

A State-of-the-Art Review of Intra-Operative Imaging Modalities Used to Quality Assure Endovascular Aneurysm Repair
 , , and
, , and
Abstract
:1. Introduction
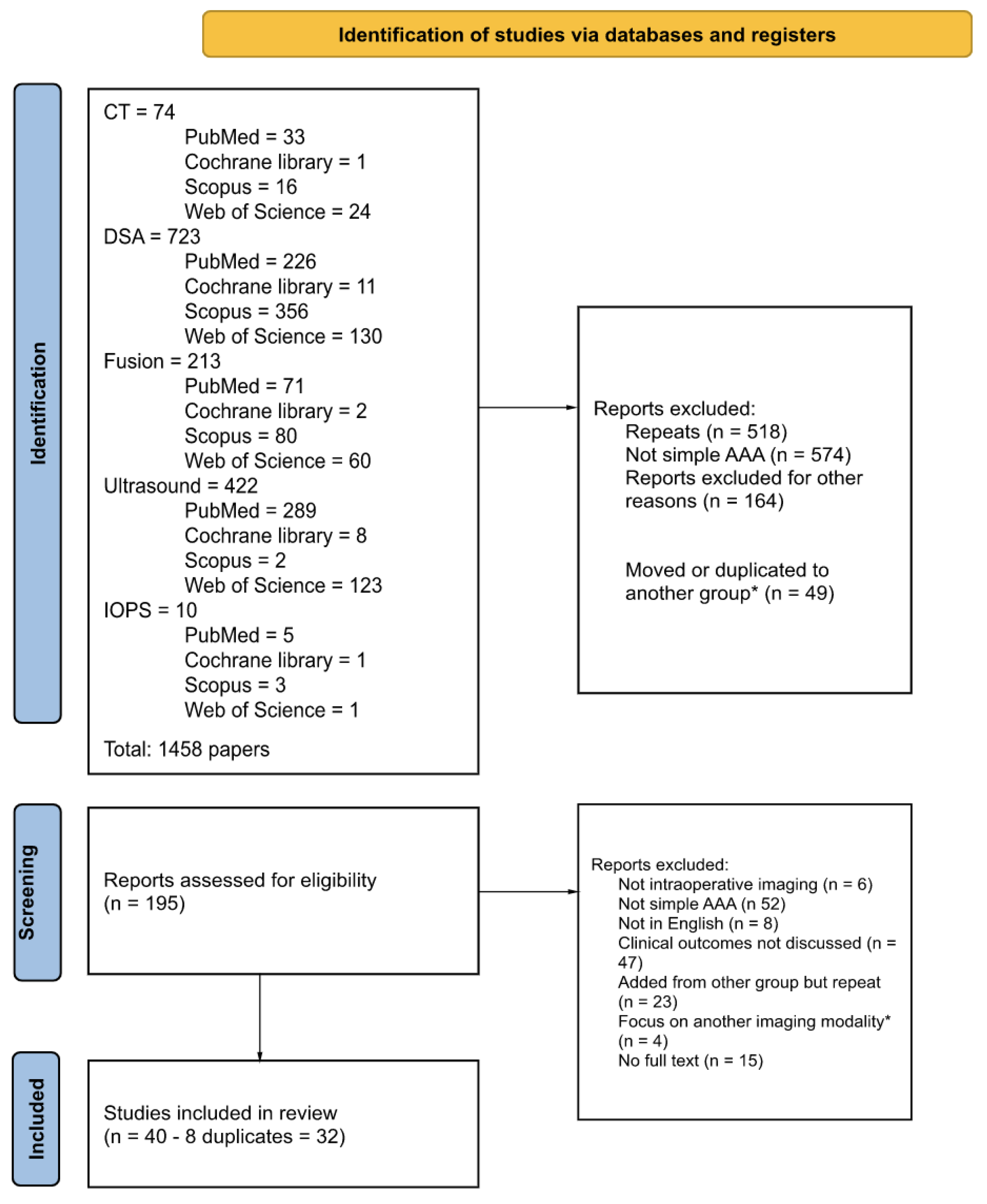
2. Materials and Methods
3. Results
3.1. Computerised Tomography
3.1.1. Detection of Endoleaks
3.1.2. Radiation Exposure
3.2. Digital Subtraction Angiography
3.2.1. Detection of Endoleaks
3.2.2. Radiation Exposure
3.3. Fusion Imaging
3.3.1. Vascular Displacement after Stiff Wire
3.3.2. Image Registration
3.3.3. 2D-3D vs. 3D-3D
3.3.4. Radiation Exposure
3.3.5. Reduction of Iodinated Contrast
3.4. Non-Contrast Imaging
3.5. Ultrasound Imaging
3.5.1. Detection of Endoleaks
3.5.2. Stent Deployment
3.5.3. Measuring Stent Graft Size
3.6. Intra-Operative Positioning System
3.7. Risk of Bias
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volodos, N.L.; Shekhanin, V.E.; Karpovich, I.P.; Troian, V.I.; Gur’ev Iu, A. A self-fixing synthetic blood vessel endoprosthesis. Vestn Khir Im I I Grek 1986, 137, 123–125. [Google Scholar]
- United Kingdom EVAR Trial Investigators; Greenhalgh, R.M.; Brown, L.C.; Powell, J.T.; Thompson, S.G.; Epstein, D.; Sculpher, M.J. Endovascular versus Open Repair of Abdominal Aortic Aneurysm. N. Engl. J. Med. 2010, 362, 1863–1871. [Google Scholar] [CrossRef] [PubMed]
- Prinssen, M.; Verhoeven, E.L.G.; Buth, J.; Cuypers, P.W.M.; van Sambeek, M.R.H.M.; Balm, R.; Buskens, E.; Grobbee, D.E.; Blankensteijn, J.D. A Randomized Trial Comparing Conventional and Endovascular Repair of Abdominal Aortic Aneurysms. N. Engl. J. Med. 2004, 351, 1607–1618. [Google Scholar] [CrossRef] [PubMed]
- Lederle, F.A.; Kyriakides, T.C.; Stroupe, K.T.; Freischlag, J.A.; Padberg, F.T.; Matsumura, J.S.; Huo, Z.; Johnson, G.R. Open versus Endovascular Repair of Abdominal Aortic Aneurysm. N. Engl. J. Med. 2019, 380, 2126–2135. [Google Scholar] [CrossRef]
- Patel, R.; Sweeting, M.J.; Powell, J.T.; Greenhalgh, R.M. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): A randomised controlled trial. Lancet 2016, 388, 2366–2374. [Google Scholar] [CrossRef]
- The Lancet. Open versus endovascular repair of aortic aneurysms. Lancet 2020, 395, 1090. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Abdominal aortic aneurysm: Diagnosis and management (NG156). NICE Guideline [NG156], 2020. Available online: https://www.nice.org.uk/guidance/ng156 (accessed on 8 January 2023).
- Dua, A.; Eagleton, M.J. A Revolution of EVAR Imaging Technologies. Endovascular Today, 1 November 2019. [Google Scholar]
- Belvroy, V.M.; Houben, I.B.; Trimarchi, S.; Patel, H.J.; Moll, F.L.; Van Herwaarden, J.A. Identifying and addressing the limitations of EVAR technology. Expert. Rev. Med. Devices 2018, 15, 541–554. [Google Scholar] [CrossRef]
- Moll, F.L.; Powell, J.T.; Fraedrich, G.; Verzini, F.; Haulon, S.; Waltham, M.; van Herwaarden, J.A.; Holt, P.J.E.; van Keulen, J.W.; Rantner, B.; et al. Management of Abdominal Aortic Aneurysms Clinical Practice Guidelines of the European Society for Vascular Surgery. Eur. J. Vasc. Endovasc. Surg. 2011, 41, S1–S58. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Biasi, L.; Ali, T.; Hinchliffe, R.; Morgan, R.; Loftus, I.; Thompson, M. Intraoperative DynaCT detection and immediate correction of a type Ia endoleak following endovascular repair of abdominal aortic aneurysm. Cardiovasc. Intervent. Radiol. 2009, 32, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Breininger, K.; Hanika, M.; Weule, M.; Kowarschik, M.; Pfister, M.; Maier, A. Simultaneous reconstruction of multiple stiff wires from a single X-ray projection for endovascular aortic repair. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1891–1899. [Google Scholar] [CrossRef]
