
Image-Based Finite Element Modeling Approach for Characterizing In Vivo Mechanical Properties of Human Arteries

Abstract
:1. Introduction
2. In Vivo Methods to Quantify Material Properties of Arterial Walls
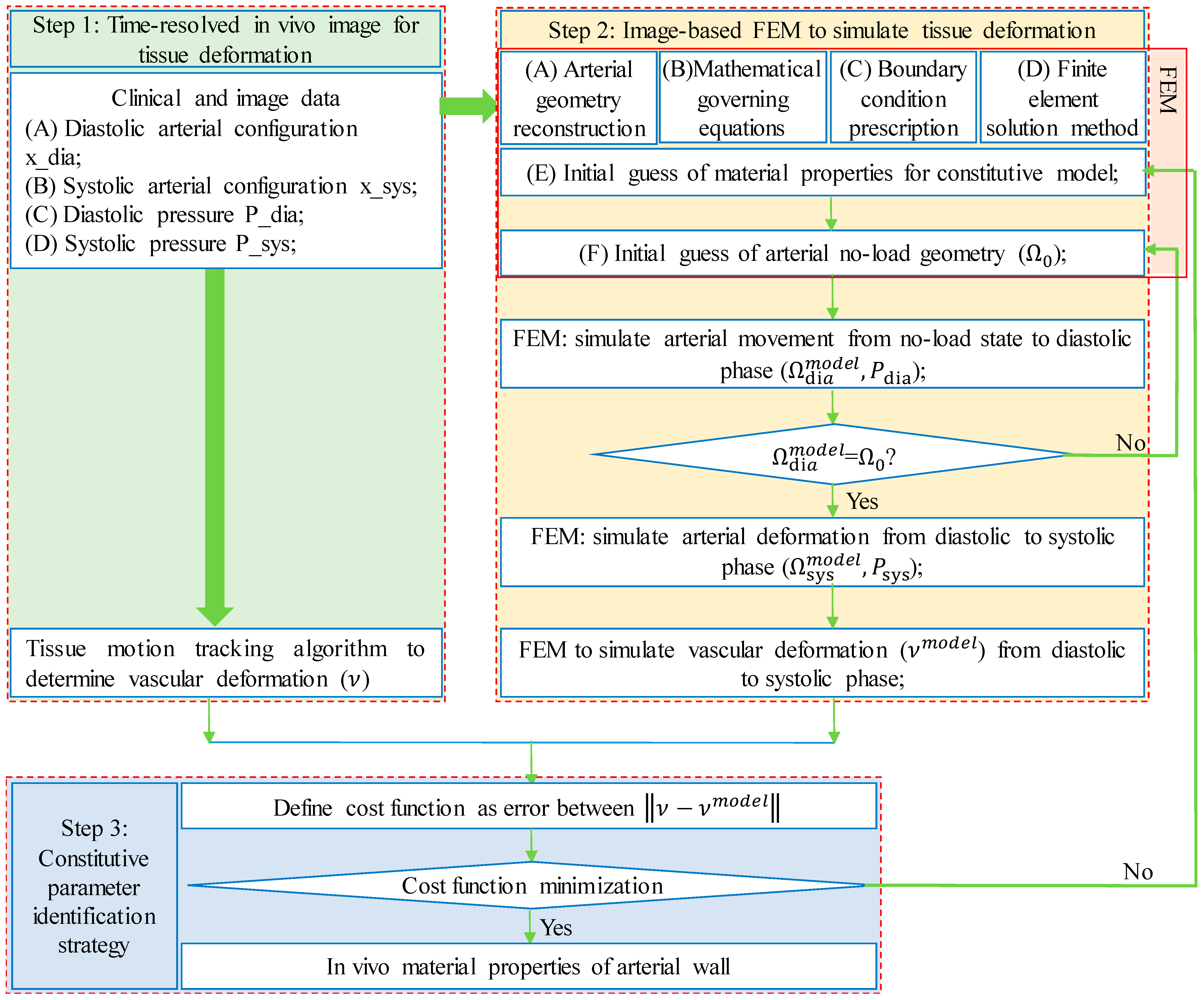
3. Framework of Finite-Element-Model-Based Updating Approach
3.1. Data Acquisition and Vessel/Tissue Motion Tracking
3.2. Image-Based Finite Element Models
3.3. Constitutive Parameter Identification Strategy
4. In Vivo Mechanical Properties of Individual-Specific Arterial Wall Tissue
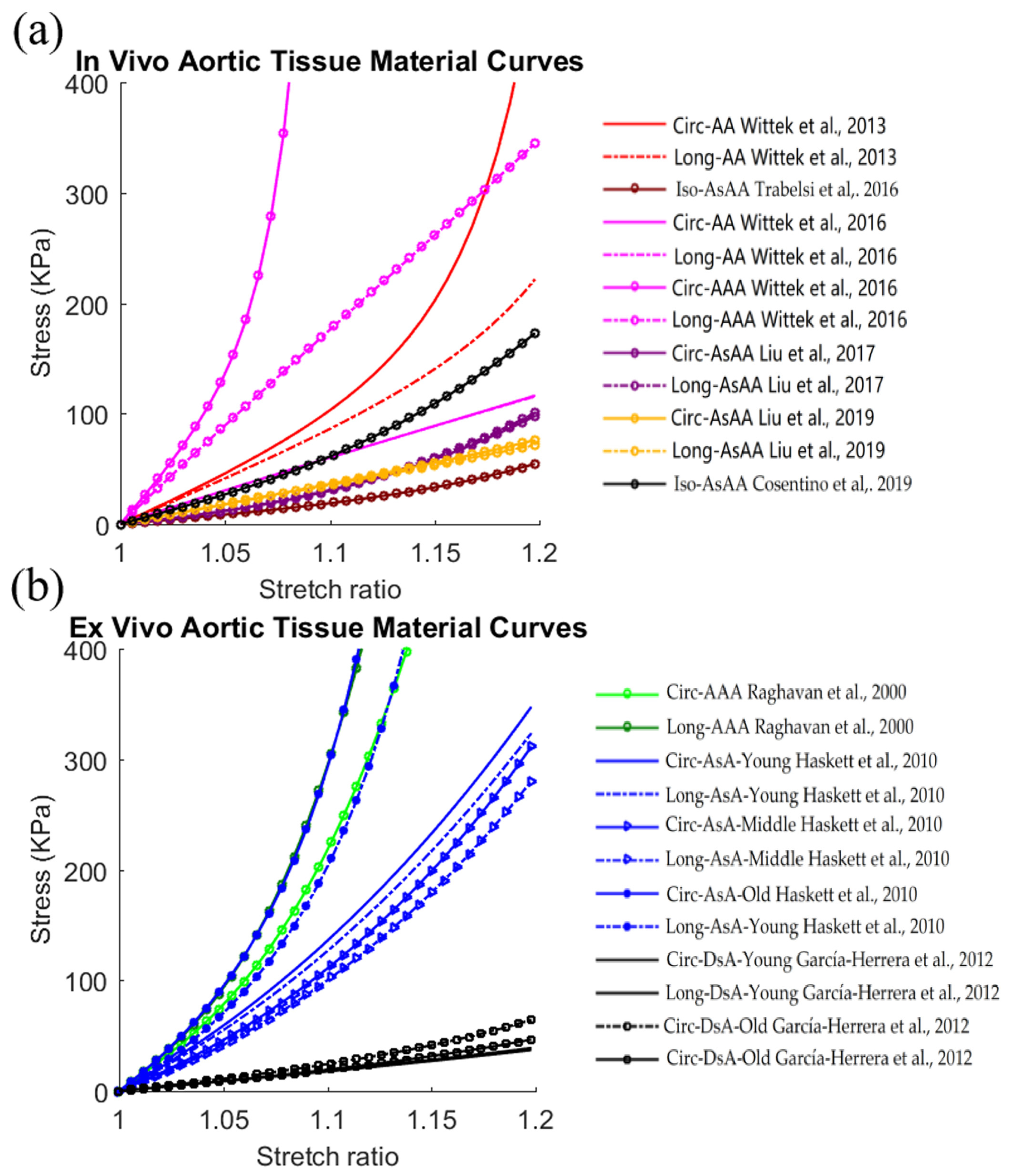
4.1. Aortic Tissue
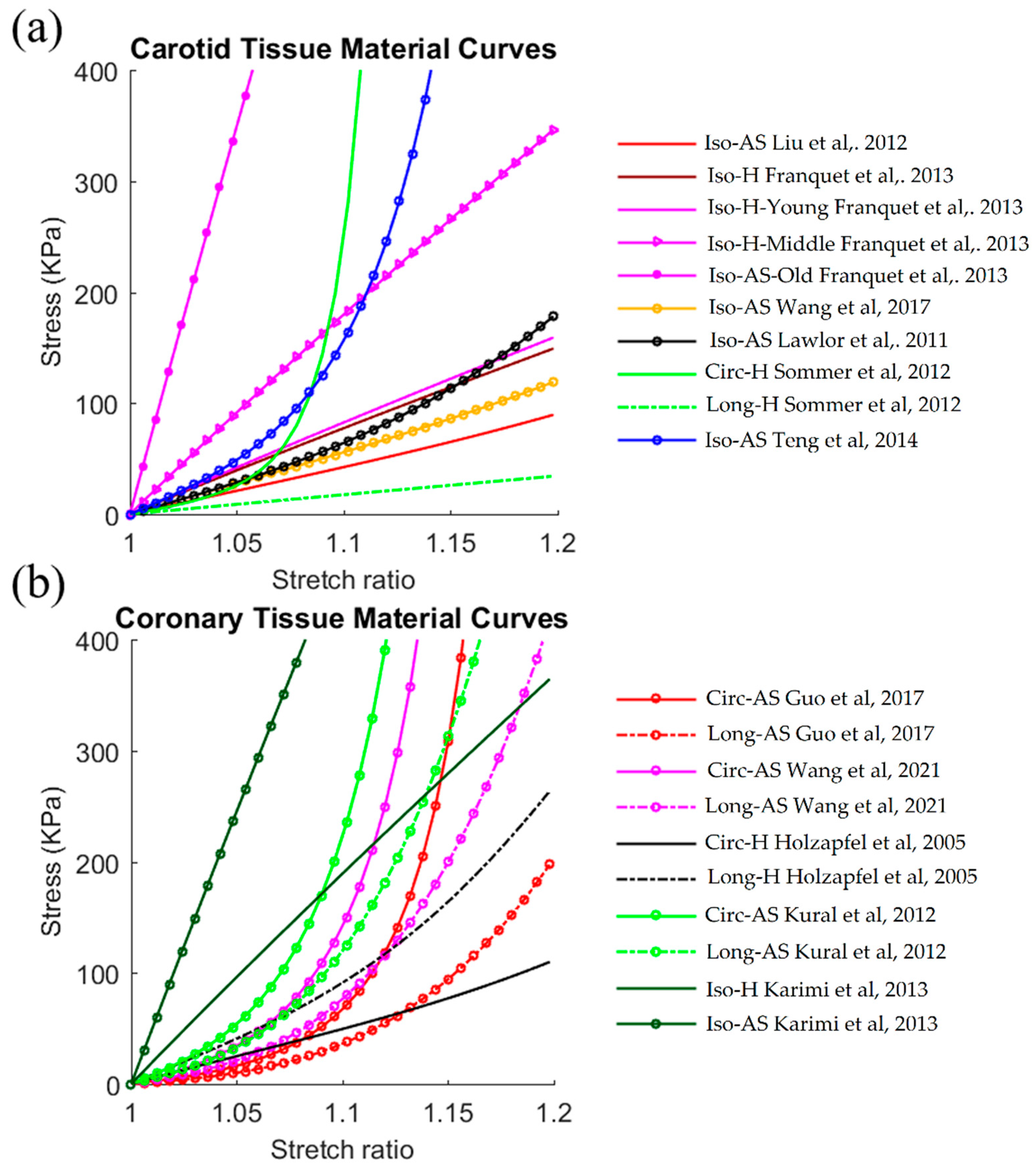
4.2. Carotid and Coronary Arterial Tissues
5. Some Methodological Issues in Finite-Element-Model-Based Updating Approach
5.1. Significance of In Vivo Identification Framework
5.2. Comparison in Tissue Stiffness from FEMBUA and Ex Vivo Experimental Approaches
5.3. Validation of In Vivo Identification Approach
5.4. Method Reproducibility and Noise Sensitivity Analysis
5.5. Modeling Assumptions and Limitations
6. Conclusions Remarks and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic shear stress and its role in atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef] [PubMed]
- Kwak, B.R.; Bäck, M.; Bochaton-Piallat, M.; Caligiuri, G.; Daemen, M.J.A.P.; Davies, P.F.; Hoefer, I.E.; Holvoet, P.; Jo, H.; Krams, R.; et al. Biomechanical factors in atherosclerosis: Mechanisms and clinical implications. Eur. Heart J. 2014, 35, 3013–3020. [Google Scholar] [CrossRef] [PubMed]
- James, F.G.; Mostafa, F.; Michael, I. Selected methods for imaging elastic properties of biological tissues. Annu. Rev. Biomed. Eng. 2003, 5, 57–78. [Google Scholar] [CrossRef]
- Susan, J.Z.; Vojtech, M.; David, A.K. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arter. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef]
- Dirk, W.; Mario, K.; Paul, S.; Frank, S.; Alexander, R.; Kerstin, W.; Wolfgang, H.; Wolfgang, P.; Matthias, P.; Heinz-Peter, S.; et al. Role of left ventricular stiffness in heart failure with normal ejection fraction. Circulation 2008, 117, 2051–2060. [Google Scholar] [CrossRef]
- Stephane, L.; John, C.; Luc, V.B.; Pierre, B.; Cristina, G.; Daniel, H.; Bruno, P.; Charalambos, V.; Ian, W.; Harry, S.-B.; et al. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef]
- Vorp, D.A.; Vande Geest, J.P. Biomechanical determinants of abdominal aortic aneurysm rupture. Arter. Thromb. Vasc. Biol. 2005, 25, 1558–1566. [Google Scholar] [CrossRef]
- Camasão, D.B.; Mantovani, D. The mechanical characterization of blood vessels and their substitutes in the continuous quest for physiological-relevant performances. A critical review. Mater. Today Bio 2021, 10, 100106. [Google Scholar] [CrossRef]
- Moore, J., Jr.; Berry, J.L. Fluid and Solid Mechanical Implications of Vascular Stenting. Ann. Biomed. Eng. 2002, 30, 498–508. [Google Scholar] [CrossRef]
- Fung, Y.C. Biomechanics: Mechanical Properties of Living Tissues; Springer: New York, NY, USA, 1993. [Google Scholar]
- Holzapfel, G.A.; Gasser, T.C.; Ogden, R.W. A New Constitutive Framework for Arterial Wall Mechanics and a Comparative Study of Material Models. J. Elast. 2000, 61, 1–48. [Google Scholar] [CrossRef]
