
Therapeutic Strategies to Prevent the Recurrence of Nasal Polyps after Surgical Treatment: An Update and In Vitro Study on Growth Inhibition of Fibroblasts
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Update of Molecules Used to Prevent Nasal Polyp Recurrences
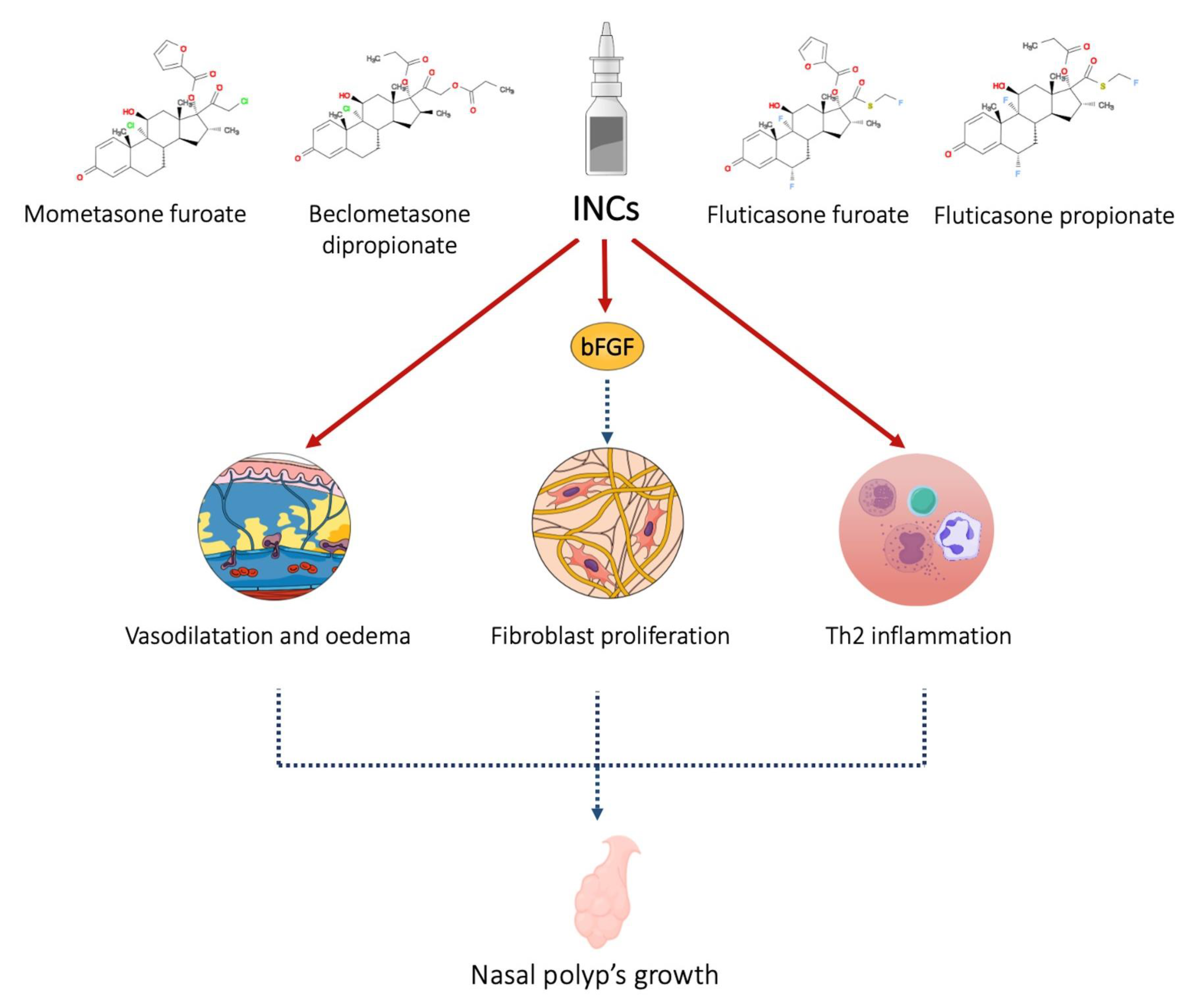
2.1. Intranasal Corticosteroids (INCs)
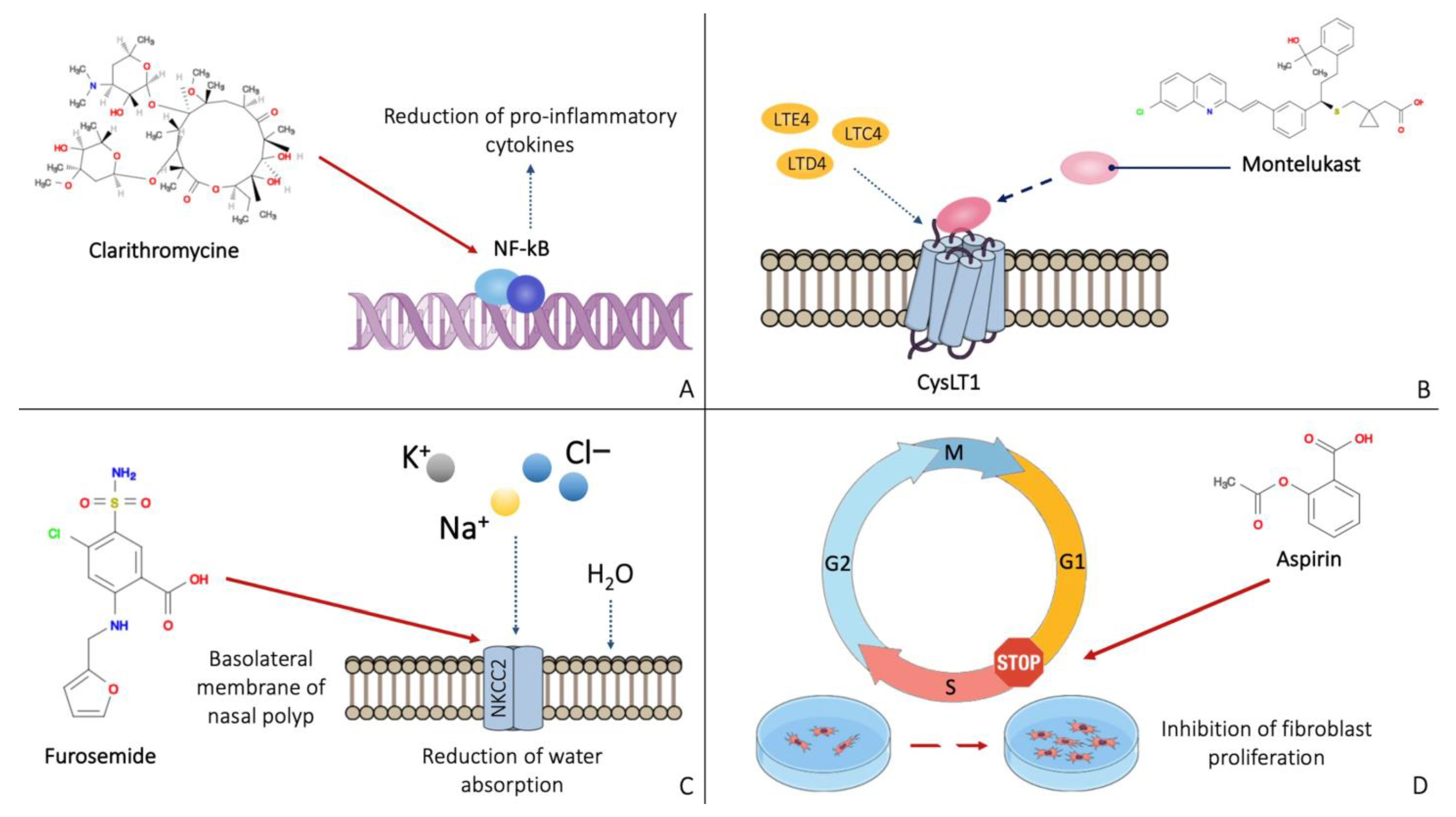
2.2. Acetylsalicylic Acid and Other NSAIDs
2.3. Furosemide
2.4. Antibiotics and Antifungal Drugs
2.5. Other Therapeutical Strategies
2.6. Biological Therapies
3. Methods
3.1. Study Design and Protocol
3.2. Skin-Prick Tests (SPTs)
3.3. Endoscopic Evaluation and Tomographic Score
3.4. Sino-Nasal Outcome Test (SNOT-22)
3.5. Tissue Samples and Cells
3.6. Statistical Analysis
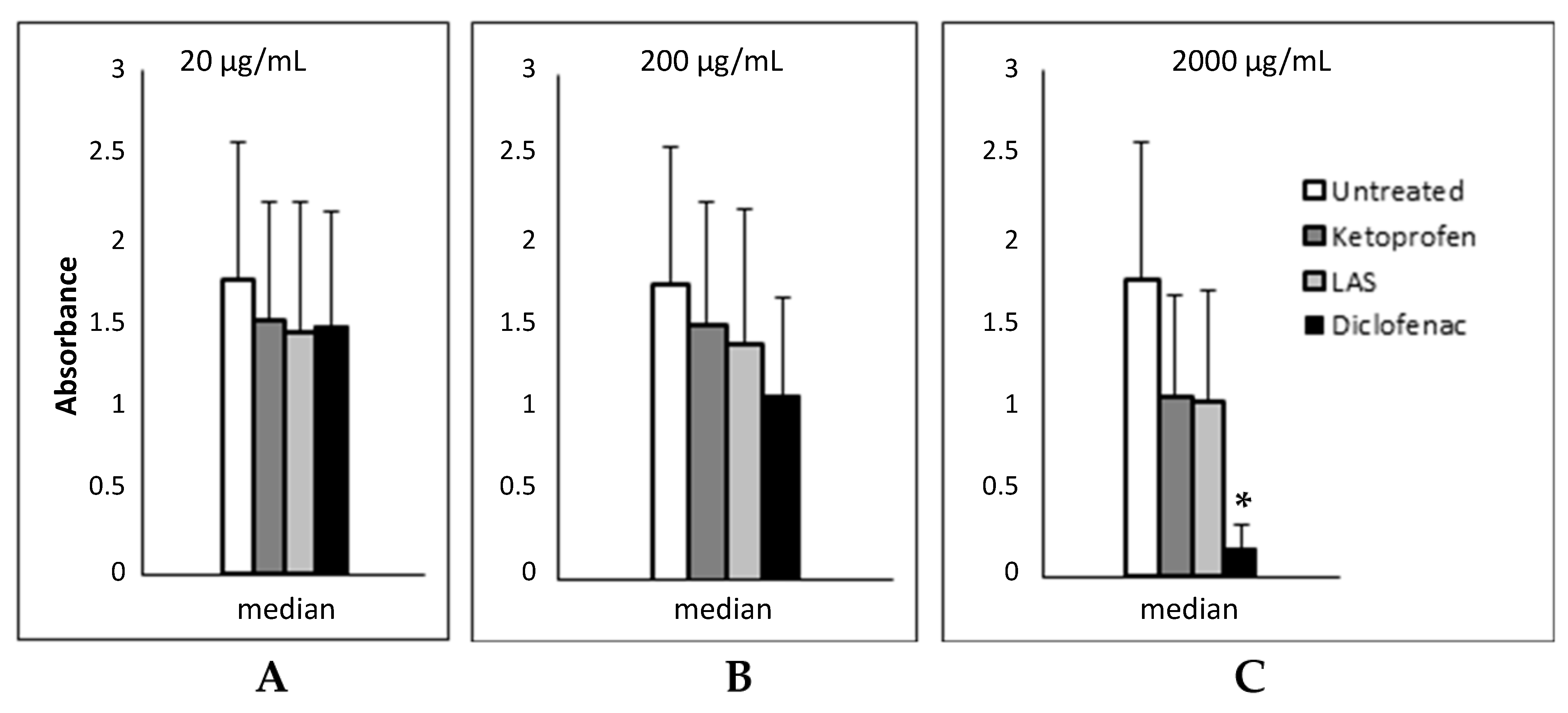
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hopkins, C. Chronic Rhinosinusitis with Nasal Polyps. N. Engl. J. Med. 2019, 381, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Brescia, G.; Zanotti, C.; Parrino, D.; Barion, U.; Marioni, G. Nasal Polyposis Pathophysiology: Endotype and Phenotype Open Issues. Am. J. Otolaryngol. 2018, 39, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Hulse, K.E.; Stevens, W.W.; Tan, B.K.; Schleimer, R.P. Pathogenesis of Nasal Polyposis. Clin. Exp. Allergy 2015, 45, 328–346. [Google Scholar] [CrossRef] [Green Version]
- Van Zele, T.; Claeys, S.; Gevaert, P.; Van Maele, G.; Holtappels, G.; Van Cauwenberge, P.; Bachert, C. Differentiation of Chronic Sinus Diseases by Measurement of Inflammatory Mediators. Allergy 2006, 61, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.; Baxter, B.; Campbell, B.C.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A. Multisociety consensus quality improvement revised consensus statement for endovascular therapy of acute ischemic stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef] [Green Version]
