

High Myopia Prevalence across Racial Groups in the United States: A Systematic Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Quality Assessment
2.2. Inclusion and Exclusion Criteria
2.3. Assessment of Study Quality
2.4. Data Extraction and Synthesis
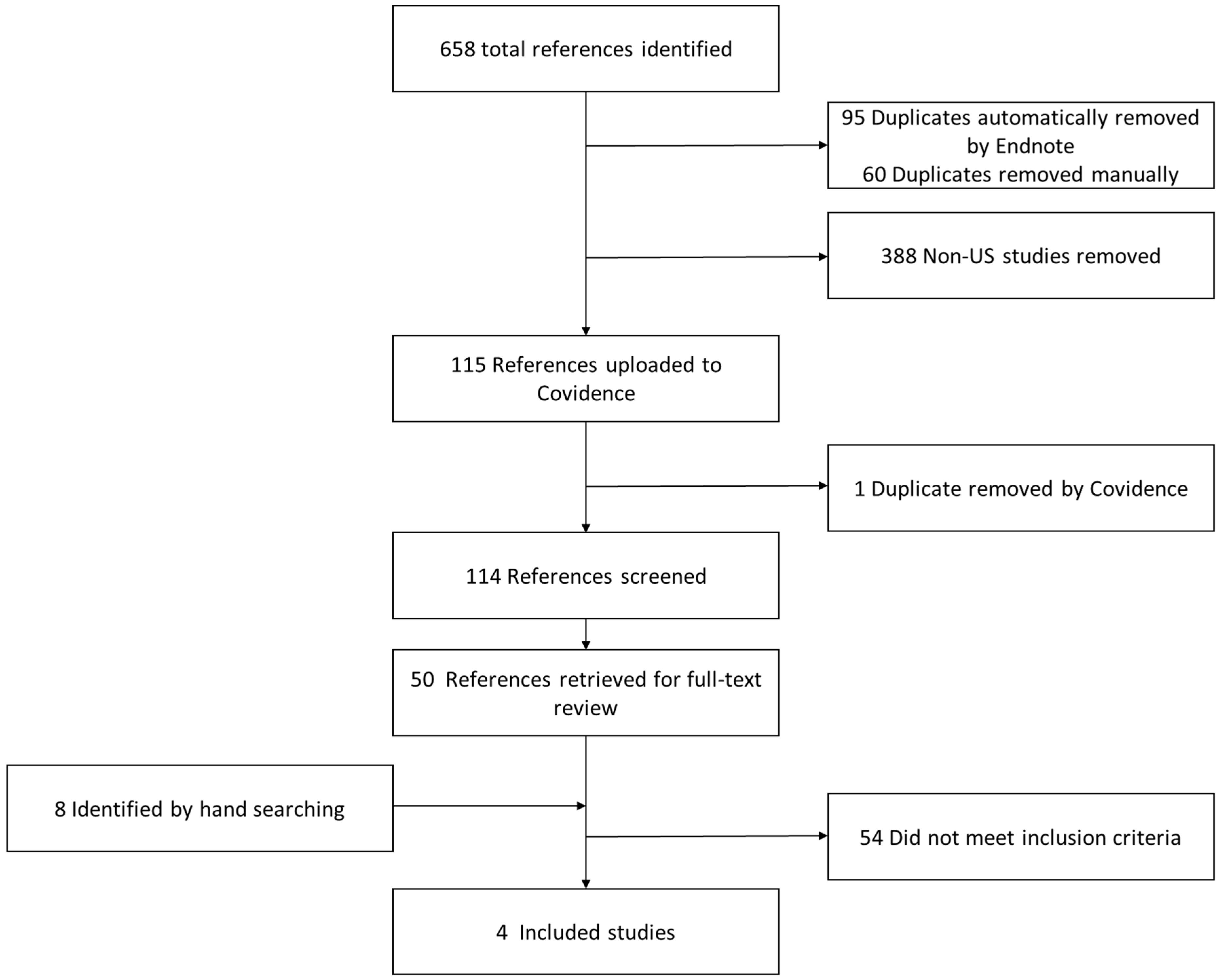
3. Results
Data Synthesis
4. Discussion
4.1. The Paucity of Data and High Degree of Variability
4.2. The Public Health Problem
4.3. Myopia’s Impact on Education and Learning
4.4. Treatment for Myopia Control
4.5. Curb Myopia Progression through Public Health Initiatives
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global Causes of Blindness and Distance Vision Impairment 1990–2020: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [PubMed]
- Rhee, M.K. Update on Myopia Control: The US Perspective. Eye Contact Lens 2022, 48, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef]
- Meng, W.; Butterworth, J.; Malecaze, F.; Calvas, P. Axial Length of Myopia: A Review of Current Research. Ophthalmologica 2011, 225, 127–134. [Google Scholar] [CrossRef]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.-M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Myopia, J.; Mariotti, S.; Kocur, I.; Resnikoff, S.; Mingguang, H.; Naidoo, K.; He, M.; Holden, B.; Salomão, S.; Sankaridurg, P.; et al. The Impact of Myopia and High Myopia. Report of the Joint World Health Organization-Brien Holden Vision Institute Global Scientific Meeting on Myopia; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Vitale, S.; Sperduto, R.D.; Ferris, F.L., 3rd. Increased Prevalence of Myopia in the United States between 1971–1972 and 1999–2004. Arch. Ophthalmol. 2009, 127, 1632–1639. [Google Scholar] [CrossRef]
- Willis, J.R.; Vitale, S.; Morse, L.; Parke, D.W., 2nd; Rich, W.L.; Lum, F.; Cantrell, R.A. The Prevalence of Myopic Choroidal Neovascularization in the United States: Analysis of the IRIS® Data Registry and NHANES. Ophthalmology 2016, 123, 1771–1782. [Google Scholar] [CrossRef]
- Zhang, X.; Cotch, M.F.; Ryskulova, A.; Primo, S.A.; Nair, P.; Chou, C.-F.; Geiss, L.S.; Barker, L.E.; Elliott, A.F.; Crews, J.E.; et al. Vision Health Disparities in the United States by Race/Ethnicity, Education, and Economic Status: Findings from Two Nationally Representative Surveys. Am. J. Ophthalmol. 2012, 154, S53–S62. [Google Scholar] [CrossRef]