- Walsh, M.T.; Cunnane, E.M.; Mulvihill, J.J.; Akyildiz, A.C.; Gijsen, F.J.H.; Holzapfel, G.A. Uniaxial tensile testing approaches for characterization of atherosclerotic plaques. J. Biomech. 2014, 47, 793–804. [Google Scholar] [CrossRef] [PubMed]
- Macrae, R.A.; Miller, K.; Doyle, B.J. Methods in Mechanical Testing of Arterial Tissue: A Review. Strain 2016, 52, 380–399. [Google Scholar] [CrossRef]
- Hayashi, K. Experimental approaches on measuring the mechanical properties and constitutive laws of arterial walls. J. Biomech. Eng. 1993, 115, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Sacks, M.S.; Sun, W. Multiaxial mechanical behavior of biological materials. Annu. Rev. Biomed. Eng. 2003, 5, 251–284. [Google Scholar] [CrossRef]
- Holzapfel, G.A.; Sommer, G.; Regitnig, P. Anisotropic Mechanical Properties of Tissue Components in Human Atherosclerotic Plaques. J. Biomech. Eng. 2004, 26, 657–665. [Google Scholar] [CrossRef]
- Teng, Z.; Zhang, Y.; Huang, Y.; Feng, J.; Yuan, J.; Lu, Q.; Sutcliffe, M.P.F.; Brown, A.J.; Jing, Z.; Gillard, J.H. Material properties of components in human carotid atherosclerotic plaques: A uniaxial extension study. Acta. Biomater. 2014, 10, 5055–5063. [Google Scholar] [CrossRef]
- Peña, J.A.; Corral, V.; Martínez, M.A.; Peña, E. Over length quantification of the multiaxial mechanical properties of the ascending, descending and abdominal aorta using Digital Image Correlation. J. Mech. Behav. Biomed. Mater. 2018, 77, 434–445. [Google Scholar] [CrossRef]
- Peterson, L.H.; Jensen, R.E.; Parnell, J. Mechanical Properties of Arteries in Vivo. Circ. Res. 1960, 8, 622–639. [Google Scholar] [CrossRef]
- Gosling, R.G.; Budge, M.M. Terminology for Describing the Elastic Behavior of Arteries. Hypertension 2003, 41, 1180–1182. [Google Scholar] [CrossRef]
- Claridge, M.W.; Bate, G.R.; Hoskins, P.R.; Adam, D.J.; Bradbury, A.W.; Wilmink, A.B. Measurement of arterial stiffness in subjects with vascular disease: Are vessel wall changes more sensitive than increase in intima–media thickness? Atherosclerosis 2009, 205, 477–480. [Google Scholar] [CrossRef]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated Aortic Pulse Wave Velocity, a Marker of Arterial Stiffness, Predicts Cardiovascular Events in Well-Functioning Older Adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef] [PubMed]
- Willum-Hansen, T.; Staessen, J.A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic Value of Aortic Pulse Wave Velocity as Index of Arterial Stiffness in the General Population. Circulation 2006, 113, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Stålhand, J.; Klarbring, A.; Karlsson, M. Towards in vivo aorta material identification and stress estimation. Biomech. Model Mechan. 2004, 2, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Bauer, C.A.J.; Holzapfel, G.A. Determination of constitutive equations for human arteries from clinical data. J. Biomech. 2003, 36, 165–169. [Google Scholar] [CrossRef]
- Masson, I.; Boutouyrie, P.; Laurent, S.; Humphrey, J.D.; Zidi, M. Characterization of arterial wall mechanical behavior and stresses from human clinical data. J. Biomech. 2008, 41, 2618–2627. [Google Scholar] [CrossRef]