- Schleimer, R.P. Immunopathogenesis of Chronic Rhinosinusitis and Nasal Polyposis. Annu. Rev. Pathol. 2017, 12, 331–357. [Google Scholar] [CrossRef] [Green Version]
- Settipane, G.A.; Chafee, F.H. Nasal Polyps in Asthma and Rhinitis. A Review of 6,037 Patients. J. Allergy Clin. Immunol. 1977, 59, 17–21. [Google Scholar] [CrossRef]
- Chong, L.Y.; Head, K.; Hopkins, C.; Philpott, C.; Burton, M.J.; Schilder, A.G.M. Different Types of Intranasal Steroids for Chronic Rhinosinusitis. Cochrane Database Syst. Rev. 2016, 4, CD011993. [Google Scholar] [CrossRef] [Green Version]
- Patel, G.B.; Peters, A.T. The Role of Biologics in Chronic Rhinosinusitis With Nasal Polyps. Ear Nose Throat J. 2021, 100, 44–47. [Google Scholar] [CrossRef]
- Effect of Subcutaneous Dupilumab on Nasal Polyp Burden in Patients with Chronic Sinusitis and Nasal Polyposis: A Randomized Clinical Trial-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26836729/ (accessed on 15 February 2023).
- Gevaert, P.; Calus, L.; Van Zele, T.; Blomme, K.; De Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; De Bacquer, D.; van Cauwenberge, P.; et al. Omalizumab Is Effective in Allergic and Nonallergic Patients with Nasal Polyps and Asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e1. [Google Scholar] [CrossRef] [PubMed]
- Gevaert, P.; Van Bruaene, N.; Cattaert, T.; Van Steen, K.; Van Zele, T.; Acke, F.; De Ruyck, N.; Blomme, K.; Sousa, A.R.; Marshall, R.P.; et al. Mepolizumab, a Humanized Anti-IL-5 MAb, as a Treatment Option for Severe Nasal Polyposis. J. Allergy Clin. Immunol. 