
Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Clinical Assessments and Data Collection
2.3. Definition of Systemic Inflammatory Markers
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Systemic Inflammatory Markers
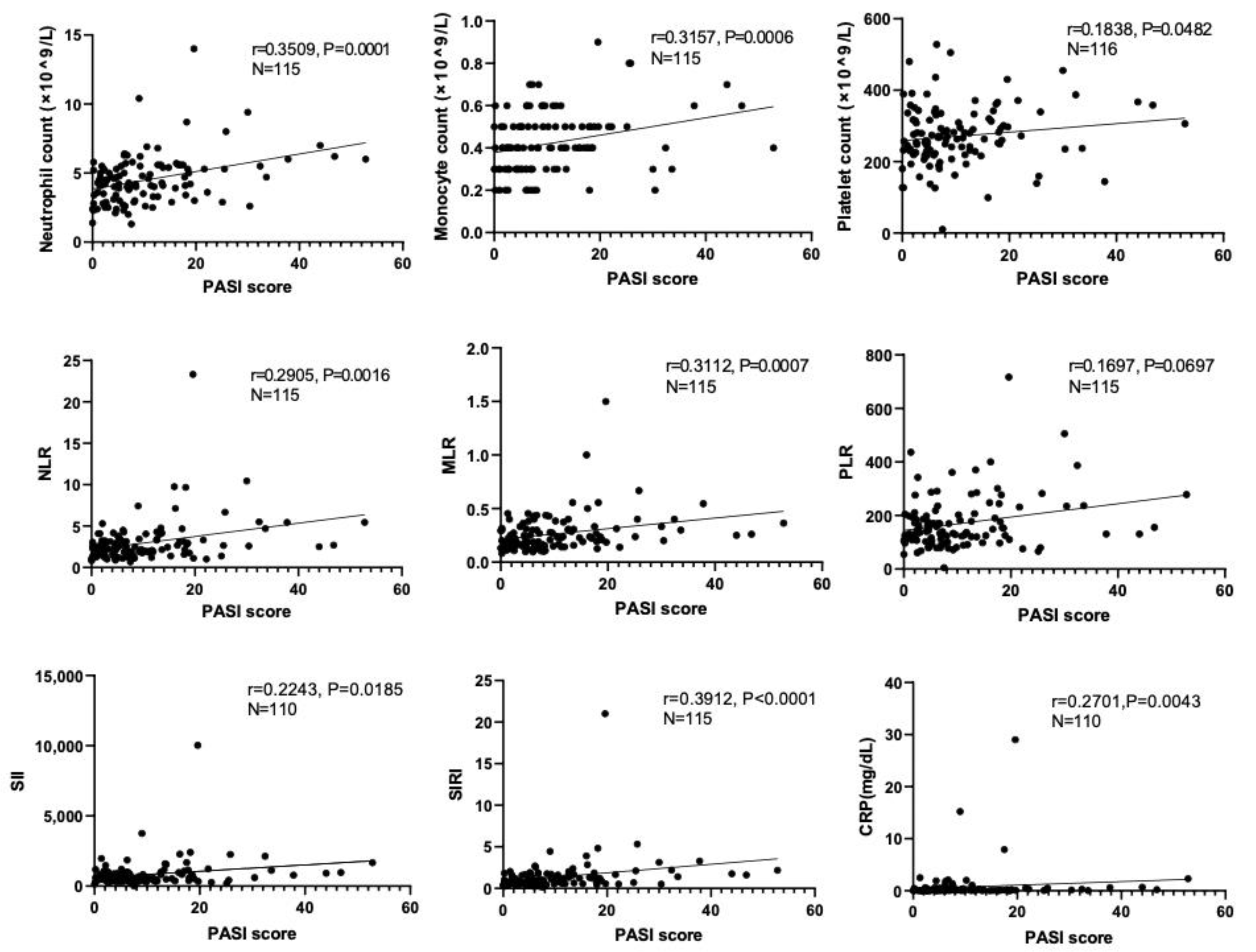
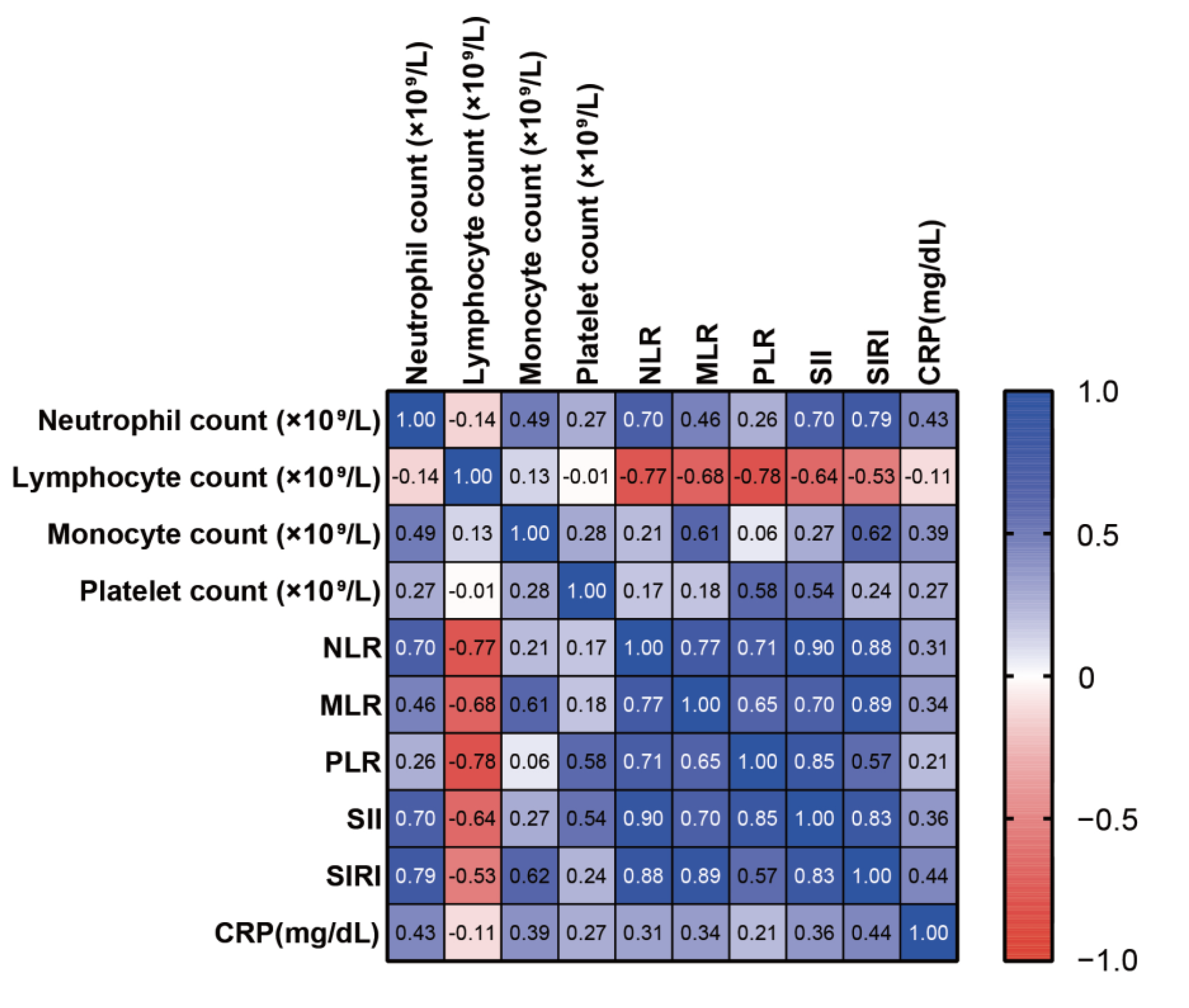
3.2. Correlations of Systemic Inflammatory Biomarkers with PASI Scores
3.3. Association between Systemic Inflammatory Markers and Diagnosis of PsA
3.4. Characteristics and Systemic Inflammatory Markers among Patients with Psoriatic Arthritis with or without Axial Lesions
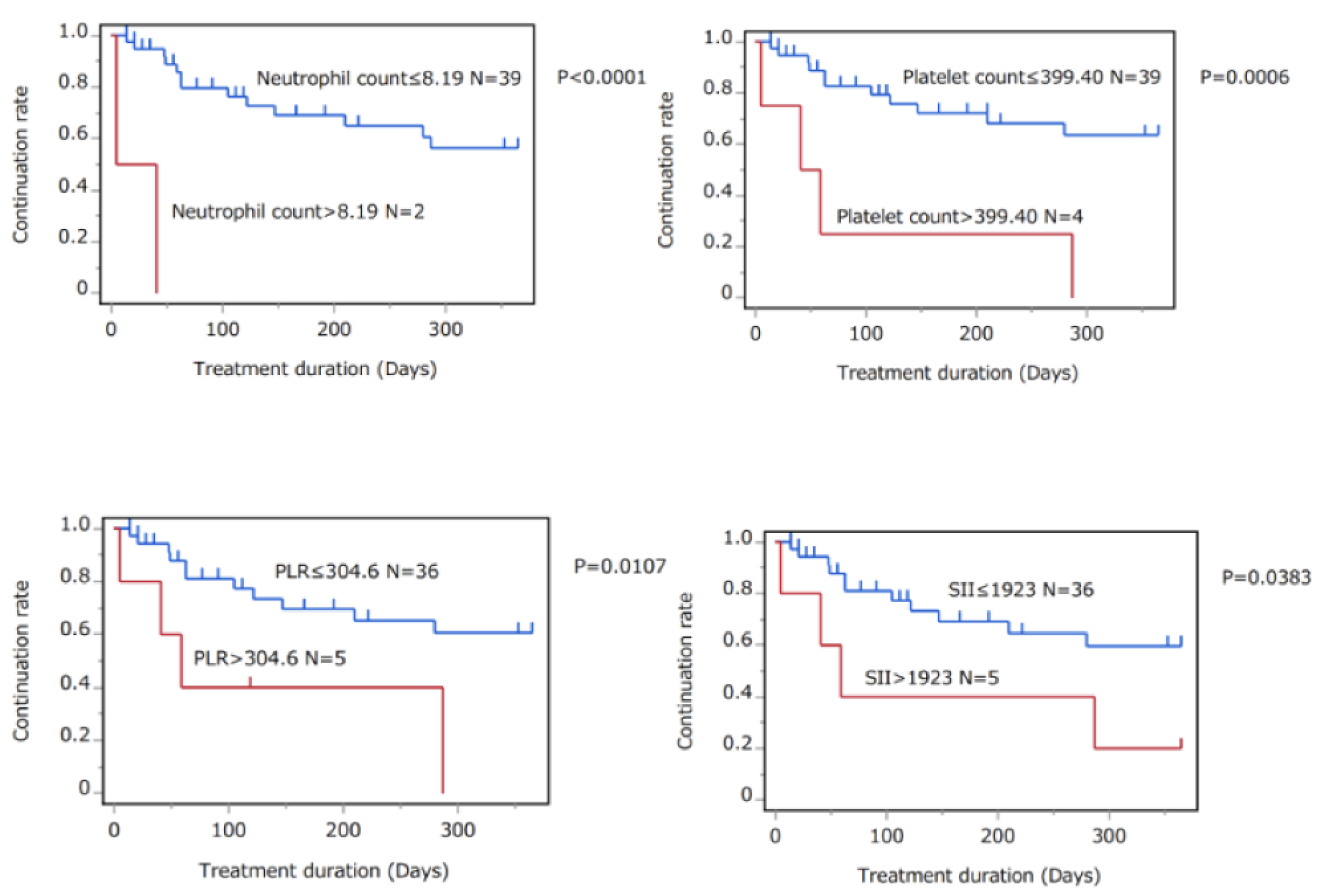
3.5. Association between Systemic Inflammatory Markers and Treatment Continuation Rates of Biologics and Conventional Systemic Agents
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Greb, J.E.; Goldminz, A.M.; Elder, J.T.; Lebwohl, M.G.; Gladman, D.D.; Wu, J.J.; Mehta, N.N.; Finlay, A.Y.; Gottlieb, A.B. Psoriasis. Nat. Rev. Dis. Prim. 2016, 2, 16082. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef]
- Słuczanowska-Głąbowska, S.; Ziegler-Krawczyk, A.; Szumilas, K.; Pawlik, A. Role of Janus Kinase Inhibitors in Therapy of Psoriasis. J. Clin. Med. 2021, 10, 4307. [Google Scholar] [CrossRef] [PubMed]
- Kamata, M.; Tada, Y. Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. Int. J. Mol. Sci. 2020, 21, 1690. [Google Scholar] [CrossRef]
- Ujiie, H.; Rosmarin, D.; Schön, M.P.; Ständer, S.; Boch, K.; Metz, M.; Maurer, M.; Thaci, D.; Schmidt, E.; Cole, C.; et al. Unmet Medical Needs in Chronic, Non-communicable Inflammatory Skin Diseases. Front. Med. 2022, 9, 875492. [Google Scholar] [CrossRef] [PubMed]
- Jadon, D.R.; Stober, C.; Pennington, S.R.; FitzGerald, O. Applying precision medicine to unmet clinical needs in psoriatic disease. Nat. Rev. Rheumatol. 2020, 16, 609–627. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Tada, Y.; Hau, C.; Tatsuta, A.; Yamamoto, M.; Kamata, M.; Karakawa, M.; Asano, Y.; Mitsui, H.; Sugaya, M.; et al. Adiponectin as an anti-inflammatory factor in the pathogenesis of psoriasis: Induction of elevated serum adiponectin levels following therapy. Br. J. Dermatol. 2010, 164, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Saeki, H.; Tada, Y.; Karakawa, M.; Komine, M.; Tamaki, K. Serum high molecular weight adiponectin levels are decreased in psoriasis patients. J. Dermatol. Sci. 2009, 55, 62–63. [Google Scholar] [CrossRef]
