
Molecular Background and Clinical Implications of Glucose Disorders in Patients with Psoriatic Arthritis

Abstract
:1. Introduction
2. Methods
3. Epidemiology of Glucose Impairment in Patients with Psoriatic Arthritis
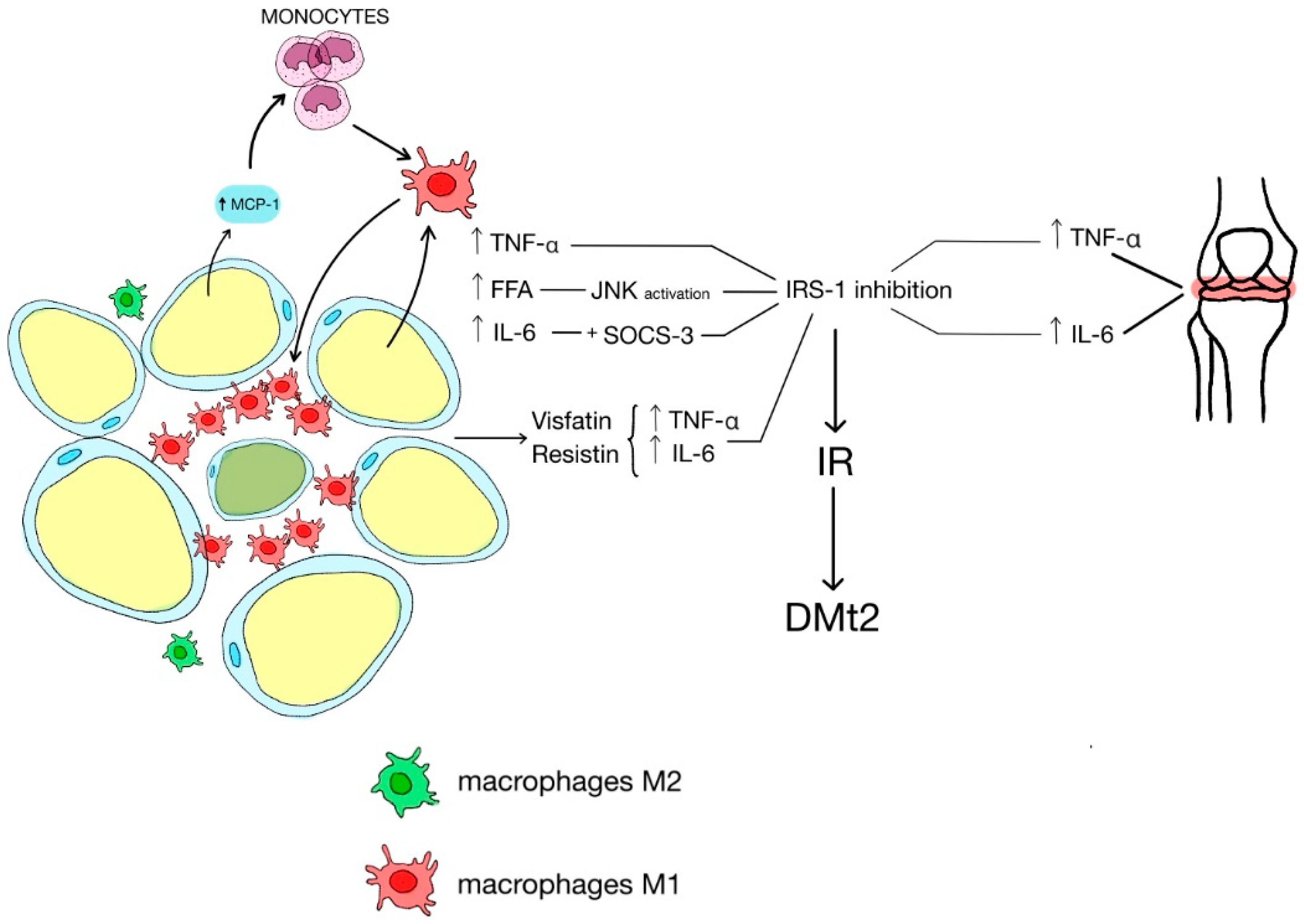
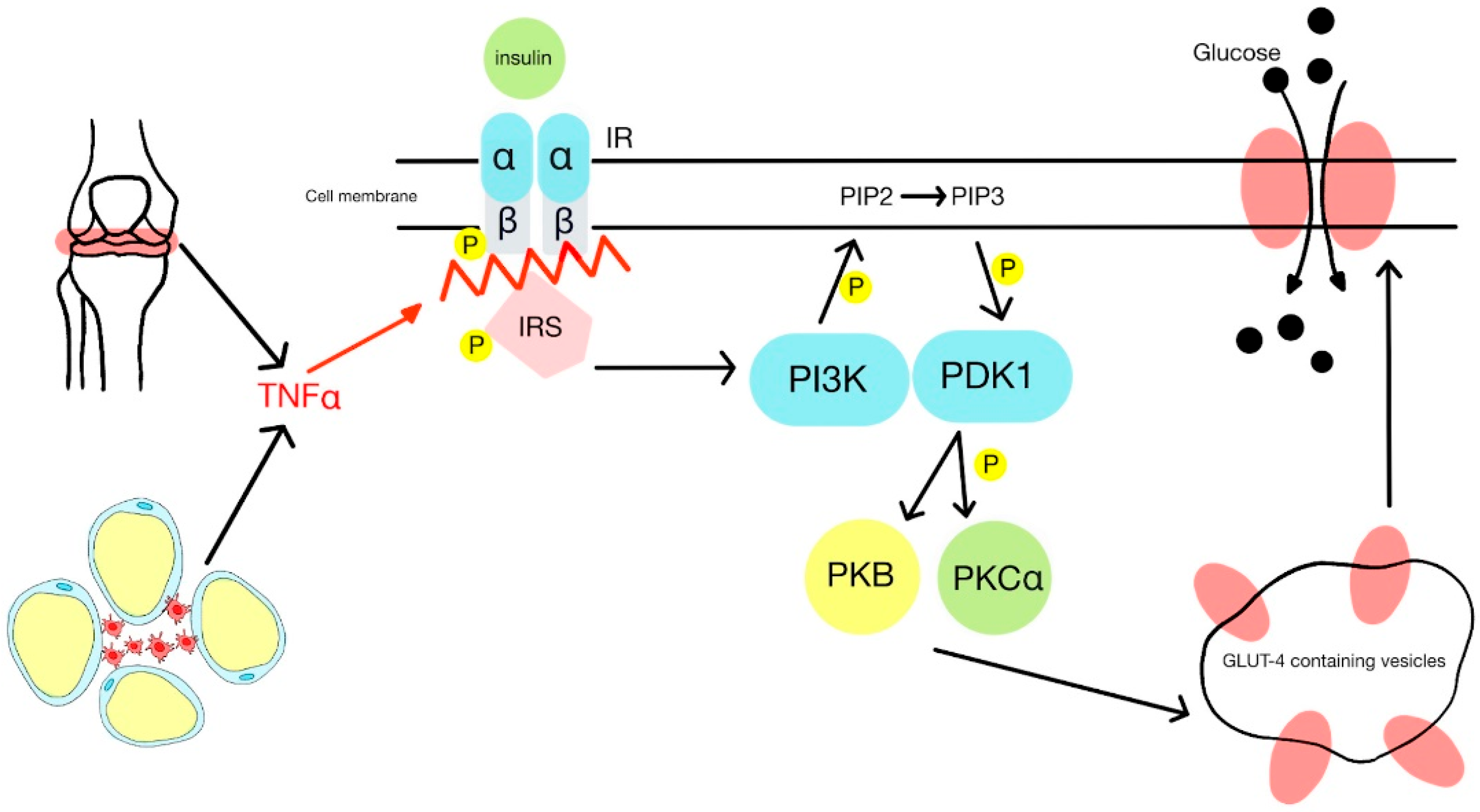
4. Mechanisms of Increased Glucose Levels in PsA
5. Adipokines Influence on Glucose Disorders
6. Psoriatic Skin Changes and Hyperglycemia
7. Effectiveness of Reducing Hyperglycemia during the Standard Treatment of PsA
8. Diabetes Mellitus Type 2 Treatment in PsA Patients
9. Non-Pharmacological Recommendations for Hyperglycemia and DMt2 Treatment in PsA

{kind=link}
{kind=link}
| Treatment Options in Patients with PsA and DMt2 | |||
|---|---|---|---|
| Treatment | Specific Recommendation | Characteristics | Reference |
| non-pharmacological | Body mass reduction |
| [12,30,67,68] |
| Well-balanced diet |
| [90,91] | |
| Physical activity |
| [73,92] | |
| Cessation of smoking |
| [94] | |
| Treatment of chronic inflammation sources |
| [96,97] | |
| Practice stress-relieving techniques |
| [93,98] | |
| pharmacological | Successful treatment of psoriasis |
| [10,70] |
| Avoiding GCS and isotretinoin in psoriasis treatment |
| [51,71] | |
| MTX administration |
| [52,53,54] | |
| NSAIDs |
| [55] | |
| TNF-α |
| [58,59,60,61,62] | |
| JAK1/2 inhibitors |
| [63] | |
| IL-17 antibody |
| [47,48,64,65,66] | |
| Combined testament | MTX and metformin |
| [75,76] |
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coates, L.; Helliwell, P.S. Psoriatic arthritis: State of the art review. Clin. Med. 2017, 17, 65–70. [Google Scholar] [CrossRef]
- Queiro, R.; Lorenzo, A.; Pardo, E.; Brandy, A.; Coto, P.; Ballina, J. Prevalence and type II diabetes-associated factors in psoriatic arthritis. Clin. Rheumatol. 2018, 37, 1059–1064. [Google Scholar] [CrossRef]
- Husni, M.E. Comorbidities in Psoriatic Arthritis. Rheum. Dis. Clin. N. Am. 2015, 41, 677–698. [Google Scholar] [CrossRef] [PubMed]
- Maliniak, M.L.; Miller-Kleinhenz, J.; Cronin-Fenton, D.P.; Lash, T.L.; Gogineni, K.; Janssen, E.A.M.; McCullough, L.E. Crown-Like Structures in Breast Adipose Tissue: Early Evidence and Current Issues in Breast Cancer. Cancers 2021, 13, 2222. [Google Scholar] [CrossRef] [PubMed]
- Akash, M.S.H.; Rehman, K.; Liaqat, A. Tumor Necrosis Factor-Alpha: Role in Development of Insulin Resistance and Pathogenesis of Type 2 Diabetes Mellitus. J. Cell. Biochem. 2018, 119, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, V.; Werner, E.D.; Giraud, J.; Lee, Y.H.; Shoelson, S.E.; White, M.F. Phosphorylation of Ser307 in insulin receptor substrate-1 blocks interactions with the insulin receptor and inhibits insulin action. J. Biol. Chem. 2002, 277, 1531–1537. [Google Scholar] [CrossRef]
- Dal Bello, G.; Gisondi, P.; Idolazzi, L.; Girolomoni, G. Psoriatic Arthritis and Diabetes Mellitus: A Narrative Review. Rheumatol. Ther. 2020, 7, 271–285. [Google Scholar] [CrossRef]
- Ogdie, A.; Weiss, P. The Epidemiology of Psoriatic Arthritis. Rheum. Dis. Clin. N. Am. 2015, 41, 545–568. [Google Scholar] [CrossRef]
