
Three-Dimensional Characterization of Aortic Root Motion by Vascular Deformation Mapping

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. VDM(D)
2.3. Metrics Extracted from VDM(D)
2.3.1. Defining a Suitable Location to Study Aortic Root Motion
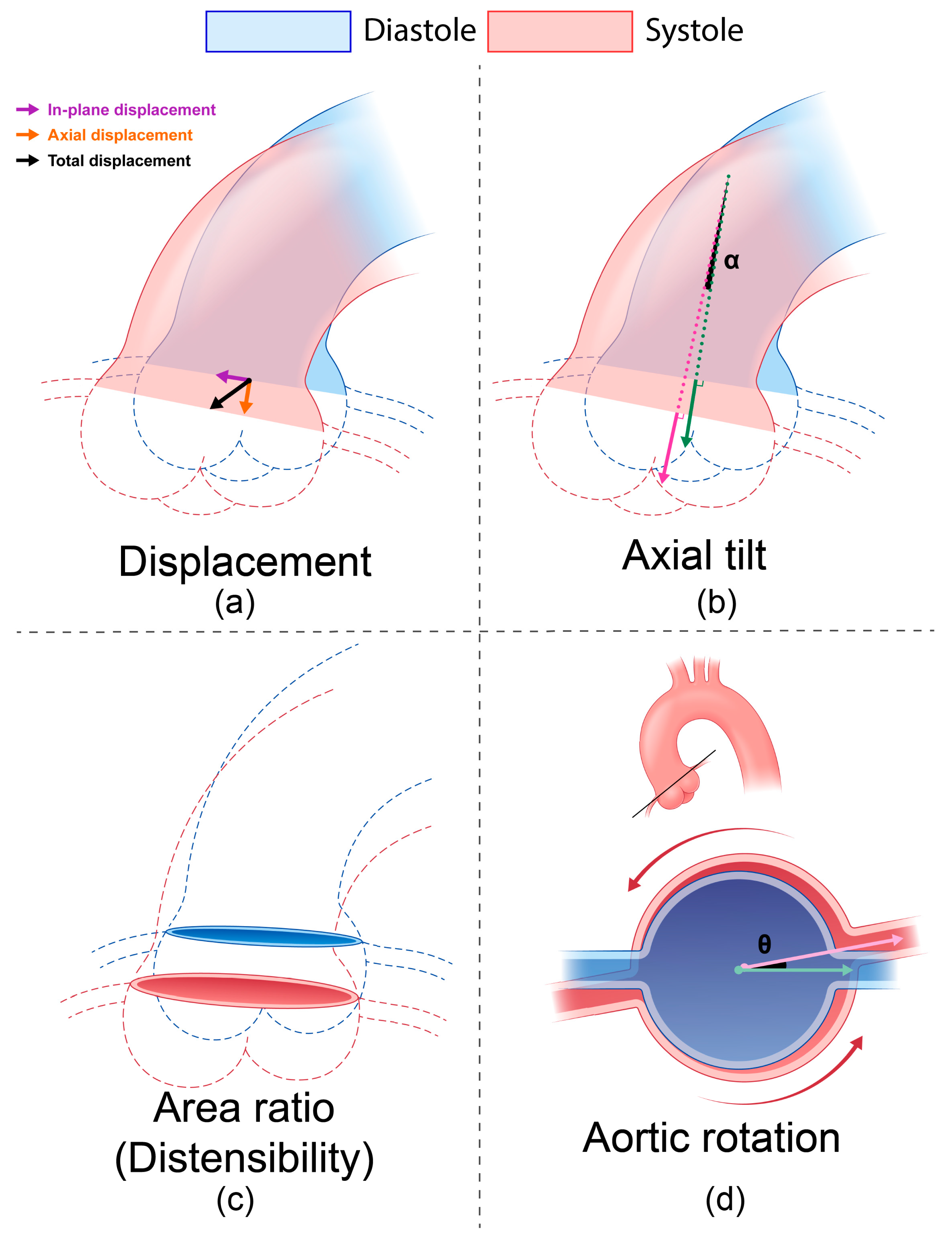
2.3.2. Displacement
2.3.3. Distensibility and Area Ratio
2.3.4. Axial Tilt and Aortic Rotation
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
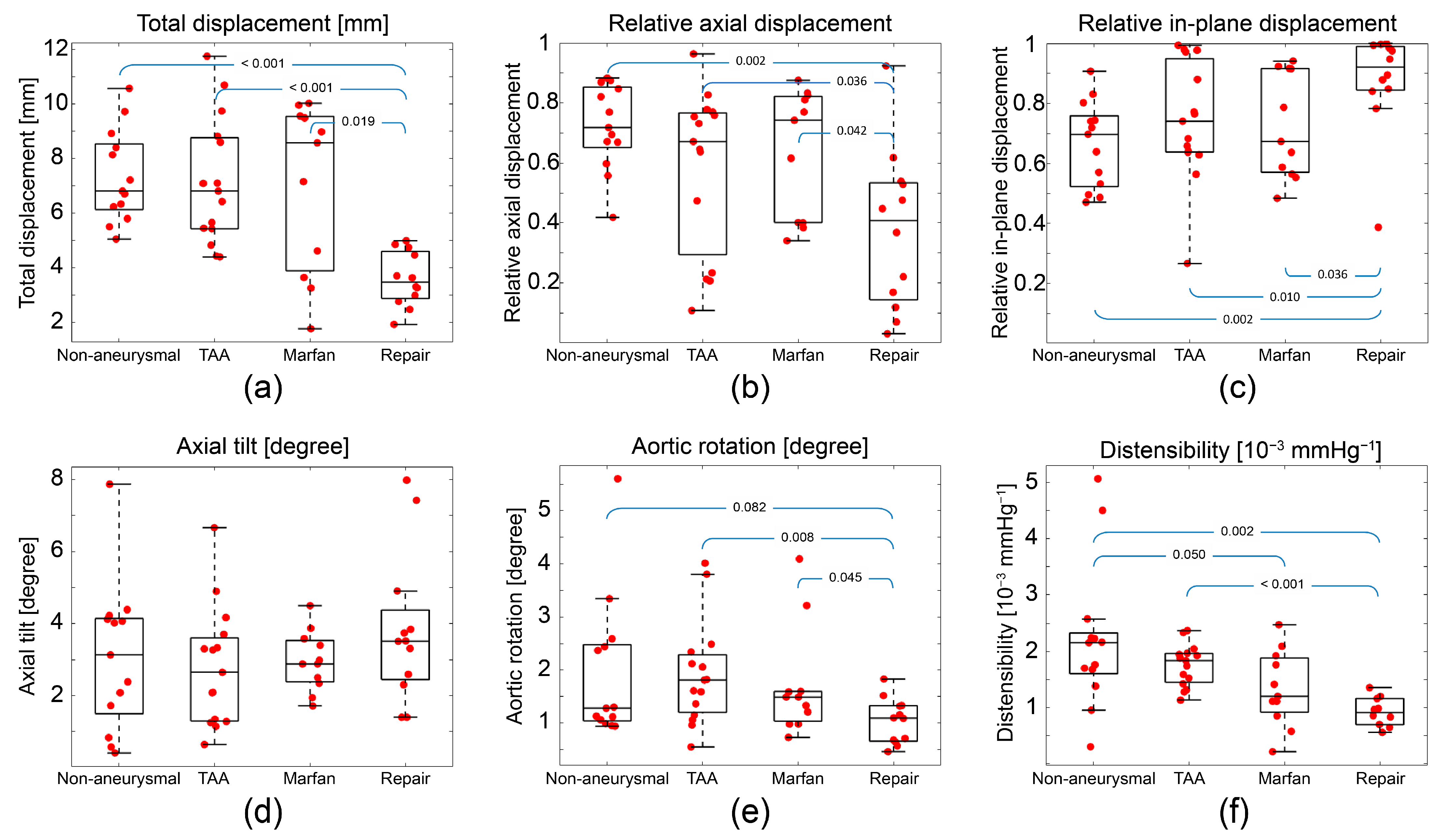
3.2. Aortic Root Motion Metrics
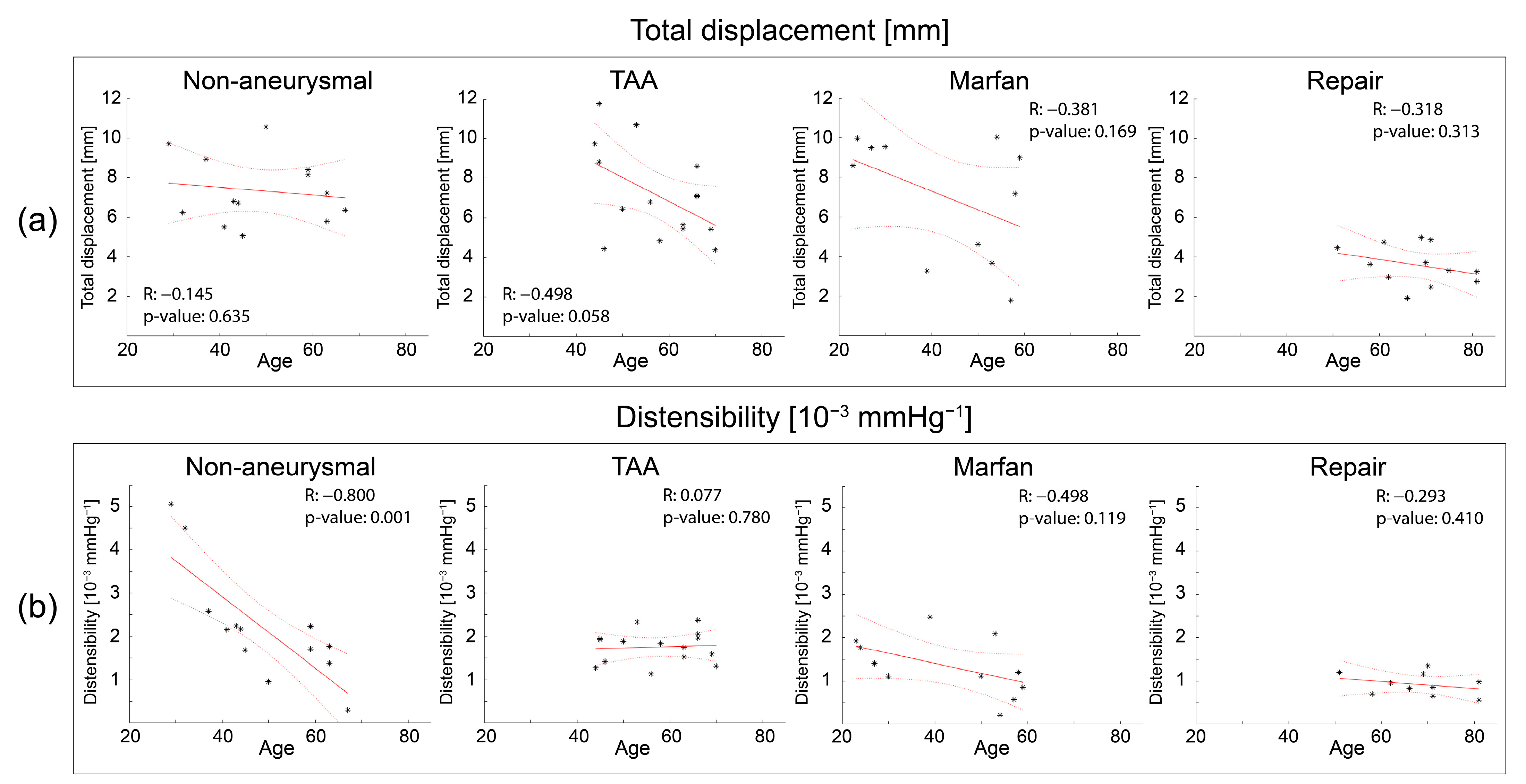
3.3. Correlation with Age
3.4. LV/Ao Angle Results
4. Discussion
4.1. Displacement Extraction Comparison between 2D and 3D
4.2. Implications for Aortic Wall Stress Analysis
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Chau, K.H.; Elefteriades, J.A. Natural history of thoracic aortic aneurysms: Size matters, plus moving beyond size. Prog. Cardiovasc. Dis. 2013, 56, 74–80. [Google Scholar] [CrossRef]
- Elefteriades, J.A.; Farkas, E.A. Thoracic aortic aneurysm: Clinically pertinent controversies and uncertainties. J. Am. Coll. Cardiol. 2010, 55, 841–857. [Google Scholar] [CrossRef] [PubMed]
- Freeman, L.A.; Young, P.M.; Foley, T.A.; Williamson, E.E.; Bruce, C.J.; Greason, K.L. CT and MRI assessment of the aortic root and ascending aorta. Am. J. Roentgenol. 2013, 200, W581–W592. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, B.; Kazerooni, E.A. ECG-gated cardiac CT. Am. J. Roentgenol. 2004, 182, 993–1010. [Google Scholar] [CrossRef] [PubMed]
- Beller, C.J.; Labrosse, M.R.; Thubrikar, M.J.; Robicsek, F. Role of aortic root motion in the pathogenesis of aortic dissection. Circulation 2004, 109, 763–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutugno, S.; Agnese, V.; Gentile, G.; Raffa, G.M.; Wisneski, A.D.; Guccione, J.M.; Pilato, M.; Pasta, S. Patient-specific analysis of ascending thoracic aortic aneurysm with the living heart human model. Bioengineering 2021, 8, 175. [Google Scholar] [CrossRef]