- Shibata, S.; Tada, Y.; Hau, C.S.; Mitsui, A.; Kamata, M.; Asano, Y.; Sugaya, M.; Kadono, T.; Masamoto, Y.; Kurokawa, M.; et al. Adiponectin regulates psoriasiform skin inflammation by suppressing IL-17 production from γδ-T cells. Nat. Commun. 2015, 6, 7687. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Boehncke, S.; Tobin, A.-M.; Kirby, B. The ‘psoriatic march’: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef]
- Liu, C.; Chen, H.; Liu, Y.; Huang, H.; Yu, W.; Du, T.; Long, X.; Chen, X.; Chen, Z.; Guo, S.; et al. Immunity: Psoriasis comorbid with atherosclerosis. Front. Immunol. 2022, 13, 7498. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.; Li, D.; Xie, B.B.; Hu, L.H.; Huang, J.; Jia, X.X.; Tang, Y.L.; Liu, G.H.; Shen, N.N.; Yu, X.B. IL-17A and TNF-α inhibitors induce multiple molecular changes in psoriasis. Front. Immunol. 2022, 13, 7012. [Google Scholar] [CrossRef] [PubMed]
- Von Stebut, E.; Boehncke, W.-H.; Ghoreschi, K.; Gori, T.; Kaya, Z.; Thaci, D.; Schäffler, A. IL-17A in Psoriasis and Beyond: Cardiovascular and Metabolic Implications. Front. Immunol. 2019, 10, 3096. [Google Scholar] [CrossRef] [PubMed]
- Larid, G.; Delwail, A.; Dalle, T.; Vasseur, P.; Silvain, C.; Jégou, J.-F.; Morel, F.; Lecron, J.-C.; Gervais, E. Ex vivo cytokine production in psoriatic disease: Towards specific signatures in cutaneous psoriasis and peripheral psoriatic arthritis. Front. Immunol. 2022, 13, 6444. [Google Scholar] [CrossRef]
- Gulliver, W. Long-term prognosis in patients with psoriasis. Br. J. Dermatol. 2008, 159 (Suppl. 2), 2–9. [Google Scholar] [CrossRef] [PubMed]
- Korman, N. Management of psoriasis as a systemic disease: What is the evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef]
- Guthrie, G.J.K.; Charles, K.A.; Roxburgh, C.S.D.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil–lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Asahina, A.; Kubo, N.; Umezawa, Y.; Honda, H.; Yanaba, K.; Nakagawa, H. Neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and mean platelet volume in Japanese patients with psoriasis and psoriatic arthritis: Response to therapy with biologics. J. Dermatol. 2017, 44, 1112–1121. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Satta, R.; Deligia, G.; Farina, G.; Bassu, S.; Mangoni, A.A.; Carru, C.; Zinellu, A. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: A systematic review and meta-analysis. Clin. Exp. Med. 2019, 19, 37–45. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gąsior, J.S.; Tuzimek, A.; Paleczny, J.; Junka, A.; Dąbrowski, M.; Jankowski, P. Investigation of the Associations of Novel Inflammatory Biomarkers—Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)—With the Severity of Coronary Artery Disease and Acute Coronary Syndrome Occurrence. Int. J. Mol. Sci. 2022, 23, 9553. [Google Scholar] [CrossRef]
- Yang, Y.-L.; Wu, C.-H.; Hsu, P.-F.; Chen, S.-C.; Huang, S.-S.; Chan, W.L.; Lin, S.-J.; Chou, C.-Y.; Chen, J.-W.; Pan, J.-P.; et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur. J. Clin. Investig. 2020, 50, e13230. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L. Scoring and monitoring the severity of psoriasis. What is the preferred method? What is the ideal method? Is PASI passé? facts and controversies. Clin. Dermatol. 2010, 28, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D. Enthesitis: An autoinflammatory lesion linking nail and joint involvement in psoriatic disease. J. Eur. Acad. Dermatol. Venereol. 2009, 23 (Suppl. 1), 9–13. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Wu, Q.; Chen, S.; Gao, J.; Li, X.; Zhang, X.; Zhou, Y.; He, D.; Cheng, Z.; Zhu, Y.; et al. The Associations of Two Novel Inflammation Indexes, SII and SIRI with the Risks for Cardiovascular Diseases and All-Cause Mortality: A Ten-Year Follow-Up Study in 85,154 Individuals. J. Inflamm. Res. 2021, 14, 131–140. [Google Scholar] [CrossRef]
- Afari, M.E.; Bhat, T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: An update. Expert Rev. Cardiovasc. Ther. 2016, 14, 573–577. [Google Scholar] [CrossRef]
- Erre, G.L.; Paliogiannis, P.; Castagna, F.; Mangoni, A.A.; Carru, C.; Passiu, G.; Zinellu, A. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur. J. Clin. Investig. 2019, 49, e13037. [Google Scholar] [CrossRef] [PubMed]
- Mercan, R.; Bitik, B.; Tufan, A.; Bozbulut, U.B.; Atas, N.; Ozturk, M.A.; Haznedaroglu, S.; Goker, B. The Association Between Neutrophil/Lymphocyte Ratio and Disease Activity in Rheumatoid Arthritis and Ankylosing Spondylitis. J. Clin. Lab. Anal. 2016, 30, 597–601. [Google Scholar] [CrossRef]
