
A Parametric Study of Flushing Conditions for Improvement of Angioscopy Visibility

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
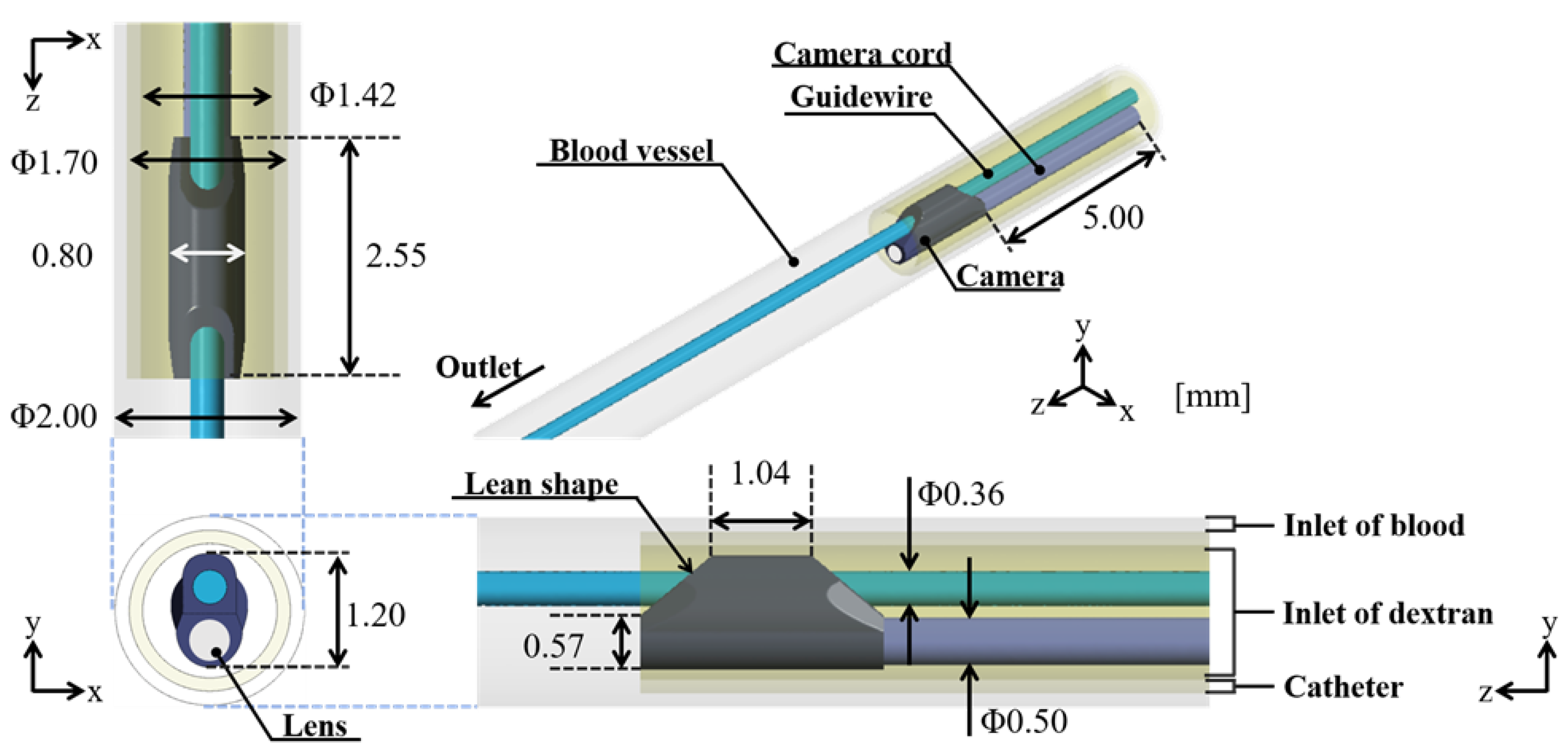
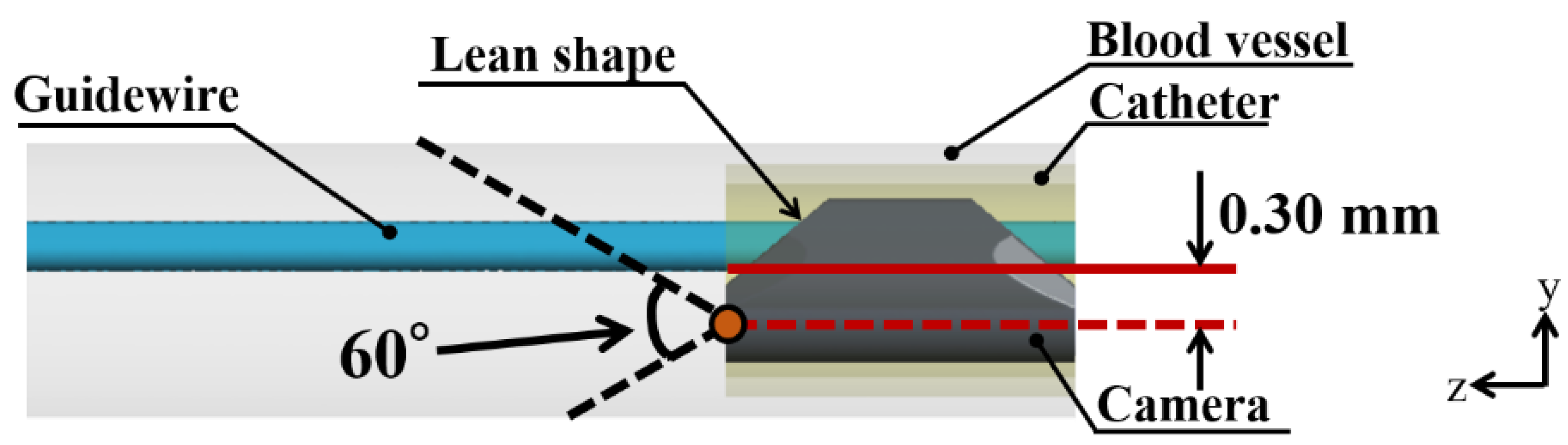
2.1. Model
2.2. Boundary Condition
2.3. Analysis Conditions
2.4. Evaluation Indices
3. Results
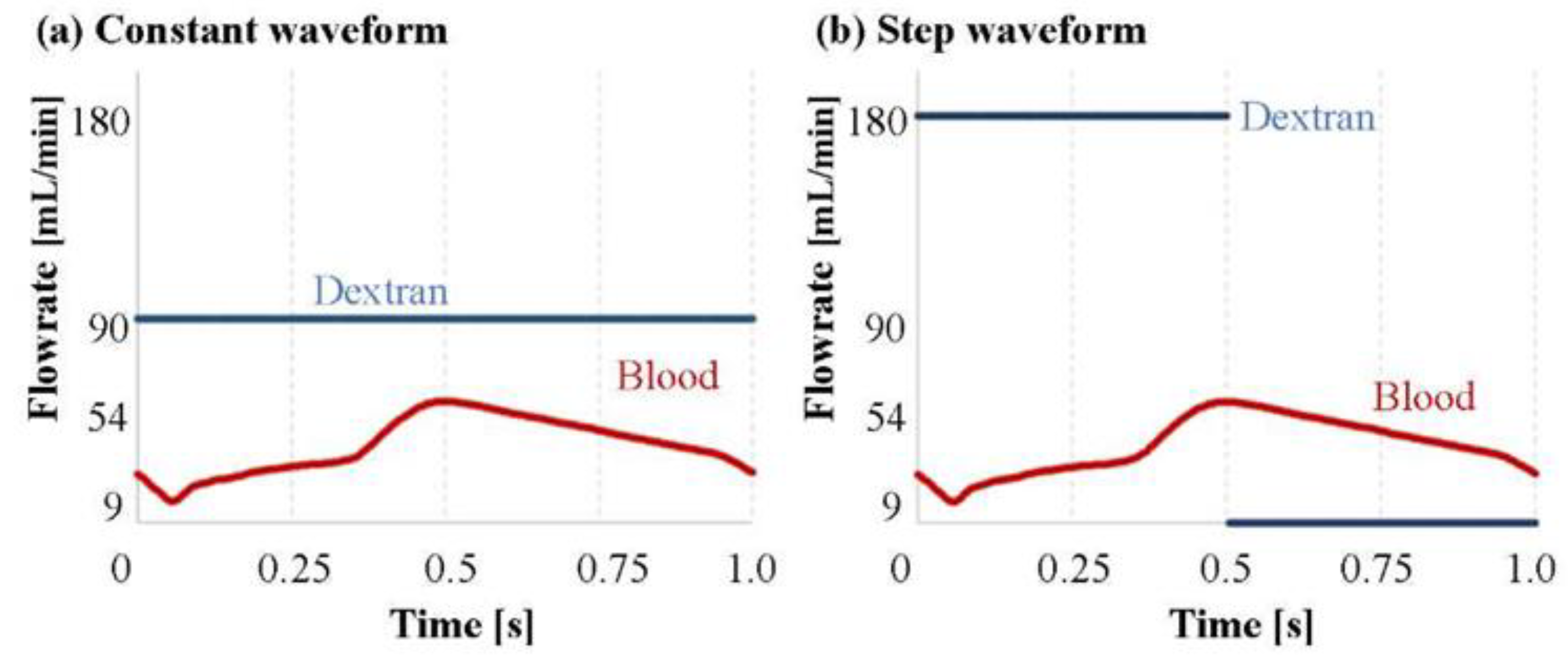
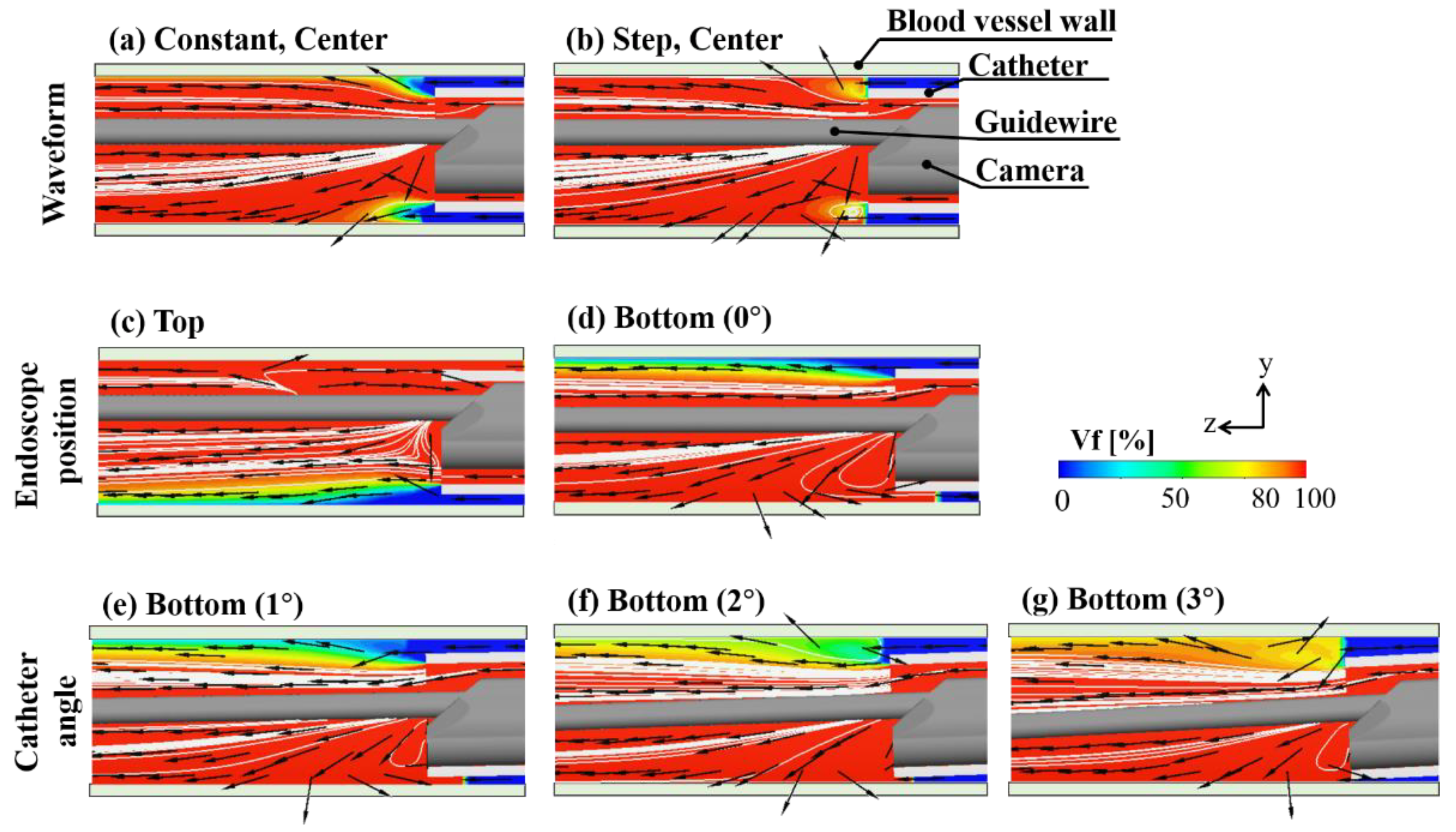
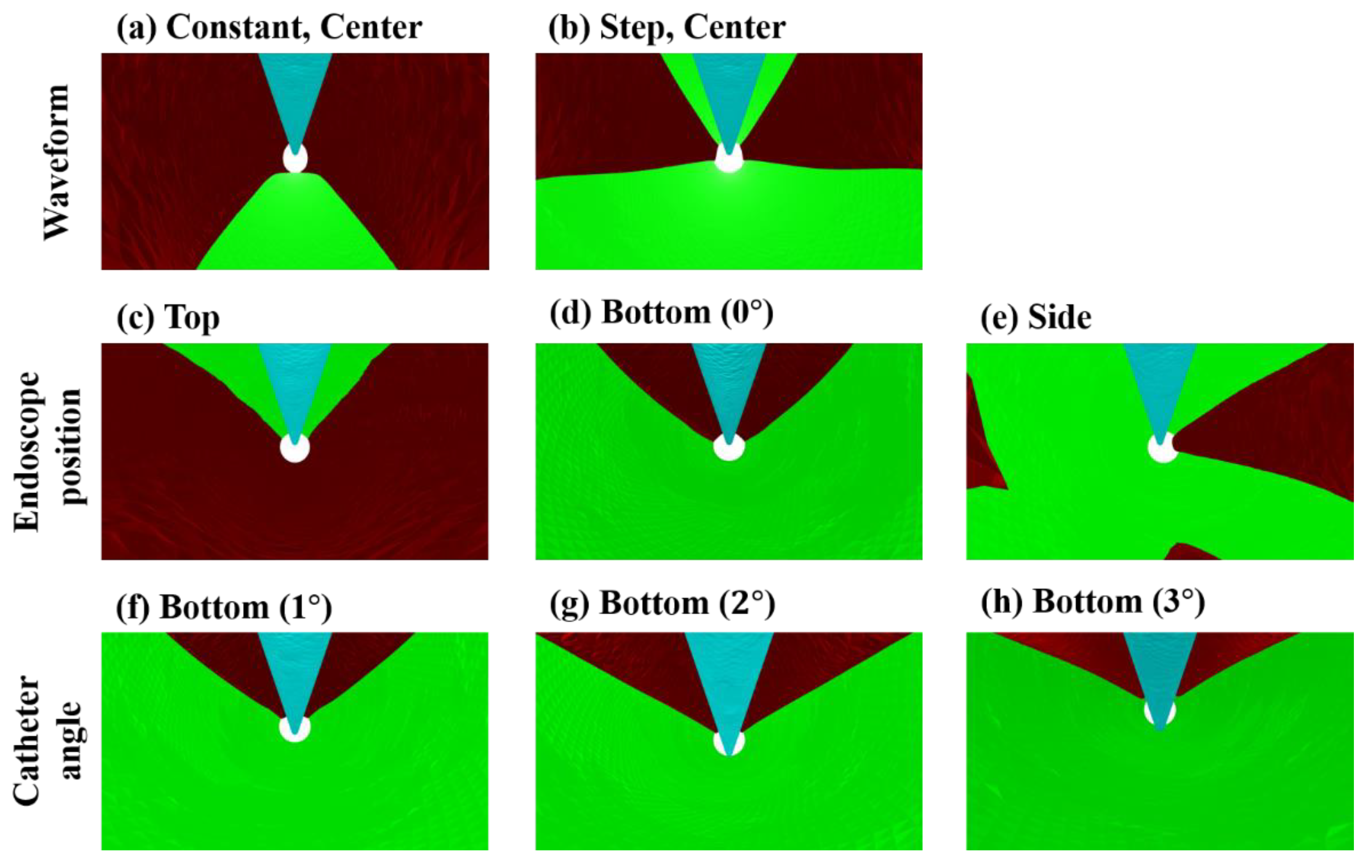
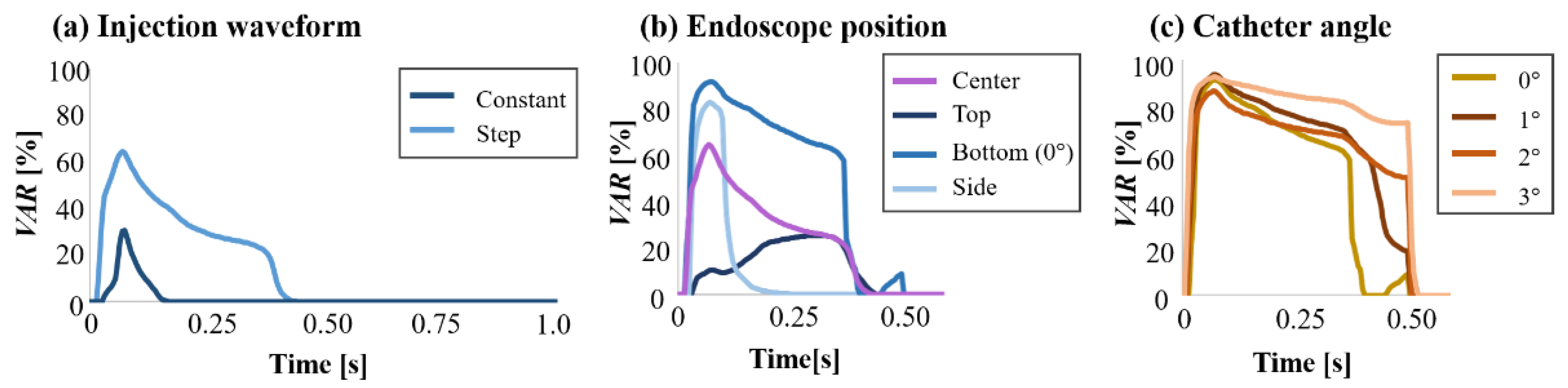
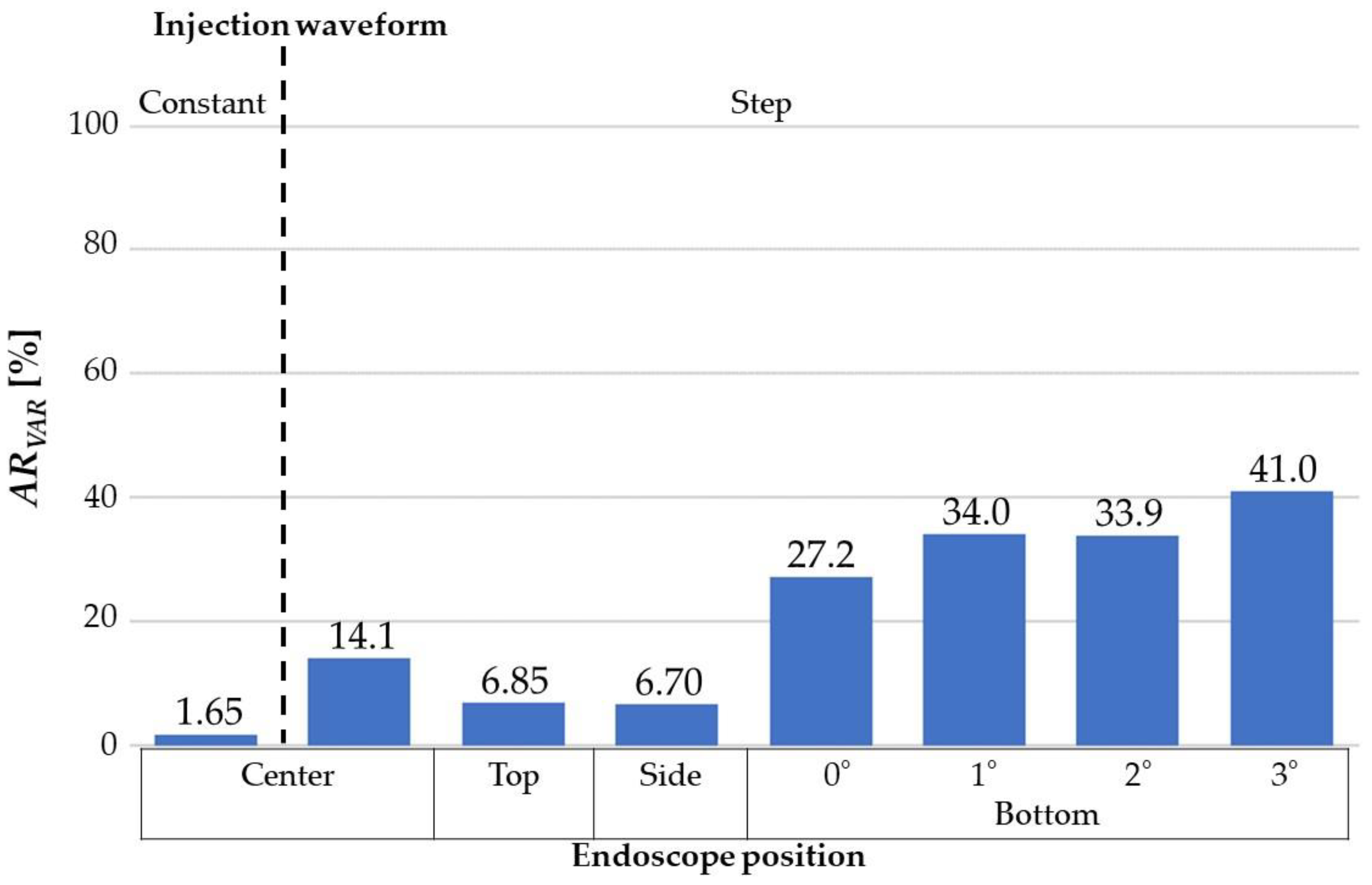
3.1. Effect of Injection Waveform
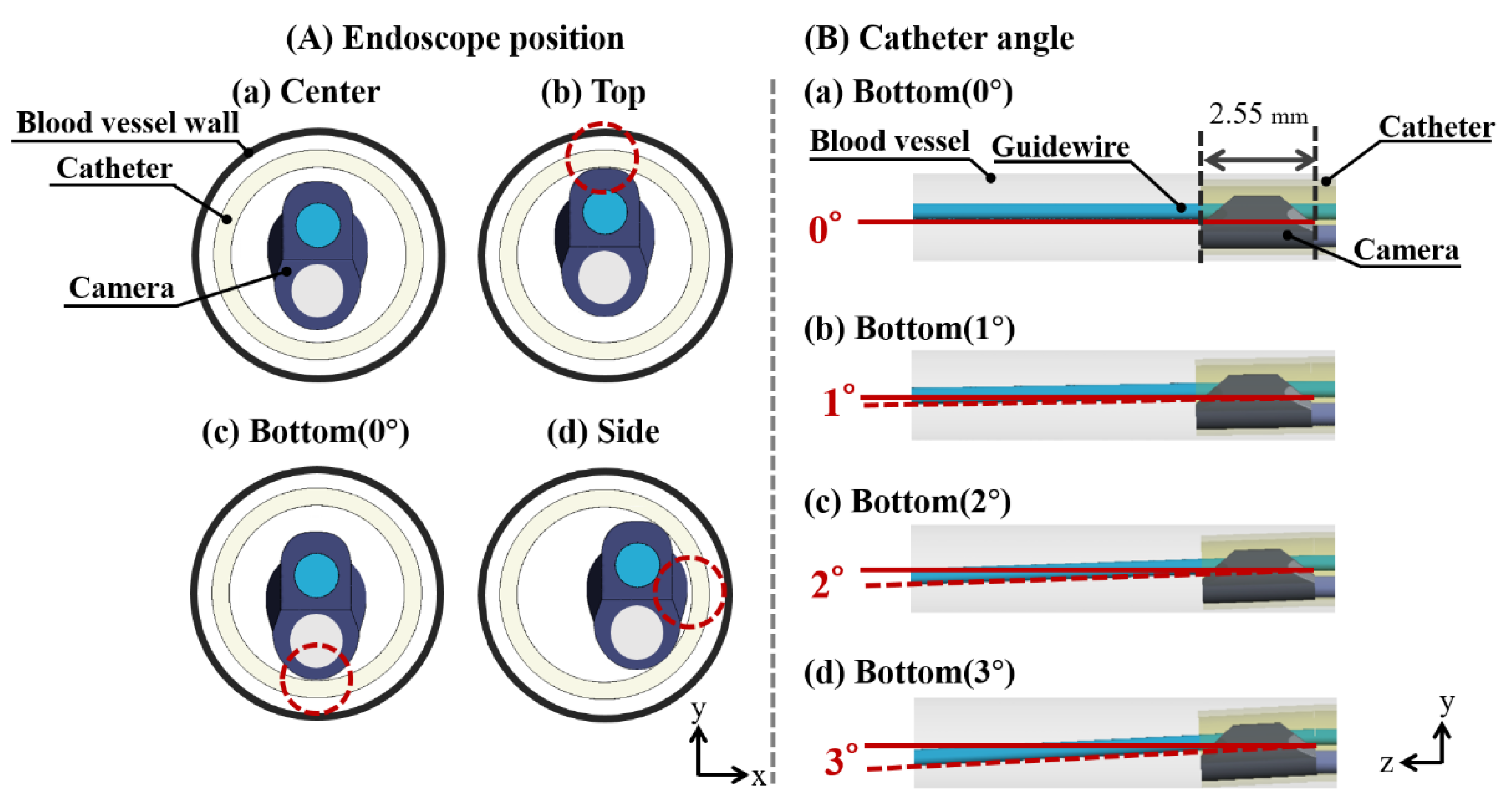
3.2. Effect of Endoscope Position
3.3. Effect of Catheter Angle
4. Discussion
4.1. The Effect of Injection
4.2. The Effect of Angioscopy Shape on Visibility Improvement
4.3. The Effects of the Parameters in Clinical Situations
4.4. Evaluation Indices
4.5. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from Ischemic Heart Disease: Analysis of Data from the World Health Organization and Coronary Artery Disease Risk Factors from NCD Risk Factor Collaboration. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Social Security. Cardiovascular Disability Criteria Cardiovascular Disability: Updating the Social Security Listings; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Nakamura, F. Clinical Application of Coronary Angioscopy for Diagnosing and Treating Coronary Artery Disease. BME 2005, 43, 8–11. [Google Scholar] [CrossRef]