- Zhang, X.; Beckles, G.L.; Chou, C.-F.; Saaddine, J.B.; Wilson, M.R.; Lee, P.P.; Parvathy, N.; Ryskulova, A.; Geiss, L.S. Socioeconomic Disparity in Use of Eye Care Services Among US Adults With Age-Related Eye Diseases: National Health Interview Survey, 2002 and 2008. JAMA Ophthalmol. 2013, 131, 1198–1206. [Google Scholar] [CrossRef]
- Williams, D.R.; Priest, N.; Anderson, N.B. Understanding Associations among Race, Socioeconomic Status, and Health: Patterns and Prospects. Health Psychol. 2016, 35, 407–411. [Google Scholar] [CrossRef]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K.; Rahi, J.; Resnikoff, S.; Vitale, S.; Yannuzzi, L. IMI–Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Ophthalmol. Vis. Sci. 2019, 60, M20–M30. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Impact of Myopia and High Myopia; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Katz, J.; Tielsch, J.M.; Sommer, A. Prevalence and Risk Factors for Refractive Errors in an Adult Inner City Population. Investig. Ophthalmol. Vis. Sci. 1997, 38, 334–340. [Google Scholar]
- Varma, R.; Torres, M.; McKean-Cowdin, R.; Rong, F.; Hsu, C.; Jiang, X. Prevalence and Risk Factors for Refractive Error in Adult Chinese Americans: The Chinese American Eye Study. Am. J. Ophthalmol. 2017, 175, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Shimada, N.; Ohno-Matsui, K.; Nishimuta, A.; Tokoro, T.; Mochizuki, M. Peripapillary Changes Detected by Optical Coherence Tomography in Eyes with High Myopia. Ophthalmology 2007, 114, 2070–2076. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Pan, C.-W.; Klein, B.E.K.; Cotch, M.F.; Shrager, S.; Klein, R.; Folsom, A.; Kronmal, R.; Shea, S.J.; Burke, G.L.; Saw, S.-M.; et al. Racial Variations in the Prevalence of Refractive Errors in the United States: The Multi-Ethnic Study of Atherosclerosis. Am. J. Ophthalmol. 2013, 155, 1129–1138.e1. [Google Scholar] [CrossRef]
- Tarczy-Hornoch, K.; Ying-Lai, M.; Varma, R. Myopic Refractive Error in Adult Latinos: The Los Angeles Latino Eye Study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1845–1852. [Google Scholar] [CrossRef]
- Turbert, D.; Puente, M.A., Jr. Nearsightedness: What Is Myopia? American Academy of Ophthalmology: San Francisco, CA, USA, 2022. [Google Scholar]
- Scott, C. Progressive (High) Myopia; American Association for Pediatric Ophthalmology & Strabismus: 2021. Available online: https://aapos.org/glossary/progressive-high-myopia (accessed on 8 February 2023).