- Mazza, M.G.; Lucchi, S.; Tringali, A.G.M.; Rossetti, A.; Botti, E.R.; Clerici, M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 84 Pt A, 229–236. [Google Scholar] [CrossRef]
- Yorulmaz, A.; Hayran, Y.; Akpinar, U.; Yalcin, B. Systemic Immune-Inflammation Index (SII) Predicts Increased Severity in Psoriasis and Psoriatic Arthritis. Curr. Health Sci. J. 2020, 46, 352–357. [Google Scholar] [CrossRef]
- Abu Rached, N.; Gambichler, T.; Dietrich, J.W.; Ocker, L.; Seifert, C.; Stockfleth, E.; Bechara, F.G. The Role of Hormones in Hidradenitis Suppurativa: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 15250. [Google Scholar] [CrossRef] [PubMed]
- Hessam, S.; Sand, M.; Gambichler, T.; Skrygan, M.; Rüddel, I.; Bechara, F. Interleukin-36 in hidradenitis suppurativa: Evidence for a distinctive proinflammatory role and a key factor in the development of an inflammatory loop. Br. J. Dermatol. 2018, 178, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Hessam, S.; Cramer, P.; Abu Rached, N.; Bechara, F. Complete blood collection-based systemic inflammation biomarkers for patients with hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1593–1596. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Shin, D.; Lee, M.S.; Kim, H.J.; Kim, D.Y.; Kim, S.M.; Lee, M.G. Assessments of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in Korean patients with psoriasis vulgaris and psoriatic arthritis. J. Dermatol. 2016, 43, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Polat, M.; Bugdayci, G.; Kaya, H.; Oğuzman, H. Evaluation of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in Turkish patients with chronic plaque psoriasis. Acta Dermatovenerol. Alp. Pannonica Adriat. 2017, 26, 97–100. [Google Scholar] [CrossRef]
- Hammad, R.; Hamdino, M.; El-Nasser, A.M. Role of Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, Mean Platelet Volume in Egyptian Patients with Psoriasis Vulgaris. Egypt J. Immunol. 2020, 27, 157–168. [Google Scholar]
- Wang, W.-M.; Wu, C.; Gao, Y.-M.; Li, F.; Yu, X.-L.; Jin, H.-Z. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and other hematological parameters in psoriasis patients. BMC Immunol. 2021, 22, 64. [Google Scholar] [CrossRef]
