
Incidence and Outcomes of Abdominal Aortic Aneurysm Repair in New Zealand from 2001 to 2021

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Protocol and Data Collection
2.3. Ethnicity Definition
2.4. New Zealand Index of Deprivation (NZDep)
2.5. AAA-Related Hospitalisations
2.6. Statistical Analysis
3. Results
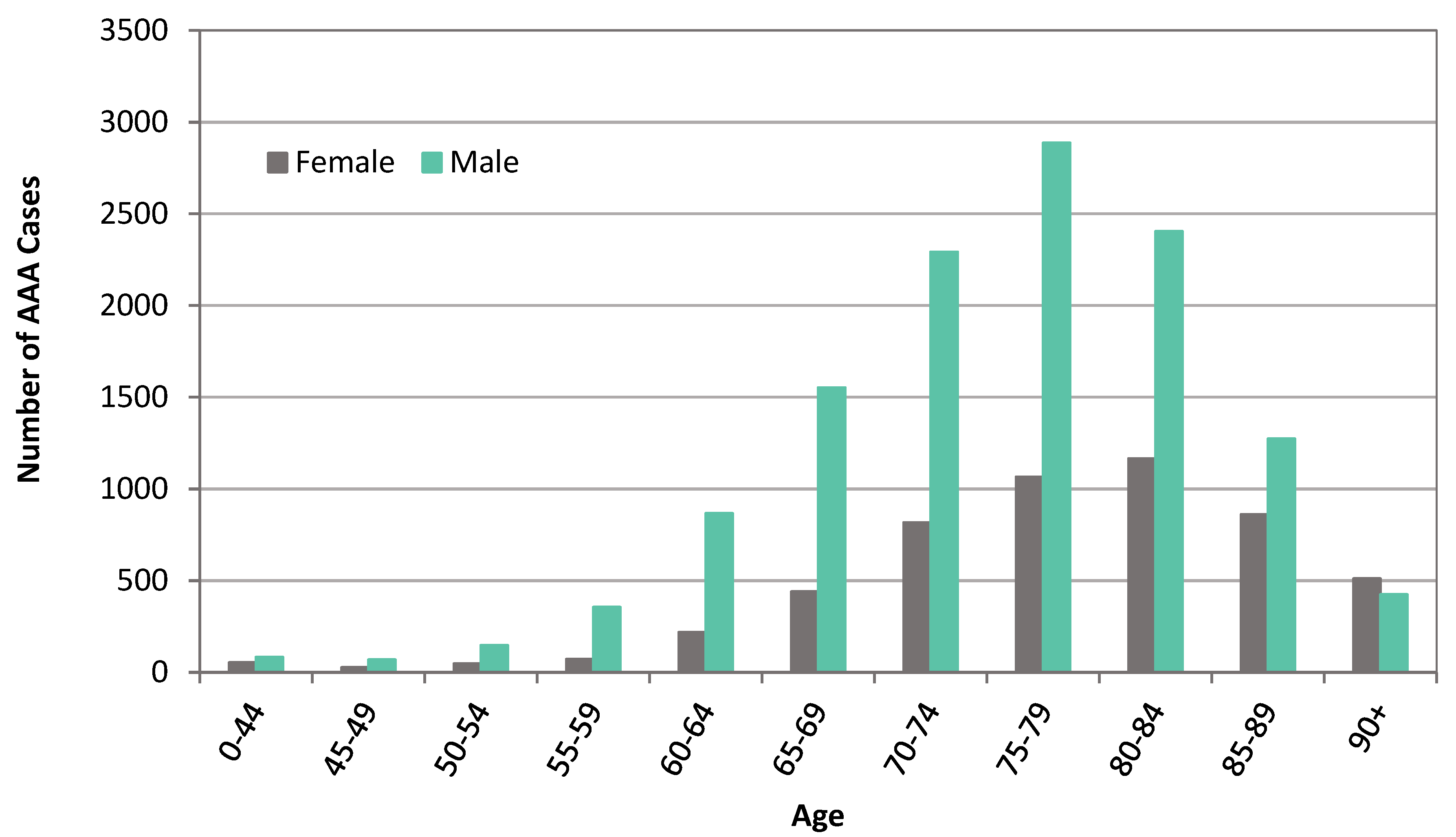
3.1. Patient Demographics
3.2. AAA Presentation and Repair
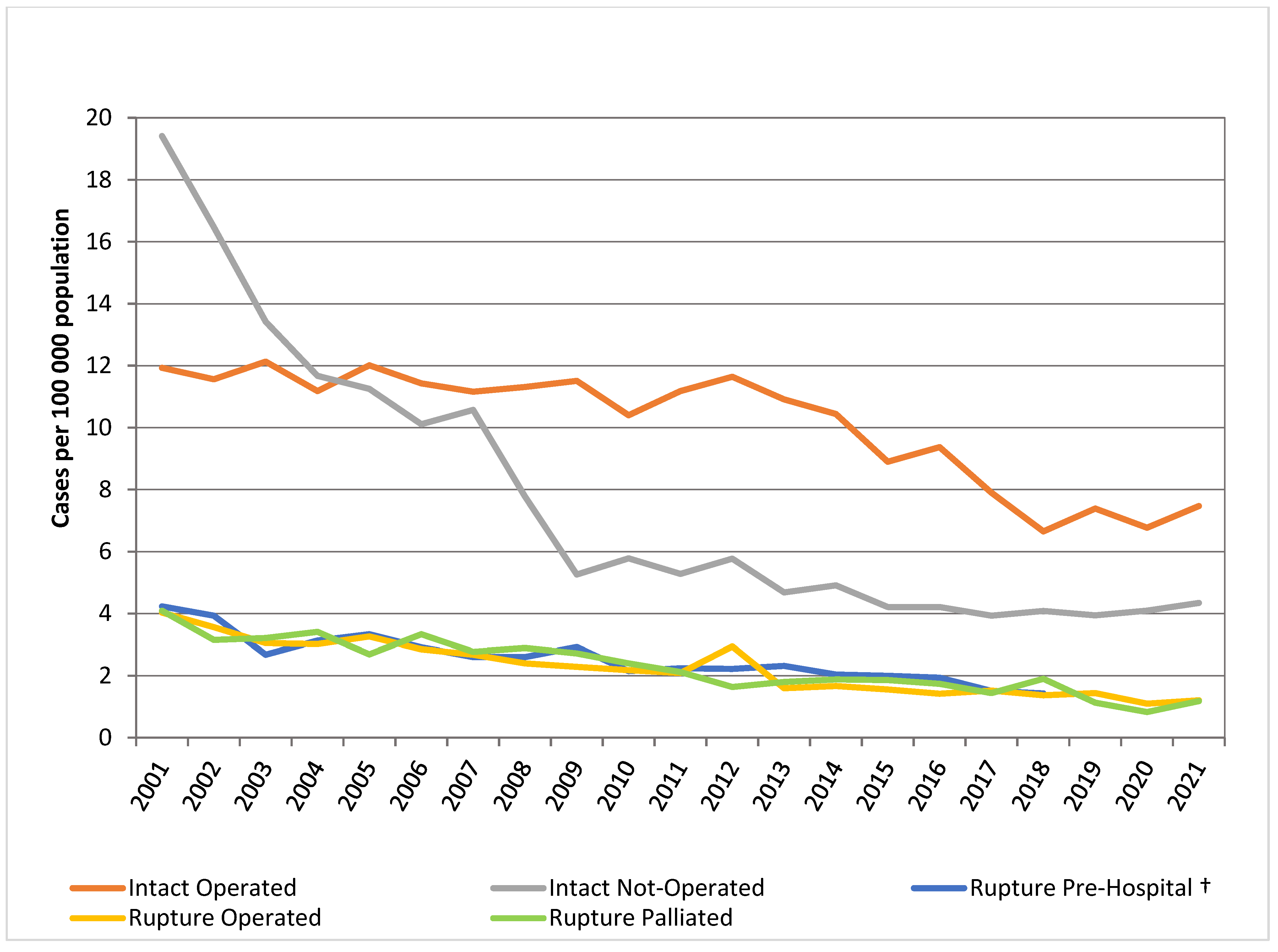
3.3. Trends of AAA Repair and Presentation
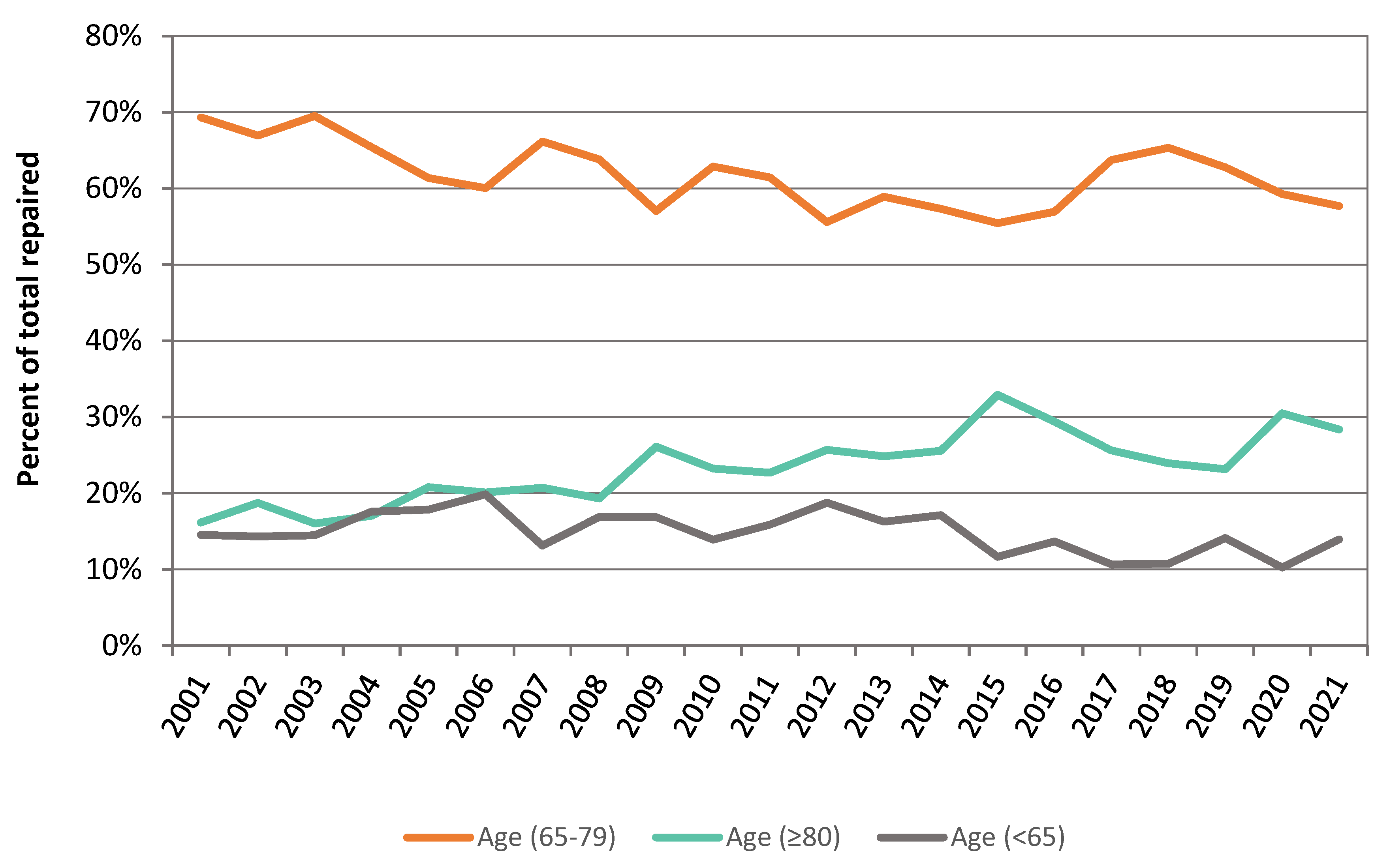
3.4. AAA Repair in Octogenarians
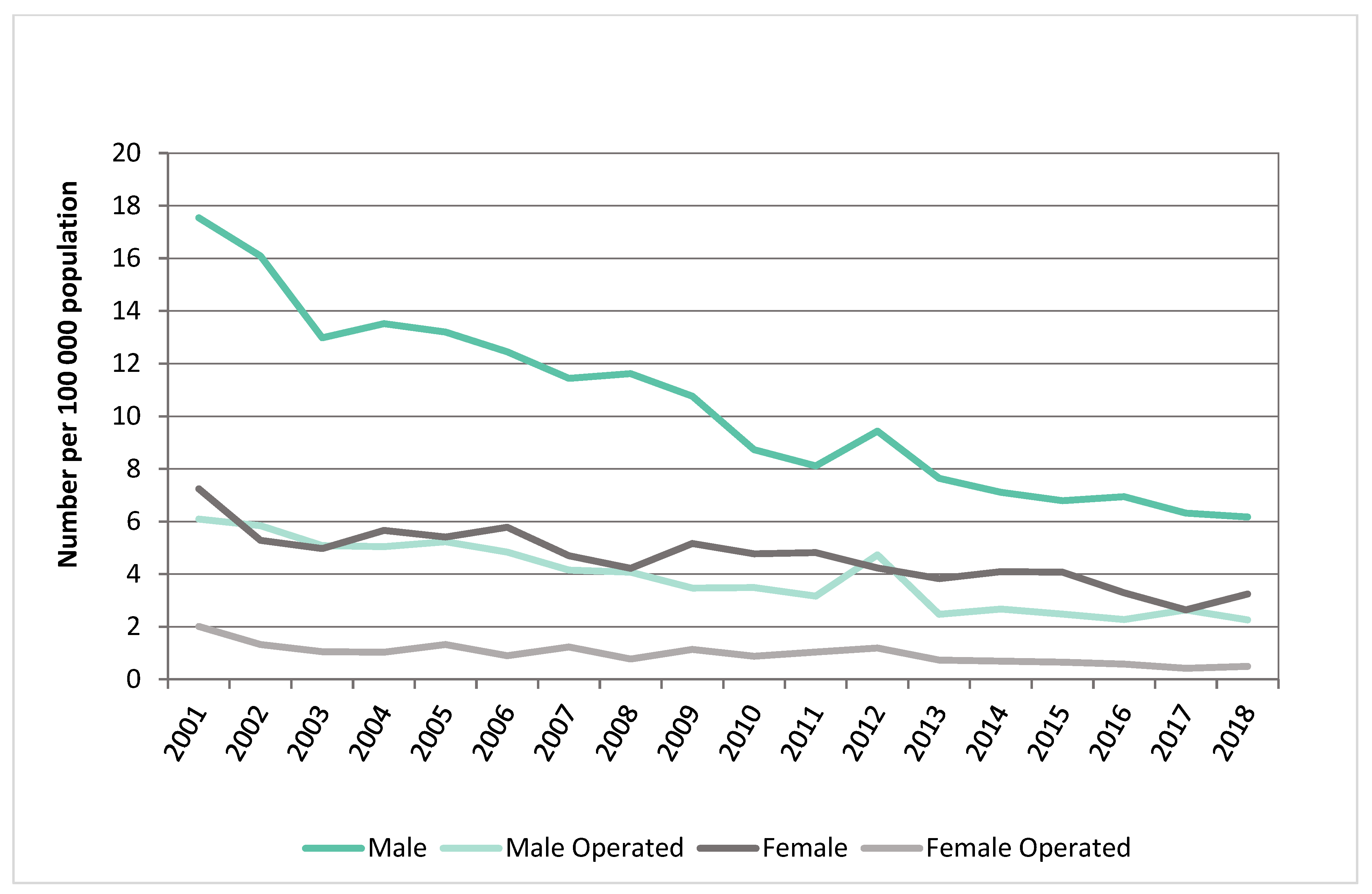
3.5. Incidence of Ruptured AAA Stratified by Sex
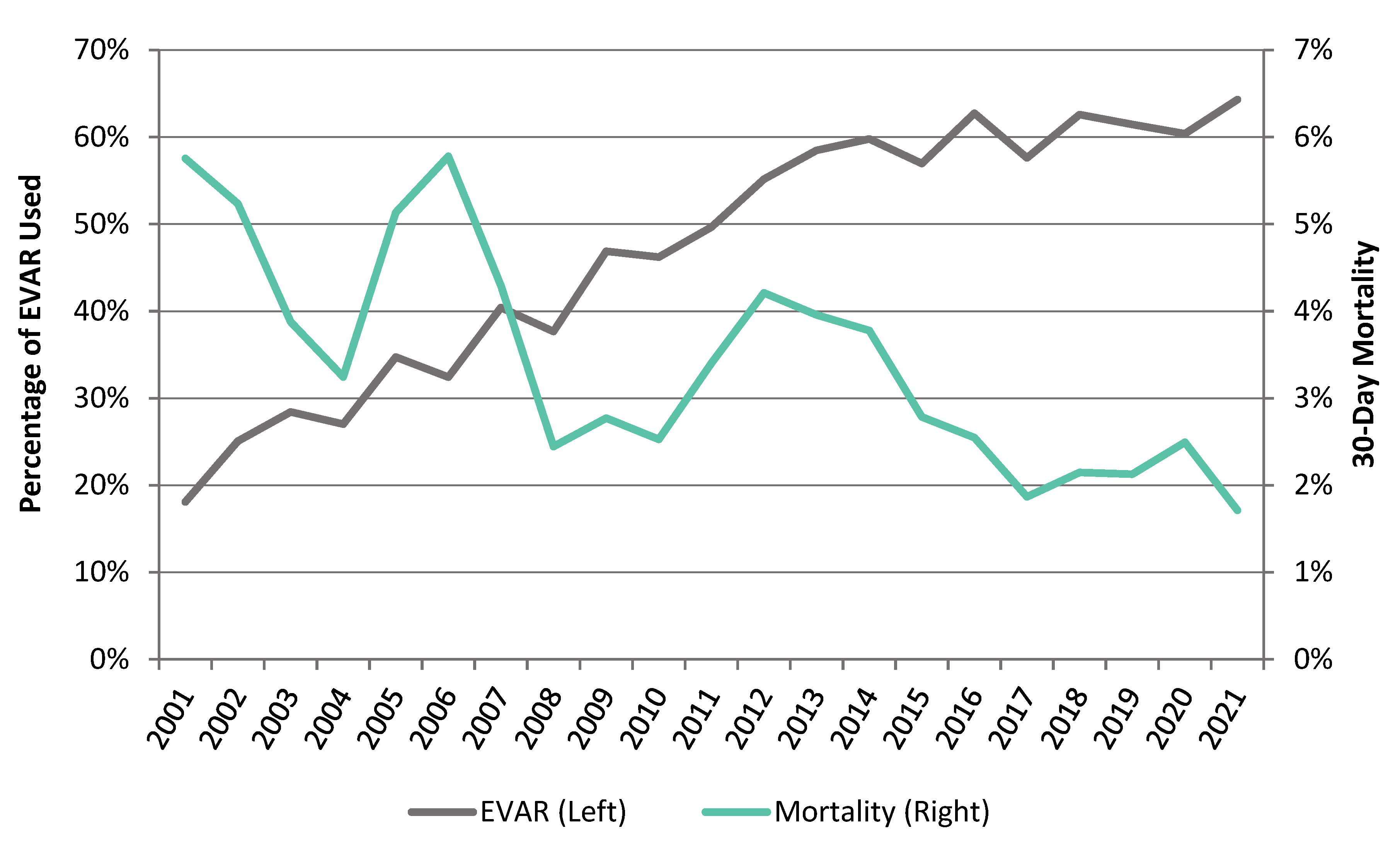
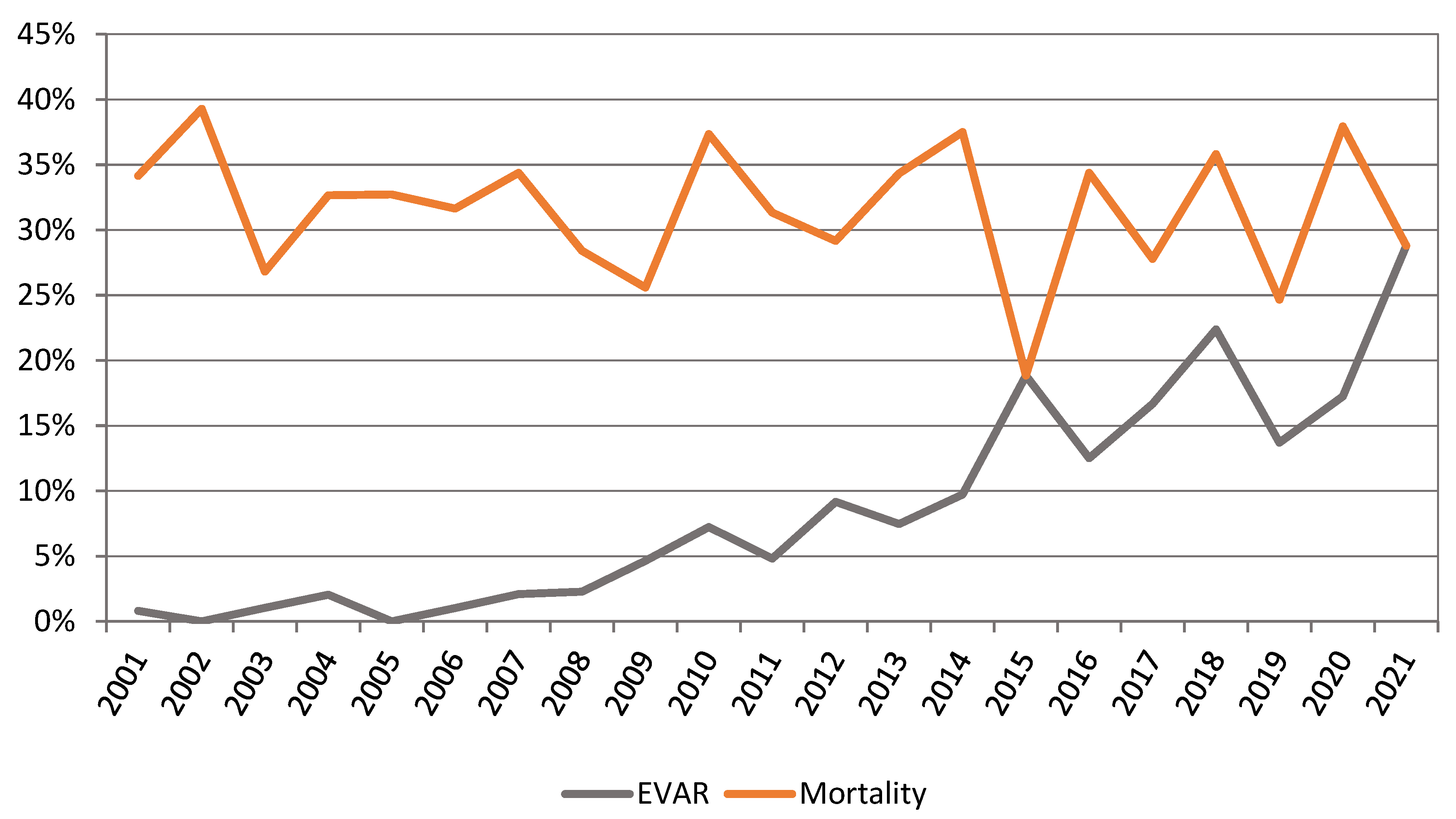
3.6. Methods of AAA Repair and Trends in Operative Mortality
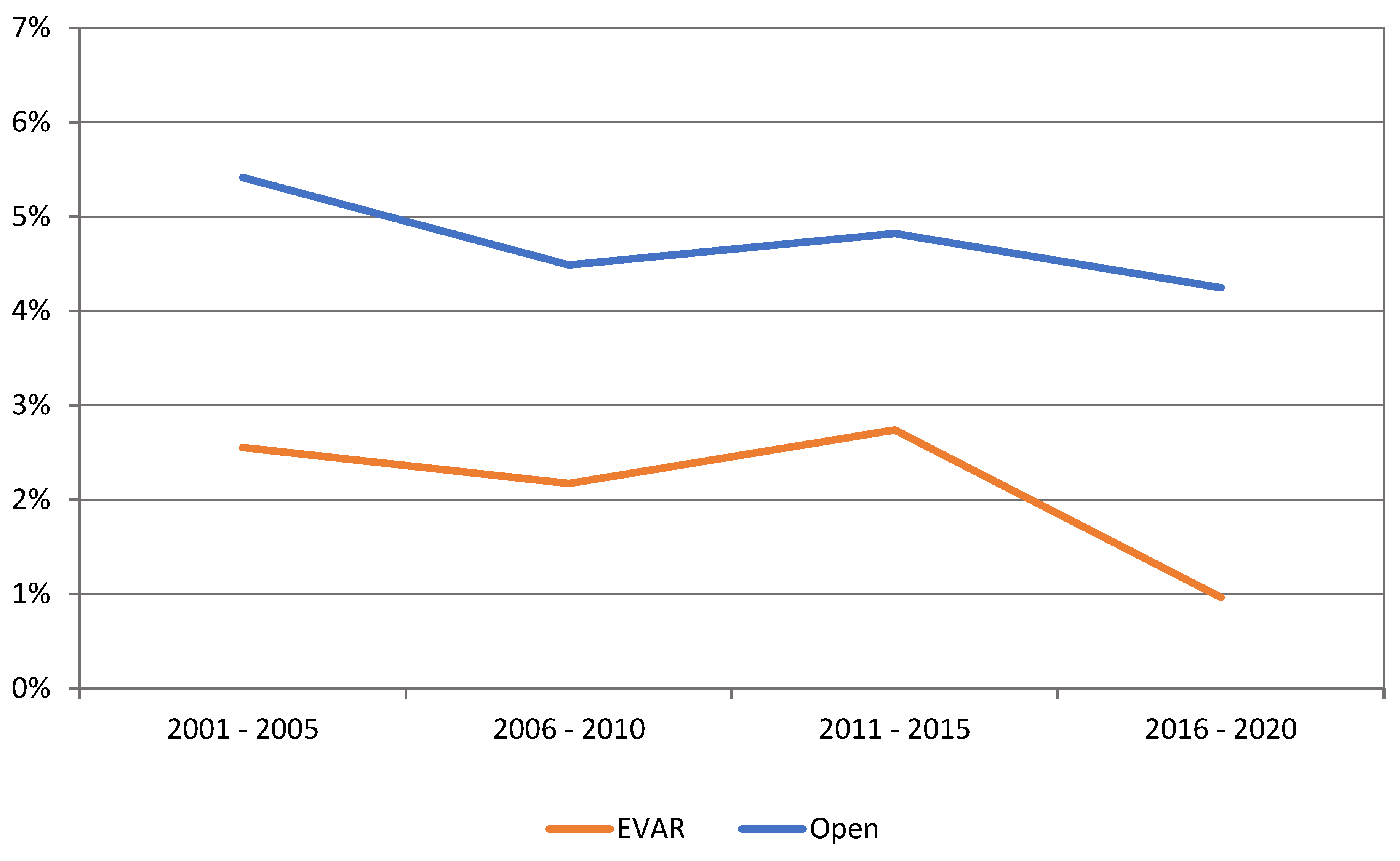
3.7. Effect of Centralisation on Intact AAA Repair
4. Discussion
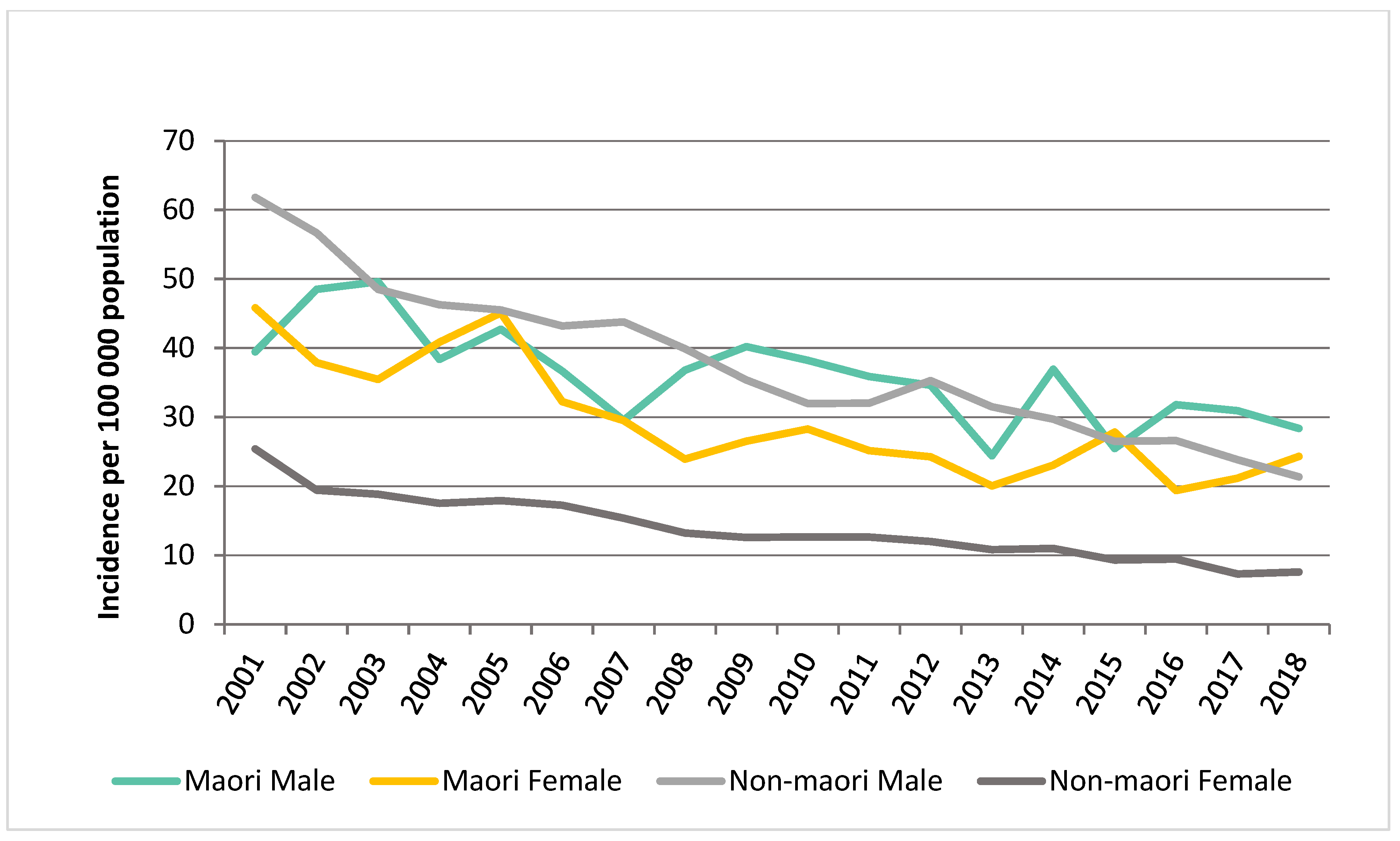
4.1. Incidence of AAA
