Antithrombotic Therapy for Percutaneous Cardiovascular Interventions: From Coronary Artery Disease to Structural Heart Interventions

 ,
, 
Abstract
:1. Introduction
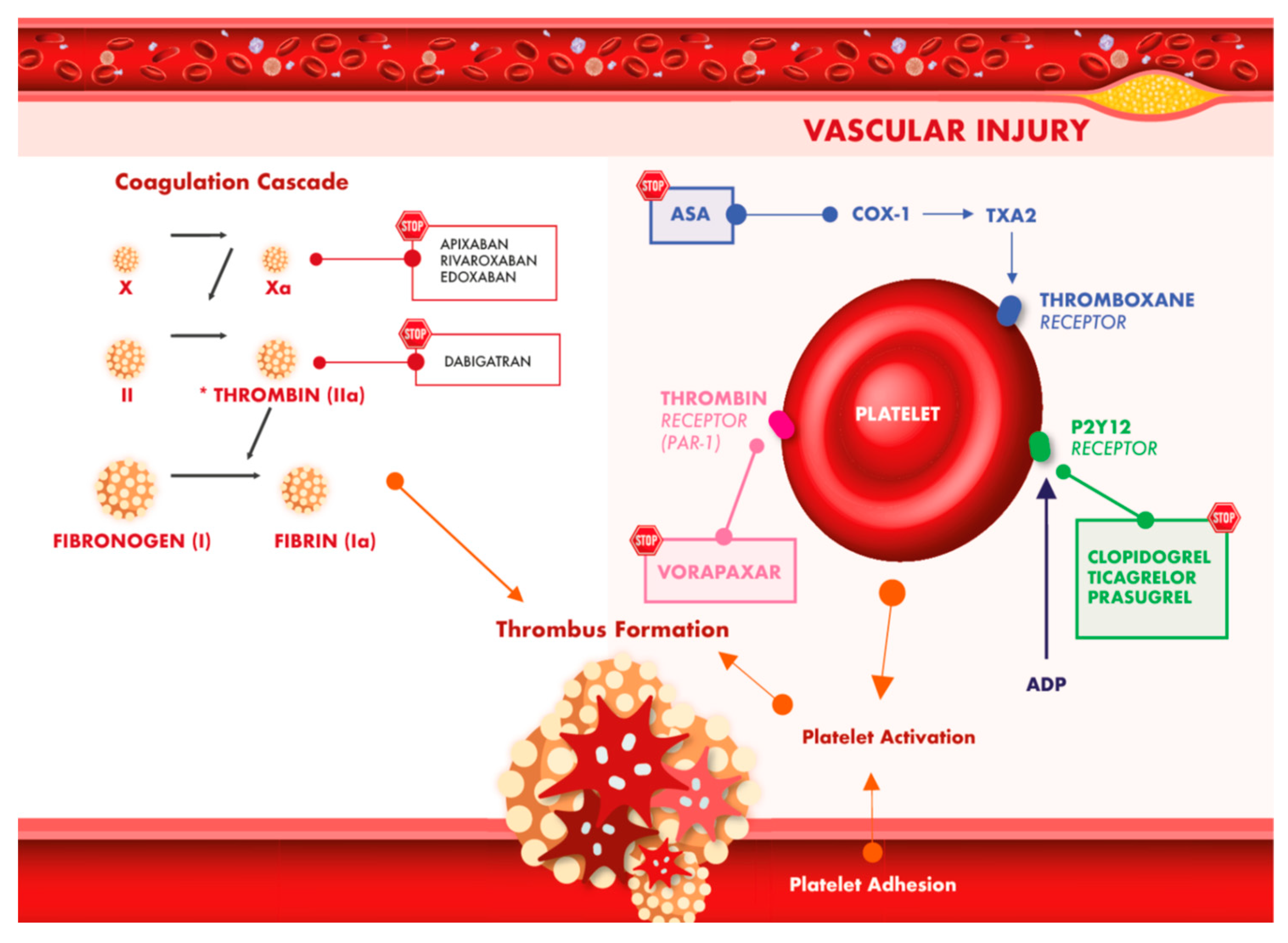
2. Type of Antithrombotic Treatment after PCI
2.1. Evidence for Clopidogrel
2.2. Evidence for Prasugrel
2.3. Evidence for Ticagrelor
2.4. Evidence for the Direct Comparison of Prasugrel and Ticagrelor
3. Duration of DAPT after PCI and Major Determinants for Treatment Selection
Randomized Trials
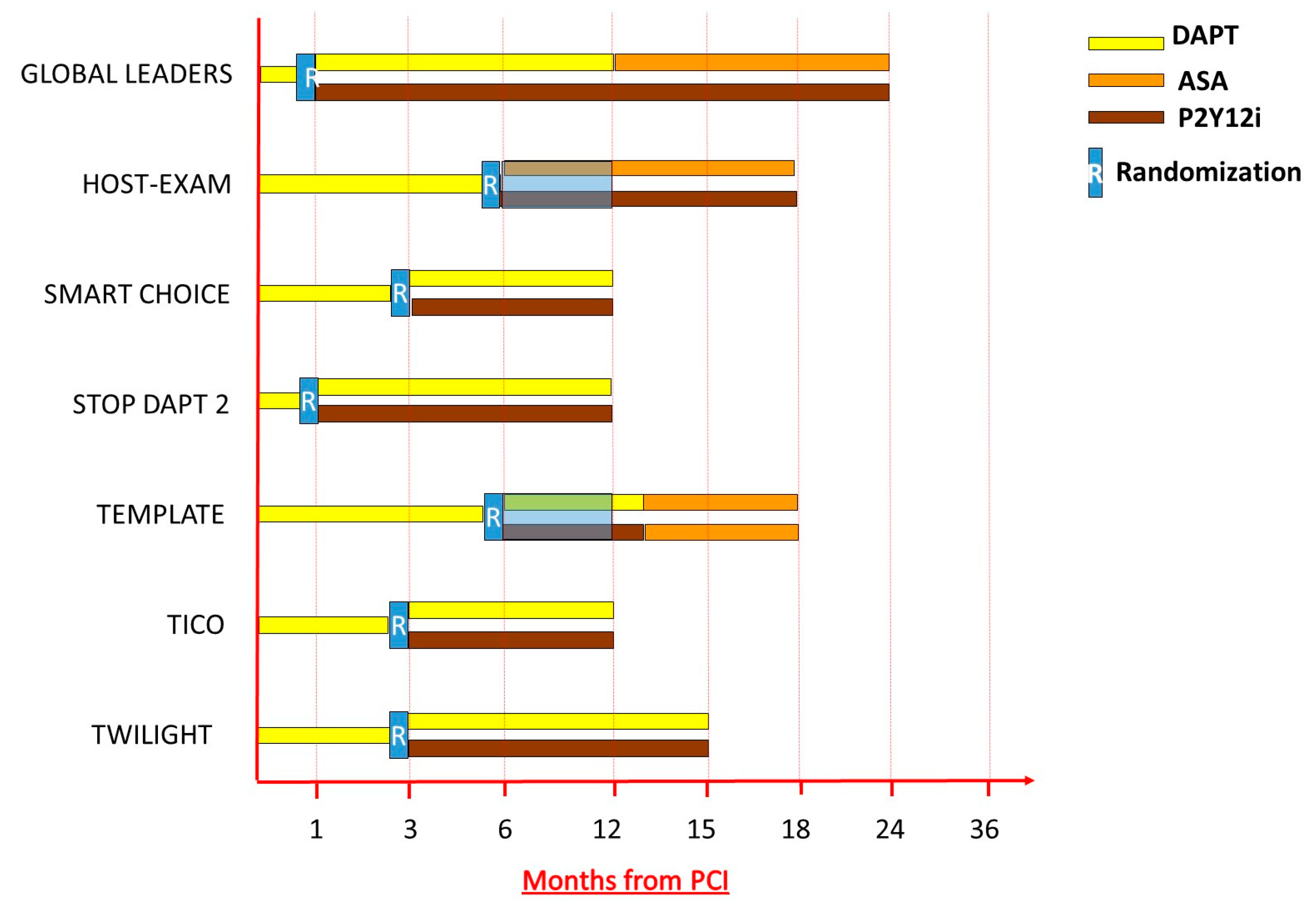
4. From DAPT to Single Antiplatelet Therapy (SAPT), Evidence for Aspirin Withdrawal and Monotherapy with P2Y12 Inhibitor
5. Combination of Oral Anticoagulants and Antiplatelet Therapy in Patients at Higher Ischemic Risk or with Non-Valvular Atrial Fibrillation
5.1. Direct-Acting Oral Anticoagulants (DOAC) in Association to Antiplatelet Therapy in Patients at High Ischemic Risk
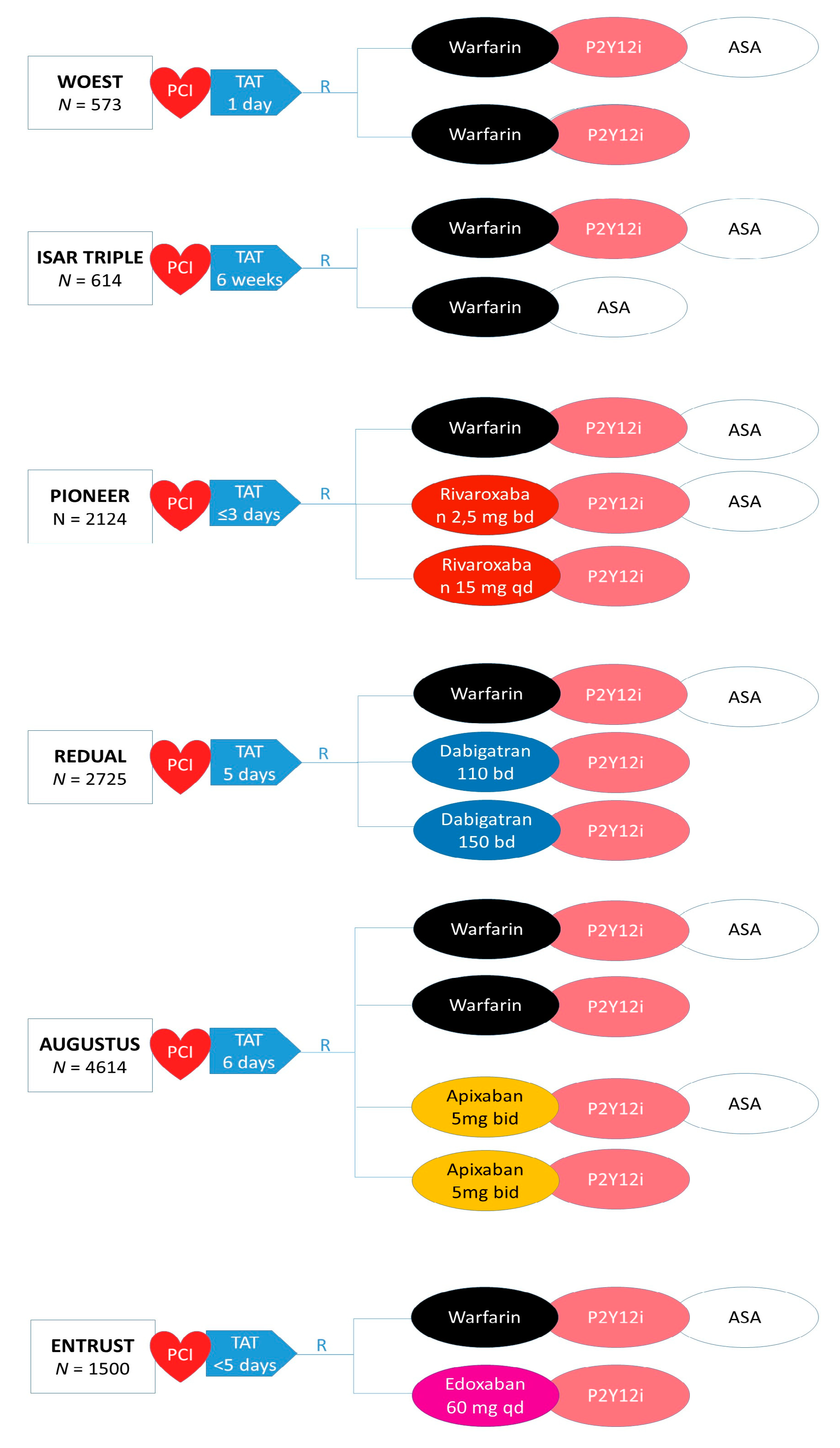
5.2. DOAC and Antiplatelet Therapy in Patients with Non-Valvular Atrial Fibrillation (AF) Undergoing PCI
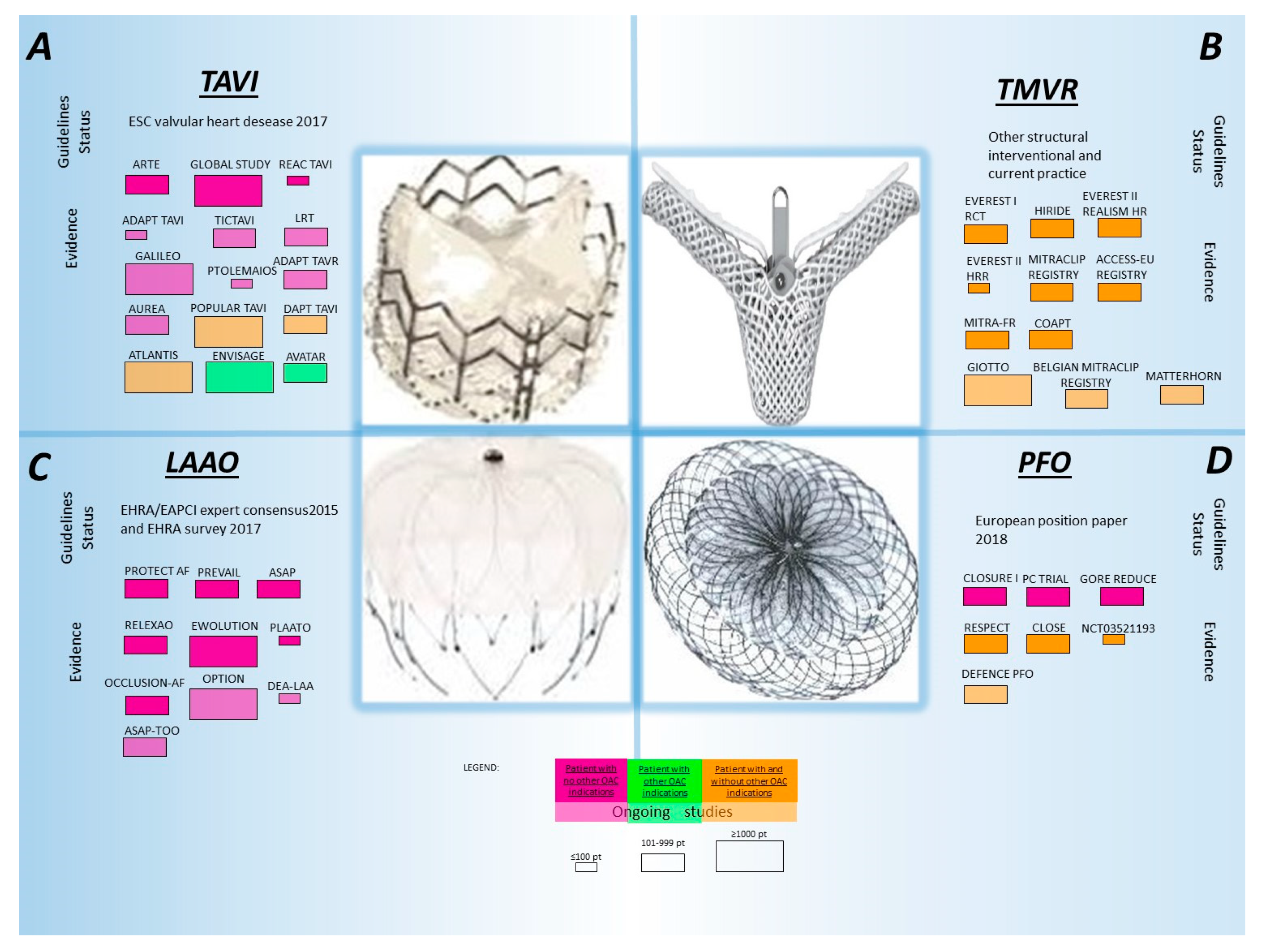
6. Current Evidence for the Type and Duration of Antithrombotic Therapy in Percutaneous Structural Heart Interventions
6.1. Transcatheter Aortic Valve Implantation (TAVI)
6.2. Evidence for MitraClip, Transcatheter Mitral Valve Interventions
6.3. Percutaneous Patent Foramen Ovale (PFO) Occlusion
6.4. Left Atrial Appendage Occlusion (LAAO)
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACS | Acute coronary syndrome |
| AF | Atrial fibrillation |
| ASA | Aspirin |
| BARC | Bleeding Academic Research Consortium |
| BMS | Bare metal stent |
| CABG | Coronary artery bypass graft surgery |
| CAD | Coronary artery disease |
| CI | Confidence interval |
| DAPT | Dual antiplatelet therapy |
| DAT | Dual antithrombotic therapy |
| DES | Drug eluting stent |
| DOAC | Direct Oral anticoagulant |
| HR | Hazard ratio |
| ISTH | International Society on Thrombosis and Haemostasis |
| LAA | Left atrial appendage |
| LAAO | Left atrial appendage occlusion |
| MACCE | Major Adverse Cardiovascular and Cerebrovascular Events |
| MI | Myocardial infraction |
| NSTEMI | Non ST-segment Elevated Myocardial Infarction |
| OAC | Oral anticoagulant |
| P2Y12i | Receptor P2Y12 inhibitor |
| PAD | Peripheral arterial disease |
| PCI | Percutaneous coronary intervention |
| PFO | Patent foramen ovale |
| PTCA | Percutaneous transluminal coronary angioplasty |
| PV | Prosthetic Valve |
| RCT | Randomized controlled trial |
| SAPT | Single antiplatelet therapy |
| TAT | Triple antithrombotic therapy |
| TAVI | Transcatheter aortic valve implantation |
| TVMR | Transcatheter mitral valve repair |
| VKA | Vitamin k antagonist |
References
- Gruntzig, A.R.; Senning, A.; Siegenthaler, W.E. Nonoperative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 1979, 301, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.A.; Gruentzig, A.R.; Hollman, J.; King, S.B., 3rd; Douglas, J.S. Coumadin and aspirin in prevention of recurrence after transluminal coronary angioplasty: A randomized study. Circulation 1984, 69, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Schömig, A.; Neumann, F.-J.; Kastrati, A.; Schühlen, H.; Blasini, R.; Hadamitzky, M.; Walter, H.; Zitzmann-Roth, E.-M.; Richardt, G.; Alt, E.; et al. A Randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N. Engl. J. Med. 1996, 334, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Baim, D.S.; Popma, J.J.; Gordon, P.C.; Cutlip, D.E.; Ho, K.K.L.; Giambartolomei, A.; Diver, D.J.; Lasorda, D.M.; Williams, D.O.; et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. N. Engl. J. Med. 1998, 339, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Costa, F.; Byrne, R.; Haude, M.; Baumbach, A.; Windecker, S. Dual antiplatelet therapy duration after coronary stenting in clinical practice: Results of an EAPCI survey. EuroIntervention 2015, 11, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Roffi, M.; Byrne, R.A.; Costa, F.; Valgimigli, M.; Task Force for the Management of Dual Antiplatelet Therapy in Coronary Artery Disease of the European Society of Cardiology (ESC); ESC Scientific Document Group. Case-based implementation of the 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease. Eur. Heart J. 2018, 39, e1–e33. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Juni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2017, 53, 34–78. [Google Scholar] [CrossRef]
- Task Force, M.; Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; et al. 2013 ESC guidelines on the management of stable coronary artery disease: The task force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar] [CrossRef]
- King, T.D.; Thompson, S.L.; Steiner, C.; Mills, N.L. Secundum atrial septal defect: Nonoperative closure during cardiac catheterization. JAMA 1976, 235, 2506–2509. [Google Scholar] [CrossRef]
- Bridges, N.D.; Hellenbrand, W.; Latson, L.; Filiano, J.; Newburger, J.W.; Lock, J.E. Transcatheter closure of patent foramen ovale after presumed paradoxical embolism. Circulation 1992, 86, 1902–1908. [Google Scholar] [CrossRef]
- Cribier, A.; Eltchaninoff, H.; Bash, A.; Borenstein, N.; Tron, C.; Bauer, F.; Derumeaux, G.; Anselme, F.; Laborde, F.o.; Leon, M.B. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis. Circulation 2002, 106, 3006–3008. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, M.E.; Rupprecht, H.-J.R.; Urban, P.; Gershlick, A.H.; CLASSICS Investigators. Double-blind study of the safety of Clopidogrel with and without a loading dose in combination with aspirin compared with Ticlopidine in combination with aspirin after coronary stenting. Circulation 2000, 102, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef]
- Serebruany, V.L.; Steinhubl, S.R.; Berger, P.B.; Malinin, A.I.; Bhatt, D.L.; Topol, E.J. Variability in platelet responsiveness to clopidogrel among 544 individuals. J. Am. Coll. Cardiol. 2005, 45, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.T.; Payne, C.D.; Wiviott, S.D.; Weerakkody, G.; Farid, N.A.; Small, D.S.; Jakubowski, J.A.; Naganuma, H.; Winters, K.J. A comparison of prasugrel and clopidogrel loading doses on platelet function: Magnitude of platelet inhibition is related to active metabolite formation. Am. Heart J. 2007, 153, 66.e9–66.e16. [Google Scholar] [CrossRef] [PubMed]