- Singh, S.; Xu, X.; Pepper, J.; Izgi, C.; Treasure, T.; Mohiaddin, R. Effects of aortic root motion on wall stress in the Marfan aorta before and after personalised aortic root support (PEARS) surgery. J. Biomech. 2016, 49, 2076–2084. [Google Scholar] [CrossRef]
- Wei, W.; Evin, M.; Rapacchi, S.; Kober, F.; Bernard, M.; Jacquier, A.; Kahn, C.J.; Behr, M. Investigating heartbeat-related in-plane motion and stress levels induced at the aortic root. BioMedical Eng. OnLine 2019, 18, 1–15. [Google Scholar] [CrossRef]
- Kozerke, S.; Scheidegger, M.B.; Pedersen, E.M.; Boesiger, P. Heart motion adapted cine phase-contrast flow measurements through the aortic valve. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 1999, 42, 970–978. [Google Scholar] [CrossRef]
- Burris, N.S.; Bian, Z.; Dominic, J.; Zhong, J.; Houben, I.B.; van Bakel, T.M.; Patel, H.J.; Ross, B.D.; Christensen, G.E.; Hatt, C.R. Vascular deformation mapping for CT surveillance of thoracic aortic aneurysm growth. Radiology 2022, 302, 218–225. [Google Scholar] [CrossRef]
- Burris, N.S.; Hoff, B.A.; Kazerooni, E.A.; Ross, B.D. Vascular deformation mapping (VDM) of thoracic aortic enlargement in aneurysmal disease and dissection. Tomography 2017, 3, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Burris, N.S.; Hoff, B.A.; Patel, H.J.; Kazerooni, E.A.; Ross, B.D. Three-dimensional growth analysis of thoracic aortic aneurysm with vascular deformation mapping. Circ. Cardiovasc. Imaging 2018, 11, e008045. [Google Scholar] [CrossRef] [Green Version]
- Rosset, A.; Spadola, L.; Ratib, O.J. OsiriX: An open-source software for navigating in multidimensional DICOM images. J. Digit. Imaging 2004, 17, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Zhong, J.; Bian, Z.; Hatt, C.R.; Burris, N.S. Segmentation of the thoracic aorta using an attention-gated u-net. In Proceedings of the Medical Imaging 2021: Computer-Aided Diagnosis, Online, 15–20 February 2021; pp. 147–153. [Google Scholar]