- Ueda, Y.; Ohtani, T.; Shimizu, M.; Hirayama, A.; Kodama, K. Assessment of Plaque Vulnerability by Angioscopic Classification of Plaque Color. Am. Heart J. 2004, 148, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Hitchner, E.; Zayed, M.A.; Lee, G.; Morrison, D.; Lane, B.; Zhou, W. Intravascular Ultrasound as a Clinical Adjunct for Carotid Plaque Characterization. J. Vasc. Surg. 2014, 59, 774–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsugi, M.; Takayama, K.; Myouchin, K.; Wada, T.; Nakagawa, I.; Nakagawa, H.; Taoka, T.; Kurokawa, S.; Nakase, H.; Kichikawa, K. Carotid Artery Stenting: Investigation of Plaque Protrusion Incidence and Prognosis. JACC Cardiovasc. Interv. 2017, 10, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, N.; Ogata, N.; Ikari, Y. Plaque Protrusion Detected by Intravascular Ultrasound during Carotid Artery Stenting. J. Stroke Cerebrovasc. Dis. 2014, 23, 2622–2625. [Google Scholar] [CrossRef] [PubMed]
- De Donato, G.; Setacci, F.; Sirignano, P.; Galzerano, G.; Cappelli, A.; Setacci, C. Optical Coherence Tomography after Carotid Stenting: Rate of Stent Malapposition, Plaque Prolapse and Fibrous Cap Rupture According to Stent Design. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 579–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimura, S.; Kawasaki, M.; Yamada, K.; Hattori, A.; Nishigaki, K.; Minatoguchi, S.; Iwama, T. Optical Coherence Tomography (OCT): A New Imaging Tool during Carotid Artery Stenting. In Optical Coherence Tomography; IntechOpen: London, UK, 2013. [Google Scholar]
- Kondo, H.; Kiura, Y.; Sakamoto, S.; Okazaki, T.; Yamasaki, F.; Iida, K.; Tominaga, A.; Kurisu, K. Comparative Evaluation of Angioscopy and Intravascular Ultrasound for Assessing Plaque Protrusion during Carotid Artery Stenting Procedures. World Neurosurg. 2019, 125, e448–e455. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.B.; Nelson, C.L.; Califf, R.M.; Harrell, F.E.; Lee, K.L.; Jones, R.H.; Fortin, D.F.; Stack, R.S.; Glower, D.D.; Smith, L.R.; et al. Continuing Evolution of Therapy for Coronary Artery Disease. Initial Results from the Era of Coronary Angioplasty. Circulation 1994, 89, 2015–2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, T.; Imanishi, T.; Takarada, S.; Kuroi, A.; Ueno, S.; Yamano, T.; Tanimoto, T.; Matsuo, Y.; Masho, T.; Kitabata, H.; et al. Implication of Plaque Color Classification for Assessing Plaque Vulnerability: A Coronary Angioscopy and Optical Coherence Tomography Investigation. JACC Cardiovasc. Interv. 2008, 1, 74–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotani, J.; Awata, M.; Nanto, S.; Uematsu, M.; Oshima, F.; Minamiguchi, H.; Mintz, G.S.; Nagata, S. Incomplete Neointimal Coverage of Sirolimus-Eluting Stents: Angioscopic Findings. J. Am. Coll. Cardiol. 