- Sankaridurg, P.; Tahhan, N.; Kandel, H.; Naduvilath, T.; Zou, H.; Frick, K.D.; Marmamula, S.; Friedman, D.S.; Lamoureux, E.; Keeffe, J.; et al. IMI Impact of Myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2. [Google Scholar] [CrossRef]
- Leveziel, N.; Marillet, S.; Dufour, Q.; Lichtwitz, O.; Bentaleb, Y.; Pelen, F.; Ingrand, P.; Bourne, R. Prevalence of Macular Complications Related to Myopia—Results of a Multicenter Evaluation of Myopic Patients in Eye Clinics in France. Acta Ophthalmol. 2020, 98, e245–e251. [Google Scholar] [CrossRef]
- US Census Bureau QuickFacts: United States; 2020. Available online: http://www.census.gov/quickfacts/US (accessed on 8 February 2023).
- US Census Bureau 2018 Population Survey. Available online: https://www.census.gov/programs-surveys/acs/news/updates/2018.html (accessed on 8 February 2023).
- Budimen, A. Key Facts about Asian Americans, a Diverse and Growing Population; Pew Research Center: Washington, DC, USA, 2021. [Google Scholar]
- Theophanous, C.; Modjtahedi, B.S.; Batech, M.; Marlin, D.S.; Luong, T.Q.; Fong, D.S. Myopia Prevalence and Risk Factors in Children. Clin. Ophthalmol. 2018, 12, 1581–1587. [Google Scholar] [CrossRef]
- Kemper, A.R.; Cohn, L.M.; Dombkowski, K.J. Patterns of Vision Care among Medicaid-Enrolled Children. Pediatrics 2004, 113, e190–e196. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Deneen, J.; Cotter, S.; Paz, S.H.; Azen, S.P.; Tarczy-Hornoch, K.; Zhao, P. The Multi-Ethnic Pediatric Eye Disease Study: Design and Methods. Ophthalmic Epidemiol. 2006, 13, 253–262. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Fast Facts about Vision Loss; Vision Health Initiative (VHI), 2020.
- Sarah, S.; Alex, H. A Third of Students Need Eye Exams, Study Finds; Education Week Research Center, 2018. Available online: https://www.edweek.org/leadership/a-third-of-students-need-eye-exams-study-finds/2018/05 US (accessed on 8 February 2023).