- Cho, K.I.; Ann, S.H.; Singh, G.B.; Her, A.-Y.; Shin, E.-S. Combined Usefulness of the Platelet-to-Lymphocyte Ratio and the Neutrophil-to-Lymphocyte Ratio in Predicting the Long-Term Adverse Events in Patients Who Have Undergone Percutaneous Coronary Intervention with a Drug-Eluting Stent. PLoS ONE 2015, 10, e0133934. [Google Scholar] [CrossRef]
- Awaji, K.; Miyagawa, T.; Omatsu, J.; Numajiri, H.; Kawai, T.; Funamizu, K.; Saigusa, R.; Yamada, D.; Asano, Y.; Sato, S. Prognostic Relevance of Pretreatment Peripheral Neutrophil Count and Neutrophil-to-lymphocyte Ratio in Primary Cutaneous Angiosarcoma. Acta Derm.-Venereol. 2021, 101, adv00527. [Google Scholar] [CrossRef]
- Gawaz, M.; Langer, H.; May, A.E. Platelets in inflammation and atherogenesis. J. Clin. Investig. 2005, 115, 3378–3384. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Brzoza, Z.; Rogala, B. Platelet function in cutaneous diseases. Platelets 2008, 19, 317–321. [Google Scholar] [CrossRef]
- Davizon-Castillo, P.; McMahon, B.; Aguila, S.; Bark, D.; Ashworth, K.; Allawzi, A.; Campbell, R.A.; Montenont, E.; Nemkov, T.; D’alessandro, A.; et al. TNF-α–driven inflammation and mitochondrial dysfunction define the platelet hyperreactivity of aging. Blood 2019, 134, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.J.; Schlegel, M.; Zhou, F.; Gorenchtein, M.; Bolstorff, J.; Moore, K.J.; Fisher, E.A.; Berger, J.S. Platelet regulation of myeloid suppressor of cytokine signaling 3 accelerates atherosclerosis. Sci. Transl. Med. 2019, 11, eaax0481. [Google Scholar] [CrossRef] [PubMed]
- Garshick, M.S.; Tawil, M.; Barrett, T.; Salud-Gnilo, C.M.; Eppler, M.; Lee, A.; Scher, J.U.; Neimann, A.L.; Jelic, S.; Mehta, N.N.; et al. Activated Platelets Induce Endothelial Cell Inflammatory Response in Psoriasis via COX-1. Arter. Thromb. Vasc. Biol. 2020, 40, 1340–1351. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, K.; Yamamoto, O.; Honda, T. Pathophysiology of psoriasis: A review. J. Dermatol. 2021, 48, 722–731. [Google Scholar] [CrossRef]
- Chiang, C.-C.; Cheng, W.-J.; Korinek, M.; Lin, C.-Y.; Hwang, T.-L. Neutrophils in Psoriasis. Front. Immunol. 2019, 10, 2376. [Google Scholar] [CrossRef]
- Herster, F.; Bittner, Z.; Archer, N.K.; Dickhöfer, S.; Eisel, D.; Eigenbrod, T.; Knorpp, T.; Schneiderhan-Marra, N.; Löffler, M.W.; Kalbacher, H.; et al. Neutrophil extracellular trap-associated RNA and LL37 enable self-amplifying inflammation in psoriasis. Nat. Commun. 2020, 11, 105. [Google Scholar] [CrossRef]