- Jernberg, T.; Payne, C.D.; Winters, K.J.; Darstein, C.; Brandt, J.T.; Jakubowski, J.A.; Naganuma, H.; Siegbahn, A.; Wallentin, L. Prasugrel achieves greater inhibition of platelet aggregation and a lower rate of non-responders compared with clopidogrel in aspirin-treated patients with stable coronary artery disease. Eur. Heart J. 2006, 27, 1166–1173. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef]
- Roe, M.T.; Armstrong, P.W.; Fox, K.A.A.; White, H.D.; Prabhakaran, D.; Goodman, S.G.; Cornel, J.H.; Bhatt, D.L.; Clemmensen, P.; Martinez, F.; et al. Prasugrel versus clopidogrel for acute coronary syndromes without revascularization. N. Engl. J. Med. 2012, 367, 1297–1309. [Google Scholar] [CrossRef]
- Husted, S.; Emanuelsson, H.; Heptinstall, S.; Sandset, P.M.; Wickens, M.; Peters, G. Pharmacodynamics, pharmacokinetics, and safety of the oral reversible P2Y12 antagonist AZD6140 with aspirin in patients with atherosclerosis: A double-blind comparison to clopidogrel with aspirin. Eur. Heart J. 2006, 27, 1038–1047. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Montalescot, G.; van’t Hof, A.W.; Lapostolle, F.; Silvain, J.; Lassen, J.F.; Bolognese, L.; Cantor, W.J.; Cequier, A.; Chettibi, M.; Goodman, S.G.; et al. Prehospital ticagrelor in ST-segment elevation myocardial infarction. N. Engl. J. Med. 2014, 371, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Rollini, F.; Franchi, F.; Cho, J.R.; DeGroat, C.; Bhatti, M.; Muniz-Lozano, A.; Singh, K.; Ferrante, E.; Wilson, R.E.; Dunn, E.C.; et al. A head-to-head pharmacodynamic comparison of prasugrel vs. ticagrelor after switching from clopidogrel in patients with coronary artery disease: Results of a prospective randomized study. Eur. Heart J. 2016, 37, 2722–2730. [Google Scholar] [CrossRef]
- Marquis-Gravel, G.; Costa, F.; Boivin-Proulx, L.A. “Ticagrelor or Prasugrel, Doctor?” The basis for decision in clinical practice. Can. J. Cardiol. 2019, 35, 1283–1285. [Google Scholar] [CrossRef] [PubMed]
- Motovska, Z.; Hlinomaz, O.; Kala, P.; Hromadka, M.; Knot, J.; Varvarovsky, I.; Dusek, J.; Jarkovsky, J.; Miklik, R.; Rokyta, R.; et al. 1-Year outcomes of patients undergoing primary angioplasty for myocardial infarction treated with Prasugrel versus Ticagrelor. J. Am. Coll. Cardiol. 2018, 71, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Rafique, A.M.; Nayyar, P.; Wang, T.Y.; Mehran, R.; Baber, U.; Berger, P.B.; Tobis, J.; Currier, J.; Dave, R.H.; Henry, T.D. Optimal P2Y12 inhibitor in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: A network meta-analysis. JACC Cardiovasc. Interv. 2016, 9, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Schüpke, S.; Neumann, F.-J.; Menichelli, M.; Mayer, K.; Bernlochner, I.; Wöhrle, J.; Richardt, G.; Liebetrau, C.; Witzenbichler, B.; Antoniucci, D.; et al. Ticagrelor or Prasugrel in patients with acute coronary syndromes. N. Engl. J. Med. 2019, 381, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Windecker, S.; Valgimigli, M. Dual antiplatelet therapy duration: Reconciling the inconsistencies. Drugs 2017, 77, 1733–1754. [Google Scholar] [CrossRef] [PubMed]
- Gwon, H.-C.; Hahn, J.-Y.; Park, K.W.; Song, Y.B.; Chae, I.-H.; Lim, D.-S.; Han, K.-R.; Choi, J.-H.; Choi, S.-H.; Kang, H.-J.; et al. Six-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents. Circulation 2012, 125, 505–513. [Google Scholar] [CrossRef]
- Colombo, A.; Chieffo, A.; Frasheri, A.; Garbo, R.; Masotti-Centol, M.; Salvatella, N.; Oteo Dominguez, J.F.; Steffanon, L.; Tarantini, G.; Presbitero, P.; et al. Second-generation drug-eluting stent implantation followed by 6- versus 12-month dual antiplatelet therapy: The SECURITY randomized clinical trial. J. Am. Coll. Cardiol. 2014, 64, 2086–2097. [Google Scholar] [CrossRef]
- Schulz-Schüpke, S.; Byrne, R.A.; Ten Berg, J.M.; Neumann, F.J.; Han, Y.; Adriaenssens, T.; Tölg, R.; Seyfarth, M.; Maeng, M.; Zrenner, B.; et al. ISAR-SAFE: A randomized, double-blind, placebo-controlled trial of 6 vs. 12 months of clopidogrel therapy after drug-eluting stenting. Eur. Heart J. 2015, 36, 1252–1263. [Google Scholar] [CrossRef]
- Hong, S.J.; Shin, D.H.; Kim, J.S.; Kim, B.K.; Ko, Y.G.; Choi, D.; Her, A.Y.; Kim, Y.H.; Jang, Y.; Hong, M.K.; et al. 6-month versus 12-month dual-antiplatelet therapy following long everolimus-eluting stent implantation: The IVUS-XPL randomized clinical trial. JACC Cardiovasc. Interv. 2016, 9, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.-Y.; Song, Y.B.; Oh, J.-H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.-S.; Jeong, J.-O.; Cho, B.R.; Oh, S.K.; et al. Effect of P2Y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention: The SMART-CHOICE randomized clinical trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kedhi, E.; Fabris, E.; van der Ent, M.; Buszman, P.; von Birgelen, C.; Roolvink, V.; Zurakowski, A.; Schotborgh, C.E.; Hoorntje, J.C.A.; Eek, C.H.; et al. Six months versus 12 months dual antiplatelet therapy after drug-eluting stent implantation in ST-elevation myocardial infarction (DAPT-STEMI): Randomised, multicentre, non-inferiority trial. BMJ 2018, 363, k3793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilard, M.; Barragan, P.; Noryani, A.A.L.; Noor, H.A.; Majwal, T.; Hovasse, T.; Castellant, P.; Schneeberger, M.; Maillard, L.; Bressolette, E.; et al. 6- versus 24-month dual antiplatelet therapy after implantation of drug-eluting stents in patients nonresistant to Aspirin: The randomized, multicenter ITALIC trial. J. Am. Coll. Cardiol. 2015, 65, 777–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, M.; Iijima, R.; Ako, J.; Shinke, T.; Okada, H.; Ito, Y.; Ando, K.; Anzai, H.; Tanaka, H.; Ueda, Y.; et al. Dual antiplatelet therapy for 6 versus 18 months after biodegradable polymer drug-eluting stent implantation. JACC Cardiovasc. Interv. 2017, 10, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Udell, J.A.; Bonaca, M.P.; Collet, J.P.; Lincoff, A.M.; Kereiakes, D.J.; Costa, F.; Lee, C.W.; Mauri, L.; Valgimigli, M.; Park, S.J.; et al. Long-term dual antiplatelet therapy for secondary prevention of cardiovascular events in the subgroup of patients with previous myocardial infarction: A collaborative meta-analysis of randomized trials. Eur. Heart J. 2016, 37, 390–399. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Costa, F.; Lokhnygina, Y.; Clare, R.M.; Wallentin, L.; Moliterno, D.J.; Armstrong, P.W.; White, H.D.; Held, C.; Aylward, P.E.; et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: Lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur. Heart J. 2017, 38, 804–810. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; Valgimigli, M. The optimal duration of dual antiplatelet therapy after coronary stent implantation: To go too far is as bad as to fall short. Cardiovasc. Diagn. Ther. 2018, 8, 630–646. [Google Scholar] [CrossRef]