2011, 128, 989–995.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galluzzi, F.; Pignataro, L.; Maddalone, M.; Garavello, W. Recurrences of Surgery for Antrochoanal Polyps in Children: A Systematic Review. Int. J. Pediatr. Otorhinolaryngol. 2018, 106, 26–30. [Google Scholar] [CrossRef]
- Aboud, S.K.; Husain, S.; Gendeh, B.S. Evaluation on Quality of Life in Patients with Nasal Polyposis Managed with Optimal Medical Therapy. Allergy Rhinol. 2014, 5, 2–8. [Google Scholar] [CrossRef] [Green Version]
- Alobid, I.; Benítez, P.; Bernal-Sprekelsen, M.; Roca, J.; Alonso, J.; Picado, C.; Mullol, J. Nasal Polyposis and Its Impact on Quality of Life: Comparison between the Effects of Medical and Surgical Treatments. Allergy 2005, 60, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Hial, V.; De Mello, M.C.; Horakova, Z.; Beaven, M.A. Antiproliferative Activity of Anti-Inflammatory Drugs in Two Mammalian Cell Culture Lines. J. Pharmacol. Exp. Ther. 1977, 202, 446–454. [Google Scholar]
- Kwah, J.H.; Peters, A.T. Nasal Polyps and Rhinosinusitis. Allergy Asthma Proc. 2019, 40, 380–384. [Google Scholar] [CrossRef]
- Sastre, J.; Mosges, R. Local and Systemic Safety of Intranasal Corticosteroids. J. Investig. Allergol. Clin. Immunol. 2012, 22, 1–12. [Google Scholar]
- Fandiño, M.; Macdonald, K.I.; Lee, J.; Witterick, I.J. The Use of Postoperative Topical Corticosteroids in Chronic Rhinosinusitis with Nasal Polyps: A Systematic Review and Meta-Analysis. Am. J. Rhinol. Allergy 2013, 27, e146–e157. [Google Scholar] [CrossRef] [Green Version]
- The Effect of Topical Corticosteroid on Basic Fibroblast Growth Factor in Nasal Polyp Tissue-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/16011129/ (accessed on 15 February 2023).