4.2. Effect of Social Deprivation and Ethnicity on Incidence of AAA
4.3. Mortality and Increase in EVAR Use
4.4. Octogenarians
4.5. Ruptured AAA Outcomes
4.6. Effect of Centralisation of Aortic Pathology in NZ
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 9022800 | Endoluminal repair of aneurysm |
| 3318100 | Repair of ruptured intra-abdominal aneurysm |
| 3316300 | Replacement of ruptured iliac artery aneurysm with graft |
| 3316000 | Replacement of ruptured infrarenal abdominal aortic aneurysm with bifurcation graft to femoral arteries |
| 3315700 | Replacement of ruptured infrarenal aortic aneurysm with bifurcation graft to iliac arteries |
| 3315400 | Replacement of ruptured infrarenal abdominal aortic aneurysm with tube graft |
| 3315100 | Replacement of ruptured suprarenal abdominal aortic aneurysm with graft |
| 3314800 | Replacement of ruptured thoraco-abdominal aneurysm with graft |
| 3312700 | Replacement of iliac artery aneurysm with graft, bilateral |
| 3312400 | Replacement of iliac artery aneurysm with graft, unilateral |
| 3312100 | Replacement of infrarenal abdominal aortic aneurysm with bifurcation graft to femoral arteries |
| 3311800 | Replacement of infrarenal abdominal aortic aneurysm with bifurcation graft to iliac arteries |
| 3311500 | Replacement of infrarenal abdominal aortic aneurysm with tube graft |
| 3311200 | Replacement of suprarenal abdominal aorta aneurysm with graft |
| 3310900 | Replacement of thoraco-abdominal aneurysm with graft |
| 3308000 | Repair of intra-abdominal aneurysm |
| 3311600 | Endovascular repair of aneurysm |
References
- Sampson, U.K.; Norman, P.E.; Fowkes, F.G.; Aboyans, V.; Song, Y.; Harrell, F.E., Jr.; Forouzanfar, M.H.; Naghavi, M.; Denenberg, J.O.; McDermott, M.M.; et al. Estimation of global and regional incidence and prevalence of abdominal aortic aneurysms 1990 to 2010. Glob. Heart 2014, 9, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Boyle, J.R.; Mao, J.; Beck, A.W.; Venermo, M.; Sedrakyan, A.; Behrendt, C.