- Groenink, M.; de Roos, A.; Mulder, B.J.; Spaan, J.A.; van der Wall, E.E. Changes in aortic distensibility and pulse wave velocity assessed with magnetic resonance imaging following beta-blocker therapy in the Marfan syndrome. Am. J. Cardiol. 1998, 82, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Kruskal, W.H.; Wallis, W.A. Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Izgi, C.; Nyktari, E.; Alpendurada, F.; Bruengger, A.S.; Pepper, J.; Treasure, T.; Mohiaddin, R. Effect of personalized external aortic root support on aortic root motion and distension in Marfan syndrome patients. Int. J. Cardiol. 2015, 197, 154–160. [Google Scholar] [CrossRef]
- De Beaufort, H.W.; Conti, M.; Kamman, A.V.; Nauta, F.J.; Lanzarone, E.; Moll, F.L.; Van Herwaarden, J.A.; Auricchio, F.; Trimarchi, S. Stent-graft deployment increases aortic stiffness in an ex vivo porcine model. Ann. Vasc. Surg. 2017, 43, 302–308. [Google Scholar] [CrossRef]
- Takeda, Y.; Sakata, Y.; Ohtani, T.; Tamaki, S.; Omori, Y.; Tsukamoto, Y.; Aizawa, Y.; Shimamura, K.; Shirakawa, Y.; Kuratani, T. Endovascular aortic repair increases vascular stiffness and alters cardiac structure and function. Circ. J. 2014, 78, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, C.; Stergiopulos, N.; Katsamouris, A.; Startchik, I.; Kalangos, A.; Licker, M.; Westerhof, N.; Morel, D. Hemodynamics induced after acute reduction of proximal thoracic aorta compliance. Eur. J. Vasc. Endovasc. Surg. 2003, 26, 195–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, D.; Zigras, T.; Cartier, R.; Leduc, L.; Butany, J.; Mongrain, R.; Leask, R.L. A comparison of mechanical properties of materials used in aortic arch reconstruction. Ann. Thorac. Surg. 2009, 88, 1484–1491. [Google Scholar] [CrossRef]
- Spadaccio, C.; Nappi, F.; Al-Attar, N.; Sutherland, F.W.; Acar, C.; Nenna, A.; Trombetta, M.; Chello, M.; Rainer, A.J. Old myths, new concerns: The long-term effects of ascending aorta replacement with dacron grafts. Not all that glitters is gold. J. Cardiovasc. Transl. Res. 2016, 9, 334–342. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, C.; Matyas, G.; Steinmann, B.; Baumgartner, D. Marfan syndrome—A diagnostic challenge caused by phenotypic and genetic heterogeneity. Methods Inf. Med. 2005, 44, 487–497. [Google Scholar] [PubMed]
