −0.1037 | 0.0121 | −0.0364 | 0.0000 | 0.0061 | −0.2236 | 0.0727 | 0.2875 | −0.0242 |
| VAS 6D | 0.0261 | −0.0262 | 0.2673 | 0.0913 | 0.0262 | 0.1174 | 0.3214 | 0.3651 | 0.2739 | 0.5051 | 0.3214 | 0.2138 | 0.4825 | 0.4169 | 0.3651 |
| Swelling 1D | 0.1905 | −0.0120 | 0.1220 | −0.0952 | −0.1317 | 0.0952 | 0.1677 | −0.0952 | −0.0238 | 0.5150 | −0.1437 | 0.1464 | 0.0952 | −0.0123 | 0.1429 |
| Swelling7D | 0.1429 | 0.3593 | −0.3660 | 0.0238 | 0.2515 | 0.0952 | 0.2156 | −0.1190 | 0.6190 | 0.2515 | 0.5749 | 0.2196 | 0.4286 | 0.6383 | 0.2381 |
| Trismus 1D | 0.0507 | 0.1212 | 0.7148 | 0.0761 | −0.4019 | 0.1142 | 0.2297 | 0.2029 | 0.4059 | 0.8230 | 0.3828 | 0.2599 | 0.4820 | 0.6343 | 0.2029 |
| Trismus 7D | −0.6789 | −0.3598 | −0.2857 | −0.3273 | −0.1403 | −0.5577 | −0.4452 | −0.2667 | −0.1576 | −0.4147 | −0.0793 | −0.4969 | −0.1818 | 0.2063 | −0.3637 |
| MIP-1b | IL-6 | IL-5 | GM-CSF | Rantes | IL-1b | bFGF | VEGF | PDGF | IL-4 | MCP-1 | MIP-1a | IL-10 | G-CSF | IL-12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L-PRF | |||||||||||||||
| VAS 0 | 0.2648 | 0.1493 | 0.4352 | −0.1053 | 0.5971 | 0.8533 * | 0.8533 | 0.5002 | −0.0294 | 0.2239 | 0.8359 * | −0.0883 | 0.7945 | −0.1045 | 0.6473 |
| VAS 1D | 0.1765 | 0.0896 | −0.7833 | 0.7105 | −0.8508 | −0.2648 | −0.2648 | 0.3531 | 0.4414 | 0.0000 | −0.2239 | 0.5296 | −0.1765 | 0.5374 | 0.0883 |
| VAS 2D | 0.3531 | 0.6717 | 0.7833 | 0.0811 | 0.1343 | 0.6179 | 0.6179 | 0.2648 | 0.1765 | 0.6269 | 0.5822 | 0.3531 | 0.5296 | 0.3582 | 0.2648 |
| VAS 3D | 0.4638 | 0.6176 | 0.2572 | 0.7632 | 0.1471 | 0.8117 * | 0.8117 | 0.7537 | 0.6377 | 0.8676 * | 0.7353 | 0.7537 | 0.6377 | 0.5441 | 0.5508 |
| VAS 4D | 0.1518 | 0.3388 | 0.1796 | 0.7895 | −0.0924 | 0.6375 | 0.6375 | 0.7590 | 0.4554 | 0.6776 | 0.5236 | 0.6983 | 0.3947 | 0.3696 | 0.3339 |
| VAS 5D | 0.4414 | 0.6717 | 0.2611 | 0.6489 | 0.1791 | 0.6179 | 0.6179 | 0.5296 | 0.7062 | 0.9404 * | 0.5374 | 0.7945 | 0.4414 | 0.5822 | 0.3531 |
| VAS 6D | 0.4554 | 0.7701 | 0.7184 | 0.1579 | 0.2772 | 0.6983 | 0.6983 | 0.3339 | 0.3947 | 0.8317 | 0.6468 | 0.5161 | 0.5768 | 0.4620 | 0.3339 |
| Swelling 1D | 0.8117 | 0.6765 | 0.0000 | −0.5526 | 0.5735 | 0.3189 | 0.3189 | −0.0580 | 0.5508 | 0.4559 | 0.4265 | 0.1739 | 0.5218 | 0.4853 | 0.5218 |
| Swelling 7D | 0.6179 | 0.1941 | −0.3482 | −0.3785 | 0.5523 | 0.4119 | 0.4119 | 0.2354 | 0.3237 | 0.0448 | 0.5224 | −0.0883 | 0.6179 | 0.1642 | 0.7356 |
| Trismus 1D | 0.1471 | −0.2090 | −0.3482 | −0.0263 | −0.2239 | 0.1177 | 0.1177 | 0.2648 | −0.2354 | −0.5224 | 0.2239 | −0.3237 | 0.3237 | −0.0746 | 0.4414 |
| Trismus 7D | 0.1471 | −0.2090 | −0.3482 | −0.0263 | −0.2239 | 0.1177 | 0.1177 | 0.2648 | −0.2354 | −0.5224 | 0.2239 | −0.3237 | 0.3237 | −0.0746 | 0.4414 |
| Alb-PRF | |||||||||||||||
| VAS 0 | 0.0381 | 0.8371 | 0.2680 | 0.3947 | 0.1649 | 0.7357 | 0.6469 | 0.6596 | 0.2361 | 0.5263 | 0.8677 | 0.4275 | 0.6571 | 0.7401 | 0.6508 |