- Yu, R.; Zhu, D.; Dong, Z. Effects of glucocorticoid on tissue remodeling of nasal mucosa of chronic rhinosinusitis with nasal polyposis after endoscopic surgery. Chin. J. Otorhinolaryngol. Head Neck Surg. 2006, 41, 773–776. [Google Scholar]
- The Effect of Intranasal Beclomethasone Dipropionate on the Recurrence of Nasal Polyps after Ethmoidectomy-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/6988929/ (accessed on 15 February 2023).
- Karlsson, G.; Rundcrantz, H. A Randomized Trial of Intranasal Beclomethasone Dipropionate after Polypectomy. Rhinology 1982, 20, 144–148. [Google Scholar] [PubMed]
- Drettner, B.; Ebbesen, A.; Nilsson, M. Prophylactive Treatment with Flunisolide after Polypectomy. Rhinology 1982, 20, 149–158. [Google Scholar]
- Flunisolide Nasal Spray 0.025% in the Prophylactic Treatment of Nasal Polyposis after Polypectomy. A Randomized, Double Blind, Parallel, Placebo Controlled Study-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/4001759/ (accessed on 15 February 2023).
- Budesonide Nasal Spray as Prophylactic Treatment after Polypectomy (a Double Blind Clinical Trial)-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/3279143/ (accessed on 15 February 2023).
- Kang, I.G.; Yoon, B.K.; Jung, J.H.; Cha, H.E.; Kim, S.T. The Effect of High-Dose Topical Corticosteroid Therapy on Prevention of Recurrent Nasal Polyps after Revision Endoscopic Sinus Surgery. Am. J. Rhinol. 2008, 22, 497–501. [Google Scholar] [CrossRef]
- Vento, S.I.; Blomgren, K.; Hytönen, M.; Simola, M.; Malmberg, H. Prevention of Relapses of Nasal Polyposis with Intranasal Triamcinolone Acetonide after Polyp Surgery: A Prospective Double-Blind, Placebo-Controlled, Randomised Study with a 9-Month Follow-Up. Clin. Otolaryngol. 2012, 37, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Seiberling, K.A.; Kidd, S.C.; Kim, G.H.; Church, C.A. Efficacy of Dexamethasone Versus Fluticasone Nasal Sprays in Postoperative Patients With Chronic Rhinosinusitis With Nasal Polyps. Am. J. Rhinol. Allergy 2019, 33, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Stjärne, P.; Olsson, P.; Alenius, M. Use of Mometasone Furoate to Prevent Polyp Relapse after Endoscopic Sinus Surgery. Arch. Otolaryngol. Head. Neck Surg. 2009, 135, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Dijkstra, M.D.; Ebbens, F.A.; Poublon, R.M.L.; Fokkens, W.J. Fluticasone Propionate Aqueous Nasal Spray Does Not Influence the Recurrence Rate of Chronic Rhinosinusitis and Nasal Polyps 1 Year after Functional Endoscopic Sinus Surgery. Clin. Exp. Allergy 2004, 34, 1395–1400. [Google Scholar] [CrossRef]
- Patriarca, G.; Nucera, E.; DiRienzo, V.; Schiavino, D.; Pellegrino, S.; Fais, G. Nasal Provocation Test with Lysine Acetylsalicylate in Aspirin-Sensitive Patients. Ann. Allergy 1991, 67, 60–62. [Google Scholar]
- Szczeklik, A.; Gryglewski, R.J.; Czerniawska-Mysik, G. Relationship of Inhibition of Prostaglandin Biosynthesis by Analgesics to Asthma Attacks in Aspirin-Sensitive Patients. Br. Med. J. 1975, 1, 67–69. [Google Scholar] [CrossRef] [Green Version]
- Bruzzese, N.; Sica, G.; Iacopino, F.; Paludetti, G.; Schiavino, D.; Nucera, E.; Scarano, E.; Patriarca, G. Growth Inhibition of Fibroblasts from Nasal Polyps and Normal Skin by Lysine Acetylsalicylate. Allergy 1998, 53, 431–434. [Google Scholar] [CrossRef]
- Patriarca, G.; Bellioni, P.; Nucera, E.; Schiavino, D.; Papa, G.; Schinco, G.; Fais, G.; Pirotta, L.R. Intranasal Treatment with Lysine Acetylsalicylate in Patients with Nasal Polyposis. Ann. Allergy 1991, 67, 588–592. [Google Scholar]
- Scadding, G.K.; Hassab, M.; Darby, Y.C.; Lund, V.J.; Freedman, A. Intranasal Lysine Aspirin in Recurrent Nasal Polyposis. Clin. Otolaryngol. Allied Sci. 1995, 20, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Nucera, E.; Schiavino, D.; Milani, A.; Del Ninno, M.; Misuraca, C.; Buonomo, A.; D’Ambrosio, C.; Paludetti, G.; Patriarca, G. Effects of Lysine-Acetylsalicylate (LAS) Treatment in Nasal Polyposis: Two Controlled Long Term Prospective Follow up Studies. Thorax 2000, 55 (Suppl. S2), S75–S78. [Google Scholar] [CrossRef] [Green Version]
- Parikh, A.A.; Scadding, G.K. Intranasal Lysine-Aspirin in Aspirin-Sensitive Nasal Polyposis: A Controlled Trial. Laryngoscope 2005, 115, 1385–1390. [Google Scholar] [CrossRef] [PubMed]