- Gabr, S.A.; Al-Ghadir, A.H. Role of cellular oxidative stress and cytochrome c in the pathogenesis of psoriasis. Arch. Dermatol. Res. 2012, 304, 451–457. [Google Scholar] [CrossRef]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O’Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat. Rev. Drug Discov. 2017, 17, 78. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Bagel, J.; Van Voorhees, A.S.; Robertson, A.D.; Yamauchi, P.S. Combining Biologic Therapies With Other Systemic Treatments in Psoriasis: Evidence-based, best-practice recommendations from the Medical Board of the National Psoriasis Foundation. JAMA Dermatol. 2015, 151, 432–438. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PsV (N = 117) | PsA (N = 47) | Healthy (N = 50) | p Value | |||
|---|---|---|---|---|---|---|
| PsV vs. Healthy | PsA vs. Healthy | PsV vs. PsA | ||||
| Age, years | 51.16 ± 18.26 | 55.49 ± 13.78 | 54.30 ± 13.62 | 0.6302 | >0.9999 | 0.4962 |
| Male, % | 68 | 62 | 64 | 0.5938 | 0.8364 | 0.4658 |
| PASI scores | 10.66 ± 10.63 | 9.18 ± 8.48 | 0.6310 | |||
| Neu (×109/L) | 4.294 ± 1.345 | 4.787 ± 2.123 | 4.154 ± 2.018 | 0.2908 | 0.0641 | 0.6745 |
| Lym (×109/L) | 1.865 ± 0.665 | 1.780 ± 0.712 | 1.744 ± 0.590 | 0.4901 | >0.9999 | 0.8067 |
| Mono (×109/L) | 0.407 ± 0.128 | 0.437 ± 0.154 | 0.368 ± 0.111 | 0.1182 | 0.0179 | 0.5777 |
| Platelet (×109/L) | 259.52 ± 71.14 | 289.85 ± 90.13 | 272.06 ± 63.668 | 0.5466 | 0.4657 | 0.0324 |
| NLR | 2.704 ± 1.659 | 3.415 ± 3.477 | 2.614 ± 1.53 | >0.9999 | 0.4631 | 0.3745 |
| MLR | 0.247 ± 0.134 | 0.294 ± 0.220 | 0.227 ± 0.082 | >0.9999 | 0.3714 | 0.4092 |
| PLR | 154.9 ± 65.11 | 196.3 ± 125.29 | 172.116 ± 66.244 | 0.3601 | >0.9999 | 0.2232 |
| SII | 687.1 ± 445.2 | 1105 ± 1515 | 733.020 ± 594.958 | >0.9999 | 0.4281 | 0.1560 |
| SIRI | 1.13 ± 0.85 | 1.74 ± 3.06 | 1.019 ± 0.964 | 0.7774 | 0.0711 | 0.2715 |
| CRP (mg/dL) | 0.29 ± 0.57 | 1.48 ± 4.84 | 0.0284 | |||
| Cut-Off Values | AUC | Sensitivity | Specificity | |
|---|---|---|---|---|
| NLR | 3.211 | 0.57012 | 0.3913 | 0.7683 |
| MLR | 0.208 | 0.56747 | 0.6739 | 0.4878 |
| PLR | 275 | 0.57887 | 0.2826 | 0.939 |
| SII | 911.6 | 0.59213 | 0.4348 | 0.7805 |