- Bush, R.L.; Lin, P.H.; Bianco, C.C.; Lumsden, A.B.; Gunnoud, A.B.; Terramani, T.T.; Brinkman, W.T.; Martin, L.G.; Weiss, V.J. Endovascular aortic aneurysm repair in patients with renal dysfunction or severe contrast allergy: Utility of imaging modalities without iodinated contrast. Ann. Vasc. Surg. 2002, 16, 537–544. [Google Scholar] [CrossRef]
- Chao, A.; Major, K.; Kumar, S.R.; Patel, K.; Trujillo, I.; Hood, D.B.; Rowe, V.L.; Weaver, F.A. Carbon dioxide digital subtraction angiography-assisted endovascular aortic aneurysm repair in the azotemic patient. J. Vasc. Surg. 2007, 45, 451–458. [Google Scholar] [CrossRef] [PubMed]
- de Ruiter, Q.M.; Moll, F.L.; Gijsberts, C.M.; van Herwaarden, J.A. AlluraClarity Radiation Dose-Reduction Technology in the Hybrid Operating Room During Endovascular Aneurysm Repair. J. Endovasc. Ther. 2016, 23, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, M.L.; Eagleton, M.J.; Greenberg, R.K.; Mastracci, T.; Hernandez, A. Intraoperative C-arm cone-beam computed tomography in fenestrated/branched aortic endografting. J. Vasc. Surg. 2011, 53, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Faries, P.L.; Briggs, V.L.; Bernheim, J.; Kent, K.C.; Hollier, L.H.; Marin, M.L. Increased recognition of type II endoleaks using a modified intraoperative angiographic protocol: Implications for intermittent endoleak and aneurysm expansion. Ann. Vasc. Surg. 2003, 17, 608–614. [Google Scholar] [CrossRef]
- Gallitto, E.; Faggioli, G.; Vacirca, A.; Pini, R.; Mascoli, C.; Fenelli, C.; Logiacco, A.; Abualhin, M.; Gargiulo, M. The benefit of combined carbon dioxide automated angiography and fusion imaging in preserving perioperative renal function in fenestrated endografting. J. Vasc. Surg. 2020, 72, 1906–1916. [Google Scholar] [CrossRef]
- Garrett, H.E.; Abdullah, A.H.; Hodgkiss, T.D.; Burgar, S.R. Intravascular ultrasound aids in the performance of endovascular repair of abdominal aortic aneurysm. J. Vasc. Surg. 2003, 37, 615–618. [Google Scholar] [CrossRef]
- Gennai, S.; Leone, N.; Saitta, G.; Migliari, M.; Lauricella, A.; Farchioni, L.; Silingardi, R. Intravascular Ultrasound in Branched and Fenestrated Endovascular Aneurysm Repair: Initial Experience in a Single-Center Cohort Study. J. Endovasc. Ther. 2021, 28, 828–836. [Google Scholar] [CrossRef]
- Hertault, A.; Rhee, R.; Antoniou, G.A.; Adam, D.; Tonda, H.; Rousseau, H.; Bianchini, A.; Haulon, S. Radiation Dose Reduction During EVAR: Results from a Prospective Multicentre Study (The REVAR Study). Eur. J. Vasc. Endovasc. Surg. 2018, 56, 426–433. [Google Scholar] [CrossRef]
- Jansen, M.M.; van der Stelt, M.; Smorenburg, S.P.M.; Slump, C.H.; van Herwaarden, J.A.; Hazenberg, C. Target vessel displacement during fenestrated and branched endovascular aortic repair and its implications for the role of traditional computed tomography angiography roadmaps. Quant. Imaging Med. Surg. 2021, 11, 3945–3955. [Google Scholar] [CrossRef] [PubMed]