- Ogata, N.; Darby, Y.; Scadding, G. Intranasal Lysine-Aspirin Administration Decreases Polyp Volume in Patients with Aspirin-Intolerant Asthma. J. Laryngol. Otol. 2007, 121, 1156–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostwald, J.; Graumüller, S.; Dommerich, S.; Hoff, M. Influence of rhinologic usual and unusual drugs on fibroblasts from nasal polyps in cell culture. Laryngorhinootologie 2003, 82, 408–415. [Google Scholar] [CrossRef]
- Beata, R.-N.; Wojciech, F.; Stanisław, S.; Ryszard, M. The Influence of Anti-Inflammatory Drugs on the Proliferation of Fibroblast Derived from Nasal Polyps. Auris Nasus Larynx 2005, 32, 225–229. [Google Scholar] [CrossRef]
- Bernstein, J.M. The Molecular Biology of Nasal Polyposis. Curr. Allergy Asthma Rep. 2001, 1, 262–267. [Google Scholar] [CrossRef]
- Passàli, D.; Bernstein, J.M.; Passali, F.M.; Damiani, V.; Passàli, G.C.; Bellussi, L. Treatment of Recurrent Chronic Hyperplastic Sinusitis with Nasal Polyposis. Arch. Otolaryngol. Head. Neck Surg. 2003, 129, 656–659. [Google Scholar] [CrossRef] [Green Version]
- Liedtke, C.M.; Cole, T.S. PKC Signaling in CF/T43 Cell Line: Regulation of NKCC1 by PKC-Delta Isotype. Biochim. Biophys. Acta 2000, 1495, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Das, S. Topical Furosemide Possibly Beneficial for Reducing Recurrence Rates After Nasal Polyp Surgery. JAMA Otolaryngol. Head. Neck Surg. 2016, 142, 1049–1050. [Google Scholar] [CrossRef]
- Passàli, D.; Mezzedimi, C.; Passàli, G.C.; Bellussi, L. Efficacy of Inhalation Form of Furosemide to Prevent Postsurgical Relapses of Rhinosinusal Polyposis. ORL J. Otorhinolaryngol. Relat. Spec. 2000, 62, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, F.; Ghorbanian, M.A.; Hashemian, F.; Mortazavi, S.A.; Sheikhi, M.; Jahanshahi, J.; Poorolajal, J. Effect of Topical Furosemide on Rhinosinusal Polyposis Relapse After Endoscopic Sinus Surgery: A Randomized Clinical Trial. JAMA Otolaryngol. Head. Neck Surg. 2016, 142, 1045–1049. [Google Scholar] [CrossRef]
- Wallwork, B.; Coman, W.; Feron, F.; Mackay-Sim, A.; Cervin, A. Clarithromycin and Prednisolone Inhibit Cytokine Production in Chronic Rhinosinusitis. Laryngoscope 2002, 112, 1827–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervin, A.; Wallwork, B. Macrolide Therapy of Chronic Rhinosinusitis. Rhinology 2007, 45, 259–267. [Google Scholar]
- Piskunov, G.Z.; Bobacheva, T.I. Experience with treatment of chronic polypoid rhinosinusitis using low doses of clarithromycin in the postoperative period. Vestn. Otorinolaringol. 2012, 1, 47–51. [Google Scholar]
- Varvyanskaya, A.; Lopatin, A. Efficacy of Long-Term Low-Dose Macrolide Therapy in Preventing Early Recurrence of Nasal Polyps after Endoscopic Sinus Surgery. Int. Forum Allergy Rhinol. 2014, 4, 533–541. [Google Scholar] [CrossRef]
- Varvianskaia, A.V.; Lopatin, A.S. The effectiveness of long-term treatment of polypous rhinosinusitis with low doses of macrolides. Vestn. Otorinolaringol. 2013, 5, 22–27. [Google Scholar]
- Chung, J.H.; Cosenza, M.J.; Rahbar, R.; Metson, R.B. Mitomycin C for the Prevention of Adhesion Formation after Endoscopic Sinus Surgery: A Randomized, Controlled Study. Otolaryngol. Head. Neck Surg. 2002, 126, 468–474. [Google Scholar] [CrossRef]
- Crosara, P.F.T.B.; Vasconcelos, A.C.; Guimarães, R.E.S.; Becker, H.M.G.; Becker, C.G.; Crosara, S.L.R.; Nascimento, E. Effect of Mitomycin C on the Secretion of Granulocyte Macrophages Colonies Stimulating Factor and Interleukin-5 in Eosinophilic Nasal Polyps Stromal Culture. Braz. J. Otorhinolaryngol. 2005, 71, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Anjos, C.P.G. dos; Vasconcelos, A.C.; Crosara, P.F.T.B.; Anjos, G.C. dos; Becker, C.G.; Guimarães, R.E.S. Apoptosis in Eosinophilic Nasal Polyps Treated in Vitro with Mitomycin C. Braz. J. Otorhinolaryngol. 2012, 78, 32–37. [Google Scholar] [CrossRef] [Green Version]
- de Castro, M.C.M.; Rocha-Silva, F.; Gomes, L.I.; Zauli, D.A.G.; de Moraes Mourão, M.; de Castro, M.M.; Guimarães, R.E.S.; Teixeira-Carvalho, A.; Martins-Filho, O.A. Impact of Mitomycin C on the MRNA Expression Signatures of Immunological Biomarkers in Eosinophilic Nasal Polyposis. Am. J. Rhinol. Allergy 2013, 27, 32–41. [Google Scholar] [CrossRef]
- Lupa, M.; Amedee, R. Is Topical Amphotericin B Efficacious in the Treatment of Chronic Rhinosinusitis? Laryngoscope 2010, 120, 1080–1081. [Google Scholar] [CrossRef]