- Seo, G.H.; Kim, Y.-M.; Kang, E.; Kim, G.-H.; Seo, E.-J.; Lee, B.H.; Choi, J.-H.; Yoo, H.-W. The phenotypic heterogeneity of patients with Marfan-related disorders and their variant spectrums. Medicine 2018, 97, e10767. [Google Scholar] [CrossRef]
- de Wit, A.; Vis, K.; Jeremy, R.W. Aortic stiffness in heritable aortopathies: Relationship to aneurysm growth rate. Heart Lung Circ. 2013, 22, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Andel, M.M.; de Waard, V.; Timmermans, J.; Scholte, A.J.; van den Berg, M.P.; Zwinderman, A.H.; Mulder, B.J.; Groenink, M. Aortic distensibility in Marfan syndrome: A potential predictor of aortic events? Open Heart 2021, 8, e001775. [Google Scholar] [CrossRef] [PubMed]
- Kolipaka, A.; Illapani, V.S.P.; Kenyhercz, W.; Dowell, J.D.; Go, M.R.; Starr, J.E.; Vaccaro, P.S.; White, R.D. Quantification of abdominal aortic aneurysm stiffness using magnetic resonance elastography and its comparison to aneurysm diameter. J. Vasc. Surg. 2016, 64, 966–974. [Google Scholar] [CrossRef] [Green Version]
- Perissiou, M.; Bailey, T.G.; Windsor, M.; Greaves, K.; Nam, M.C.; Russell, F.D.; O’Donnell, J.; Magee, R.; Jha, P.; Schulze, K.; et al. Aortic and systemic arterial stiffness responses to acute exercise in patients with small abdominal aortic aneurysms. European J. Vasc. Endovasc. Surg. 2019, 58, 708–718. [Google Scholar] [CrossRef]
- van Disseldorp, E.M.; Petterson, N.J.; van de Vosse, F.N.; van Sambeek, M.R.; Lopata, R.G. Quantification of aortic stiffness and wall stress in healthy volunteers and abdominal aortic aneurysm patients using time-resolved 3D ultrasound: A comparison study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 185–191. [Google Scholar] [CrossRef]
- Kwon, D.H.; Smedira, N.G.; Popovic, Z.B.; Lytle, B.W.; Setser, R.; Thamilarasan, M.; Schoenhagen, P.; Flamm, S.D.; Lever, H.M.; Desai, M.Y. Steep left ventricle to aortic root angle and hypertrophic obstructive cardiomyopathy: Study of a novel association using three-dimensional multimodality imaging. Heart 2009, 95, 1784–1791. [Google Scholar] [CrossRef]