- Albaladejo, P.; Charbonneau, H.; Samama, C.M.; Collet, J.P.; Marret, E.; Piriou, V.; Genty, C.; Bosson, J.L. Bleeding complications in patients with coronary stents during non-cardiac surgery. Thromb. Res. 2014, 134, 268–272. [Google Scholar] [CrossRef]
- Valgimigli, M.; Campo, G.; Monti, M.; Vranckx, P.; Percoco, G.; Tumscitz, C.; Castriota, F.; Colombo, F.; Tebaldi, M.; Fucà, G.; et al. Short- versus long-term duration of dual-antiplatelet therapy after coronary stenting. Circulation 2012, 125, 2015–2026. [Google Scholar] [CrossRef] [Green Version]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, F.; Adamo, M.; Ariotti, S.; Navarese, E.P.; Biondi-Zoccai, G.; Valgimigli, M. Impact of greater than 12-month dual antiplatelet therapy duration on mortality: Drug-specific or a class-effect? A meta-analysis. Int. J. Cardiol. 2015, 201, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bhatt, D.L.; Cohen, M.; Steg, P.G.; Storey, R.F.; Jensen, E.C.; Magnani, G.; Bansilal, S.; Fish, M.P.; Im, K.; et al. Long-term use of Ticagrelor in patients with prior myocardial infarction. N. Engl. J. Med. 2015, 372, 1791–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, D.L.; Steg, P.G.; Mehta, S.R.; Leiter, L.A.; Simon, T.; Fox, K.; Held, C.; Andersson, M.; Himmelmann, A.; Ridderstråle, W.; et al. Ticagrelor in patients with diabetes and stable coronary artery disease with a history of previous percutaneous coronary intervention (THEMIS-PCI): A phase 3, placebo-controlled, randomised trial. Lancet 2019, 394, 1169–1180. [Google Scholar] [CrossRef]
- Navarese, E.P.; Andreotti, F.; Schulze, V.; Kolodziejczak, M.; Buffon, A.; Brouwer, M.; Costa, F.; Kowalewski, M.; Parati, G.; Lip, G.Y.; et al. Optimal duration of dual antiplatelet therapy after percutaneous coronary intervention with drug eluting stents: Meta-analysis of randomised controlled trials. BMJ 2015, 350, h1618. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Ariotti, S.; Costa, F. Duration of dual antiplatelet therapy after drug-eluting stent implantation: Will we ever reach a consensus? Eur. Heart J. 2015, 36, 1219–1222. [Google Scholar] [CrossRef] [Green Version]
- Adamo, M.; Costa, F.; Vranckx, P.; Leonardi, S.; Navarese, E.P.; Garcia-Garcia, H.M.; Valgimigli, M. Does smoking habit affect the randomized comparison of 6 versus 24-month dual antiplatelet therapy duration? Insights from the PRODIGY trial. Int. J. Cardiol. 2015, 190, 242–245. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Juni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur. J. Cardiothorac. Surg. 2018, 53, 34–78. [Google Scholar] [CrossRef] [Green Version]
- Gargiulo, G.; Ariotti, S.; Santucci, A.; Piccolo, R.; Baldo, A.; Franzone, A.; Magnani, G.; Marino, M.; Esposito, G.; Windecker, S.; et al. Impact of sex on 2-year clinical outcomes in patients treated with 6-month or 24-month dual-antiplatelet therapy duration: A pre-specified analysis from the PRODIGY trial. JACC Cardiovasc. Interv. 2016, 9, 1780–1789. [Google Scholar] [CrossRef]
- Gargiulo, G.; Costa, F.; Ariotti, S.; Biscaglia, S.; Campo, G.; Esposito, G.; Leonardi, S.; Vranckx, P.; Windecker, S.; Valgimigli, M. Impact of proton pump inhibitors on clinical outcomes in patients treated with a 6- or 24-month dual-antiplatelet therapy duration: Insights from the PROlonging Dual-antiplatelet treatment after Grading stent-induced Intimal hyperplasia studY trial. Am. Heart J. 2016, 174, 95–102. [Google Scholar] [CrossRef]
- McAllister, K.S.L.; Ludman, P.F.; Hulme, W.; de Belder, M.A.; Stables, R.; Chowdhary, S.; Mamas, M.A.; Sperrin, M.; Buchan, I.E. A contemporary risk model for predicting 30-day mortality following percutaneous coronary intervention in England and Wales. Int. J. Cardiol. 2016, 210, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, F.; Vranckx, P.; Leonardi, S.; Moscarella, E.; Ando, G.; Calabro, P.; Oreto, G.; Zijlstra, F.; Valgimigli, M. Impact of clinical presentation on ischaemic and bleeding outcomes in patients receiving 6- or 24-month duration of dual-antiplatelet therapy after stent implantation: A pre-specified analysis from the PRODIGY (Prolonging Dual-Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia) trial. Eur. Heart J. 2015, 36, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Crimi, G.; Leonardi, S.; Costa, F.; Ariotti, S.; Tebaldi, M.; Biscaglia, S.; Valgimigli, M. Incidence, prognostic impact, and optimal definition of contrast-induced acute kidney injury in consecutive patients with stable or unstable coronary artery disease undergoing percutaneous coronary intervention. insights from the all-comer PRODIGY trial. Catheter. Cardiovasc. Interv. 2015, 86, E19–E27. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Valgimigli, M. Impact of clinical presentation on dual antiplatelet therapy duration: Let’s re-evaluate our priorities. J. Am. Coll. Cardiol. 2015, 66, 1203–1204. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; Adamo, M.; Ariotti, S.; Ferrante, G.; Navarese, E.P.; Leonardi, S.; Garcia-Garcia, H.; Vranckx, P.; Valgimigli, M. Left main or proximal left anterior descending coronary artery disease location identifies high-risk patients deriving potentially greater benefit from prolonged dual antiplatelet therapy duration. EuroIntervention 2016, 11, e1222–e1230. [Google Scholar] [CrossRef]
- Giustino, G.; Chieffo, A.; Palmerini, T.; Valgimigli, M.; Feres, F.; Abizaid, A.; Costa, R.A.; Hong, M.-K.; Kim, B.-K.; Jang, Y.; et al. Efficacy and safety of dual antiplatelet therapy after complex PCI. J. Am. Coll. Cardiol. 2016, 68, 1851–1864. [Google Scholar] [CrossRef]