- Wilson, F.C.; Icen, M.; Crowson, C.S.; McEvoy, M.T.; Gabriel, S.E.; Kremers, H.M. Incidence and clinical predictors of psoriatic arthritis in patients with psoriasis: A population-based study. Arthritis Care Res. 2009, 61, 233–239. [Google Scholar] [CrossRef]
- Eder, L.; Haddad, A.; Rosen, C.F.; Lee, K.A.; Chandran, V.; Cook, R.; Gladman, D.D. The Incidence and Risk Factors for Psoriatic Arthritis in Patients with Psoriasis: A Prospective Cohort Study. Arthritis Rheumatol. 2016, 68, 915–923. [Google Scholar] [CrossRef]
- Soltani-Arabshahi, R.; Wong, B.; Feng, B.J.; Goldgar, D.E.; Duffin, K.C.; Krueger, G.G. Obesity in early adulthood as a risk factor for psoriatic arthritis. Arch. Dermatol. 2010, 146, 721–726. [Google Scholar] [CrossRef]
- Mok, C.C.; Ko, G.T.; Ho, L.Y.; Yu, K.L.; Chan, P.T.; To, C.H. Prevalence of atherosclerotic risk factors and the metabolic syndrome in patients with chronic inflammatory arthritis. Arthritis Care Res. 2011, 63, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Queiro, R.; Tejón, P.; Alonso, S.; Coto, P. Age at disease onset: A key factor for understanding psoriatic disease. Rheumatology 2014, 53, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Dreiher, J.; Freud, T.; Cohen, A.D. Psoriatic arthritis and diabetes: A population-based cross-sectional study. Dermatol. Res. Pract. 2013, 2013, 580404. [Google Scholar] [CrossRef]
- Gialouri, C.G.; Evangelatos, G.; Iliopoulos, A.; Tektonidou, M.G.; Sfikakis, P.P.; Fragoulis, G.E.; Nikiphorou, E. Late-Onset Psoriatic Arthritis: Are There Any Distinct Characteristics? A Retrospective Cohort Data Analysis. Life 2023, 13, 792. [Google Scholar] [CrossRef]
- Tam, L.-S.; Tomlinson, B.; Chu, T.T.-W.; Li, M.; Leung, Y.-Y.; Kwok, L.-W.; Li, T.K.; Yu, T.; Zhu, Y.-E.; Wong, K.-C.; et al. Cardiovascular risk profile of patients with psoriatic arthritis compared to controls—The role of inflammation. Rheumatology 2008, 47, 718–723. [Google Scholar] [CrossRef]
- Houmard, J.A.; Weidner, M.D.; Dolan, P.L.; Leggett-Frazier, N.; Gavigan, K.E.; Hickey, M.S.; Tyndall, G.L.; Zheng, D.; Alshami, A.; Dohm, G.L. Skeletal muscle GLUT4 protein concentration and aging in humans. Diabetes 1995, 44, 555–560. [Google Scholar] [CrossRef]
- Sesti, G. Pathophysiology of insulin resistance. Best Pract. Res. Clin. Endocrinol. Metab. 2006, 20, 665–679. [Google Scholar] [CrossRef]
- Guo, S. Insulin signaling, resistance, and the metabolic syndrome: Insights from mouse models into disease mechanisms. J. Endocrinol. 2014, 220, T1–T23. [Google Scholar] [CrossRef]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: An endocrine organ. Arch. Med. Sci. 2013, 9, 191–200. [Google Scholar] [CrossRef]
- Senn, J.J.; Klover, P.J.; Nowak, I.A.; Zimmers, T.A.; Koniaris, L.G.; Furlanetto, R.W.; Mooney, R.A. Suppressor of cytokine signaling-3 (SOCS-3), a potential mediator of interleukin-6-dependent insulin resistance in hepatocytes. J. Biol. Chem. 2003, 278, 13740–13746. [Google Scholar] [CrossRef]
- Ueki, K.; Kadowaki, T.; Kahn, C.R. Role of suppressors of cytokine signaling SOCS-1 and SOCS-3 in hepatic steatosis and the metabolic syndrome. Hepatol. Res. 2005, 33, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020, 877, 173090. [Google Scholar] [CrossRef]
- Matulewicz, N.; Karczewska-Kupczewska, M. Insulin resistance and chronic inflammation. Postep. Hig. Med. Dosw. 2016, 70, 1245–1258. [Google Scholar]