2006, 47, 2108–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komatsu, S.; Ohara, T.; Takahashi, S.; Takewa, M.; Minamiguchi, H.; Imai, A.; Kobayashi, Y.; Iwa, N.; Yutani, C.; Hirayama, A.; et al. Early Detection of Vulnerable Atherosclerotic Plaque for Risk Reduction of Acute Aortic Rupture and Thromboemboli and Atheroemboli Using Non-Obstructive Angioscopy. Circ. J. 2015, 79, 742–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, Y.; Asakura, M.; Yamaguchi, O.; Hirayama, A.; Hori, M.; Kodama, K. The Healing Process of Infarct-Related Plaques: Insights from 18 Months of Serial Angioscopic Follow-Up. J. Am. Coll. Cardiol. 2001, 38, 1916–1922. [Google Scholar] [CrossRef] [Green Version]
- Harken, D.E.; Glidden, E.M. Experiments in Intracardiac Surgery. J. Thorac. Surg. 1943, 12, 566–572. [Google Scholar] [CrossRef]
- Komatsu, S.; Ohara, T.; Takahashi, S.; Takewa, M.; Yutani, C.; Kodama, K. Improving the Visual Field in Coronary Artery by with Non-Obstructive Angioscopy: Dual Infusion Method. Int. J. Cardiovasc. Imaging 2017, 33, 789–796. [Google Scholar] [CrossRef]
- Mitsutake, Y.; Ueno, T. The Role of Coronary Angioscopy in the BRS Era. J. Jpn. Coron. Assoc. 2017, 23, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhang, M.; Tupin, S.; Mitsuzuka, K.; Nakayama, T.; Anzai, H.; Ohta, M. Flush Flow Behaviour Affected by the Morphology of Intravascular Endoscope: A Numerical Simulation and Experimental Study. Front. Physiol. 2021, 12, 733767. [Google Scholar] [CrossRef]