- Kaladji, A.; Dumenil, A.; Mahé, G.; Castro, M.; Cardon, A.; Lucas, A.; Haigron, P. Safety and accuracy of endovascular aneurysm repair without pre-operative and intra-operative contrast agent. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Keschenau, P.R.; Alkassam, H.; Kotelis, D.; Jacobs, M.J.; Kalder, J. Intraoperative contrast-enhanced ultrasound examination for endoleak detection after complex and infrarenal endovascular aortic repair. J. Vasc. Surg. 2020, 71, 1200–1206. [Google Scholar] [CrossRef]
- Kobeiter, H.; Nahum, J.; Becquemin, J.P. Zero-contrast thoracic endovascular aortic repair using image fusion. Circulation 2011, 124, e280–e282. [Google Scholar] [CrossRef]
- Kopp, R.; Zürn, W.; Weidenhagen, R.; Meimarakis, G.; Clevert, D.A. First experience using intraoperative contrast-enhanced ultrasound during endovascular aneurysm repair for infrarenal aortic aneurysms. J. Vasc. Surg. 2010, 51, 1103–1110. [Google Scholar] [CrossRef]
- Koutouzi, G.; Roos, H.; Henrikson, O.; Leonhardt, H.; Falkenberg, M. Orthogonal Rings, Fiducial Markers, and Overlay Accuracy When Image Fusion is Used for EVAR Guidance. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 604–611. [Google Scholar] [CrossRef]
- Lalys, F.; Barré, A.; Kafi, M.; Benziane, M.; Saudreau, B.; Dupont, C.; Kaladji, A. Identification of Parameters Influencing the Vascular Structure Displacement in Fusion Imaging during Endovascular Aneurysm Repair. J. Vasc. Interv. Radiol. 2019, 30, 1386–1392. [Google Scholar] [CrossRef]
- Massoni, C.B.; Perini, P.; Fanelli, M.; Ucci, A.; Azzarone, M.; Rossi, G.; D’ospina, R.M.; Freyrie, A. The utility of intraoperative contrast-enhanced ultrasound for immediate treatment of type ia endoleak during evar: Initial experience. Acta Biomed. 2021, 92, e2021046. [Google Scholar] [CrossRef]
- Massoni, C.B.; Perini, P.; Fanelli, M.; Ucci, A.; Rossi, G.; Azzarone, M.; Tecchio, T.; Freyrie, A. Intraoperative contrast-enhanced ultrasound for early diagnosis of endoleaks during endovascular abdominal aortic aneurysm repair. J. Vasc. Surg. 2019, 70, 1844–1850. [Google Scholar] [CrossRef]
- Maurel, B.; Hertault, A.; Gonzalez, T.M.; Sobocinski, J.; Le Roux, M.; Delaplace, J.; Azzaoui, R.; Midulla, M.; Haulon, S. Evaluation of visceral artery displacement by endograft delivery system insertion. J. Endovasc. Ther. 2014, 21, 339–347. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.M.; Scali, S.T.; Feezor, R.J.; Neal, D.; Huber, T.S.; Beck, A.W. Three-dimensional fusion computed tomography decreases radiation exposure, procedure time, and contrast use during fenestrated endovascular aortic repair. J. Vasc. Surg. 2015, 61, 309–316. [Google Scholar] [CrossRef]
- Panuccio, G.; Torsello, G.F.; Pfister, M.; Bisdas, T.; Bosiers, M.J.; Torsello, G.; Austermann, M. Computer-aided endovascular aortic repair using fully automated two- and three-dimensional fusion imaging. J. Vasc. Surg. 2016, 64, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Rolls, A.E.; Rosen, S.; Constantinou, J.; Davis, M.; Cole, J.; Desai, M.; Stoyanov, D.; Mastracci, T.M. Introduction of a Team Based Approach to Radiation Dose Reduction in the Enhancement of the Overall Radiation Safety Profile of FEVAR. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 451–457. [Google Scholar] [CrossRef]