- Avril, S.; Evans, S.; Miller, K. Inverse problems and material identification in tissue biomechanics. J. Mech. Behav. Biomed. Mater. 2013, 27, 129–131. [Google Scholar] [CrossRef]
- Narayanan, B.; Olender, M.L.; Marlevi, D.; Edelman, E.R.; Nezami, F.R. An inverse method for mechanical characterization of heterogeneous diseased arteries using intravascular imaging. Sci. Rep. 2021, 11, 22540. [Google Scholar] [CrossRef]
- Wittek, A.; Karatolios, K.; Bihari, P.; Schmitz-Rixen, T.; Moosdorf, R.; Vogt, S.; Blasé, C. In vivo determination of elastic properties of the human aorta based on 4D ultrasound data. J. Mech. Behav. Biomed. Mater. 2013, 27, 167–183. [Google Scholar] [CrossRef]
- Trabelsi, O.; Duprey, A.; Favre, J.-P.; Avril, S. Predictive Models with Patient Specific Material Properties for the Biomechanical Behavior of Ascending Thoracic Aneurysms. Ann. Biomed. Eng. 2016, 44, 84–98. [Google Scholar] [CrossRef]
- Franquet, A.; Avril, S.; Le Riche, R.; Badel, P.; Schneider, F.C.; Li, Z.; Boissier, C.; Pierre Favre, J. A New Method for the In Vivo Identification of Mechanical Properties in Arteries From Cine MRI Images: Theoretical Framework and Validation. IEEE Trans. Med. Imaging 2013, 32, 1448–1461. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Zhu, J.; Maehara, A.; Monoly, D.; Samady, H.; Wang, L.; Billiar, K.L.; Zheng, J.; Yang, C.; Mintz, G.S.; et al. Quantify patient-specific coronary material property and its impact on stress/strain calculations using in vivo IVUS data and 3D FSI models: A pilot study. Biomech. Model Mechan. 2017, 16, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Wittek, A.; Derwich, W.; Karatolios, K.; Fritzen, C.P.; Vogt, S.; Schmitz-Rixen, T.; Blasé, C. A finite element updating approach for identification of the anisotropic hyperelastic properties of normal and diseased aortic walls from 4D ultrasound strain imaging. J. Mech. Behav. Biomed. Mater. 2016, 58, 122–138. [Google Scholar] [CrossRef]
- Liu, M.; Liang, L.; Sun, W. A new inverse method for estimation of in vivo mechanical properties of the aortic wall. J. Mech. Behav. Biomed. Mater. 2017, 72, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Liang, L.; Sulejmani, F.; Lou, X.; Iannucci, G.; Chen, E.; Leshnower, B.; Sun, W. Identification of in vivo nonlinear anisotropic mechanical properties of ascending thoracic aortic aneurysm from patient-specific CT scans. Sci. Rep. 2019, 9, 12983. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Canton, G.; Yuan, C.; Yang, C.; Billiar, K.; Teng, Z.; Hoffman, A.H.; Tang, D. Using In Vivo Cine and 3D Multi-Contrast MRI to Determine Human Atherosclerotic Carotid Artery Material Properties and Circumferential Shrinkage Rate and Their Impact on Stress/Strain Predictions. J. Biomech. Eng. 2012, 134, 011008. [Google Scholar] [CrossRef]
- Franquet, A.; Avril, S.; Le Riche, R.; Badel, P.; Schneider, F.C.; Boissier, C.; Favre, J.-P. Identification of the in vivo elastic properties of common carotid arteries from MRI: A study on subjects with and without atherosclerosis. J. Mech. Behav. Biomed. Mater. 2013, 27, 184–203. [Google Scholar] [CrossRef]