- Yamakoshi, K.; Tanaka, S. Endoscope and Blood Vessel Endoscope System. JP Patent P2011-87859A, 2011. [Google Scholar]
- Okayama, K.; Nanto, S.; Sakata, Y. Vascular Endoscope Catheter and Vascular Endoscope. JP Patent P2019-115755A, 2019. [Google Scholar]
- Faisal, S. Hemodynamics of Endoscopic Imaging of Chronic Total Occlusions. Master’s Thesis, University of Washington, Seattle, WA, USA, 2018. [Google Scholar]
- Saitta, S.; Pirola, S.; Piatti, F.; Votta, E.; Lucherini, F.; Pluchinotta, F.; Carminati, M.; Lombardi, M.; Geppert, C.; Cuomo, F.; et al. Evaluation of 4D Flow MRI-Based Non-Invasive Pressure Assessment in Aortic Coarctations. J. Biomech. 2019, 94, 13–21. [Google Scholar] [CrossRef]
- Xie, X.; Wang, Y.; Zhu, H.; Zhou, H.; Zhou, J. Impact of Coronary Tortuosity on Coronary Blood Supply: A Patient-Specific Study. PLoS ONE 2013, 8, e64564. [Google Scholar] [CrossRef] [Green Version]
- Hoi, Y.; Meng, H.; Woodward, S.H.; Bendok, B.R.; Hanel, R.A.; Guterman, L.R.; Hopkins, L.N. Effects of Arterial Geometry on Aneurysm Growth: Three-Dimensional Computational Fluid Dynamics Study. J. Neurosurg. 2004, 101, 676–681. [Google Scholar] [CrossRef]