- Costa, F.; Tijssen, J.G.; Ariotti, S.; Giatti, S.; Moscarella, E.; Guastaroba, P.; De Palma, R.; Ando, G.; Oreto, G.; Zijlstra, F.; et al. Incremental value of the CRUSADE, ACUITY, and HAS-BLED risk scores for the prediction of hemorrhagic events after coronary stent implantation in patients undergoing long or short duration of dual antiplatelet therapy. J. Am. Heart Assoc. 2015, 4, e002524. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; van Klaveren, D.; James, S.; Heg, D.; Räber, L.; Feres, F.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: A pooled analysis of individual-patient datasets from clinical trials. Lancet 2017, 389, 1025–1034. [Google Scholar] [CrossRef]
- Yeh, R.W.; Secemsky, E.A.; Kereiakes, D.J.; Normand, S.L.; Gershlick, A.H.; Cohen, D.J.; Spertus, J.A.; Steg, P.G.; Cutlip, D.E.; Rinaldi, M.J.; et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA 2016, 315, 1735–1749. [Google Scholar] [CrossRef] [Green Version]
- Ando, G.; Costa, F. Bleeding risk stratification in acute coronary syndromes. Is it still valid in the era of the radial approach? Postepy Kardiol. Interwencyjnej 2015, 11, 170–173. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; Van Klaveren, D.; Feres, F.; James, S.; Räber, L.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; Steg, P.G.; et al. Dual antiplatelet therapy duration based on ischemic and bleeding risks after coronary stenting. J. Am. Coll. Cardiol. 2019, 73, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Costa, F. Characterization of the individual patient risk after percutaneous coronary intervention: At the crossroads of bleeding and thrombosis. JACC Cardiovasc. Interv. 2019, 12, 831–834. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Brugaletta, S.; Pernigotti, A.; Flores-Ulmanzor, E.; Ortega-Paz, L.; Cequier, A.; Iniguez, A.; Serra, A.; Jimenez-Quevedo, P.; Mainar, V.; et al. Does large vessel size justify use of bare-metal stents in primary percutaneous coronary intervention? Circ. Cardiovasc. Interv. 2019, 12, e007705. [Google Scholar] [CrossRef] [PubMed]
- Ariotti, S.; Adamo, M.; Costa, F.; Patialiakas, A.; Briguori, C.; Thury, A.; Colangelo, S.; Campo, G.; Tebaldi, M.; Ungi, I.; et al. Is bare-metal stent implantation still justifiable in high bleeding risk patients undergoing percutaneous coronary intervention?: A pre-specified analysis from the ZEUS trial. JACC Cardiovasc. Interv. 2016, 9, 426–436. [Google Scholar] [CrossRef]
- Ariotti, S.; Costa, F.; Valgimigli, M. Coronary stent selection and optimal course of dual antiplatelet therapy in patients at high bleeding or thrombotic risk: Navigating between limited evidence and clinical concerns. Curr. Opin. Cardiol. 2015, 30, 325–332. [Google Scholar] [CrossRef]
- Crimi, G.; Leonardi, S.; Costa, F.; Adamo, M.; Ariotti, S.; Valgimigli, M. Role of stent type and of duration of dual antiplatelet therapy in patients with chronic kidney disease undergoing percutaneous coronary interventions. Is bare metal stent implantation still a justifiable choice? A post-hoc analysis of the all comer PRODIGY trial. Int. J. Cardiol. 2016, 212, 110–117. [Google Scholar] [CrossRef]
- Varenne, O.; Cook, S.; Sideris, G.; Kedev, S.; Cuisset, T.; Carrié, D.; Hovasse, T.; Garot, P.; Mahmoud, R.E.; Spaulding, C.; et al. Drug-eluting stents in elderly patients with coronary artery disease (SENIOR): A randomised single-blind trial. Lancet 2018, 391, 41–50. [Google Scholar] [CrossRef]
- Watanabe, H.; Domei, T.; Morimoto, T.; Natsuaki, M.; Shiomi, H.; Toyota, T.; Ohya, M.; Suwa, S.; Takagi, K.; Nanasato, M.; et al. Effect of 1-month dual antiplatelet therapy followed by Clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI: The STOPDAPT-2 randomized clinical trial. JAMA 2019, 321, 2414–2427. [Google Scholar] [CrossRef] [Green Version]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef]
- Valgimigli, M.; Garcia-Garcia, H.M.; Vrijens, B.; Vranckx, P.; McFadden, E.P.; Costa, F.; Pieper, K.; Vock, D.M.; Zhang, M.; Van Es, G.A.; et al. Standardized classification and framework for reporting, interpreting, and analysing medication non-adherence in cardiovascular clinical trials: A consensus report from the Non-adherence Academic Research Consortium (NARC). Eur. Heart J. 2019, 40, 2070–2085. [Google Scholar] [CrossRef]
- Costa, F.; Brugaletta, S. Antithrombotic therapy in acute coronary syndrome: Striking a happy medium. Rev. Esp. Cardiol. (Engl. Ed.) 2018, 71, 782–786. [Google Scholar] [CrossRef]
- Mega, J.L.; Braunwald, E.; Wiviott, S.D.; Bassand, J.P.; Bhatt, D.L.; Bode, C.; Burton, P.; Cohen, M.; Cook-Bruns, N.; Fox, K.A.; et al. Rivaroxaban in patients with a recent acute coronary syndrome. N. Engl. J. Med. 2012, 366, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.H.; Lopes, R.D.; James, S.; Kilaru, R.; He, Y.; Mohan, P.; Bhatt, D.L.; Goodman, S.; Verheugt, F.W.; Flather, M.; et al. Apixaban with antiplatelet therapy after acute coronary syndrome. N. Engl. J. Med. 2011, 365, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in stable cardiovascular disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Group, T.A.W. Clopidogrel plus aspirin versus oral anticoagulation for atrial fi brillation in the Atrial fi brillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): A randomised controlled trial. Lancet 2006, 367, 1903–1942. [Google Scholar]
- Sorensen, R.; Hansen, M.L.; Abildstrom, S.Z.; Hvelplund, A.; Andersson, C.; Jorgensen, C.; Madsen, J.K.; Hansen, P.R.; Kober, L.; Torp-Pedersen, C.; et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: A retrospective analysis of nationwide registry data. Lancet 2009, 374, 1967–1974. [Google Scholar] [CrossRef]
- Dewilde, W.J.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; van Eickels, M.; et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [Green Version]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual antithrombotic therapy with Dabigatran after PCI in atrial fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N. Engl. J. Med. 2019, 10.1056/NEJMoa1817083. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Berg, J.M.T.; et al. Safety and efficacy of antithrombotic strategies in patients with atrial fibrillation undergoing percutaneous coronary intervention: A network meta-analysis of randomized controlled trials. JAMA Cardiol. 2019, 4, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Goodman, S.G.; Bhatt, D.L.; Eikelboom, J.W.; Price, M.J.; Moliterno, D.J.; Cannon, C.P.; Tanguay, J.-F.; Granger, C.B.; Mauri, L.; et al. Antithrombotic therapy in patients with atrial fibrillation treated with oral anticoagulation undergoing percutaneous coronary intervention. Circulation 2018, 138, 527–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; John, P.; Erwin, I.; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2017, 70, 252–289. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Amat-Santos, I.J.; Rodés-Cabau, J.; Urena, M.; DeLarochellière, R.; Doyle, D.; Bagur, R.; Villeneuve, J.; Côté, M.; Nombela-Franco, L.; Philippon, F.; et al. Incidence, predictive factors, and prognostic value of new-onset atrial fibrillation following transcatheter aortic valve implantation. J. Am. Coll. Cardiol. 2012, 59, 178–188. [Google Scholar] [CrossRef] [Green Version]