- Wang, L.; Zhu, J.; Maehara, A.; Lv, R.; Qu, Y.; Zhang, X.; Guo, X.; Billiar, K.L.; Chen, L.; Ma, G.; et al. Quantifying Patient-Specific in vivo Coronary Plaque Material Properties for Accurate Stress/Strain Calculations: An IVUS-Based Multi-Patient Study. Front. Physiol. 2021, 12, 721195. [Google Scholar] [CrossRef]
- Seo, Y.; Ishizu, T.; Enomoto, Y.; Sugimori, H.; Yamamoto, M.; Machino, T.; Kawamura, R.; Aonuma, K. Validation of 3-dimensional speckle tracking imaging to quantify regional myocardial deformation. Circ. Cardiovasc. Imaging 2009, 2, 451–459. [Google Scholar] [CrossRef]
- Pan, B.; Qian, K.; Xie, H.; Asundi, A. Two-dimensional digital image correlation for in-plane displacement and strain measurement: A review. Meas. Sci. Technol. 2009, 20, 6. [Google Scholar] [CrossRef]
- Mondillo, S.; Galderisi, M.; Mele, D.; Cameli, M.; Lomoriello, V.S.; Zacà, V.; Ballo, P.; D’Andrea, A.; Muraru, D.; Losi, M.; et al. Echocardiography Study Group Of The Italian Society Of Cardiology (Rome, Italy). Speckle-tracking echocardiography: A new technique for assessing myocardial function. J. Ultrasound. Med. 2011, 30, 71–83. [Google Scholar] [CrossRef]
- Yang, C.; Bach, R.G.; Zheng, J.; Naqa, E.I.; Woodard, P.K.; Teng, Z.; Billiar, K.; Tang, D. In vivo IVUS-based 3-D fluid-structure interaction models with cyclic bending and anisotropic vessel properties for human atherosclerotic coronary plaque mechanical analysis. IEEE Trans. Bio-Med. Eng. 2009, 56, 2420–2428. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, H.J.; Gholipour, A.; Ghayesh, M.H.; Zander, A.C.; Psaltis, P.J. A review on the biomechanics of coronary arteries. Int. J. Eng. Sci. 2020, 147, 103201. [Google Scholar] [CrossRef]
- Speelman, L.; Bosboom, E.M.; Schurink, G.W.; Buth, J.; Breeuwer, M.; Jacobs, M.J.; van de Vosse, F.N. Initial stress and nonlinear material behavior in patient-specific AAA wall stress analysis. J. Biomech. 2009, 7, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Gee, M.W.; Förster, C.H.; Wall, W.A. A Computational Strategy for Prestressing Patient-Specific Biomechanical Problems Under Finite Deformation. Int. J. Numer. Methods Biomed. Eng. 2010, 26, 52–72. [Google Scholar] [CrossRef]
- Tang, D.; Yang, C.; Zheng, J.; Woodard, P.K.; Sicard, G.A.; Saffitz, J.E.; Yuan, C. 3D MRI-Based Multicomponent FSI Models for Atherosclerotic Plaques. Ann. Biomed. Eng. 2004, 32, 947–960. [Google Scholar] [CrossRef]
- Avril, S.; Badel, P.; Duprey, A. Anisotropic and hyperelastic identification of in vitro human arteries from full-field optical measurements. J. Biomech. 2010, 43, 2978–2985. [Google Scholar] [CrossRef]
- Maso Talou, G.D.; Blanco, P.J.; Ares, G.D.; Guedes Bezerra, C.; Lemos, P.A.; Feijóo, R.A. Mechanical Characterization of the Vessel Wall by Data Assimilation of Intravascular Ultrasound Studies. Front. Physiol. 2018, 28, 292. [Google Scholar] [CrossRef]
- Raghavan, M.L.; Vorp, D.A. Toward a biomechanical tool to evaluate rupture potential of abdominal aortic aneurysm: Identification of a finite strain constitutive model and evaluation of its applicability. J. Biomech. 2000, 33, 475–482. [Google Scholar] [CrossRef]