- Mroczka, J.; Szczepanowski, R. Modeling of Light Transmittance Measurement in a Finite Layer of Whole Blood-a Collimated Transmittance Problem in Monte Carlo Simulation and Diffusion Model. Opt. Appl. 2005, 35, 311–331. [Google Scholar]
- Banks, J.; Bressloff, N.W. Turbulence Modeling in Three-Dimensional Stenosed Arterial Bifurcations. J. Biomech. Eng. 2007, 129, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahangiri, M.; Saghafian, M.; Sadeghi, M.R. Numerical Simulation of Hemodynamic Parameters of Turbulent and Pulsatile Blood Flow in Flexible Artery with Single and Double Stenoses. J. Mech. Sci. Technol. 2015, 29, 3549–3560. [Google Scholar] [CrossRef]
- Saqr, K.M.; Tupin, S.; Rashad, S.; Endo, T.; Niizuma, K.; Tominaga, T.; Ohta, M. Physiologic Blood Flow Is Turbulent. Sci. Rep. 2020, 10, 15492. [Google Scholar] [CrossRef]
- Tupin, S.; Saqr, K.M.; Ohta, M. Effects of Wall Compliance on Multiharmonic Pulsatile Flow in Idealized Cerebral Aneurysm Models: Comparative PIV Experiments. Exp. Fluids 2020, 61, 164. [Google Scholar] [CrossRef]
- Anzai, H.; Ohta, M.; Falcone, J.L.; Chopard, B. Optimization of Flow Diverters for Cerebral Aneurysms. J. Comput. Sci. 2012, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Putra, N.K.; Palar, P.S.; Anzai, H.; Shimoyama, K.; Ohta, M. Multiobjective Design Optimization of Stent Geometry with Wall Deformation for Triangular and Rectangular Struts. Med. Biol. Eng. Comput. 2019, 57, 15–26. [Google Scholar] [CrossRef]