| SIRI | 0.870 | 0.57542 | 0.6522 | 0.5122 |
| CRP (mg/dL) | 0.30 | 0.58643 | 0.4130 | 0.7927 |
| Factors | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR (95 % CI) | p Value | OR (95 % CI) | p Value | ||
| NLR | ≥3.211 | 2.184 (0.918–5.194) | 0.077 | 0.579 (0.134–2.498) | 0.464 |
| MLR | ≥0.208 | 2.355 (1.044–5.316) | 0.039 | 2.789 (0.845–9.201) | 0.092 |
| PLR | ≥275 | 5.775 (1.698–19.643) | 0.005 | 7.027 (1.089–45.348) | 0.040 |
| SII | ≥911.6 | 1.682 (0.759–3.728) | 0.200 | 0.506 (0.139–1.843) | 0.302 |
| SIRI | ≥0.870 | 2.423 (1.024–5.729) | 0.044 | 0.915 (0.227–3.682) | 0.901 |
| CRP (mg/dL) | ≥0.30 | 3.251 (1.379–7.716) | 0.008 | 3.179 (1.183–8.538) | 0.022 |
| With Axial Lesions | Without Axial Lesions | p Value | |
|---|---|---|---|
| Age, years | 55.5 ± 14.8 | 55.5 ± 12.9 | 0.8699 |
| Male, % | 64 | 59 | 0.7712 |
| PASI scores | 12.02 ± 9.75 | 6.05 ± 5.52 | 0.0227 |
| Neutrophil count (×109/L) | 4.96 ± 2.59 | 4.60 ± 1.50 | 0.7894 |
| Lymphocyte count (×109/L) | 1.88 ± 0.84 | 1.67 ± 0.54 | 0.5518 |
| Monocyte count (×109/L) | 0.44 ± 0.17 | 0.43 ± 0.14 | 0.8643 |
| Platelet count (×109/L) | 295.72 ± 100.06 | 283.18 ± 79.14 | 0.5019 |
| NLR | 3.68 ± 4.53 | 3.13 ± 1.80 | 0.4887 |
| MLR | 0.31 ± 0.28 | 0.28 ± 0.12 | 0.5820 |
| PLR | 199.13 ± 148.26 | 193.20 ± 97.69 | 0.6869 |
| SII | 1288.77 ± 2031.87 | 903.87 ± 562.58 | 0.7522 |
| SIRI | 2.08 ± 4.15 | 1.36 ± 0.96 | 0.6200 |
| ESR (mm/h) | 28.28 ± 36.00 | 16.10 ± 18.02 | 0.8397 |
| CRP (mg/dL) | 2.60 ± 6.55 | 0.26 ± 0.53 | 0.0271 |
| Treatment | Number of Patients | Concomitant Treatments during the One-Year Follow-Up | |
|---|---|---|---|
| Biologics (N = 51) | Infliximab | 9 | None |
| Adalimumab | 2 | None | |
| Certolizumab Pegol | 0 | None | |
| Secukinumab | 11 | One patient received cyclosporine. One patient received apremilast. | |
| Ixekizumab | 5 | None | |
| Brodalumab | 1 | None | |
| Bimekizumab | 0 | None | |
| Guselkumab | 8 | None | |
| Risankizumab | 11 | None | |
| Tildrakizumab | 4 | None | |
| Ustekinumab | 0 | None | |
| Conventional systemic agents (N = 48) | Methotrexate | 8 | One patient received cyclosporine. |
| Etretinate | 6 | One patient received apremilast. | |
| Cyclosporine | 3 | None | |
| Apremilast | 31 | One patient received etretinate. One patient received secukinumab. |