- Swinne, C.J.; Shapiro, E.P.; Jamart, J.; Fleg, J.L. Age-associated changes in left ventricular outflow tract geometry in normal subjects. Am. J. Cardiol. 1996, 78, 1070–1073. [Google Scholar] [CrossRef]
- Cuomo, F.; Roccabianca, S.; Dillon-Murphy, D.; Xiao, N.; Humphrey, J.D.; Figueroa, C.A. Effects of age-associated regional changes in aortic stiffness on human hemodynamics revealed by computational modeling. PLoS ONE 2017, 12, e0173177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickson, S.S.; Butlin, M.; Graves, M.; Taviani, V.; Avolio, A.P.; McEniery, C.M.; Wilkinson, I.B. The relationship of age with regional aortic stiffness and diameter. JACC Cardiovasc. Imaging 2010, 3, 1247–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Rourke, M.F.; Nichols, W.W. Aortic diameter, aortic stiffness, and wave reflection increase with age and isolated systolic hypertension. Hypertension 2005, 45, 652–658. [Google Scholar] [CrossRef] [Green Version]
- Cain, P.A.; Ahl, R.; Hedstrom, E.; Ugander, M.; Allansdotter-Johnsson, A.; Friberg, P.; Arheden, H. Age and gender specific normal values of left ventricular mass, volume and function for gradient echo magnetic resonance imaging: A cross sectional study. BMC Med. Imaging 2009, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Port, S.; Cobb, F.R.; Coleman, R.E.; Jones, R.H. Effect of age on the response of the left ventricular ejection fraction to exercise. N. Engl. J. Med. 1980, 303, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Nollen, G.J.; Groenink, M.; Tijssen, J.G.; Van Der Wall, E.E.; Mulder, B.J. Aortic stiffness and diameter predict progressive aortic dilatation in patients with Marfan syndrome. Eur. Heart J. 2004, 25, 1146–1152. [Google Scholar] [CrossRef]
- Vriz, O.; Driussi, C.; Bettio, M.; Ferrara, F.; D’Andrea, A.; Bossone, E. Aortic root dimensions and stiffness in healthy subjects. Am. J. Cardiol. 2013, 112, 1224–1229. [Google Scholar] [CrossRef]
- Duprey, A.; Trabelsi, O.; Vola, M.; Favre, J.-P.; Avril, S. Biaxial rupture properties of ascending thoracic aortic aneurysms. Acta Biomater. 2016, 42, 273–285. [Google Scholar] [CrossRef] [Green Version]