- Schulz, C.J.; Schmitt, M.; Böckler, D.; Geisbüsch, P. Intraoperative contrast-enhanced cone beam computed tomography to assess technical success during endovascular aneurysm repair. J. Vasc. Surg. 2016, 64, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.J.; Böckler, D.; Krisam, J.; Geisbüsch, P. Two-dimensional-three-dimensional registration for fusion imaging is noninferior to three-dimensional- three-dimensional registration in infrarenal endovascular aneurysm repair. J. Vasc. Surg. 2019, 70, 2005–2013. [Google Scholar] [CrossRef]
- Schwein, A.; Chinnadurai, P.; Behler, G.; Lumsden, A.B.; Bismuth, J.; Bechara, C.F. Computed tomography angiography-fluoroscopy image fusion allows visceral vessel cannulation without angiography during fenestrated endovascular aneurysm repair. J. Vasc. Surg. 2018, 68, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Stangenberg, L.; Shuja, F.; Carelsen, B.; Elenbaas, T.; Wyers, M.C.; Schermerhorn, M.L. A novel tool for three-dimensional roadmapping reduces radiation exposure and contrast agent dose in complex endovascular interventions. J. Vasc. Surg. 2015, 62, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Steuwe, A.; Geisbüsch, P.; Schulz, C.J.; Böckler, D.; Kauczor, H.U.; Stiller, W. Comparison of Radiation Exposure Associated With Intraoperative Cone-Beam Computed Tomography and Follow-up Multidetector Computed Tomography Angiography for Evaluating Endovascular Aneurysm Repairs. J. Endovasc. Ther. 2016, 23, 583–592. [Google Scholar] [CrossRef]
- Tenorio, E.R.; Oderich, G.S.; Sandri, G.A.; Ozbek, P.; Kärkkäinen, J.M.; Macedo, T.A.; Vrtiska, T.; Cha, S. Impact of onlay fusion and cone beam computed tomography on radiation exposure and technical assessment of fenestrated-branched endovascular aortic repair. J. Vasc. Surg. 2019, 69, 1045–1058.e1043. [Google Scholar] [CrossRef]
- Timaran, L.I.; Timaran, C.H.; Scott, C.K.; Soto-Gonzalez, M.; Timaran-Montenegro, D.E.; Guild, J.B.; Kirkwood, M.L. Dual fluoroscopy with live-image digital zooming significantly reduces patient and operating staff radiation during fenestrated-branched endovascular aortic aneurysm repair. J. Vasc. Surg. 2021, 73, 601–607. [Google Scholar] [CrossRef]
- Törnqvist, P.; Dias, N.; Sonesson, B.; Kristmundsson, T.; Resch, T. Intra-operative cone beam computed tomography can help avoid reinterventions and reduce CT follow up after infrarenal EVAR. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Gyánó, M.; Berczeli, M.; Csobay-Novák, C.; Szöllősi, D.; Óriás, V.I.; Góg, I.; Kiss, J.P.; Veres, D.S.; Szigeti, K.; Osváth, S.; et al. Digital variance angiography allows about 70% decrease of DSA-related radiation exposure in lower limb X-ray angiography. Sci. Rep. 2021, 11, 21790. [Google Scholar] [CrossRef]
- Rezaee, A.; Mehrabinejad, M.-M.; Bell, D.J.; Weerakkody, Y. Carbon dioxide angiography. Available online: https://radiopaedia.org/articles/53045 (accessed on 24 January 2023).