- Ciner, E.B.; Schmidt, P.P.; Orel-Bixler, D.; Dobson, V.; Maguire, M.; Cyert, L.; Moore, B.; Schultz, J. Vision Screening of Preschool Children: Evaluating the Past, Looking toward the Future. Optom. Vis. Sci. 1998, 75, 571–584. [Google Scholar] [CrossRef] [PubMed]
- White, S.L.J.; Wood, J.M.; Black, A.A.; Hopkins, S. Vision Screening Outcomes of Grade 3 Children in Australia: Differences in Academic Achievement. Int. J. Educ. Res. 2017, 83, 154–159. [Google Scholar] [CrossRef]
- Cornelissen, P.; Bradley, L.; Fowler, S.; Stein, J. What Children See Affects How They Read. Dev. Med. Child Neurol. 1991, 33, 755–762. [Google Scholar] [CrossRef]
- Kulp, M.T.; Ciner, E.; Maguire, M.; Moore, B.; Pentimonti, J.; Pistilli, M.; Cyert, L.; Candy, T.R.; Quinn, G.; Ying, G.-S. Uncorrected Hyperopia and Preschool Early Literacy: Results of the Vision in Preschoolers-Hyperopia in Preschoolers (VIP-HIP) Study. Ophthalmology 2016, 123, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Rosner, J.; Rosner, J. The Relationship between Moderate Hyperopia and Academic Achievement: How Much plus Is Enough? J. Am. Optom. Assoc. 1997, 68, 648–650. [Google Scholar]
- Williams, W.R.; Latif, A.H.A.; Hannington, L.; Watkins, D.R. Hyperopia and Educational Attainment in a Primary School Cohort. Arch. Dis. Child. 2005, 90, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, A.J.; Wolf, B.; Guo, X.; Shakarchi, A.F.; Madden, N.A.; Repka, M.X.; Friedman, D.S.; Collins, M.E. Effect of a Randomized Interventional School-Based Vision Program on Academic Performance of Students in Grades 3 to 7: A Cluster Randomized Clinical Trial. JAMA Ophthalmol. 2021, 139, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Recko, M.; Stahl, E.D. Childhood Myopia: Epidemiology, Risk Factors, and Prevention. Mo. Med. 2015, 112, 116–121. [Google Scholar] [PubMed]
- Lanca, C.; Saw, S.-M. The Association between Digital Screen Time and Myopia: A Systematic Review. Ophthalmic Physiol. Opt. 2020, 40, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Walline, J.J.; Walker, M.K.; Mutti, D.O.; Jones-Jordan, L.A.; Sinnott, L.T.; Giannoni, A.G.; Bickle, K.M.; Schulle, K.L.; Nixon, A.; Pierce, G.E.; et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA 2020, 324, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Anstice, N.S.; Phillips, J.R. Effect of Dual-Focus Soft Contact Lens Wear on Axial Myopia Progression in Children. Ophthalmology 2011, 118, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Cheung, S.-W. Retardation of Myopia in Orthokeratology (ROMIO) Study: A 2-Year Randomized Clinical Trial. Investig. Ophthalmol. Vis. Sci. 2012, 53, 7077–7085. [Google Scholar] [CrossRef]
- VanderVeen, D.K.; Kraker, R.T.; Pineles, S.L.; Hutchinson, A.K.; Wilson, L.B.; Galvin, J.A.; Lambert, S.R. Use of Orthokeratology for the Prevention of Myopic Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology 2019, 126, 623–636. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.Y.; Lam, C.S.Y.; Tang, W.C.; Leung, M.; To, C.H. Defocus Incorporated Multiple Segments Spectacle Lenses Changed the Relative Peripheral Refraction: A 2-Year Randomized Clinical Trial. Investig. Ophthalmol. Vis. Sci. 2020, 61, 53. [Google Scholar] [CrossRef]
- Kanda, H.; Oshika, T.; Hiraoka, T.; Hasebe, S.; Ohno-Matsui, K.; Ishiko, S.; Hieda, O.; Torii, H.; Varnas, S.R.; Fujikado, T. Effect of Spectacle Lenses Designed to Reduce Relative Peripheral Hyperopia on Myopia Progression in Japanese Children: A 2-Year Multicenter Randomized Controlled Trial. Jpn. J. Ophthalmol. 2018, 62, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.; Lu, Q.-S.; Tan, D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016, 123, 391–399. [Google Scholar] [CrossRef]
- Chia, A.; Chua, W.-H.; Cheung, Y.-B.; Wong, W.-L.; Lingham, A.; Fong, A.; Tan, D. Atropine for the Treatment of Childhood Myopia: Safety and Efficacy of 0.5%, 0.1%, and 0.01% Doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012, 119, 347–354. [Google Scholar] [CrossRef]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef]
- Wu, P.-C.; Chen, C.-T.; Chang, L.-C.; Niu, Y.-Z.; Chen, M.-L.; Liao, L.-L.; Rose, K.; Morgan, I.G. Increased Time Outdoors Is Followed by Reversal of the Long-Term Trend to Reduced Visual Acuity in Taiwan Primary School Students. Ophthalmology 2020, 127, 1462–1469. [Google Scholar] [CrossRef] [PubMed]
- Fricke, T.R.; Sankaridurg, P.; Naduvilath, T.; Resnikoff, S.; Tahhan, N.; He, M.; Frick, K.D. Establishing a Method to Estimate the Effect of Antimyopia Management Options on Lifetime Cost of Myopia. Br. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Modjtahedi, B.S.; Abbott, R.L.; Fong, D.S.; Lum, F.; Tan, D. Reducing the Global Burden of Myopia by Delaying the Onset of Myopia and Reducing Myopic Progression in Children: The Academy’s Task Force on Myopia. Ophthalmology 2021, 128, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Wahl, M.D.; Fishman, D.; Block, S.S.; Baldonado, K.N.; Friedman, D.S.; Repka, M.X.; Collins, M.E. A Comprehensive Review of State Vision Screening Mandates for Schoolchildren in the United States. Optom. Vis. Sci. 2021, 98, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Helen, C. “Oh, That’s an Idea”: US Parents Respond to China Screen Time Ban. 2021. Available online: https://www.reuters.com/world/china/oh-thats-an-idea-us-parents-respond-china-screen-time-ban-2021-08-31/ (accessed on 8 February 2023).