- Pichamuthu, J.E.; Phillippi, J.A.; Cleary, D.A.; Chew, D.W.; Hempel, J.; Vorp, D.A.; Gleason, T.G. Differential tensile strength and collagen composition in ascending aortic aneurysms by aortic valve phenotype. Ann. Thorac. Surg. 2013, 96, 2147–2154. [Google Scholar] [CrossRef] [Green Version]
- Vianna, E.; Kramer, B.; Tarraf, S.; Gillespie, C.; Colbrunn, R.; Bellini, C.; Roselli, E.E.; Cikach, F.; Germano, E.; Emerton, K.; et al. Aortic diameter is a poor predictor of aortic tissue failure metrics in patients with ascending aneurysms. J. Thorac. Cardiovasc. Surg. 2022, in press. [CrossRef]
- Weber, T.F.; Ganten, M.-K.; Böckler, D.; Geisbüsch, P.; Kauczor, H.-U.; von Tengg-Kobligk, H. Heartbeat-related displacement of the thoracic aorta in patients with chronic aortic dissection type B: Quantification by dynamic CTA. Eur. J. Radiol. 2009, 72, 483–488. [Google Scholar] [CrossRef]
- Rengier, F.; Weber, T.F.; Henninger, V.; Böckler, D.; Schumacher, H.; Kauczor, H.-U.; von Tengg-Kobligk, H. Heartbeat-related distension and displacement of the thoracic aorta in healthy volunteers. Eur. J. Radiol. 2012, 81, 158–164. [Google Scholar] [CrossRef]
- Moireau, P.; Xiao, N.; Astorino, M.; Figueroa, C.A.; Chapelle, D.; Taylor, C.A.; Gerbeau, J.-F. External tissue support and fluid–structure simulation in blood flows. Biomech. Model. Mechanobiol. 2012, 11, 1–18. [Google Scholar] [CrossRef]
- Maeda, E.; Ando, Y.; Takeshita, K.; Matsumoto, T. Through the cleared aorta: Three-dimensional characterization of mechanical behaviors of rat thoracic aorta under intraluminal pressurization using optical clearing method. Sci. Rep. 2022, 12, 8632. [Google Scholar] [CrossRef] [PubMed]
- Meierhofer, C.; Schneider, E.P.; Lyko, C.; Hutter, A.; Martinoff, S.; Markl, M.; Hager, A.; Hess, J.; Stern, H.; Fratz, S. Wall shear stress and flow patterns in the ascending aorta in patients with bicuspid aortic valves differ significantly from tricuspid aortic valves: A prospective study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, D.P.; Xu, C.; Plappert, T.; Desjardins, B.; Gorman, J.H., III; Bavaria, J.E.; Gorman, R.C.; Chandran, K.B.; Jackson, B.M. Increased ascending aortic wall stress in patients with bicuspid aortic valves. Ann. Thorac. Surg. 2011, 92, 1384–1389. [Google Scholar] [CrossRef] [Green Version]