- Takashima, K.; Ota, S.; Ohta, M.; Yoshinaka, K.; Ikeuchi, K. Development of Computer-Based Simulator for Catheter Navigation in Blood Vessels (1st Report, Evaluation of Fundamental Parameters of Guidewire and Blood Vessel). Trans. Jpn. Soc. Mech. Eng. Ser. C 2006, 72, 2137–2145. [Google Scholar] [CrossRef] [Green Version]
- Takashima, K.; Ota, S.; Ohta, M.; Yoshinaka, K.; Mukai, T. Development of Computer-Based Simulator for Catheter Navigation in Blood Vessels (2nd Report, Evaluation of Torquability of Guidewire). Trans. Jpn. Soc. Mech. Eng. Ser. C 2007, 73, 2988–2995. [Google Scholar] [CrossRef] [Green Version]
- Takashima, K.; Ohta, M.; Yoshinaka, K.; Mukai, T.; Oota, S. Catheter and Guidewire Simulator for Intravascular Surgery (Comparison between Simulation Results and Medical Images). IFMBE Proc. 2009, 25, 128–131. [Google Scholar] [CrossRef]
- Takashima, K.; Horie, S.; Takenaka, M.; Mukai, T.; Ishida, K.; Ueda, Y. Fundamental Study on Medical Tactile Sensor Composed of Organic Ferroelectrics. In Proceedings of the 2012 Fifth International Conference on Emerging Trends in Engineering and Technology, Himeji, Japan, 5–7 November 2012; IEEE: Piscataway, NJ, USA, 2012; pp. 132–136. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flushing Conditions | |
|---|---|
| Geometry | Flow |