- Gasser, T.C.; Ogden, R.W.; Holzapfel, G.A. Hyperelastic modelling of arterial layers with distributed collagen fibre orientations. J. R. Soc. Interface 2006, 3, 15–35. [Google Scholar] [CrossRef]
- Holzapfel, G.A.; Sommer, G.; Gasser, C.T.; Regitnig, P. Determination of layer-specific mechanical properties of human coronary arteries with nonatherosclerotic intimal thickening and related constitutive modeling. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, 2048–2058. [Google Scholar] [CrossRef] [Green Version]
- Jankowska, M.A.; Bartkowiak-Jowsa, M.; Bedzinski, R. Experimental and constitutive modeling approaches for a study of biomechanical properties of human coronary arteries. J. Mech. Behav. Biomed. Mater. 2015, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Yang, C.; Zheng, J.; Bach, R.; Muccigrosso, D.; Woodard, P.K.; Tang, D. 3D MRI-based multicomponent thin layer structure only plaque models for atherosclerotic plaques. J. Biomech. 2016, 49, 2726–2733. [Google Scholar] [CrossRef]
- Baldewsing, R.A.; Danilouchkine, M.G.; Mastik, F.; Schaar, J.A.; Serruys, P.W.; van der Steen, F.W.A. An Inverse Method for Imaging the Local Elasticity of Atherosclerotic Coronary Plaques. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Agnese, V.; Raffa, G.M.; Gentile, G.; Bellavia, D.; Zingales, M.; Pilato, M.; Pasta, S. On the role of material properties in ascending thoracic aortic aneurysms. Comput. Biol. Med. 2019, 109, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Chandran, K.B.; Mun, J.H.; Choi, K.K.; Chen, J.S.; Hamilton, A.; Nagaraj, A.; McPherson, D.D. A method for in-vivo analysis for regional arterial wall material property alterations with atherosclerosis: Preliminary results. Med. Eng. Phys. 2003, 25, 289–298. [Google Scholar] [CrossRef]
- Nelder, J.A.; Mead, R. A Simplex Method for Function Minimization. Comput. J. 1965, 7, 308–313. [Google Scholar] [CrossRef]
- Wang, Q.; Canton, G.; Guo, J.; Guo, X.; Hatsukami, T.S.; Billiar, K.L.; Yuan, C.; Wu, Z.; Tang, D. MRI-based patient-specific human carotid atherosclerotic vessel material property variations in patients, vessel location and long-term follow up. PLoS ONE 2017, 12, e0180829. [Google Scholar] [CrossRef]
- Ghassan, S.K. Biomechanics of the cardiovascular system: The aorta as an illustratory example. J. R. Soc. Interface 2006, 3, 719–740. [Google Scholar] [CrossRef]
- Haskett, D.; Johnson, G.; Zhou, A.; Utzinger, U.; Vande Geest, J. Microstructural and biomechanical alterations of the human aorta as a function of age and location. Biomech. Model Mechanobiol. 2010, 9, 725–736. [Google Scholar] [CrossRef]
- García-Herrera, C.M.; Celentano, D.J.; Cruchaga, M.A.; Rojo, F.J.; Atienza, J.M.; Guinea, G.V.; Goicolea, J.M. Mechanical characterisation of the human thoracic descending aorta: Experiments and modelling. Comput. Methods Biomech. Biomed. Engin. 2012, 15, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, M.G.; O’Donnell, M.R.; O’Connell, B.M.; Walsh, M.T. Experimental determination of circumferential properties of fresh carotid artery plaques. J. Biomech. 