| VAS 1D | −0.0121 | −0.3395 | 0.1098 | −0.3479 | −0.7638 | −0.4243 | −0.3516 | 0.4122 | −0.0610 | −0.3926 | −0.2012 | −0.2988 | 0.2805 | −0.2622 | 0.2805 |
| VAS 2D | 0.3805 | 0.2578 | 0.4199 | 0.2648 | −0.3805 * | 0.1350 | 0.1719 | 0.5524 | −0.1173 | 0.2858 | 0.4755 | −0.2470 | 0.7410 | 0.2038 | 0.7039 |
| VAS 3D | −0.0124 | 0.3212 | 0.7830 | −0.0883 | −0.6054 | 0.1482 | 0.2100 | 0.5930 | 0.6152 | 0.3001 | 0.2361 | 0.3915 | 0.4039 | 0.3977 | 0.3480 |
| VAS 4D | 0.1091 | −0.0364 | 0.4756 | −0.0294 | −0.4364 | −0.1940 | 0.1818 | 0.0364 | 0.5366 | 0.3374 | −0.3171 | 0.0610 | 0.0061 | 0.2012 | −0.1159 |
| VAS 5D | 0.0242 | 0.1697 | 0.6098 | −0.0883 | −0.7759 * | 0.0727 | 0.1576 | 0.7274 | 0.5854 | 0.1288 | 0.1403 | 0.3476 | 0.4391 | 0.2866 | 0.4025 |
| VAS 6D | 0.1826 | 0.7303 | 0.7347 | 0.3086 | −0.2608 | 0.4564 | 0.5477 | 0.7303 | 0.6888 | 0.5544 | 0.5969 | 0.5510 | 0.6888 | 0.7806 | 0.6428 |
| Swelling 1D | −0.2857 | 0.4286 | 0.4192 | 0.0857 | 0.0714 | 0.5238 | 0.3571 | 0.1905 | −0.7545 * | 0.3012 | 0.2275 | 0.9341 | −0.1916 | 0.4311 | −0.1796 |
| Swelling 7D | 0.1905 | −0.0714 | −0.2755 | −0.3143 | −0.1667 | −0.2619 | −0.2143 | 0.3571 | 0.0838 | −0.5061 | −0.0599 | 0.0479 | 0.3234 | 0.0000 | 0.4192 |
| Trismus 1D | 0.2771 | −0.2048 | −0.0364 | 0.1449 | −0.1084 | −0.3133 | 0.0602 | −0.2289 | −0.2546 | 0.2378 | −0.2606 | −0.6364 | 0.0909 | −0.0788 | −0.0242 |
| Trismus 7D | 0.2771 | −0.2048 | −0.0364 | 0.1449 | −0.1084 | −0.3133 | 0.0602 | −0.2289 | −0.2546 | 0.2378 | −0.2606 | −0.6364 | 0.0909 | −0.0788 | −0.0242 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javid, K.; Mourão, C.F.; Mello-Machado, R.C.; Sartoretto, S.C.; Torres, M.; Stellet Lourenço, E.; Leite, P.E.C.; Granjeiro, J.M.; Alves, G.G.; Calasans-Maia, M.D. Clinical and Biochemical Evaluation of the Use of Alb-PRF versus L-PRF in Mandibular Third Molar Extractions: A Split-Mouth Randomized Clinical Trial. J. Funct. Biomater. 2023, 14, 505. https://doi.org/10.3390/jfb14100505
Javid K, Mourão CF, Mello-Machado RC, Sartoretto SC, Torres M, Stellet Lourenço E, Leite PEC, Granjeiro JM, Alves GG, Calasans-Maia MD. Clinical and Biochemical Evaluation of the Use of Alb-PRF versus L-PRF in Mandibular Third Molar Extractions: A Split-Mouth Randomized Clinical Trial. Journal of Functional Biomaterials. 2023; 14(10):505. https://doi.org/10.3390/jfb14100505
Chicago/Turabian StyleJavid, Kayvon, Carlos Fernando Mourão, Rafael Coutinho Mello-Machado, Suelen Cristina Sartoretto, Madelaine Torres, Emanuelle Stellet Lourenço, Paulo Emilio Correa Leite, José Mauro Granjeiro, Gutemberg Gomes Alves, and Monica Diuana Calasans-Maia. 2023. "Clinical and Biochemical Evaluation of the Use of Alb-PRF versus L-PRF in Mandibular Third Molar Extractions: A Split-Mouth Randomized Clinical Trial" Journal of Functional Biomaterials 14, no. 10: 505. https://doi.org/10.3390/jfb14100505