- Rodés-Cabau, J.; Masson, J.-B.; Welsh, R.C.; Garcia del Blanco, B.; Pelletier, M.; Webb, J.G.; Al-Qoofi, F.; Généreux, P.; Maluenda, G.; Thoenes, M.; et al. Aspirin versus Aspirin plus Clopidogrel as antithrombotic treatment following transcatheter aortic valve replacement with a balloon-expandable valve: The ARTE (Aspirin versus Aspirin + Clopidogrel following transcatheter aortic valve implantation) randomized clinical trial. JACC Cardiovasc. Interv. 2017, 10, 1357–1365. [Google Scholar] [CrossRef]
- Sherwood, M.W.; Vemulapalli, S.; Harrison, J.K.; Dai, D.; Vora, A.N.; Mack, M.J.; Holmes, D.R.; Rumsfeld, J.S.; Cohen, D.J.; Thourani, V.H.; et al. Variation in post-TAVR antiplatelet therapy utilization and associated outcomes: Insights from the STS/ACC TVT registry. Am. Heart J. 2018, 204, 9–16. [Google Scholar] [CrossRef]
- Kalra, R.; Patel, N.; Doshi, R.; Arora, G.; Arora, P. Evaluation of the incidence of new-onset atrial fibrillation after aortic valve replacement. JAMA Intern. Med. 2019, 179, 1122–1130. [Google Scholar] [CrossRef]
- Windecker, S.; Tijssen, J.; Giustino, G.; Guimarães, A.H.C.; Mehran, R.; Valgimigli, M.; Vranckx, P.; Welsh, R.C.; Baber, U.; van Es, G.-A.; et al. Trial design: Rivaroxaban for the prevention of major cardiovascular events after transcatheter aortic valve replacement: Rationale and design of the GALILEO study. Am. Heart J. 2017, 184, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latib, A.; Naganuma, T.; Abdel-Wahab, M.; Danenberg, H.; Cota, L.; Barbanti, M.; Baumgartner, H.; Finkelstein, A.; Legrand, V.; de Lezo, J.S.; et al. Treatment and clinical outcomes of transcatheter heart valve thrombosis. Circ. Cardiovasc. Interv. 2015, 8, e001779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dangas, G.D.; Weitz, J.I.; Giustino, G.; Makkar, R.; Mehran, R. Prosthetic heart valve thrombosis. J. Am. Coll. Cardiol. 2016, 68, 2670–2689. [Google Scholar] [CrossRef] [PubMed]
- Puri, R.; Auffret, V.; Rodés-Cabau, J. Bioprosthetic valve thrombosis. J. Am. Coll. Cardiol. 2017, 69, 2193–2211. [Google Scholar] [CrossRef]
- Makkar, R.R.; Fontana, G.; Jilaihawi, H.; Chakravarty, T.; Kofoed, K.F.; De Backer, O.; Asch, F.M.; Ruiz, C.E.; Olsen, N.T.; Trento, A.; et al. Possible subclinical leaflet thrombosis in bioprosthetic aortic valves. N. Engl. J. Med. 2015, 373, 2015–2024. [Google Scholar] [CrossRef]
- Holy, E.W.; Kebernik, J.; Allali, A.; El-Mawardy, M.; Richardt, G.; Abdel-Wahab, M. Comparison of dual antiplatelet therapy versus oral anticoagulation following transcatheter aortic valve replacement: A retrospective single-center registry analysis. Cardiol. J. 2017, 24, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Jose, J.; Sulimov, D.S.; El-Mawardy, M.; Sato, T.; Allali, A.; Holy, E.W.; Becker, B.; Landt, M.; Kebernik, J.; Schwarz, B.; et al. Clinical bioprosthetic heart valve thrombosis after transcatheter aortic valve replacement: Incidence, characteristics, and treatment outcomes. JACC Cardiovasc. Interv. 2017, 10, 686–697. [Google Scholar] [CrossRef]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef]
- Maisano, F.; La Canna, G.; Colombo, A.; Alfieri, O. The evolution from surgery to percutaneous mitral valve interventions: The role of the edge-to-edge technique. J. Am. Coll. Cardiol. 2011, 58, 2174–2182. [Google Scholar] [CrossRef] [Green Version]
- Glower, D.D.; Kar, S.; Trento, A.; Lim, D.S.; Bajwa, T.; Quesada, R.; Whitlow, P.L.; Rinaldi, M.J.; Grayburn, P.; Mack, M.J.; et al. Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: Results of the EVEREST II study. J. Am. Coll. Cardiol. 2014, 64, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.S.; Reynolds, M.R.; Feldman, T.; Kar, S.; Herrmann, H.C.; Wang, A.; Whitlow, P.L.; Gray, W.A.; Grayburn, P.; Mack, M.J.; et al. Improved functional status and quality of life in prohibitive surgical risk patients with degenerative mitral regurgitation after transcatheter mitral valve repair. J. Am. Coll. Cardiol. 2014, 64, 182–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, R.W.; Mottram, P.M.; McGaw, D.J. Closure of secundum atrial septal defects with the amplatzer septal occluder device: Techniques and problems. Catheter. Cardiovasc. Interv. 2002, 57, 508–524. [Google Scholar] [CrossRef]
- Windecker, S.; Wahl, A.; Chatterjee, T.; Garachemani, A.; Eberli, F.R.; Seiler, C.; Meier, B. Percutaneous closure of patent foramen ovale in patients with paradoxical embolism. Circulation 2000, 101, 893–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clergeau, M.-R.; Hamon, M.L.; Morello, R.M.; Saloux, E.; Viader, F.; Hamon, M. Silent cerebral infarcts in patients with pulmonary embolism and a patent foramen ovale. Stroke 2009, 40, 3758–3762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pell, A.C.H.; Hughes, D.; Keating, J.; Christie, J.; Busuttil, A.; Sutherland, G.R. Fulminating fat embolism syndrome caused by paradoxical embolism through a patent foramen ovale. N. Engl. J. Med. 1993, 329, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Braun, M.; Gliech, V.; Boscheri, A.; Schoen, S.; Gahn, G.; Reichmann, H.; Haass, M.; Schraeder, R.; Strasser, R.H. Transcatheter closure of patent foramen ovale (PFO) in patients with paradoxical embolism. Periprocedural safety and mid-term follow-up results of three different device occluder systems. Eur. Heart J. 2004, 25, 424–430. [Google Scholar] [CrossRef]
- Brandt, R.R.; Neumann, T.; Neuzner, J.; Rau, M.; Faude, I.; Hamm, C.W. Transcatheter closure of atrial septal defect and patent foramen ovale in adult patients using the Amplatzer occlusion device: No evidence for thrombus deposition with antiplatelet agents. J. Am. Soc. Echocardiogr. 2002, 15, 1094–1098. [Google Scholar] [CrossRef]