2011, 44, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Sommer, G.; Holzapfel, G.A. 3D constitutive modeling of the biaxial mechanical response of intact and layer-dissected human carotid arteries. J. Mech. Behav. Biomed. Mater. 2012, 5, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Kural, M.H.; Cai, M.; Tang, D.; Gwyther, T.; Zheng, J.; Billiar, K.L. Planar biaxial characterization of diseased human coronary and carotid arteries for computational modeling. J. Biomech. 2012, 45, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Navidbakhsh, M.; Shojaei, A.; Faghihi, S. Measurement of the uniaxial mechanical properties of healthy and atherosclerotic human coronary arteries. Mater. Sci. Eng. C. Mater Biol. Appl. 2013, 33, 2550–2554. [Google Scholar] [CrossRef] [PubMed]
- Niestrawska, J.A.; Viertler, C.; Regitnig, P.; Cohnert, T.U.; Sommer, G.; Holzapfel, G.A. Microstructure and mechanics of healthy and aneurysmatic abdominal aortas: Experimental analysis and modelling. J. R. Soc. Interface 2016, 13, 20160620. [Google Scholar] [CrossRef]
- Zhao, X.; Raghavan, M.L.; Lu, J. Identifying heterogeneous anisotropic properties in cerebral aneurysms: A pointwise approach. Biomech. Model. Mechanobiol. 2011, 10, 177–189. [Google Scholar] [CrossRef]
- Yu, H.; Del Nido, P.J.; Geva, T.; Yang, C.; Tang, A.; Wu, Z.; Rathod, R.H.; Huang, X.; Billiar, K.L.; Tang, D. Patient-specific in vivo right ventricle material parameter estimation for patients with tetralogy of Fallot using MRI-based models with different zero-load diastole and systole morphologies. Int. J. Cardiol. 2019, 276, 93–99. [Google Scholar] [CrossRef]
- Affagard, J.S.; Feissel, P.; Bensamoun, S.F. Identification of hyperelastic properties of passive thigh muscle under compression with an inverse method from a displacement field measurement. J. Biomech. 2015, 48, 4081–4086. [Google Scholar] [CrossRef]
- Tran, H.V.; Charleux, F.; Rachik, M.; Ehrlacher, A.; Ho Ba Tho, M.C. In vivo characterization of the mechanical properties of human skin derived from MRI and indentation techniques. Comput. Methods Biomech. Biomed. Eng. 2007, 10, 401–407. [Google Scholar] [CrossRef]
- Moerman, K.M.; Holt, C.A.; Evans, S.L.; Simms, C.K. Digital image correlation and finite element modelling as a method to determine mechanical properties of human soft tissue in vivo. J. Biomech. 2009, 42, 1150–1153. [Google Scholar] [CrossRef] [Green Version]
- Meuwissen, M.H.H.; Oomens, C.W.J.; Baaijens, F.P.T.; Petterson, R.; Janssen, J.D. Determination of the elasto-plastic properties of aluminium using a mixed numerical–experimental method. J. Mater Process. Technol. 1998, 75, 204–211. [Google Scholar] [CrossRef]
- Davis, F.M.; Luo, Y.; Avril, S.; Duprey, A.; Lu, J. Local mechanical properties of human ascending thoracic aneurysms. J. Mech. Behav. Biomed. Mater. 2016, 61, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Roach, M.R.; Burton, A.C. The reason for the shape of the distensibility curves of arteries. Can. J. Biochem. Physiol. 1957, 35, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, D.; Cartier, R.; Mongrain, R.; Leask, R.L. Regional dependency of the vascular smooth muscle cell contribution to the mechanical properties of the pig ascending aortic tissue. J. Biomech. 2010, 43, 2448–2451. [Google Scholar] [CrossRef]