- Weston, C.R.; Davis, R.J. The JNK signal transduction pathway. Curr. Opin. Genet. Dev. 2002, 12, 14–21. [Google Scholar] [CrossRef]
- Han, Z.; Boyle, D.L.; Chang, L.; Bennett, B.; Karin, M.; Yang, L.; Manning, A.M.; Firestein, G.S. c-Jun N-terminal kinase is required for metalloproteinase expression and joint destruction in inflammatory arthritis. J. Clin. Investig. 2001, 108, 73–81. [Google Scholar] [CrossRef]
- Bhole, V.M.; Choi, H.K.; Burns, L.C.; Vera Kellet, C.; Lacaille, D.V.; Gladman, D.D.; Dutz, J.P. Differences in body mass index among individuals with PsA, psoriasis, RA and the general population. Rheumatology 2012, 51, 552–556. [Google Scholar] [CrossRef]
- Caso, F.; Chimenti, M.S.; Navarini, L.; Ruscitti, P.; Peluso, R.; Girolimetto, N.; Del Puente, A.; Giacomelli, R.; Scarpa, R.; Costa, L. Metabolic Syndrome and psoriatic arthritis: Considerations for the clinician. Expert Rev. Clin. Immunol. 2020, 16, 409–420. [Google Scholar] [CrossRef]
- Queiro, R.; Lorenzo, A.; Tejón, P.; Coto, P.; Pardo, E. Obesity in psoriatic arthritis: Comparative prevalence and associated factors. Medicine 2019, 98, e16400. [Google Scholar] [CrossRef] [PubMed]
- Bastard, J.P.; Maachi, M.; Lagathu, C.; Kim, M.J.; Caron, M.; Vidal, H.; Capeau, J.; Feve, B. Recent advances in the relationship between obesity, inflammation, and insulin resistance. Eur. Cytokine Netw. 2006, 17, 4–12. [Google Scholar]
- Dikbas, O.; Tosun, M.; Bes, C.; Tonuk, S.B.; Aksehirli, O.Y.; Soy, M. Serum levels of visfatin, resistin and adiponectin in patients with psoriatic arthritis and associations with disease severity. Int. J. Rheum. Dis. 2016, 19, 672–677. [Google Scholar] [CrossRef]
- Borst, S.E. The role of TNF-alpha in insulin resistance. Endocrine 2004, 23, 177–182. [Google Scholar] [CrossRef]
- Krysiak, R.; Handzlik-Orlik, G.; Okopien, B. The role of adipokines in connective tissue diseases. Eur. J. Nutr. 2012, 51, 513–528. [Google Scholar] [CrossRef]
- Ismail, S.; Mohamed, S.A. Serum levels of visfatin and omentin-1 in patients with psoriasis and their relation to disease severity. Brit. J. Dermatol. 2012, 162, 436–439. [Google Scholar] [CrossRef]
- Dağdelen, D.; Karadag, A.S.; Kasapoğlu, E.; Wang, J.V.; Erman, H. Correlation of metabolic syndrome with serum omentin-1 and visfatin levels and disease severity in psoriasis and psoriatic arthritis. Dermatol. Ther. 2020, 33, e14378. [Google Scholar] [CrossRef]
- Chang, Y.H.; Chang, D.M.; Lin, K.C.; Shin, S.J.; Lee, Y.J. Visfatin in overweight/obesity, type 2 diabetes mellitus, insulin resistance, metabolic syndrome and cardiovascular diseases: A meta-analysis and systemic review. Diabetes Metab. Res. Rev. 2011, 27, 515–527. [Google Scholar] [CrossRef]
- López-Bermejo, A.; Chico-Julià, B.; Fernàndez-Balsells, M.; Recasens, M.; Esteve, E.; Casamitjana, R.; Ricart, W.; Fernández-Real, J.M. Serum visfatin increases with progressive beta-cell deterioration. Diabetes 2006, 55, 2871–2875. [Google Scholar] [CrossRef]
- Esteghamati, A.; Alamdari, A.; Zandieh, A.; Elahi, S.; Khalilzadeh, O.; Nakhjavani, M.; Meysamie, A. Serum visfatin is associated with type 2 diabetes mellitus independent of insulin resistance and obesity. Diabetes Res. Clin. Pract. 2011, 91, 154–158. [Google Scholar] [CrossRef]