-A.; Szeberin, Z.; Eldrup, N.; Schermerhorn, M.; Beiles, B.; et al. Editor’s Choice–Variation in Intact Abdominal Aortic Aneurysm Repair Outcomes by Country: Analysis of International Consortium of Vascular Registries 2010–2016. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Nair, N.; Kvizhinadze, G.; Jones, G.T.; Rush, R.; Khashram, M.; Roake, J.; Blakely, A. Health gains, costs and cost-effectiveness of a population-based screening programme for abdominal aortic aneurysms. Br. J. Surg. 2019, 106, 1043–1054. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, M.J.; Marshall, J.; Glover, M.; Nasim, A.; Bown, M.J. Evaluating the Cost-Effectiveness of Changes to the Surveillance Intervals in the UK Abdominal Aortic Aneurysm Screening Programme. Value Health 2021, 24, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Hultgren, R.; Linné, A.; Holst, J.; Gottsäter, A.; Langenskiöld, M.; Smidfelt, K.; Björck, M.; Svensjö, S. Outcome of the Swedish Nationwide Abdominal Aortic Aneurysm Screening Program. Circulation 2016, 134, 1141–1148. [Google Scholar] [CrossRef]
- Sandiford, P.; Mosquera, D.; Bramley, D. Trends in incidence and mortality from abdominal aortic aneurysm in New Zealand. Br. J. Surg. 2011, 98, 645–651. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Beiles, C.B.; Bourke, B.M. Validation of Australian data in the Australasian Vascular Audit. ANZ J. Surg. 2014, 84, 624–627. [Google Scholar] [CrossRef]
- Khashram, M.; Thomson, I.A.; Jones, G.T.; Roake, J.A. Abdominal aortic aneurysm repair in New Zealand: A validation of the Australasian Vascular Audit. ANZ J. Surg. 2017, 87, 394–398. [Google Scholar] [CrossRef] [Green Version]
- Bernau, O.; Gormley, S.; Khashram, M. Validation of New Zealand Data in the Australasian Vascular Audit. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 771–772. [Google Scholar] [CrossRef]
- Khashram, M.; Pitama, S.; Williman, J.A.; Jones, G.T.; Roake, J.A. Survival Disparity Following Abdominal Aortic Aneurysm Repair Highlights Inequality in Ethnic and Socio-economic Status. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Salmond, C.; Crampton, P.; King, P.; Waldegrave, C. NZiDep: A New Zealand index of socioeconomic deprivation for individuals. Soc. Sci. Med. 2006, 62, 1474–1485. [Google Scholar] [CrossRef]
- Jeffreys, M.; Sarfati, D.; Stevanovic, V.; Tobias, M.; Lewis, C.; Pearce, N.; Blakely, T. Socioeconomic inequalities in cancer survival in New Zealand: The role of extent of disease at diagnosis. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 915–921. [Google Scholar] [CrossRef] [Green Version]
- Robson, B.; Purdie, G.; Cram, F.; Simmonds, S. Age standardisation—An indigenous standard? Emerg. Themes Epidemiol. 2007, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Team R.C. A language and environment for statistical computing. R Foundation for Statistical Computing: Vienna, Austria, 2015. Available online: http://www.R-project.org (accessed on 6 September 2022).