- Fung, Y.C.; Liu, S.Q. Strain distribution in small blood vessel with zero-stress state taken into consideration. Am. J. Physiol. 1992, 262, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, J.; Dubreuil, O.; Tracqui, P.; Le Floc’h, S.; Rioufol, G.; Chalabreysse, L.; Thivolet, F.; Pettigrew, R.I.; Finet, G. Influence of residual stress/strain on the biomechanical stability of vulnerable coronary plaques: Potential impact for evaluating the risk of plaque rupture. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, 1987–1996. [Google Scholar] [CrossRef]
- Singh, T.P.; Moxon, J.V.; Gasser, T.C.; Golledge, J. Systematic Review and Meta-Analysis of Peak Wall Stress and Peak Wall Rupture Index in Ruptured and Asymptomatic Intact Abdominal Aortic Aneurysms. J. Am. Heart Assoc. 2021, 10, e019772. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wu, W.; Samant, S.; Khan, B.; Kassab, G.S.; Watanabe, Y.; Murasato, Y.; Sharzehee, M.; Makadia, J.; Zolty, D.; et al. Patient-specific computational simulation of coronary artery bifurcation stenting. Sci. Rep. 2021, 11, 16486. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Image Modality | Temporal Resolution | Spatial Resolution | Artery | Strength and Weakness in Arterial Wall Detection | Reference |
|---|---|---|---|---|---|
| t + 3D (4D) US | ~10 frames/s | ~0.5 mm | Aorta | Cheap, fast and easy way to detect arterial boundaries and tissue compositions, but inter- and intra-observer variability in image interpretation; | [29,33] |
| ECG-gated CT | ~10 frames/cardiac cycle | ~0.5 mm | Aorta | Superb calcified tissue detection and lumen detection; limited in detecting other plaque compositions, such as lipid and vessel wall; | [30,34,35] |
| Cine MRI | ~50 frames/cardiac cycle | ~0.6 mm | Carotid | Detection of the whole vascular cross-section with superior soft-tissue contrast, but long scanning time; | [31,36,37] |
| Cine IVUS | ~30 frames/s | 100 µm | Coronary | High resolution and large penetration depth for arterial tissue detection, also can detect arterial tissue compositions; | [32,38] |
| Reference | Tissue Sample Information | Material Model | Imaging/Experiment Techniques | Effective Young’s Modulus |
|---|---|---|---|---|
| In Vivo Aorta | ||||
| [29] | 5 AA samples from 5 healthy subjects | GOH model | t + 3D US | Ec = 969.5 kPa Ea = 843.7 kPa |
| [30] | 5 AsAA samples from 5 patients | Demiray model | ECG-gated CT | Ec = Ea = 180.3 kPa |
| [33] | 1 AA sample from 1 healthy subject | GOH model | t + 3D US | Ec = 605.7 kPa Ea = 605.4 kPa |
| 1 AAA sample from 1 patient | Ec = 5576.7 kPa Ea = 1770.2 kPa | |||
| [34] | 4 AsAA samples from 4 patients | GOH model | ECG-gated CT | Ec = 270.2 kPa Ea = 276.5 kPa |
| [35] | 4 AsAA samples from 4 patients | GOH model | ECG-gated CT | Ec = 363.1 kPa Ea = 355.7 kPa |
| [55] | 9 AsAA samples from 9 patients | Yeoh model | ECG-gated CT | Ec = Ea = 573.9 kPa |
| Ex Vivo Aorta | ||||
| [49] | 69 AAA specimens | Yeoh model | Uniaxial testing | Ec = 2382.4 kPa Ea = 1856.3 kPa |
| [60] | 6 AsA specimens from donors with age 0 to 30 | GOH model | Biaxial testing | Ec = 1268.4 kPa Ea = 1182.1 kPa |