- Gerlinger, I.; Fittler, A.; Mayer, A.; Patzkó, A.; Fónay, F.; Pytel, J.; Botz, L. Postoperative application of amphotericin B nasal spray in chronic rhinosinusitis with nasal polyposis. Can recidive polyposis be prevented? Orv. Hetil. 2008, 149, 1737–1746. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Jiménez, J.C.; Moreno-Paz, F.J.; Terán, L.M.; Guaní-Guerra, E. Aspirin Exacerbated Respiratory Disease: Current Topics and Trends. Respir. Med. 2018, 135, 62–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasp, G. Is There a Role for Leukotriene Antagonists in the Prevention of Recurrent Nasal Polyps? Curr. Opin. Allergy Clin. Immunol. 2010, 10, 200–205. [Google Scholar] [CrossRef]
- Vuralkan, E.; Saka, C.; Akin, I.; Hucumenoglu, S.; Unal, B.U.; Kuran, G.; Ocal, B. Comparison of Montelukast and Mometasone Furoate in the Prevention of Recurrent Nasal Polyps. Ther. Adv. Respir. Dis. 2012, 6, 5–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacroix, J.S.; Buvelot, J.M.; Polla, B.S.; Lundberg, J.M. Improvement of Symptoms of Non-Allergic Chronic Rhinitis by Local Treatment with Capsaicin. Clin. Exp. Allergy 1991, 21, 595–600. [Google Scholar] [CrossRef]
- Lacroix, J.S.; Kurt, A.M.; Pochon, N.; Bretton, C.; Lundberg, J.M.; Deshusses, J. Neutral Endopeptidase Activity and Concentration of Sensory Neuropeptide in the Human Nasal Mucosa. Eur. Arch. Otorhinolaryngol. 1995, 252, 465–468. [Google Scholar] [CrossRef]
- Zheng, C.; Wang, Z.; Lacroix, J.S. Effect of Intranasal Treatment with Capsaicin on the Recurrence of Polyps after Polypectomy and Ethmoidectomy. Acta Otolaryngol. 2000, 120, 62–66. [Google Scholar] [CrossRef]
- Freeman, S.R.M.; Sivayoham, E.S.G.; Jepson, K.; de Carpentier, J. A Preliminary Randomised Controlled Trial Evaluating the Efficacy of Saline Douching Following Endoscopic Sinus Surgery. Clin. Otolaryngol. 2008, 33, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Perić, A.; Kovačević, S.V.; Barać, A.; Gaćeša, D.; Perić, A.V.; Jožin, S.M. Efficacy of Hypertonic (2.3%) Sea Water in Patients with Aspirin-Induced Chronic Rhinosinusitis Following Endoscopic Sinus Surgery. Acta Otolaryngol. 2019, 139, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Portenko, G.M.; Dobrynin, K.V. Anti-recurrence treatment of patients with polyposis rhinosinusitis in initial vagotonic type of the vegetative tonus. Vestn. Otorinolaringol. 2001, 5, 36–39. [Google Scholar]
- Gammeri, L.; Panzera, C.; Calapai, F.; Cicero, N.; Gangemi, S. Asian Herbal Medicine and Chronic Urticaria: Which Are the Therapeutic Perspectives? Nat. Prod. Res. 2022, 12, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Pittler, M.H.; Ernst, E. Herbal Medicines for the Treatment of Allergic Rhinitis: A Systematic Review. Ann. Allergy Asthma Immunol. 2007, 99, 483–495. [Google Scholar] [CrossRef]
- Miao, E.Y. Recurrent Nasal Polyps Treated by Chinese Herbal Decoction and Acupuncture: A Case Report. J. Altern. Complement. Med. 2010, 16, 691–695. [Google Scholar] [CrossRef]
- Chang, G.-H.; Yang, P.-R.; Cheng, Y.-C.; Hsu, K.-H.; Wu, C.-Y.; Yang, Y.-H.; Lin, Y.-S.; Hsu, C.-M.; Tsai, M.-S.; Tsai, Y.-T.; et al. Nasal Irrigation with Licorice Extract (Glycyrrhiza Glabra) in Treating Nasal Polyps by Reducing Fibroblast Differentiation and Extracellular Matrix Production in TGF-Β1-Stimulated Nasal Polyp-Derived Fibroblasts by Inhibiting the MAPK/ERK-1/2 Pathway-An in Vitro and in Clinic Study. BMC Complement. Med. Ther. 2022, 22, 313. [Google Scholar] [CrossRef]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and Safety of Omalizumab in Nasal Polyposis: 2 Randomized Phase 3 Trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef]
- Harb, H.; Chatila, T.A. Mechanisms of Dupilumab. Clin. Exp. Allergy 2020, 50, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Hoy, S.M. Dupilumab: A Review in Chronic Rhinosinusitis with Nasal Polyps. Drugs 2020, 80, 711–717. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and Safety of Dupilumab in Patients with Severe Chronic Rhinosinusitis with Nasal Polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from Two Multicentre, Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Phase 3 Trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haxel, B.R.; Hummel, T.; Fruth, K.; Lorenz, K.; Gunder, N.; Nahrath, P.; Cuevas, M. Real-World-Effectiveness of Biological Treatment for Severe Chronic Rhinosinusitis with Nasal Polyps. Rhinology 2022, 60, 435–443. [Google Scholar] [CrossRef]
- Mepolizumab in the Management of Severe Eosinophilic Asthma in Adults: Current Evidence and Practical Experience-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30354852/ (accessed on 15 February 2023).
- Available online: https://www.ema.europa.eu/en/documents/product-information/nucala-epar-product-information_it.pdf (accessed on 10 April 2023).