- Schoels, M.M.; Aletaha, D.; Alasti, F.; Smolen, J.S. Disease activity in psoriatic arthritis (PsA): Defining remission and treatment success using the DAPSA score. Ann. Rheum. Dis. 2016, 75, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Toussirot, E. Mini-Review: The Contribution of Adipokines to Joint Inflammation in Inflammatory Rheumatic Diseases. Front. Endocrinol. 2020, 11, 606560. [Google Scholar] [CrossRef]
- Steppan, C.M.; Bailey, S.T.; Bhat, S.; Brown, E.J.; Banerjee, R.R.; Wright, C.M.; Patel, H.R.; Ahima, R.S.; Lazar, M.A. The hormone resistin links obesity to diabetes. Nature 2001, 409, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Bokarewa, M.; Nagaev, I.; Dahlberg, L.; Smith, U.; Tarkowski, A. Resistin, an adipokine with potent pro-inflammatory properties. J. Immunol. 2005, 174, 5789–5795. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Sarkar, M.K.; Tsoi, L.C.; Gudjonsson, J.E. Psoriasis: A mixed autoimmune and autoinflammatory disease. Curr. Opin. Immunol. 2017, 49, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. Psoriasis and the risk of diabetes mellitus: A systematic review and meta-analysis. JAMA Dermatol. 2013, 149, 84–91. [Google Scholar] [CrossRef]
- Azfar, R.S.; Seminara, N.M.; Shin, D.B.; Troxel, A.B.; Margolis, D.J.; Gelfand, J.M. Increased risk of diabetes mellitus and likelihood of receiving diabetes mellitus treatment in patients with psoriasis. Arch. Dermatol. 2012, 148, 995–1000. [Google Scholar] [CrossRef]
- Malakouti, M.; Brown, G.E.; Wang, E.; Koo, J.; Levin, E.C. The role of IL-17 in psoriasis. J. Dermatol. Treat. 2015, 26, 41–44. [Google Scholar] [CrossRef]
- Kyriakou, A.; Patsatsi, A.; Vyzantiadis, T.A.; Sotiriadis, D. Serum levels of TNF-α, IL-12/23p40, and IL-17 in plaque psoriasis and their correlation with disease severity. J. Immunol. Res. 2014, 2014, 467541. [Google Scholar] [CrossRef]
- Rajendran, S.; Quesada-Masachs, E.; Zilberman, S.; Graef, M.; Kiosses, W.B.; Chu, T.; Benkahla, M.A.; Lee, J.M.; von Herrath, M. IL-17 is expressed on beta and alpha cells of donors with type 1 and type 2 diabetes. J. Autoimmun. 2021, 123, 102708. [Google Scholar] [CrossRef]
- Ikumi, K.; Odanaka, M.; Shime, H.; Imai, M.; Osaga, S.; Taguchi, O.; Nishida, E.; Hemmi, H.; Kaisho, T.; Morita, A.; et al. Hyperglycemia Is Associated with Psoriatic Inflammation in Both Humans and Mice. J. Investig. Dermatol. 2019, 139, 1329–1338.e7. [Google Scholar] [CrossRef]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef]
- Elena, C.; Chiara, M.; Angelica, B.; Chiara, M.A.; Laura, N.; Chiara, C.; Claudio, C.; Antonella, F.; Nicola, G. Hyperglycemia and Diabetes Induced by Glucocorticoids in Non-diabetic and Diabetic Patients: Revision of Literature and Personal Considerations. Curr. Pharm. Biotechnol. 2018, 19, 1210–1220. [Google Scholar] [CrossRef]
- Perdan-Pirkmajer, K.; Pirkmajer, S.; Thevis, M.; Thomas, A.; Praprotnik, S.; Hočevar, A.; Rotar, Ž.; Gašperšič, N.; Sodin-Šemrl, S.; Žibert, J.; et al. Methotrexate reduces HbA1c concentration but does not produce chronic accumulation of ZMP in patients with rheumatoid or psoriatic arthritis. Scand. J. Rheumatol. 2016, 45, 347–355. [Google Scholar] [CrossRef]