| Cut-Off Values | Median Treatment Duration (Days) | Log-Rank Test | ||
|---|---|---|---|---|
| High-Score Group | Non-High-Score Group | p Value | ||
| Neu (×109/L) | 8.19 | 365 | 365 ± 102.48 | 0.6483 |
| Lym (×109/L) | 2.92 | 308.5 ± 81.79 | 365 ± 104.89 | 0.8662 |
| Mono (×109/L) | 0.59 | 365 ± 27.98 | 365 ± 108.76 | 0.6100 |
| Platelet (×109/L) | 399.40 | 365 | 365 ± 102.48 | 0.6483 |
| NLR | 5.674 | 365 | 365 ± 104.54 | 0.3418 |
| MLR | 0.391 | 365 ± 68.99 | 365 ± 106.45 | 0.5994 |
| PLR | 304.6 | 365 | 365 ± 102.48 | 0.6483 |
| SII | 1923 | 365 | 365 ± 103.16 | 0.5133 |
| SIRI | 2.95 | 365 ± 20.78 | 365 ± 104.18 | 0.5638 |
| CRP (mg/dL) | 0.69 | 365 ± 98.84 | 365 ± 102.32 | 0.3290 |
| Cut-Off Values | Median Treatment Duration (Days) | Log-Rank Test | ||
|---|---|---|---|---|
| High-Score Group | Non-High-Score Group | p Value | ||
| Neu (×109/L) | 8.19 | 23 ± 25.46 | 147 ± 142.22 | <0.0001 |
| Lym (×109/L) | 2.92 | 166 | 120.5 ± 145.10 | 0.5101 |
| Mono (×109/L) | 0.59 | 63 ± 167.27 | 147 ± 139.52 | 0.3175 |
| Platelet (×109/L) | 399.40 | 50 ± 127.98 | 166 ± 142.58 | 0.0006 |
| NLR | 5.674 | 41 ± 198.27 | 134.5 ± 141.10 | 0.1335 |
| MLR | 0.391 | 59 ± 144.21 | 156.5 ± 143.01 | 0.1053 |
| PLR | 304.6 | 59 ± 111.23 | 156.5 ± 145.12 | 0.0107 |
| SII | 1923 | 59 ± 162.92 | 134.5 ± 142.47 | 0.0383 |
| SIRI | 2.95 | 41 ± 198.27 | 134.5 ± 141.10 | 0.1335 |
| CRP (mg/dL) | 0.69 | 280 ± 156.94 | 122 ± 144.04 | 0.1303 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugimoto, E.; Matsuda, H.; Shibata, S.; Mizuno, Y.; Koyama, A.; Li, L.; Taira, H.; Ito, Y.; Awaji, K.; Yamashita, T.; et al. Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis. J. Clin. Med. 2023, 12, 3046. https://doi.org/10.3390/jcm12083046
Sugimoto E, Matsuda H, Shibata S, Mizuno Y, Koyama A, Li L, Taira H, Ito Y, Awaji K, Yamashita T, et al. Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis. Journal of Clinical Medicine. 2023; 12(8):3046. https://doi.org/10.3390/jcm12083046
Chicago/Turabian StyleSugimoto, Eiki, Hiroki Matsuda, Sayaka Shibata, Yuka Mizuno, Asumi Koyama, Lixin Li, Haruka Taira, Yukiko Ito, Kentaro Awaji, Takashi Yamashita, and et al. 2023. "Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis" Journal of Clinical Medicine 12, no. 8: 3046. https://doi.org/10.3390/jcm12083046