- Nathan, D.P.; Xu, C.; Gorman III, J.H.; Fairman, R.M.; Bavaria, J.E.; Gorman, R.C.; Chandran, K.B.; Jackson, B.M. Pathogenesis of acute aortic dissection: A finite element stress analysis. Ann. Thorac. Surg. 2011, 91, 458–463. [Google Scholar] [CrossRef]
- Di Martino, E.S.; Guadagni, G.; Fumero, A.; Ballerini, G.; Spirito, R.; Biglioli, P.; Redaelli, A. Fluid–structure interaction within realistic three-dimensional models of the aneurysmatic aorta as a guidance to assess the risk of rupture of the aneurysm. Med. Eng. Phys. 2001, 23, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Venkatasubramaniam, A.; Fagan, M.; Mehta, T.; Mylankal, K.; Ray, B.; Kuhan, G.; Chetter, I.; McCollum, P. A comparative study of aortic wall stress using finite element analysis for ruptured and non-ruptured abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2004, 28, 168–176. [Google Scholar]
- Martin, C.; Sun, W.; Elefteriades, J. Patient-specific finite element analysis of ascending aorta aneurysms. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H1306–H1316. [Google Scholar] [CrossRef] [Green Version]
- Schwarze, M.L.; Shen, Y.; Hemmerich, J.; Dale, W. Age-related trends in utilization and outcome of open and endovascular repair for abdominal aortic aneurysm in the United States, 2001–2006. J. Vasc. Surg. 2009, 50, 722–729.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic (n = 45) | Non-Aneurysmal (n = 13) | TAA (n = 15) | Marfan (n = 11) | Repair (n = 12) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 48.6 ± 12.5 | 57.3 ± 9.5 | 43.1 ± 14.7 | 68.0 ± 9.0 | <0.01 |
| Female (n) | 6 | 5 | 6 | 2 | - |
| BP (systolic) (mmHg) | 130 ± 22 | 125 ± 19 | 125 ± 17 | 129 ± 11 | 0.86 |
| BP (diastolic) (mmHg) | 77 ± 15 | 68 ± 8 | 69 ± 10 | 71 ± 10 | 0.21 |
| Pulse pressure (mmHg) | 53 ± 12 | 56 ± 19 | 56 ± 14 | 58 ± 16 | 0.86 |
| HTN (n) | 8 | 8 | 7 | 6 | - |
| BAV (n) | 0 | 6 | 1 | 0 | - |
| AS (n) | 0 | 5 | 0 | 0 | - |
| AI (n) | 0 | 3 | 0 | 0 | - |