- Dehpouri, T.; Rokni, G.R.; Narenjbon, N.A.; Goldust, M.; Yamauchi, P.S.; Wollina, U.; Lotti, T.; Kircik, L.; Lernia, V.G.D.; Sonthalia, S.; et al. Evaluation of the glycemic effect of methotrexate in psoriatic arthritis patients with metabolic syndrome: A pilot study. Dermatol. Rep. 2019, 11, 7965. [Google Scholar] [CrossRef]
- Sjöholm, A.; Nyström, T. Inflammation and the etiology of type 2 diabetes. Diabetes Metab. Res. Rev. 2006, 22, 4–10. [Google Scholar] [CrossRef]
- Tsai, H.J.; Hsu, Y.H.; Huang, Y.W.; Chang, Y.K.; Liu, J.S.; Hsu, C.C. Use of non-steroidal anti-inflammatory drugs and risk of chronic kidney disease in people with Type 2 diabetes mellitus, a nationwide longitudinal cohort study. Diabet. Med. 2015, 32, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Mantravadi, S.; George, M.; Brensinger, C.; Du, M.; Baker, J.F.; Ogdie, A. Impact of tumor necrosis factor inhibitors and methotrexate on diabetes mellitus among patients with inflammatory arthritis. BMC Rheumatol. 2020, 4, 39. [Google Scholar] [CrossRef] [PubMed]
- Stagakis, I.; Bertsias, G.; Karvounaris, S.; Kavousanaki, M.; Virla, D.; Raptopoulou, A.; Kardassis, D.; Boumpas, D.T.; Sidiropoulos, P.I. Anti-tumor necrosis factor therapy improves insulin resistance, beta cell function and insulin signaling in active rheumatoid arthritis patients with high insulin resistance. Arthritis Res. Ther. 2012, 14, R141. [Google Scholar] [CrossRef] [PubMed]
- Corrado, A.; Colia, R.; Rotondo, C.; Sanpaolo, E.; Cantatore, F.P. Changes in serum adipokines profile and insulin resistance in patients with rheumatoid arthritis treated with anti-TNF-α. Curr. Med. Res. Opin. 2019, 35, 2197–2205. [Google Scholar] [CrossRef]
- Gupta-Ganguli, M.; Cox, K.; Means, B.; Gerling, I.; Solomon, S.S. Does therapy with anti-TNF-alpha improve glucose tolerance and control in patients with type 2 diabetes? Diabetes Care 2011, 34, e121. [Google Scholar] [CrossRef] [PubMed]
- Kimball, A.B.; Bensimon, A.G.; Guerin, A.; Yu, A.P.; Wu, E.Q.; Okun, M.M.; Bao, Y.; Gupta, S.R.; Mulani, P.M. Efficacy and safety of adalimumab among patients with moderate to severe psoriasis with comorbidities: Subanalysis of results from a randomized, double-blind, placebo-controlled, phase III trial. Am. J. Clin. Dermatol. 2011, 12, 51–62. [Google Scholar] [CrossRef]
- Da Silva, B.S.; Bonfá, E.; de Moraes, J.C.; Saad, C.G.; Ribeiro, A.C.; Gonçalves, C.R.; de Carvalho, J.F. Effects of anti-TNF therapy on glucose metabolism in patients with ankylosing spondylitis, psoriatic arthritis or juvenile idiopathic arthritis. Biologicals 2010, 38, 567–569. [Google Scholar] [CrossRef]
- Collotta, D.; Hull, W.; Mastrocola, R.; Chiazza, F.; Cento, A.S.; Murphy, C.; Verta, R.; Alves, G.F.; Gaudioso, G.; Fava, F.; et al. Baricitinib counteracts metaflammation, thus protecting against diet-induced metabolic abnormalities in mice. Mol. Metab. 2020, 39, 101009. [Google Scholar] [CrossRef]
- Egeberg, A.; Wu, J.J.; Korman, N.; Solomon, J.A.; Goldblum, O.; Zhao, F.; Mallbris, L. Ixekizumab treatment shows a neutral impact on cardiovascular parameters in patients with moderate-to-severe plaque psoriasis: Results from UNCOVER-1, UNCOVER-2, and UNCOVER-3. J. Am. Acad. Dermatol. 2018, 79, 104–109.e8. [Google Scholar] [CrossRef]