- Sandiford, P.; Mosquera, D.; Bramley, D. Ethnic inequalities in incidence, survival and mortality from abdominal aortic aneurysm in New Zealand. J. Epidemiol. Community Health 2012, 66, 1097–1103. [Google Scholar] [CrossRef]
- Eickhoff, J.H. Incidence of diagnosis, operation and death from abdominal aortic aneurysms in Danish hospitals: Results from a nation-wide survey, 1977–1990. Eur. J. Surg. Acta Chir. 1993, 159, 619–623. [Google Scholar]
- Singh, K.; Bønaa, K.H.; Jacobsen, B.K.; Bjørk, L.; Solberg, S. Prevalence of and Risk Factors for Abdominal Aortic Aneurysms in a Population-based Study: The Tromsø Study. Am. J. Epidemiol. 2001, 154, 236–244. [Google Scholar] [CrossRef]
- Norman, P.E.; Spilsbury, K.; Semmens, J.B. Falling rates of hospitalization and mortality from abdominal aortic aneurysms in Australia. J. Vasc. Surg. 2011, 53, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Lilja, F.; Mani, K.; Wanhainen, A. Editor’s Choice—Trend-break in Abdominal Aortic Aneurysm Repair With Decreasing Surgical Workload. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Hanna, L.; Sounderajah, V.; Abdullah, A.A.; Marshall, D.C.; Salciccioli, J.D.; Shalhoub, J.; Gibbs, R.G.J. Trends in Thoracic Aortic Aneurysm Hospital Admissions, Interventions, and Mortality in England between 1998 and 2020: An Observational Study. Eur. J. Vasc. Endovasc. Surg. 2022, 64, 340–348. [Google Scholar] [CrossRef]
- Han, Y.; Zhang, S.; Zhang, J.; Ji, C.; Eckstein, H.H. Outcomes of Endovascular Abdominal Aortic Aneurysm Repair in Octogenarians: Meta-analysis and Systematic Review. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 454–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khashram, M.; Jones, G.T.; Roake, J.A. Prevalence of abdominal aortic aneurysm (AAA) in a population undergoing computed tomography colonography in Canterbury, New Zealand. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 199–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karthikesalingam, A.; Holt, P.J.; Vidal-Diez, A.; Bahia, S.S.; Patterson, B.O.; Hinchliffe, R.J.; Thompson, M.M. The impact of endovascular aneurysm repair on mortality for elective abdominal aortic aneurysm repair in England and the United States. J. Vasc. Surg. 2016, 64, 321–327.e2. [Google Scholar] [CrossRef] [PubMed]
- Choke, E.; Vijaynagar, B.; Thompson, J.; Nasim, A.; Bown, M.J.; Sayers, R.D. Changing epidemiology of abdominal aortic aneurysms in England and Wales: Older and more benign? Circulation 2012, 125, 1617–1625. [Google Scholar] [CrossRef] [Green Version]
- Sidloff, D.; Stather, P.; Dattani, N.; Bown, M.; Thompson, J.; Sayers, R.; Choke, E. Aneurysm global epidemiology study: Public health measures can further reduce abdominal aortic aneurysm mortality. Circulation 2014, 129, 747–753. [Google Scholar] [CrossRef] [Green Version]
- Mani, K.; Venermo, M.; Beiles, B.; Menyhei, G.; Altreuther, M.; Loftus, I.; Björck, M. Regional Differences in Case Mix and Peri-operative Outcome After Elective Abdominal Aortic Aneurysm Repair in the Vascunet Database. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 646–652. [Google Scholar] [CrossRef] [Green Version]
- Kobeissi, E.; Hibino, M.; Pan, H.; Aune, D. Blood pressure, hypertension and the risk of abdominal aortic aneurysms: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 2019, 34, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Wang, Z.; Shen, Z.; Lei, F.; Liu, Y.-M.; Chen, Z.; Qin, J.-J.; Liu, H.; Ji, Y.-X.; Zhang, P.; et al. Projection of global burden and risk factors for aortic aneurysm—Timely warning for greater emphasis on managing blood pressure. Ann. Med. 2022, 54, 553–564. [Google Scholar] [CrossRef]
- Roosendaal, L.C.; Kramer, G.M.; Wiersema, A.M.; Wisselink, W.; Jongkind, V. Outcome of Ruptured Abdominal Aortic Aneurysm Repair in Octogenarians: A Systematic Review and Meta-Analysis. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Park, B.D.; Azefor, N.M.; Huang, C.C.; Ricotta, J.J. Elective endovascular aneurysm repair in the elderly: Trends and outcomes from the Nationwide Inpatient Sample. Ann. Vasc. Surg. 2014, 28, 798–807. [Google Scholar] [CrossRef]
- Sweeting, M.J.; Ulug, P.; Powell, J.T.; Desgranges, P.; Balm, R. Ruptured Aneurysm Trials: The Importance of Longer-term Outcomes and Meta-analysis for 1-year Mortality. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 297–302. [Google Scholar] [CrossRef] [Green Version]
- Roosendaal, L.C.; Wiersema, A.M.; Yeung, K.K.; Ünlü, Ç.; Metz, R.; Wisselink, W.; Jongkind, V. Survival and Living Situation After Ruptured Abdominal Aneurysm Repair in Octogenarians. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 375–381. [Google Scholar] [CrossRef]
- Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [CrossRef] [Green Version]
- Visser, P.; Akkersdijk, G.J.; Blankensteijn, J.D. In-hospital operative mortality of ruptured abdominal aortic aneurysm: A population-based analysis of 5593 patients in The Netherlands over a 10-year period. Eur. J. Vasc. Endovasc. Surg. 2005, 30, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Bown, M.J.; Sutton, A.J.; Bell, P.R.; Sayers, R.D. A meta-analysis of 50 years of ruptured abdominal aortic aneurysm repair. Br. J. Surg. 2002, 89, 714–730. [Google Scholar] [CrossRef]
- Larzon, T.; Lindgren, R.; Norgren, L. Endovascular treatment of ruptured abdominal aortic aneurysms: A shift of the paradigm? J. Endovasc. Ther. 2005, 12, 548–555. [Google Scholar] [CrossRef]
- Holt, P.J.; Poloniecki, J.D.; Gerrard, D.; Loftus, I.M.; Thompson, M.M. Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br. J. Surg. 2007, 94, 395–403. [Google Scholar] [CrossRef]
- Giles, K.A.; Hamdan, A.D.; Pomposelli, F.B.; Wyers, M.C.; Dahlberg, S.E.; Schermerhorn, M.L. Population-based outcomes following endovascular and open repair of ruptured abdominal aortic aneurysms. J. Endovasc. Ther. 2009, 16, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Young, E.L.; Holt, P.J.; Poloniecki, J.D.; Loftus, I.M.; Thompson, M.M. Meta-analysis and systematic review of the relationship between surgeon annual caseload and mortality for elective open abdominal aortic aneurysm repairs. J. Vasc. Surg. 2007, 46, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Loftus, I.M.; Boyle, J.R. A Decade of Centralisation of Vascular Services in the UK. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 315–316. [Google Scholar] [CrossRef]
- Mohan, I.V.; Khashram, M.; Fitridge, R. Vascular Surgery in Australia and New Zealand (Australasia). Eur. J. Vasc. Endovasc. Surg. 2021, 62, 338–339. [Google Scholar] [CrossRef] [PubMed]









| Intact (n = 14,436) | Ruptured (n = 5000) | |||||
|---|---|---|---|---|---|---|
| Male | Female | p-Value | Male | Female | p-Value | |
| Number | 10,336 | 4100 | 3324 | 1676 | ||
| Age, mean (SD) | 74.5 | 76.8 | <0.001 | 76.5 | 80.6 | <0.001 |
| Ethnicity | ||||||
| NZ/Other European | 8794 (85.1%) | 3319 (81%) | <0.001 | 2853 (85.8%) | 1402 (83.7%) | <0.001 |
| Māori | 614 (5.9%) | 480 (11.7%) | 232 (7.0%) | 176 (10.5%) | ||
| Pacific | 240 (2.3%) | 84 (2.0%) | 75 (2.3%) | 40 (2.4%) | ||
| Asian, African, Hispanic | 295 (2.9%) | 100 (2.4%) | 80 (2.4%) | 40 (2.4%) | ||
| Not specified | 393 (3.8%) | 117 (2.9%) | 84 (2.5%) | 18 (1.1%) | ||
| Deprivation index | ||||||
| 1–2 | 1371 (13.3%) | 452 (11%) | <0.001 | 308 (9.3%) | 122 (7.3%) | <0.001 |
| 3–4 | 1687 (16.3%) | 601 (14.7%) | 410 (12.3%) | 199 (11.9%) | ||
| 5–6 | 2129 (20.6%) | 867 (21.1%) | 520 (15.6%) | 235 (14%) | ||
| 7–8 | 2557 (24.7%) | 1060 (25.9%) | 631 (19%) | 304 (18.1%) | ||
| 9–10 | 2349 (22.7%) | 1058 (25.8%) | 665 (20%) | 342 (20.4%) | ||
| Not available | 243 (2.4%) | 62 (1.5%) | 790 (23.8%) | 474 (28.3%) | ||
| Intervention | ||||||
| OAR | 3411 (33%) | 1028 (25.1%) | <0.001 | 1190 (35.8%) | 321 (19.2%) | <0.001 |
| EVAR | 3150 (30.5%) | 832 (20.3%) | 76 (2.3%) | 18 (1.1%) | ||
| Not operated | 3775 (36.5%) | 2240 (54.6%) | <0.001 | 2058 (61.9%) | 1337 (79.8%) | <0.001 |
| Category | Cases | Crude Overall Incidence (95% CI) |
|---|---|---|
| Gender | ||
| Female | 5905 | 12.44 (12.13–12.76) |
| Male | 13929 | 30.34 (29.84–30.85) |
| Age Group | ||
| 44 Years and Under | 300 | 0.04 (0.04–0.05) |
| 45–49 Years | 210 | 0.27 (0.23–0.31) |
| 50–54 Years | 432 | 0.59 (0.53–0.64) |
| 55–59 Years | 1016 | 1.52 (1.43–1.62) |
| 60–64 Years | 2424 | 4.22 (4.06–4.39) |
| 65–69 Years | 4530 | 9.49 (9.22–9.77) |
| 70–74 Years | 7038 | 18.44 (18.01–18.88) |
| 75–79 Years | 8788 | 30.46 (29.38–31.1) |
| 80–84 Years | 8024 | 39.8 (38.93–40.68) |
| 85–89 Years | 4780 | 40.98 (39.83–42.16) |
| 90 Years and Over | 2126 | 35.66 (34.16–37.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gormley, S.; Bernau, O.; Xu, W.; Sandiford, P.; Khashram, M. Incidence and Outcomes of Abdominal Aortic Aneurysm Repair in New Zealand from 2001 to 2021. J. Clin. Med. 2023, 12, 2331. https://doi.org/10.3390/jcm12062331
Gormley S, Bernau O, Xu W, Sandiford P, Khashram M. Incidence and Outcomes of Abdominal Aortic Aneurysm Repair in New Zealand from 2001 to 2021. Journal of Clinical Medicine. 2023; 12(6):2331. https://doi.org/10.3390/jcm12062331
Chicago/Turabian StyleGormley, Sinead, Oliver Bernau, William Xu, Peter Sandiford, and Manar Khashram. 2023. "Incidence and Outcomes of Abdominal Aortic Aneurysm Repair in New Zealand from 2001 to 2021" Journal of Clinical Medicine 12, no. 6: 2331. https://doi.org/10.3390/jcm12062331