- Bashir, U.; Bell, D.J.; Chieng, R.; Yap, J.; Francavilla, M.; Sharma, R.; MacManus, D.; Gaillard, F.; Gamage, P.J.; Murphy, A.; et al. Gadolinium Contrast Agents. Available online: https://radiopaedia.org/articles/18340 (accessed on 24 January 2023).
- Shlofmitz, E.; Kerndt, C.C.; Parekh, A.; Khalid, N. Intravascular Ultrasound. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Muluk, S.C.; Elrakhawy, M.; Chess, B.; Rosales, C.; Goel, V. Successful endovascular treatment of severe chronic mesenteric ischemia facilitated by intraoperative positioning system image guidance. J. Vasc. Surg. Cases Innov. Tech. 2022, 8, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Vano, E.; Gonzalez, L.; Fernández, J.M.; Haskal, Z.J. Eye Lens Exposure to Radiation in Interventional Suites: Caution Is Warranted. Radiology 2008, 248, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Wan, R.C.; Chau, W.W.; Tso, C.Y.; Tang, N.; Chow, S.K.; Cheung, W.-H.; Wong, R.M. Occupational hazard of fluoroscopy: An invisible threat to orthopaedic surgeons. J. Orthop. Trauma Rehabil. 2021, 28, 22104917211035547. [Google Scholar] [CrossRef]
- Mastrangelo, G.; Fedeli, U.; Fadda, E.; Giovanazzi, A.; Scoizzato, L.; Saia, B. Increased cancer risk among surgeons in an orthopaedic hospital. Occup. Med. 2005, 55, 498–500. [Google Scholar] [CrossRef]
- Modarai, B.; Haulon, S.; Ainsbury, E.; Böckler, D.; Vano-Carruana, E.; Dawson, J.; Farber, M.; Van Herzeele, I.; Hertault, A.; van Herwaarden, J.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on Radiation Safety. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 171–222. [Google Scholar] [CrossRef]
- Jansen, M.; Khandige, A.; Kobeiter, H.; Vonken, E.-J.; Hazenberg, C.; van Herwaarden, J. Three dimensional visualisation of endovascular guidewires and catheters based on laser light instead of fluoroscopy with fiber optic RealShape technology: Preclinical results. Eur. J. Vasc. Endovasc. Sur. 2020, 60, 135–143. [Google Scholar] [CrossRef]
- Panuccio, G.; Schanzer, A.; Rohlffs, F.; Heidemann, F.; Wessels, B.; Schurink, G.W.; van Herwaarden, J.A.; Kölbel, T. Endovascular navigation with fiber optic RealShape technology. J. Vasc. Surg. 2023, 77, 3–8.e2. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| In English | Not in English |
| EVAR procedures | Not EVAR procedures |
| Intra-operative imaging | Involvement of iliac arteries in the aneurysm or not simple AAA (e.g., rupture or mycotic, etc.) Pre-operative or post-operative imaging only |
| Full text available | Clinical outcomes of imaging not discussed (e.g., purely technical papers, phantoms, etc.) Animal studies |
| Author | Year | Imaging Modality | Aneurysm Type | Study Type | n | Summary of Technical Success & Complications | Contrast Usage | Radiation Dose |
|---|---|---|---|---|---|---|---|---|
| Biasi et al. [12] | 2009 | DynaCT vs DSA | Infrarenal | Prospective | 392 | DynaCT found 5 (6.25%) complications not seen on completion DSA with 3.8% having immediate intervention | No difference | Increased |
| Breininger et al. [13] | 2019 | 2D3D | Non-specified EVAR | Retrospective | 19 | Successfully reconstructs Iliac displacement after stiffwire insertion from a 2D image | - | - |