- Frieder, J.; Kivelevitch, D.; Menter, A. Secukinumab: A review of the anti-IL-17A biologic for the treatment of psoriasis. Ther. Adv. Chronic. Dis. 2018, 9, 5–21. [Google Scholar] [CrossRef]
- Ohshima, K.; Mogi, M.; Jing, F.; Iwanami, J.; Tsukuda, K.; Min, L.J.; Higaki, J.; Horiuchi, M. Roles of interleukin 17 in angiotensin II type 1 receptor-mediated insulin resistance. Hypertension. 2012, 59, 493–499. [Google Scholar] [CrossRef]
- Di Minno, M.N.; Peluso, R.; Iervolino, S.; Russolillo, A.; Lupoli, R.; Scarpa, R. CaRRDs Study Group. Weight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor α blockers. Ann. Rheum. Dis. 2014, 73, 1157–1162. [Google Scholar] [CrossRef]
- Klingberg, E.; Björkman, S.; Eliasson, B.; Larsson, I.; Bilberg, A. Weight loss is associated with sustained improvement of disease activity and cardiovascular risk factors in patients with psoriatic arthritis and obesity: A prospective intervention study with two years of follow-up. Arthritis Res. Ther. 2020, 22, 254. [Google Scholar] [CrossRef]
- Huizinga, T.; Nigrovic, P.; Ruderman, E.; Schulze-Koops, H. Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis: Commentary. Int. J. Adv. Rheumatol. 2011, 9, 143. [Google Scholar]
- Ogdie, A.; Shin, D.B.; Love, T.J.; Gelfand, J.M. Body surface area affected by psoriasis and the risk for psoriatic arthritis: A prospective population-based cohort study. Rheumatology 2022, 61, 1877–1884. [Google Scholar] [CrossRef]
- Lowe, N.J.; Lazarus, V.; Matt, L. Systemic retinoid therapy for psoriasis. J. Am. Acad. Dermatol. 1988, 19, 186–191. [Google Scholar] [CrossRef]
- Thrasher, J. Pharmacologic Management of Type 2 Diabetes Mellitus: Available Therapies. Am. J. Med. 2017, 130, S4–S17. [Google Scholar] [CrossRef]
- Kessler, J.; Chouk, M.; Ruban, T.; Prati, C.; Wendling, D.; Verhoeven, F. Psoriatic arthritis and physical activity: A systematic review. Clin. Rheumatol. 2021, 40, 4379–4389. [Google Scholar] [CrossRef]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2014, 37 (Suppl. S1), S120–S143. [Google Scholar] [CrossRef]
- Abou-Raya, A.; Abou-Raya, S.; Helmii, M. SAT0384. Metformin: A Valid ADD-ON Drug in the Treatment of Psoriatic Arthritis—Randomized Controlled Trial. Ann. Rheum. Dis. 2014, 73, 733. Available online: https://ard.bmj.com/content/73/Suppl_2/733.1 (accessed on 23 March 2023). [CrossRef]
- Kooy, A.; de Jager, J.; Lehert, P.; Bets, D.; Wulffelé, M.G.; Donker, A.J.; Stehouwer, C.D. Long-term effects of metformin on metabolism and microvascular and macrovascular disease in patients with type 2 diabetes mellitus. Arch. Intern. Med. 2009, 169, 616–625. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Ørsted, D.D.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Tornøe, K.; Zinman, B.; Buse, J.B. LEADER Steering Committee and Investigators. Liraglutide and Renal Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 839–848. [Google Scholar] [CrossRef]
- Keser, M.; Cetin, P.; Solmaz, D.; Kozacı, D.; Gunay, N.; Oztürk, S.; Sarı, I.; Akar, S.; Birlik, M.; Akkoc, N.; et al. AB0744 There is NO Relationship between Glucagon like Peptide-1 and Inflammation in Psoriasis and Psoriatic Arthritis. Ann. Rheum. Dis. 2014, 73, 1049–1050. [Google Scholar] [CrossRef]
