When a Differential Diagnosis Is Fundamental: Choriocarcinoma Mimicking Lung Carcinoma

 , , and
, , and
Abstract
:1. Introduction
2. Case Presentation
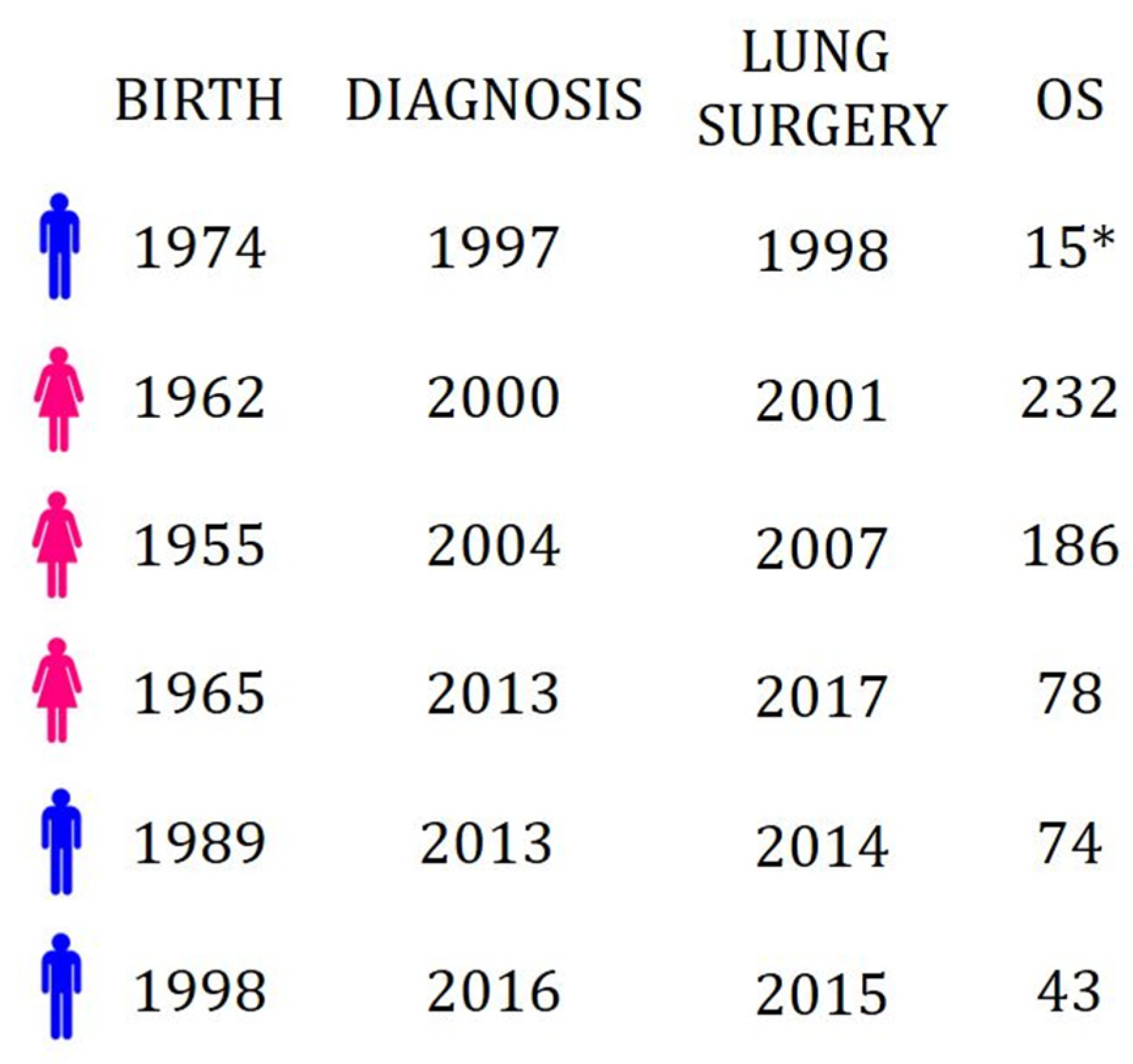
3. Retrospective Analysis
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| beta-human chorionic gonadotropin | β-hCG |
| computed tomography | CT |
| 18F-fluorodeoxyglucose | 18F-FDG |
| positron-emission tomography | PET |
| endobronchial ultrasound-guided transbronchial needle aspiration | EBUS-TBNA |
| etoposide methotrexate and dactinomycin/cyclophosphamide and vincristine | EMA-CO schemed |
References
- Takahashi, T.; Kobayashi, R. Choriocarcinoma syndrome after resection of primary pulmonary choriocarcinoma: Report of a case. Surg. Case Rep. 2016, 2, 122. [Google Scholar] [CrossRef] [PubMed]
- Stockton, L.; Green, E.; Kaur, B.; De Winton, E. Non-Gestational Choriocarcinoma with Widespread Metastases Presenting with Type 1 Respiratory Failure in a 39-Year-Old Female: Case Report and Review of the Literature. Case Rep. Oncol. 2018, 11, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Mangla, M.; Singla, D.; Kaur, H.; Sharma, S. Unusual clinical presentations of choriocarcinoma: A systematic review of case reports. Taiwan. J. Obstet. Gynecol. 2017, 56, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shih, I.-M.; Mazur, M.T.; Kurman, R.J. Gestational Trophoblastic Tumors and Related Tumor-Like Lesions. In Blaustein’s Pathology of the Female Genital Tract; Springer: Boston, MA, USA, 2011; Volume 2, pp. 1075–1135. ISBN 0791463974. [Google Scholar]
- Hui, P. Gestational trophoblastic tumors: A timely review of diagnostic pathology. Arch. Pathol. Lab. Med. 2019, 143, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Ning, F.; Hou, H.; Morse, A.N.; Lash, G.E. Understanding and management of gestational trophoblastic disease [version 1; peer review: 2 approved]. F1000Research 2019, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.L.; Devi, R.S. An unusual presentation of choriocarcinoma. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 1668. [Google Scholar] [CrossRef]
- Seidler, D.; Franklin, M. Metastatic Choriocarcinoma to the Lung: Changing Dogma. Chest 2016, 150, 765A. [Google Scholar] [CrossRef]
- Downey, R.; Zakowski, M.; Moreira, A. Rare primary malignant neoplasms of the lung. In Pearson’s Thoracic and Esophageal Surgery; Elsevier: Churchill, UK, 2008; Volume 102, pp. 841–850. ISBN 9780443068614. [Google Scholar]
- Maruoka, Y.; Abe, K.; Baba, S.; Isoda, T.; Matsuo, Y.; Kubo, Y.; Ogawa, S.; Yano, T.; Sasaki, M.; Honda, H. A case of pulmonary choriocarcinoma metastasis with unusual FDG-PET and CT findings: Correlation with pathology. Ann. Nucl. Med. 2012, 26, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Ibi, T.; Hirai, K.; Bessho, R.; Kawamoto, M.; Koizumi, K.; Shimizu, K. Choriocarcinoma of the lung: Report of a case. Gen. Thorac. Cardiovasc. Surg. 2012, 60, 377–380. [Google Scholar] [PubMed]