| Bush et al. [14] | 2002 | Gadolinium-enhanced MRA, non-contrast CT, gadolinium or CO2 aortography, and IVUS | Infrarenal | Retrospective | 297 | Non-contrast technically successful in all patients | Reduced | - |
| Chao et al. [15] | 2007 | CO2-DSA vs. ICA-DSA | Infrarenal | Retrospective | 100 | No significant difference in technical success between groups | Reduced | Increased |
| de Ruiter et al. [16] | 2016 | DSA (mobile C-arm vs fixed C-arm/allura vs. fixed c-arm /AlluraClarity) | Infrarenal, complex | Retrospective | 85 | Image processing technology adjuncts can significantly help to reduce radiation exposure | - | Reduced |
| Dijkstra et al. [17] | 2011 | CBCT and 3D-3D fusion | Complex | Retrospective | 82 | Fusion technical success non inferior. No additional endoleaks found on MDCT. | Reduced | Reduced |
| Faries et al. [18] | 2003 | Standard angiography vs modified protocol | Non-specified AAA | Retrospective | 391 | Modified protocol detected more type II endoleaks but there was no significant difference in incidence of type II endoleaks by follow-up. | - | - |
| Gallitto et al. [19] | 2020 | 3D2D fusion with intraop CO2-DSA | Complex | Prospective | 45 | CO2 angiography results in better renal function preservation | No contrast use | Increased |
| Garret, Jr. et al. [20] | 2003 | CT vs. IVUS | Infrarenal | Retrospective | 78 | IVUS resulted in changing stent graft size (n = 22). 4 patients treated with EVAR using IVUS after preop CT suggesting unsuitable. | - | - |
| Gennai et al. [21] | 2021 | Fusion but vessel cannulation with IVUS | Complex | Retrospective | 10 | IVUS was technically successful in all cases, identifying problems in 12% of bridging stents that were not detected by completion angiography. | Reduced | Reduced |
| Hertault et al. [22] | 2018 | 3D2D with strict ALARA | Infrarenal | Prospective | 85 | - | Reduced | Reduced |
| Jansen et al. [23] | 2021 | 3D2D | Complex | Retrospective | 20 | - | - | - |
| Kaladji et al. [24] | 2015 | 3D2D without contrast | Infrarenal, thoracic | Prospective | 6 | EVAR graft deployment | No contrast use | - |
| Keschenau et al. [25] | 2020 | CEUS vs. DSA | Infrarenal, complex | Prospective | 21 | CEUS detected significantly more type II endoleaks than DSA. But only 5 of the 16 still persisted on pre-discharge CTA. | Reduced | Reduced |
| Kobeiter et al. [26] | 2011 | 3D2D without ICM for registration | Thoracic | Retrospective | 1 | TEVAR deployment | No contrast use | - |
| Kopp et al. [27] | 2010 | CEUS vs. DSA | Infrarenal | Prospective | 37 | CEUS was effective at identifying proximal (82.4%) and distal (89.3%) landing zones and identified more endoleaks than angiography. | Reduced | Reduced |
| Koutouzi et al. [28] | 2016 | 3D3D registration and 2D3D overlay | Infrarenal | Prospective | 19 | EVAR deployment | Reduced | Reduced |
| Lalys et al. [29] | 2019 | 3D2D fusion | Infrarenal | Prospective | 50 | Assessment of displacement | - | - |
| Massoni et al. [30] | 2021 | CEUS vs. DSA | Infrarenal | Prospective | 3 | In two cases type Ia endoleak was missed by angiography but detected by CEUS | - | - |
| Massoni et al. [31] | 2019 | CEUS vs. DSA | Infrarenal | Prospective | 60 | Postdeployment CEUS detected more endoleaks than DSA | - | - |