- Faurschou, A.; Gyldenløve, M.; Rohde, U.; Thyssen, J.P.; Zachariae, C.; Skov, L.; Knop, F.K.; Vilsbøll, T. Lack of effect of the glucagon-like peptide-1 receptor agonist liraglutide on psoriasis in glucose-tolerant patients—A randomized placebo-controlled trial. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.E.; Tobin, A.M.; Ahern, T.; Corrigan, M.A.; Gaoatswe, G.; Jackson, R.; O’reilly, V.; Lynch, L.; Doherty, D.G.; Moynagh, P.N.; et al. Glucagon-like peptide-1 (GLP-1) and the regulation of human invariant natural killer T cells: Lessons from obesity, diabetes and psoriasis. Diabetologia 2011, 54, 2745–2754. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, G.; Curatolo, S.; Busà, B.; Belfiore, A.; Gullo, D. Two birds one stone: Semaglutide is highly effective against severe psoriasis in a type 2 diabetic patient. Endocrinol. Diabetes Metab. Case Rep. 2021, 2021, 21-0007. [Google Scholar] [CrossRef]
- Andreea, M.M.; Surabhi, S.; Razvan-Ionut, P.; Lucia, C.; Camelia, N.; Emil, T.; Tiberiu, N.I. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors: Harms or Unexpected Benefits? Medicina 2023, 59, 742. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.J.; Wie, J.C.; Liu, Y.T.; Lin, C.H.; Lin, C.C.; Chen, H.H. Association between α-glucosidase inhibitor use and psoriatic disease risk in patients with type 2 diabetes mellitus: A population-based cohort study. Int. J. Clin. Pract. 2021, 75, e14819. [Google Scholar] [CrossRef]
- Smith, U. Pioglitazone: Mechanism of action. Int. J. Clin. Pract. Suppl. 2001, 121, 13–18. [Google Scholar]
- Bongartz, T.; Coras, B.; Vogt, T.; Schölmerich, J.; Müller-Ladner, U. Treatment of active psoriatic arthritis with the PPARgamma ligand pioglitazone: An open-label pilot study. Rheumatology 2005, 44, 126–129. [Google Scholar] [CrossRef]
- Cernea, S.; Raz, I. Insulin Therapy: Future Perspectives. Am. J. Ther. 2020, 27, e121–e132. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 4, 851–863. [Google Scholar] [CrossRef]
- Chang, S.C.; Yang, W.V. Hyperglycemia, tumorigenesis, and chronic inflammation. Crit. Rev. Oncol. Hematol. 2016, 108, 146–153. [Google Scholar] [CrossRef]
- Meigs, J.B.; Rutter, M.K.; Sullivan, L.M.; Fox, C.S.; D’Agostino, R.B.; Wilson, P.W.F. Impact of insulin resistance on risk of type 2 diabetes and cardiovascular. Diabetes Care 2007, 30, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef] [PubMed]
- Caso, F.; Navarini, L.; Carubbi, F.; Picchianti-Diamanti, A.; Chimenti, M.S.; Tasso, M.; Currado, D.; Ruscitti, P.; Ciccozzi, M.; Annarumma, A. Mediterranean diet and Psoriatic Arthritis activity: A multicenter cross-sectional study. Rheumatol. Int. 2020, 40, 951–958. [Google Scholar] [CrossRef]
- Esposito, K.; Giugliano, D. Mediterranean diet and type 2 diabetes. Diabetes Metab. Res. Rev. 2014, 30 (Suppl. S1), 34–40. [Google Scholar] [CrossRef]
- Hamasaki, H. Daily physical activity and type 2 diabetes: A review. World J. Diabetes 2016, 7, 243–251. [Google Scholar] [CrossRef]