- Rickers, C.; Hamm, C.; Stern, H.; Hofmann, T.; Franzen, O.; Schräder, R.; Sievert, H.; Schranz, D.; Michel-Behnke, I.; Vogt, J.; et al. Percutaneous closure of secundum atrial septal defect with a new self centring device (“angel wings”). Heart 1998, 80, 517–521. [Google Scholar] [CrossRef]
- Krumsdorf, U.; Ostermayer, S.; Billinger, K.; Trepels, T.; Zadan, E.; Horvath, K.; Sievert, H. Incidence and clinical course of thrombus formation on atrial septal defect and patient foramen ovale closure devices in 1,000 consecutive patients. J. Am. Coll. Cardiol. 2004, 43, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.A.; Latson, L.A.; Cheatham, J.P.; McManus, B.; Anderson, J.M.; Kilzer, K.L.; Furst, J. Biological response to Bard Clamshell Septal Occluders in the canine heart. Circulation 1996, 93, 1459–1463. [Google Scholar] [CrossRef]
- Davies, A.; Ekmejian, A.; Collins, N.; Bhagwandeen, R. Multidisciplinary assessment in optimising results of percutaneous patent foramen ovale closure. Heart Lung Circ. 2017, 26, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Pristipino, C.; Sievert, H.; D’Ascenzo, F.; Louis Mas, J.; Meier, B.; Scacciatella, P.; Hildick-Smith, D.; Gaita, F.; Toni, D.; Kyrle, P.; et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur. Heart J. 2019, 40, 3182–3195. [Google Scholar] [CrossRef]
- Messé, S.R.; Gronseth, G.; Kent, D.M.; Kizer, J.R.; Homma, S.; Rosterman, L.; Kasner, S.E. Practice advisory: Recurrent stroke with patent foramen ovale (update of practice parameter): Report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology 2016, 87, 815–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Søndergaard, L.; Kasner, S.E.; Rhodes, J.F.; Andersen, G.; Iversen, H.K.; Nielsen-Kudsk, J.E.; Settergren, M.; Sjöstrand, C.; Roine, R.O.; Hildick-Smith, D.; et al. Patent foramen ovale closure or antiplatelet therapy for cryptogenic stroke. N. Engl. J. Med. 2017, 377, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Mas, J.-L.; Derumeaux, G.; Guillon, B.; Massardier, E.; Hosseini, H.; Mechtouff, L.; Arquizan, C.; Béjot, Y.; Vuillier, F.; Detante, O.; et al. Patent foramen ovale closure or anticoagulation vs. antiplatelets after stroke. N. Engl. J. Med. 2017, 377, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Wintzer-Wehekind, J.; Alperi, A.; Houde, C.; Côté, J.-M.; de Freitas Campos Guimaraes, L.; Côté, M.; Rodés-Cabau, J. Impact of discontinuation of antithrombotic therapy following closure of patent foramen ovale in patients with cryptogenic embolism. Am. J. Cardiol. 2019, 123, 1538–1545. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.M.; Mehran, R.; Povsic, T.J.; Zelenkofske, S.L.; Huang, Z.; Armstrong, P.W.; Steg, P.G.; Bode, C.; Cohen, M.G.; Buller, C.; et al. Effect of the REG1 anticoagulation system versus bivalirudin on outcomes after percutaneous coronary intervention (REGULATE-PCI): A randomised clinical trial. Lancet 2016, 387, 349–356. [Google Scholar] [CrossRef]
- Blackshear, J.L.; Odell, J.A. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann. Thorac. Surg. 1996, 61, 755–759. [Google Scholar] [CrossRef]
- Stoddard, M.F.; Dawkins, P.R.; Prince, C.R.; Ammash, N.M. Left atrial appendage thrombus is not uncommon in patients with acute atrial fibrillation and a recent embolic event: A transesophageal echocardiographics tudy. J. Am. Coll. Cardiol. 1995, 25, 452–459. [Google Scholar] [CrossRef] [Green Version]
- Madden, J.L. Resection of the left auricular appendix: A prophylaxis for recurrent arterial emboli. JAMA 1949, 140, 769–772. [Google Scholar] [CrossRef]
- Ostermayer, S.H.; Reisman, M.; Kramer, P.H.; Matthews, R.V.; Gray, W.A.; Block, P.C.; Omran, H.; Bartorelli, A.L.; Della Bella, P.; Di Mario, C.; et al. Percutaneous Left Atrial Appendage Transcatheter Occlusion (PLAATO System) to prevent stroke in high-risk patients with non-rheumatic atrial fibrillation: Results from the international multi-center feasibility trials. J. Am. Coll. Cardiol. 2005, 46, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Reddy, V.Y.; Möbius-Winkler, S.; Miller, M.A.; Neuzil, P.; Schuler, G.; Wiebe, J.; Sick, P.; Sievert, H. Left atrial appendage closure with the watchman device in patients with a contraindication for oral anticoagulation: The ASAP study (ASA plavix feasibility study with watchman left atrial appendage closure technology). J. Am. Coll. Cardiol. 2013, 61, 2551–2556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, D.R.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 177–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauchier, L.; Cinaud, A.; Brigadeau, F.; Lepillier, A.; Pierre, B.; Abbey, S.; Fatemi, M.; Franceschi, F.; Guedeney, P.; Jacon, P.; et al. Device-related thrombosis after percutaneous left atrial appendage occlusion for atrial fibrillation. J. Am. Coll. Cardiol. 2018, 71, 1528–1536. [Google Scholar] [CrossRef] [PubMed]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.V.; Betts, T.; et al. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017, 14, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Tilz, R.R.; Potpara, T.; Chen, J.; Dobreanu, D.; Larsen, T.B.; Haugaa, K.H.; Dagres, N. Left atrial appendage occluder implantation in Europe: Indications and anticoagulation post-implantation. Results of the European Heart Rhythm Association survey. Europace 2017, 19, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Tzikas, A.; Shakir, S.; Gafoor, S.; Omran, H.; Nielsen-Kudsk, J.E.; Kefer, J.; Aminian, A.; Berti, S.; Santoro, G.; et al. Incidence and clinical impact of device-associated thrombus and peri-device leak following left atrial appendage closure with the amplatzer cardiac plug. JACC Cardiovasc. Interv. 2017, 10, 391–399. [Google Scholar] [CrossRef]
- Plicht, B.; Konorza, T.F.M.; Kahlert, P.; Al-Rashid, F.; Kaelsch, H.; Jánosi, R.A.; Buck, T.; Bachmann, H.S.; Siffert, W.; Heusch, G.; et al. Risk factors for thrombus formation on the amplatzer cardiac plug after left atrial appendage occlusion. JACC Cardiovasc. Interv. 2013, 6, 606–613. [Google Scholar] [CrossRef] [Green Version]
- Sedaghat, A.; Schrickel, J.-W.; Andrié, R.; Schueler, R.; Nickenig, G.; Hammerstingl, C. Thrombus formation after left atrial appendage occlusion with the amplatzer amulet device. JACC Clin. Electrophysiol. 2017, 3, 71–75. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | N | Study Design | Population Type | Type of Stent | Type of P2Y12 Inhibitor | DAPT Duration | Primary Endpoint | Event Rates (Short vs. Long) | Duration of Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|