- Ong, E.H.H.; Lim, J.Z.M.; Conceicao, J.F.; Tang, S.F.S.L. Seek Singapore: Stop the Eye Epidemic in Kids. 2015. Available online: https://blogs.ntu.edu.sg/wkwsci-fyp-collection/2016/05/30/seek-singapore-stop-the-eye-epidemic-in-kids-2/ (accessed on 8 February 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Dataset/ Study | Number of Participants | Study Publication Year | Data Collection Year | Study Population | Racial Groups | High Myopia Definition | High Myopia Prevalence |
|---|---|---|---|---|---|---|---|---|
| Varma, et al. [15] | The Chinese American Eye Study (CHES) | 4582 eyes | 2016 | 2009–2013 | Residents in ten census tracts in Monterey Park, California Age 50 or older | Self-identified Chinese Americans | ≤−5.0D | Chinese—8.60% |
| Pan, et al. [18] | Multi-Ethnic Study of Atherosclerosis (MESA) | 4430 eyes | 2013 | 2002–2004 | Prospective cohort study sampled from: Baltimore, Maryland; Chicago, Illinois; Forsyth County, North Carolina; Los Angeles, California; New York, New York; and St Paul, Minnesota restricted to adults without known cardiovascular disease Age 45–84 years old | Self-identified: Black—1230 (27.8%) Chinese—487 (11%) Hispanic—1046 (23.6%) White—1667 (37.6%) | ≤−5.0D | Black—3.1% Chinese—11.8% Hispanic—1.8% White—5.4% |
| Tarczy-Hornoch, et al. [19] | Los Angeles Latino Eye Study (LALES) | 5396 eyes | 2006 | 2000–2003 | Residents in six census tracts in La Puente, California Age 40 or older | Self-identified Latino ethnicity | ≤−5.0D | Hispanic—2.40% |
| Katz, et al. [14] | Baltimore Eye Survey (BES) | 4859 eyes | 1996 | 1985–1988 | Population- based sample survey in Baltimore Age 40 or older | Self-identified: Black—2200 (45%) White—2659 (55%) | ≤−6.0D | Black—0.9% White—1.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banashefski, B.; Rhee, M.K.; Lema, G.M.C. High Myopia Prevalence across Racial Groups in the United States: A Systematic Scoping Review. J. Clin. Med. 2023, 12, 3045. https://doi.org/10.3390/jcm12083045
Banashefski B, Rhee MK, Lema GMC. High Myopia Prevalence across Racial Groups in the United States: A Systematic Scoping Review. Journal of Clinical Medicine. 2023; 12(8):3045. https://doi.org/10.3390/jcm12083045
Chicago/Turabian StyleBanashefski, Bryana, Michelle K. Rhee, and Gareth M. C. Lema. 2023. "High Myopia Prevalence across Racial Groups in the United States: A Systematic Scoping Review" Journal of Clinical Medicine 12, no. 8: 3045. https://doi.org/10.3390/jcm12083045