| 6 AsA specimens from donors with age 31 to 60 | Ec = 1025.5 kPa Ea = 905.9 kPa | |||
| 17 AsA specimens from donors with age above 61 | Ec = 2365.8 kPa Ea = 1698.6 kPa | |||
| [61] | 5 DsA specimens from 5 young donors with age 20 to 36 | MR model | Uniaxial testing | Ec = 181.5 kPa Ea = 176.0 kPa |
| 5 DsA specimens from 5 old donors with age 45 to 60 | Ec = 232.0 kPa Ea = 186.5 kPa | |||
| In Vivo Carotid | ||||
| [36] | 12 atherosclerotic carotid samples from 12 patients | MR model | Cine MRI | Ec = Ea = 422.6 kPa |
| [31] | 2 carotid samples from 2 healthy subjects | Hookean model | Cine MRI | Ec = Ea = 781.8 kPa |
| [37] | 4 carotid samples from 4 young healthy subjects with age 24 to 26 | Hookean model | Cine MRI | Ec = Ea = 833.7 kPa |
| 5 carotid samples from 5 middle-age healthy subjects with age 51 to 63 | Ec = Ea = 1815.3 kPa | |||
| 4 atherosclerotic carotid samples from 4 old patients with age 68 to 76 | Ec = Ea = 6926.2 kPa | |||
| [58] | 81 atherosclerotic carotid samples from 8 patients | MR model | Cine MRI | Ec = Ea = 555.1 kPa |
| Ex Vivo Carotid | ||||
| [62] | 14 atherosclerotic carotid specimens from 14 patients | Yeoh model | Uniaxial testing | Ec = Ea = 606.2 kPa |
| [63] | 11 common carotid specimens from 11 relatively healthy subjects | Hozapfel2005 model | Extension-inflation tests | Ec = 1235.7 kPa Ea = 176.7 kPa |
| [17] | 59 atherosclerotic carotid specimens of fibrous cap | MR model | Uniaxial testing | Ec = Ea = 1245.4 kPa |
| In Vivo Coronary | ||||
| [32] | 2 atherosclerotic coronary samples from 1 patient | MR model | Cine IVUS | Ec = 484.6 kPa Ea = 279.8 kPa |
| [38] | 20 atherosclerotic coronary samples from 13 patients | MR model | Cine IVUS | Ec = 1022.5 kPa Ea = 590.6 kPa |
| Ex Vivo Coronary | ||||
| [51] | 13 coronary intima specimens from 13 relatively healthy subjects | Hozapfel2005 model | Uniaxial testing | Ec = 497.5 kPa Ea = 862.6 kPa |
| [64] | 4 coronary specimens from 2 relatively healthy subjects | MR model | Biaxial testing | Ec = 1602.5 kPa Ea = 925.3 kPa |
| [65] | 14 healthy coronary specimens | Hookean model | Uniaxial testing | Ec = Ea = 1909.5 kPa |
| 8 atherosclerotic coronary specimens | Ec = Ea = 4864.1 kPa | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Maehara, A.; Lv, R.; Guo, X.; Zheng, J.; Billiar, K.L.; Mintz, G.S.; Tang, D. Image-Based Finite Element Modeling Approach for Characterizing In Vivo Mechanical Properties of Human Arteries. J. Funct. Biomater. 2022, 13, 147. https://doi.org/10.3390/jfb13030147
Wang L, Maehara A, Lv R, Guo X, Zheng J, Billiar KL, Mintz GS, Tang D. Image-Based Finite Element Modeling Approach for Characterizing In Vivo Mechanical Properties of Human Arteries. Journal of Functional Biomaterials. 2022; 13(3):147. https://doi.org/10.3390/jfb13030147
Chicago/Turabian StyleWang, Liang, Akiko Maehara, Rui Lv, Xiaoya Guo, Jie Zheng, Kisten L. Billiar, Gary S. Mintz, and Dalin Tang. 2022. "Image-Based Finite Element Modeling Approach for Characterizing In Vivo Mechanical Properties of Human Arteries" Journal of Functional Biomaterials 13, no. 3: 147. https://doi.org/10.3390/jfb13030147