| CREDO | 2002 | 2116 | Superiority of 12 mo DAPT * | ACS 67% | BMS 76.3% POBA 23.7% | Clopidogrel 100% | 1 vs. 12 | Death MI or stroke | 11.5% vs. 8.5% | 12 mo |
| PRODIGY | 2012 | 1970 | Superiority of 24 mo DAPT | ACS 75% | BMS 25% 1st gen DES 25% 2nd gen DES 50% | Clopidogrel 100% | 6 vs. 24 | All-cause death, MI, CVA | 10% vs. 10.1% | 24 mo |
| ARTIC INTERRUPTION | 2012 | 1259 | Superiority of 12 mo DAPT | ACS 34% | 1st gen DES 41% 2nd gen DES 63% | Clopidogrel 91% Prasugrel 9% | 12 vs. 18–24 | All-cause death, MI, ST, stroke, TVR | 4% vs. 4%. | 17 mo |
| EXCELLENT | 2012 | 1443 | Non-inferiority of 6 mo DAPT | ACS 51% | 1st gen DES 25% 2nd gen DES 75% | Clopidogrel 100% | 6 vs. 12 | Cardiac death, MI, TVR | 4.8% vs. 4.3% | 12 mo |
| RESET | 2012 | 2117 | Non-inferiority of 3 mo DAPT | ACS 59% | 1st gen DES 21% 2nd gen DES 85% | Clopidogrel 100% | 3 vs. 12 | Cardiac death, MI, ST, TVR, major bleeding | 4.7% vs. 4.7% | 12 mo |
| OPTIMIZE | 2013 | 3119 | Non-inferiority of 3 mo DAPT | ACS 35% | 2nd gen DES 100% | Clopidogrel 100% | 3 vs. 12 | All-cause death, MI, stroke, major bleeding | 6% vs. 5.8% | 12 mo |
| DES-LATE | 2014 | 5045 | Superiority of 24 mo DAPT | ACS 61% | 1st gen DES 64% 2nd gen DES 30% | Clopidogrel 100% | 12 vs. 36 | Cardiac death, MI, stroke | 2.4% vs. 2.6% | 24 mo |
| DAPT | 2014 | 9961 | Superiority of 30 mo DAPT | ACS 43% | 1st gen DES 38% 2nd gen DES 60% | Clopidogrel 65.3% Prasugrel 34.7% | 12 vs. 30 | Death, MI, stroke, ST. | 7.3% vs. 4.7% | 33 mo |
| SECURITY | 2014 | 1399 | Non-inferiority of 6 mo DAPT | 28% ACS | 2nd gen DES 100% | Clopidogrel 98.7% Prasugrel 0.2% Ticagrelor 0.4% | 6 vs. 12 | Cardiac death, MI, ST, or stroke | 4.5% vs. 3.7% | 12 mo |
| ISAR SAFE | 2015 | 4000 | Non-inferiority of 6 mo DAPT | ACS 40% | 1st gen DES 10% 2nd gen DES 89% | Clopidogrel 100% | 6 vs. 12 | Death, MI, ST, stroke, major bleeding | 1.5% vs. 1.6% | 15 mo |
| ITALIC | 2015 | 1822 | Non-inferiority of 6 mo DAPT | ACS 24% | 2nd gen DES 100% | Clopidogrel 98.6% Prasugrel 1.7% Ticagrelor 0.05% | 6 vs. 24 | Death, MI, TVR, stroke, major bleeding | 1.6% vs. 1.5% | 24 mo |
| I LOVE IT 2 | 2016 | 1829 | Non-inferiority of 6 mo DAPT | ACS 64% | 2nd gen DES 100% | Clopidogrel 100% | 6 vs. 12 | Cardiac death, target vessel MI | 7.5% vs. 6.3% | 18 mo |
| OPTIDUAL | 2016 | 1385 | Superiority of 48 mo DAPT | ACS 36% | 1st gen DES 34% 2nd gen DES 59% | Clopidogrel 100% | 12 vs. 48 | Death, MI, stroke, ISTH major bleeding | 7.5% vs. 5.8% | 33 mo after randomization |
| IVUS XPL | 2016 | 1400 | Comparability of 6 vs. 12 mo DAPT | ACS 49% | 2nd gen DES 100% | Clopidogrel 100% | 6 vs. 12 | Cardiac death, MI, stroke, or major bleeding | 2.2% vs. 2.1% | 12 mo |
| NIPPON | 2016 | 3307 | Non-inferiority of 6 mo DAPT | ACS 33% | 2nd gen DES 100% | Clopidogrel 97.5% Prasugrel 0.1% Ticlopidine 2.3% | 6 vs. 18 | Death, MI, CVA, major bleeding | 2.1% vs. 1.5% | 18 mo |
| REDUCE | 2017 | 1496 | Non-inferiority of 3 mo DAPT | ACS 100% | 2nd gen DES 100% | Clopidogrel 40.8% Prasugrel 10.4% Ticagrelor 48.9% | 3 vs. 12 | All-cause death, MI, ST, stroke, TVR, or bleeding | 8.3% vs. 8.5% | 12 mo |
| DAPT-STEMI | 2017 | 861 | Non-inferiority of 6 mo DAPT | ACS (STEMI) 100% | 2nd gen DES 100% | Clopidogrel 42.0% Prasugrel 29.5% Ticagrelor 28.5% | 6 vs. 12 | All-cause mortality, MI, revascularization, stroke, and TIMI major bleeding | 4.8% vs. 6.6% | 24 mo |
| OPTIMA-C | 2018 | 1368 | Non-inferiority of 6 vs. 12 mo DAPT | ACS 50% | 2nd gen DES 100% | Clopidogrel 100% | 6 vs. 12 | Cardiac death, TVR MI, Ischemia-driven TVR | 1.2% vs. 0.6% | 12 mo |
| SMART-DATE | 2018 | 2712 | Non-inferiority of 6 mo DAPT | ACS 100% | 2nd gen DES 100% | Clopidogrel 80.7% Prasugrel/ Ticagrelor 19.3% | 6 vs. 12 | All-cause mortality, MI, stroke | 4.7% vs. 4.2% | 18 mo |
| GLOBAL LEADERS | 2018 | 15,968 | Superiority of 1 mo DAPT followed by 23 mo ticagrelor monotherapy vs. 12 mo DAPT followed by 12 mo ASA | ACS 47% | 2nd gen DES 100% | Ticagrelor 46.8% Clopidogrel 53.2% | 1 vs. 12 | All-cause mortality non-fatal Q-wave MI | 3.8% vs. 4.3% | 24 mo |
| STOP DAPT 2 | 2019 | 3045 | Non-inferiority of 1 month of DAPT followed by clopidogrel monotherapy compared with 12 mo DAPT | ACS 38.2% | 2nd gen DES 100% | Clopidogrel 100% | 1 vs. 12 | CV death, MI, ischemic or hemorrhagic stroke, definite ST, or major or minor bleeding | 2.4% vs. 3.7% | 12 mo |
| SMART CHOICE | 2019 | 2993 | Non-inferiority of 3 mo of DAPT followed by P2Y12 inhibitor monotherapy compared with 12 mo DAPT | ACS 58.2% | 2nd gen DES 100% | Clopidogrel 77.2% Prasugrel or Ticagrelor 22.8% | 3 vs. 12 | Death, MI or stroke | 2.9% vs. 2.5% | 12 mo |
| Randomization | N | Study Type | Recent ACS% | Age | Type of Antiplatelet Therapy Associated | F.U | Study Hypothesis | Primary Efficacy Endpoint | Primary Safety Endpoint | Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RE-DEEM | Dabigatran 50 mg bid 75 mg bid 110 mg bid 150 mg bid vs. Placebo | 1861 | Double Blind Phase 2 | 100% | 61.8 | Aspirin + Clopidogrel | 6 month | Explore the rate of bleeding with dose escalating Dabigatran triple therapy | Reduction in D-dimer levels | Major or clinically relevant minor bleeding (ISTH, TIMI e GUSTO) | Dose-dependent increase in bleeding events with Dabigatran on top of antiplatelet therapy |
| ATLAS ACS-TIMI 46 | Rivaroxaban 5 mg od (or 2.5 mg bid) or 20 mg od (or 10 mg bid) vs. Placebo | 3491 | Double Blind Phase 2 | 100% | 58 | Aspirin Alone or Aspirin + Thyenopiridine | 6 month | Explore the rate of bleeding with dose escalating Rivaroxaban triple/dual therapy | Death, myocardial infarction, stroke, or severe recurrent ischemia requiring revascularization | TIMI major, TIMI minor, or requiring medical attention | Dose-dependent increase in bleeding events with Rivaroxaban on top of antiplatelet therapy |
| ATLAS ACS 2–TIMI 51 | Rivaroxaban 2.5 mg bid or 5 mg bid vs. Placebo | 15526 | Double Blind Phase 3 | 100% | 61.7 | Aspirin + Thienopyridine | 13 month | Rivaroxaban superior to placebo for the study primary efficacy endpoint | Death from cardiovascular causes, myocardial infarction, or stroke | Major non-CABG related bleeding (TIMI) | Rivaroxaban significantly reduced the primary efficacy endpoint |