| Maurel et al. [32] | 2014 | 3D3D | Infrarenal, complex | Prospective | 20 | Stiffwire insertion causes significant diplacement of main aortic branches | Reduced | Increased |
| McNally et al. [33] | 2015 | 3D3D vs. fluoroscopy/DSA/IVUS | Complex | Retrospective | 72 | FEVAR deployment | Reduced | Reduced |
| Panuccio et al. [34] | 2016 | 3D2D but with mathematical model | Infrarenal, complex | Prospective | 25 | Fully automated fusion imaging is possible although manual intervention may be needed in some cases | Reduced | Reduced |
| Rolls et al. [35] | 2016 | 3D3D vs. standard fluoroscopic imaging | Complex | Prospective | 42 | Target vessel catheterisation and endoleak detection satisfactory. Fusion and team based approach reduced procedure time | - | Reduced |
| Schulz et al. [36] | 2016 | ceCBCT vs. cDSA | Infrarenal | Prospective | 98 | ceCBCT detected more endoleaks than CTA or DSA | Reduced | - |
| Schulz et al. [37] | 2019 | 2D3D fusion vs. 3D3D fusion | Non-specified EVAR | Prospective | 151 | Fusion imaging is feasible, and non-inferior to 3D3D offering better radiation exposure and time demand | - | Reduced |
| Schwein et al. [38] | 2018 | 3D-3D fusion and CTA-fluoroscopy | Complex | Retrospective | 26 | 83% of ostia cannulated without angiogram | Reduced | Reduced |
| Stangenberg et al. [39] | 2015 | 3D2D fusion using VesselNavigator | Infrarenal | Retrospective | 75 | Procedure time, fluoroscopy time and air kerma was lower with fusion | Reduced | Reduced |
| Steuwe et al. [40] | 2016 | CBCT vs MDCT | Infrarenal | Retrospective | 66 | CBCT reduces radiation dose compared to 3-phase MDCT required to assess technical success of EVAR | - | Reduced |
| Tenorio et al. [41] | 2019 | 3D3D onlay CTA fusion and CBCT without digital zoom capability 2D3D onlay CTA fusion, high definition CBCT with subtraction capability and digital zoom. | Complex | Retrospective | 386 | Successful stent deployment and endoleak detection | Reduced | Reduced |
| Timaran et al. [42] | 2021 | Standard vs. dual fluoroscopy with live-image digital zooming | Complex | Prospective | 151 | No difference in technical success between the two groups | - | Reduced |
| Törnqvist et al. [43] | 2015 | CBCT vs. DSA | Infrarenal | Prospective | 51 | CBCT more effective at detecting stent graft compression and kinks. DSA detected more endoleaks than CBCT | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bachrati, P.Z.; La Torre, G.; Chowdhury, M.M.; Healy, S.J.; Singh, A.A.; Boyle, J.R. A State-of-the-Art Review of Intra-Operative Imaging Modalities Used to Quality Assure Endovascular Aneurysm Repair. J. Clin. Med. 2023, 12, 3167. https://doi.org/10.3390/jcm12093167
Bachrati PZ, La Torre G, Chowdhury MM, Healy SJ, Singh AA, Boyle JR. A State-of-the-Art Review of Intra-Operative Imaging Modalities Used to Quality Assure Endovascular Aneurysm Repair. Journal of Clinical Medicine. 2023; 12(9):3167. https://doi.org/10.3390/jcm12093167
Chicago/Turabian StyleBachrati, Petra Z., Guglielmo La Torre, Mohammed M. Chowdhury, Samuel J. Healy, Aminder A. Singh, and Jonathan R. Boyle. 2023. "A State-of-the-Art Review of Intra-Operative Imaging Modalities Used to Quality Assure Endovascular Aneurysm Repair" Journal of Clinical Medicine 12, no. 9: 3167. https://doi.org/10.3390/jcm12093167