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for Chronic Rhinosinusitis with Nasal Polyps (SYNAPSE): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Respir. Med. 2021, 9, 1141–1153. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Sousa, A.R.; Han, J.K.; Schlosser, R.J.; Sowerby, L.J.; Hopkins, C.; Maspero, J.F.; Smith, S.G.; Kante, O.; Karidi-Andrioti, D.E.; et al. Mepolizumab for Chronic Rhinosinusitis with Nasal Polyps: Treatment Efficacy by Comorbidity and Blood Eosinophil Count. J. Allergy Clin. Immunol. 2022, 149, 1711–1721.e6. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Castelnuovo, P.; Spirito, L.; Feduzi, M.; Seccia, V.; Visca, D.; Spanevello, A.; Statuti, E.; Latorre, M.; Montuori, C.; et al. Mepolizumab Improves Outcomes of Chronic Rhinosinusitis with Nasal Polyps in Severe Asthmatic Patients: A Multicentric Real-Life Study. J. Pers. Med. 2022, 12, 1304. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Maurer, M.; Palomares, O.; Busse, W.W. What Is the Contribution of IgE to Nasal Polyposis? J. Allergy Clin. Immunol. 2021, 147, 1997–2008. [Google Scholar] [CrossRef]
- Eschenbacher, W.; Straesser, M.; Knoeddler, A.; Li, R.-C.; Borish, L. Biologics for the Treatment of Allergic Rhinitis, Chronic Rhinosinusitis, and Nasal Polyposis. Immunol. Allergy Clin. North. Am. 2020, 40, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Bakakos, A.; Schleich, F.; Bakakos, P. Biological Therapy of Severe Asthma and Nasal Polyps. J. Pers. Med. 2022, 12, 976. [Google Scholar] [CrossRef]
- Damask, C.; Chen, M.; Holweg, C.T.J.; Yoo, B.; Millette, L.A.; Franzese, C. Defining the Efficacy of Omalizumab in Nasal Polyposis: A POLYP 1 and POLYP 2 Subgroup Analysis. Am. J. Rhinol. Allergy 2022, 36, 135–141. [Google Scholar] [CrossRef]
- Bousquet, J.; Heinzerling, L.; Bachert, C.; Papadopoulos, N.G.; Bousquet, P.J.; Burney, P.G.; Canonica, G.W.; Carlsen, K.H.; Cox, L.; Haahtela, T.; et al. Practical Guide to Skin Prick Tests in Allergy to Aeroallergens. Allergy 2012, 67, 18–24. [Google Scholar] [CrossRef]
- Lund, V.J.; Kennedy, D.W. Quantification for Staging Sinusitis. Ann. Otol. Rhinol. Laryngol. 1995, 104, 17–21. [Google Scholar] [CrossRef]
- Lund, V.J.; Mackay, I.S. Staging in Rhinosinusitus. Rhinology 1993, 31, 183–184. [Google Scholar] [PubMed]
- Morley, A.D.; Sharp, H.R. A Review of Sinonasal Outcome Scoring Systems-Which Is Best? Clin. Otolaryngol. 2006, 31, 103–109. [Google Scholar] [CrossRef]
- Hopkins, C.; Gillett, S.; Slack, R.; Lund, V.J.; Browne, J.P. Psychometric Validity of the 22-Item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, S.; Alreefy, H.; Hopkins, C. Prevalence of Sinonasal Outcome Test (SNOT-22) Symptoms in Patients Undergoing Surgery for Chronic Rhinosinusitis in the England and Wales National Prospective Audit. Clin. Otolaryngol. 2012, 37, 276–282. [Google Scholar] [CrossRef]
- DeConde, A.S.; Mace, J.C.; Levy, J.M.; Rudmik, L.; Alt, J.A.; Smith, T.L. Prevalence of Polyp Recurrence after Endoscopic Sinus Surgery for Chronic Rhinosinusitis with Nasal Polyposis. Laryngoscope 2017, 127, 550–555. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, J.M.; Yankaskas, J.R. Increased Ion Transport in Cultured Nasal Polyp Epithelial Cells. Arch. Otolaryngol. Head. Neck Surg. 1994, 120, 993–996. [Google Scholar] [CrossRef]
- Jiang, Y.; Xu, J.; Chen, Y.; Shi, J.; Zhang, C.; Li, J. Expression and Distribution of Epithelial Sodium Channel in Nasal Polyp and Nasal Mucosa. Eur. Arch. Otorhinolaryngol. 2015, 272, 3361–3366. [Google Scholar] [CrossRef]
- Saber, A.; Nakka, S.S.; Hussain, R.; Hugosson, S. Staphylococcus Aureus in Chronic Rhinosinusitis: The Effect on the Epithelial Chloride Channel (Cystic Fibrosis Transmembrane Conductance Regulator, CFTR) and the Epithelial Sodium Channel (ENaC) Physiology. Acta Otolaryngol. 2019, 139, 652–658. [Google Scholar] [CrossRef]
- Li, Z.; Gao, Q.; Zhen, H.; Cui, Y. Effects of intranasal cortocosteroidson on the expression of Aquaporin-5 in human nasal polyps. Lin. Chuang Er Bi Yan Hou Ke Za Zhi 2004, 18, 647–649. [Google Scholar]
- Zhang, X.; Yuan, Y.; Gu, W.; Mu, J.; Qu, Y. The effects of intranasal FP on the expression of aquaporin-2 in nasal polyps. Lin. Chuang Er Bi Yan Hou Ke Za Zhi 2003, 17, 472–473. [Google Scholar]