| GEMINI ACS 1 | Rivaroxaban 2.5 mg bid vs. Aspirin | 3037 | Double Blind Phase 2 | 100% | 62.3 | clopidogrel/ ticagrelor | 13 month | Estimate the bleeding risk of rivaroxaban compared with aspirin on top of standard P2Y12 inhibitor therapy | Cardiovascular death, myocardial infarction, stroke, or definite stent thrombosis | Non-CABG clinically signicant bleeding (TIMI) | Similar bleeding rate between rivaroxaban and aspirin on top of P2Y12i. |
| COMPASS | Rivaroxaban 2.5 mg bid + Aspirin Rivaroxaban 5 mg bid vs. Aspirin | 27395 | Double Blind Phase 3 | 0% | 68 | N.A. | 23 month | Rivaroxaban superior to aspirin for the study primary efficacy endpoint | Cardiovascular death, myocardial infarction and stroke | Major or minor bleeding (ISTH) | Rivaroxaban 2.5 mg bid + aspirin significantly reduced the primary efficacy endpoint compared to aspirin alone |
| COMMANDER HF | Rivaroxaban 2.5 mg bid vs. Placebo | 5022 | Double Blind Phase 3 | 0% | 66.4 | N.A. | 21 month | Rivaroxaban superior to placebo for the study primary efficacy endpoint | Death from any cause, myocardial infarction, or stroke | Fatal bleeding or bleeding into a critical space with a potential for permanent disability | No difference for the primary efficacy endpoint neither for the safety endpoint between rivaroxaban and placebo. |
| APPRAISE | Apixaban 2.5 mg bid or 10 mg od 10 mg bid 20 mg od vs. Placebo | 1715 | Double Blind Phase 2 | 100% | 60.8 | Aspirin + Clopidogrel | 6 month | Explore the rate of bleeding with dose escalating Apixaban triple/dual therapy | Cardiovascular death, myocardial infarction, severe recurrent ischemia, or ischemic stroke | Major or clinically relevant nonmajor bleeding (ISTH) | Dose-dependent increase in bleeding events with Apixaban on top of antiplatelet therapy |
| APPRAISE J | Apixaban 2.5 mg bid or 5 mg bid vs. Placebo | 150 | Double Blind Phase 2 | 100% | 64.6 | Aspirin + Clopidogrel | 6 month | Explore the rate of bleeding with dose escalating Apixaban triple/dual therapy in a Japanese population | Deaths, nonfatal myocardial infarction, unstable angina and stroke | Major or clinically relevant nonmajor bleeding (ISTH) | Dose-dependent increase in bleeding events with Apixaban on top of antiplatelet therapy |
| APPRAISE II | Apixaban 5 mg bid vs. Placebo | 7392 | Double Blind Phase 3 | 100% | 67 | Apirin + Clopidogrel | 8 month | Apixaban superior to placebo for the study primary endpoint | Cardiovascular death, myocardial infarction, or ischemic stroke | Major bleeding (TIMI) | Apixaban increased the number of major bleeding without a reduction in ischemic events |
| AFIRE | Rivaroxaban 15 mg or 10 mg vs. Rivaroxaban + Antiplatelet therapy | 2236 | Open Label Phase 4 | 0% | 74 | Aspirin or Clopidogrel | 24 month | Rivaroxaban monotherapy non-inferior for ischemia and superior for bleeding vs. Rivaroxaban + antiplatelet therapy | All-cause mortality, myocardial infarction, stroke, unstable angina requiring revascularization, or systemic embolism | Major bleeding (ISTH criteria) | Rivaroxaban monotherapy was non-inferior to the combination therapy for efficacy and superior for safety in patients with atrial fibrillation and stable coronary artery disease |
| N | Randomization | P2Y12i Type | OAC Type | ACS | Age * | CHAD2Ds2 VASc | HAS BLEED | F.U. | Primary Endpoint | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| WOEST | 573 | W-DT vs. W-TT | C (100%) | W | ACS 27% | 70 | 1.5 | N.A. | 12 mo | Any bleeding (TIMI, GUSTO, BARC) | W-DT 19.4% vs. W-TT 44.4% HR 0.36 (95% CI 0.26–0.50) p < 0.0001 |
| ISAR TRIPLE | 614 | W-TT 6 wk vs. W-TT 6 mo | C (100%) | W | ACS 32% | 73 | 3.9 | N.A. | 9 mo | Death, MI, ST, stroke or major bleeding (TIMI) | 6wkTT 9.8% vs. 6moTT 8.8% HR 1.14 (95% CI 0.68–1.91) p = 0.63 |
| PIONEER AF PCI | 2124 | R-DT vs. W-TT vs. R-TT | C (94.3%)/ T (4.2%)/ p (1.3%) | W rivaroxaban 2,5 mg bid rivaroxaban 15 mg od | ACS 51.6% | 70 | n.a. | N.A. | 12 mo | Major or minor bleeding (TIMI) or bleeding requiring medical attention | R-DT 16.8% vs. W-TT 26.7% HR 0.59 (CI 0.47–0.76) p < 0.001 |
| RE-DUAL PCI | 2725 | D-DT110 or D-DT150 vs. W-TT | C (86%) T (12%) | W Dabigatran 110 mg bid Dabigatran 150 mg bid | ACS 50.5% | 70 | 3.6 | 2.7 | 14 mo | Major or clinically relevant nonmajor bleeding event (ISTH) | D-DT110 15.4% vs. W-TT 26.9% HR 0.52 (95% CI 0.42–0.63) p < 0.001 |
| D-DT150 20.2% vs. W-TT 25.7% HR 0.72 (95% CI 0.58–0.88) p = 0.002 | |||||||||||
| AUGUSTUS | 4614 | Factorial A vs. W DT vs. TT | C (92,6%) T (6,2%) p (1,1%) | W Apixaban 5 mg bid ** | ACS 37.3% | 70.7 | 4 | 2.9 | 12 mo | Major or clinically relevant nonmajor bleeding (ISTH) | A 10.5% vs. W 14.7% HR 0.69 (95% CI 0.58–0.81) p < 0.001 |
| DT 9% vs. TT 16.1% HR 1.89 (95% CI 1.59–2.24) p < 0.001 | |||||||||||
| ENTRUST AF-PCI | 1506 | E-DT vs. W-TT | C (92%) T (8%) p (2%) | W Edoxaban 60 mg *** | ACS 52% | 69 | 4 | 3 | 12 mo | Major or clinically relevant non-major bleeding (ISTH) | E-DT 17% vs. W-TT 20% HR 0.83 (0.65–1.05) p non-inferiority = 0.001 p superiority = 0.12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caracciolo, A.; Mazzone, P.; Laterra, G.; Garcia-Ruiz, V.; Polimeni, A.; Galasso, S.; Saporito, F.; Carerj, S.; D’Ascenzo, F.; Marquis-Gravel, G.; et al. Antithrombotic Therapy for Percutaneous Cardiovascular Interventions: From Coronary Artery Disease to Structural Heart Interventions. J. Clin. Med. 2019, 8, 2016. https://doi.org/10.3390/jcm8112016
Caracciolo A, Mazzone P, Laterra G, Garcia-Ruiz V, Polimeni A, Galasso S, Saporito F, Carerj S, D’Ascenzo F, Marquis-Gravel G, et al. Antithrombotic Therapy for Percutaneous Cardiovascular Interventions: From Coronary Artery Disease to Structural Heart Interventions. Journal of Clinical Medicine. 2019; 8(11):2016. https://doi.org/10.3390/jcm8112016
Chicago/Turabian StyleCaracciolo, Alessandro, Paolo Mazzone, Giulia Laterra, Victoria Garcia-Ruiz, Alberto Polimeni, Salvatore Galasso, Francesco Saporito, Scipione Carerj, Fabrizio D’Ascenzo, Guillaume Marquis-Gravel, and et al. 2019. "Antithrombotic Therapy for Percutaneous Cardiovascular Interventions: From Coronary Artery Disease to Structural Heart Interventions" Journal of Clinical Medicine 8, no. 11: 2016. https://doi.org/10.3390/jcm8112016