| Endoscope position in the catheter | Dextran injection waveform |
| Catheter angle | Dextran flow rate |
| Catheter position in the blood vessel | Dextran injection timing |
| Use of balloon | Blood flow rate |
| Model | Mesh Number (Million) | Model | Mesh Number (Million) | Model | Mesh Number (Million) |
|---|---|---|---|---|---|
| center | 3.3 | Top | 3.8 | Bottom (1°) | 6.0 |
| Bottom (0°) | 5.6 | Bottom (2°) | 6.2 | ||
| Side | 3.8 | Bottom (3°) | 5.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitsuzuka, K.; Li, Y.; Nakayama, T.; Anzai, H.; Goanno, D.; Tupin, S.; Zhang, M.; Wang, H.; Horie, K.; Ohta, M. A Parametric Study of Flushing Conditions for Improvement of Angioscopy Visibility. J. Funct. Biomater. 2022, 13, 69. https://doi.org/10.3390/jfb13020069
Mitsuzuka K, Li Y, Nakayama T, Anzai H, Goanno D, Tupin S, Zhang M, Wang H, Horie K, Ohta M. A Parametric Study of Flushing Conditions for Improvement of Angioscopy Visibility. Journal of Functional Biomaterials. 2022; 13(2):69. https://doi.org/10.3390/jfb13020069
Chicago/Turabian StyleMitsuzuka, Kohei, Yujie Li, Toshio Nakayama, Hitomi Anzai, Daisuke Goanno, Simon Tupin, Mingzi Zhang, Haoran Wang, Kazunori Horie, and Makoto Ohta. 2022. "A Parametric Study of Flushing Conditions for Improvement of Angioscopy Visibility" Journal of Functional Biomaterials 13, no. 2: 69. https://doi.org/10.3390/jfb13020069