- Sargeant, L.A.; Khaw, K.T.; Bingham, S.; Day, N.E.; Luben, R.N.; Oakes, S.; Welch, A.; Wareham, N.J. Cigarette smoking and glycaemia: The EPIC-Norfolk Study. European Prospective Investigation into Cancer. Int. J. Epidemiol. 2001, 30, 547–554. [Google Scholar] [CrossRef]
- Maddatu, J.; Anderson-Baucum, E.; Evans-Molina, C. Smoking and the risk of type 2 diabetes. Transl. Res. 2017, 184, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Debbaneh, M.; Moslehi, H.; Koo, J.; Liao, W. Tonsillectomy as a treatment for psoriasis: A review. J. Dermatolog. Treat. 2014, 25, 482–486. [Google Scholar] [CrossRef]
- Nijakowski, K.; Gruszczyński, D.; Kolasińska, J.; Kopała, D.; Surdacka, A. Periodontal Disease in Patients with Psoriasis: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 11302. [Google Scholar] [CrossRef]
- Vasey, F.B.; Deitz, C.; Fenske, N.A.; Germain, B.F.; Espinoza, L.R. Possible involvement of group A streptococci in the pathogenesis of psoriatic arthritis. J. Rheumatol. 1982, 9, 719–722. [Google Scholar]
- Dalmády, S.; Kemény, L.; Antal, M.; Gyulai, R. Periodontitis: A newly identified comorbidity in psoriasis and psoriatic arthritis. Expert Rev. Clin. Immunol. 2020, 16, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Rousset, L.; Halioua, B. Stress and psoriasis. Int. J. Dermatol. 2018, 57, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J.; Wheeler, E.; Light, T.; Skillings, A.; Scharf, M.J.; Cropley, T.G.; Hosmer, D.; Bernhard, J.D. Influence of a mindfulness meditation-based stress reduction intervention on rates of skin clearing in patients with moderate to severe psoriasis undergoing phototherapy (UVB) and photochemotherapy (PUVA). Psychosom. Med. 1998, 60, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Tausk, F.; Whitmore, S.E. A pilot study of hypnosis in the treatment of patients with psoriasis. Psychother. Psychosom. 1999, 68, 221–225. [Google Scholar] [CrossRef] [PubMed]


| Treatment of Diabetes Mellitus Type 2 in PsA Patients | |||
|---|---|---|---|
| Type of Therapy | Drug/ Management | Characteristics of Management | Reference |
| non-pharmacological management | personalized management |
| [67,73,74] |
| metabolic parameters |
| [73,74,94,95,97,98] | |
| ↓ stress level |
| [97,102,103,104] | |
| pharmacological oral hypoglycemic therapy | metformin |
| [71,72,73,74,75,76] |
| GLP-1 |
| [77,78,79,82,83,84] | |
| SGLT2 inhibitors |
| [72,85] | |
| AGIs |
| [86] | |
| pioglitazone |
| [87,88] | |
| insulin therapy |
| [89] | |
| other therapies | heart and vessel diseases |
| [16,36,64,68,72,77,78,92] |
| infection |
| [99,100,101,102] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grygiel-Górniak, B.; Skoczek, W. Molecular Background and Clinical Implications of Glucose Disorders in Patients with Psoriatic Arthritis. J. Clin. Med. 2023, 12, 5814. https://doi.org/10.3390/jcm12185814
Grygiel-Górniak B, Skoczek W. Molecular Background and Clinical Implications of Glucose Disorders in Patients with Psoriatic Arthritis. Journal of Clinical Medicine. 2023; 12(18):5814. https://doi.org/10.3390/jcm12185814
Chicago/Turabian StyleGrygiel-Górniak, Bogna, and Weronika Skoczek. 2023. "Molecular Background and Clinical Implications of Glucose Disorders in Patients with Psoriatic Arthritis" Journal of Clinical Medicine 12, no. 18: 5814. https://doi.org/10.3390/jcm12185814