- Fénichel, P.; Rouzier, C.; Butori, C.; Chevallier, P.; Poullot, A.G.; Thyss, A.; Mouroux, J. Extragestational βHCG secretion due to an isolated lung epithelioid trophoblastic tumor: Microsatellite genotyping of tumoral cells confirmed their placental origin and oriented specific chemotherapy. J. Clin. Endocrinol. Metab. 2014, 99, 3515–3520. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Reid, S.; Pixton, S.; Harnett, P.; Condous, G. Choriocarcinoma of the lung masquerading as a persisting pregnancy of unknown location (PUL). Aust. N. Z. J. Obstet. Gynaecol. 2012, 52, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Gvinianidze, L.; Panagiotopoulos, N.; Woo, W.L.; Borg, E.; Lawrence, D. The challenging management of lung choriocarcinoma. J. Thorac. Dis. 2014, 6, E220–E222. [Google Scholar] [PubMed]
- Iijima, Y.; Akiyama, H.; Nakajima, Y.; Kinoshita, H.; Mikami, I.; Uramoto, H.; Hirata, T. Solitary lung metastasis from gestational choriocarcinoma resected six years after hydatidiform mole: A case report. Int. J. Surg. Case Rep. 2016, 28, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Froylich, D.; Shiloni, E.; Lavie, O.; Neumann, A.; Vlodavsky, E.; Hazzan, D. Colon and lung choriocarcinoma. Isr. Med. Assoc. J. 2010, 12, 642–644. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age | Origin | Chemotherapy | Type of Chemotherapy | OS (months) | |
|---|---|---|---|---|---|---|
| Patient 1 | M | 24 | Testicular | Post-surgery | Different lines | 15 * |
| Patient 2 | F | 52 | Uterus | Before surgery | Different lines | 209 |
| Patient 3 | F | 52 | Hydatidiform mole | Before and post-surgery | Methotrexate and Actinomycin-D (before); EMA-CO scheme (post) | 139 |
| Patient 4 | M | 17 | Mediastinal anterior masses | Before surgery | Bleomycin, Etoposide, Cisplatin (BEP scheme) | 32 |
| Patient 5 | F | 52 | Hydatidiform mole | Before and post-surgery | Methotrexate and EMA-CO scheme | 9 |
| Patient 6 | M | 25 | Mediastinal anterior masses | Before surgery | Bleomycin, Etoposide, Cisplatin (BEP scheme) | 58 |
| Ref | Age | Hypothesized Origin | Treatment | OS (months) |
|---|---|---|---|---|
| [10] | 26 | Hydatidiform mole 6 years early | Surgery | not reported |
| [11] | 27 | Gestational | Surgery | 19 |
| [12] | 29 | Gestational | Surgery + Chemotherapy 3 | 12 |
| [13] | 36 | Gestational | Chemotherapy 1 + Surgery + Chemotherapy 2 | 8 |
| [14] | 42 | Gestational | Surgery + Chemotherapy 2 | 6 |
| [15] | 45 | Hydatidiform mole 6 years early | Surgery + Chemotherapy 1 | 87 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparri, R.; Sedda, G.; Brambilla, D.; Girelli, L.; Diotti, C.; Spaggiari, L. When a Differential Diagnosis Is Fundamental: Choriocarcinoma Mimicking Lung Carcinoma. J. Clin. Med. 2019, 8, 2018. https://doi.org/10.3390/jcm8112018
Gasparri R, Sedda G, Brambilla D, Girelli L, Diotti C, Spaggiari L. When a Differential Diagnosis Is Fundamental: Choriocarcinoma Mimicking Lung Carcinoma. Journal of Clinical Medicine. 2019; 8(11):2018. https://doi.org/10.3390/jcm8112018
Chicago/Turabian StyleGasparri, Roberto, Giulia Sedda, Daniela Brambilla, Lara Girelli, Cristina Diotti, and Lorenzo Spaggiari. 2019. "When a Differential Diagnosis Is Fundamental: Choriocarcinoma Mimicking Lung Carcinoma" Journal of Clinical Medicine 8, no. 11: 2018. https://doi.org/10.3390/jcm8112018