- Cingi, C.; Bayar Muluk, N.; Mitsias, D.I.; Papadopoulos, N.G.; Klimek, L.; Laulajainen-Hongisto, A.; Hytönen, M.; Toppila-Salmi, S.K.; Scadding, G.K. The Nose as a Route for Therapy: Part 1. Pharmacotherapy. Front. Allergy 2021, 2, 638136. [Google Scholar] [CrossRef]
- Dundar, R.; Bayar Muluk, N.; Vejselova Sezer, C.; Kaya, F.; Kutlu, H.M.; Cingi, C. A Safety Investigation into Topical Effects of Naproxen Sodium on Nasal Epithelial Cells and Potential Toxicity in Local Application. Am. J. Otolaryngol. 2023, 44, 103689. [Google Scholar] [CrossRef] [PubMed]
- Kar, M.; Ince, I.; Yildirim, C.; Burukoğlu Dönmez, D.; Karasulu, Y.; Cingi, C. Development of an Intranasal Formulation Containing Indomethacin and Xylometazoline for Rhinosinusitis Treatment. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Di Rienzo, L.; Artuso, A.; Cerqua, N. Antileukotrienes in the prevention of postoperative recurrence of nasal polyposis in ASA syndrome. Acta Otorhinolaryngol. Ital. 2000, 20, 336–342. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Age [Years] | SNOT-22 | Nasal Polyp Score (NPS) | Lund-Mackay Score | Perennial Allergen | Seasonal Allergen |
|---|---|---|---|---|---|---|
| #5 | 60 | 32 | 3 | 10-9 | Yes | None |
| #11 | 55 | 33 | 3 | 9-8 | None | None |
| #13 | 53 | 28 | 2 | 7-6 | Yes | Yes |
| #14 | 69 | 35 | 4 | 12-12 | Yes | None |
| #16 | 71 | 36 | 4 | 10-11 | None | Yes |
| #17 | 57 | 23 | 2 | 7-7 | None | None |
| #18 | 51 | 26 | 2 | 8-7 | Yes | Yes |
| #19 | 49 | 25 | 3 | 7-6 | Yes | None |
| #20 | 29 | 25 | 3 | 6-7 | Yes | None |
| #22 | 55 | 27 | 3 | 8-7 | Yes | Yes |
| #23 | 53 | 22 | 2 | 7-5 | None | None |
| #25 | 42 | 37 | 4 | 9-11 | None | None |
| Patients | #5 | #11 | #13 | #14 | #16 | #17 | #18 | #19 | #20 | #22 | #23 | #25 | Median |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Untreated | 2.3715 | 1.787 | 1.202 | 2.6218 | 2.3605 | 2.8755 | 1.617 | 1.4245 | 1.129 | 0.1373 | 2.3623 | 1.2198 | 1.702 |
| 20 µg/mL | |||||||||||||
| Diclofenac | 1.845 | 1.5093 | 1.1458 | 2.0838 | 2.0078 | 2.7838 | 1.419 | 1.267 | 0.8843 | 0.167 | 1.8443 | 1.0708 | 1.419 |
| Ketoprofen | 1.9828 | 1.539 | 1.167 | 2.0848 | 2.22 | 2.6737 | 1.479 | 1.2525 | 0.9623 | 0.1845 | 2.036 | 1.0625 | 1.509 |
| LAS | 1.9485 | 0.8665 | 1.0578 | 2.195 | 2.218 | 2.6933 | 1.468 | 1.2598 | 0.8853 | 0.0965 | 2.118 | 1.0243 | 1.3639 |
| 200 µg/mL | |||||||||||||
| Diclofenac | 1.51925 | 1.1573 | 0.948 | 1.5153 | 1.6033 | 2.2533 | 1.0163 | 0.9938 | 0.628 | 0.0583 | 1.0518 | 0.82 | 1.034 |
| Ketoprofen | 1.9165 | 1.6093 | 1.0598 | 2.0133 | 2.2838 | 2.7077 | 1.4755 | 1.3095 | 0.8785 | 0.1808 | 1.9455 | 1.1203 | 1.5424 |
| LAS | 1.8888 | 0.7288 | 1.143 | 2.0575 | 2.217 | 2.697 | 1.421 | 1.172 | 0.829 | 0.0933 | 2.0435 | 1.058 | 1.2965 |
| 2000 µg/mL | |||||||||||||
| Diclofenac | 0.8615 | 0.5005 | 0.22 | 0.1143 | 0.0858 | 0.258 | 0.1633 | 0.0665 | 0.1318 | 0.0125 | 0.1493 | 0.1188 | 0.1405 |
| Ketoprofen | 1.365 | 1.2745 | 0.8313 | 1.516 | 1.6878 | 2.1663 | 0.8798 | 0.832 | 0.5155 | 0.1133 | 1.1848 | 0.7887 | 1.0323 |
| LAS | 1.5223 | 0.5135 | 1.0483 | 1.774 | 1.776 | 2.0195 | 0.9043 | 0.4963 | 0.7365 | 0.0403 | 1.4398 | 0.7285 | 0.9763 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzi, A.; Gammeri, L.; Cordiano, R.; Valentini, M.; Centrone, M.; Marrone, S.; Inchingolo, R.; Lohmeyer, F.M.; Cavaliere, C.; Ria, F.; et al. Therapeutic Strategies to Prevent the Recurrence of Nasal Polyps after Surgical Treatment: An Update and In Vitro Study on Growth Inhibition of Fibroblasts. J. Clin. Med. 2023, 12, 2841. https://doi.org/10.3390/jcm12082841
Rizzi A, Gammeri L, Cordiano R, Valentini M, Centrone M, Marrone S, Inchingolo R, Lohmeyer FM, Cavaliere C, Ria F, et al. Therapeutic Strategies to Prevent the Recurrence of Nasal Polyps after Surgical Treatment: An Update and In Vitro Study on Growth Inhibition of Fibroblasts. Journal of Clinical Medicine. 2023; 12(8):2841. https://doi.org/10.3390/jcm12082841
Chicago/Turabian StyleRizzi, Angela, Luca Gammeri, Raffaele Cordiano, Mariagrazia Valentini, Michele Centrone, Sabino Marrone, Riccardo Inchingolo, Franziska Michaela Lohmeyer, Carlo Cavaliere, Francesco Ria, and et al. 2023. "Therapeutic Strategies to Prevent the Recurrence of Nasal Polyps after Surgical Treatment: An Update and In Vitro Study on Growth Inhibition of Fibroblasts" Journal of Clinical Medicine 12, no. 8: 2841. https://doi.org/10.3390/jcm12082841