| CAD (n) | 2 | 2 | 0 | 3 | - |
| Hyperlipidemia (n) | 2 | 7 | 2 | 5 | - |
| Diameter (sinus) (mm) | 32 ± 4 | 43 ± 5 | 43 ± 6 | 36 ± 5 | <0.01 |
| Diameter (STJ) (mm) | 28 ± 3 | 43 ± 5 | 36 ± 6 | 32 ± 3 | <0.01 |
| Diameter (MAA) (mm) | 30 ± 4 | 45 ± 4 | 33 ± 4 | 32 ± 3 | <0.01 |
| LV/Ao angle (degrees) | 132.5 ± 9.5 | 134.4 ± 6.4 | 134.9 ± 7.4 | 126.4 ± 6.4 | <0.01 |
| Non-Aneurysmal | TAA | Marfan | Repair | ||
|---|---|---|---|---|---|
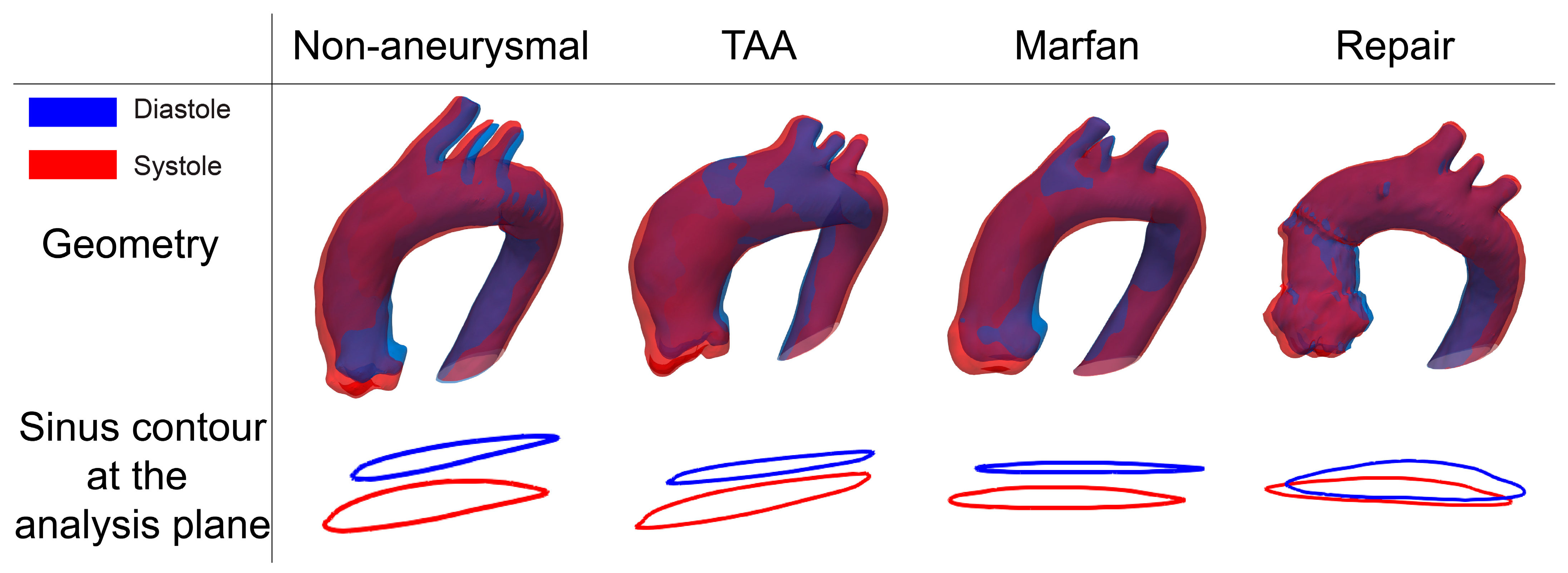
| Sinus contour at the analysis plane (blue= diastolic, red= systolic) |  |  |  |  | |
| Displacement [mm] | Total | 7.34 ± 1.69 | 7.14 ± 2.30 | 7.01 ± 3.09 | 3.60 ± 1.00 |
| Axial | 5.20 ± 1.17 | 4.23 ± 2.27 | 4.84 ± 2.88 | 1.37 ± 1.14 | |
| In-plane | 4.98 ± 1.93 | 5.33 ± 2.32 | 4.79 ± 2.08 | 3.13 ± 1.06 | |
| Relative axial displacement | 0.72 ± 0.14 | 0.58 ± 0.27 | 0.63 ± 0.21 | 0.38 ± 0.26 | |
| Relative in-plane displacement | 0.66 ± 0.14 | 0.68 ± 0.25 | 0.73 ± 0.17 | 0.88 ± 0.17 | |
| Axial tilt (degree) | 3.06 ± 2.06 | 2.79 ± 1.65 | 2.96 ± 0.83 | 3.83 ± 2.08 | |
| Aortic rotation (degree) | 1.93 ± 1.35 | 1.92 ± 0.97 | 1.70 ± 1.02 | 1.03 ± 0.43 | |
| Distensibility (10−3 mmHg−1) | 2.21 ±1.30 | 1.75 ± 0.37 | 1.34 ± 0.68 | 0.93 ± 0.26 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.; Tjahjadi, N.S.; He, X.; van Herwaarden, J.; Patel, H.J.; Burris, N.S.; Figueroa, C.A. Three-Dimensional Characterization of Aortic Root Motion by Vascular Deformation Mapping. J. Clin. Med. 2023, 12, 4471. https://doi.org/10.3390/jcm12134471
Kim T, Tjahjadi NS, He X, van Herwaarden J, Patel HJ, Burris NS, Figueroa CA. Three-Dimensional Characterization of Aortic Root Motion by Vascular Deformation Mapping. Journal of Clinical Medicine. 2023; 12(13):4471. https://doi.org/10.3390/jcm12134471
Chicago/Turabian StyleKim, Taeouk, Nic S. Tjahjadi, Xuehuan He, JA van Herwaarden, Himanshu J. Patel, Nicholas S. Burris, and C. Alberto Figueroa. 2023. "Three-Dimensional Characterization of Aortic Root Motion by Vascular Deformation Mapping" Journal of Clinical Medicine 12, no. 13: 4471. https://doi.org/10.3390/jcm12134471