
Identifying Residual Psychological Symptoms after Nasal Reconstruction Surgery in Patients with Empty Nose Syndrome
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Submucosal Medpor Implantation
2.3. Questionnaire Evaluations
2.4. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Participants
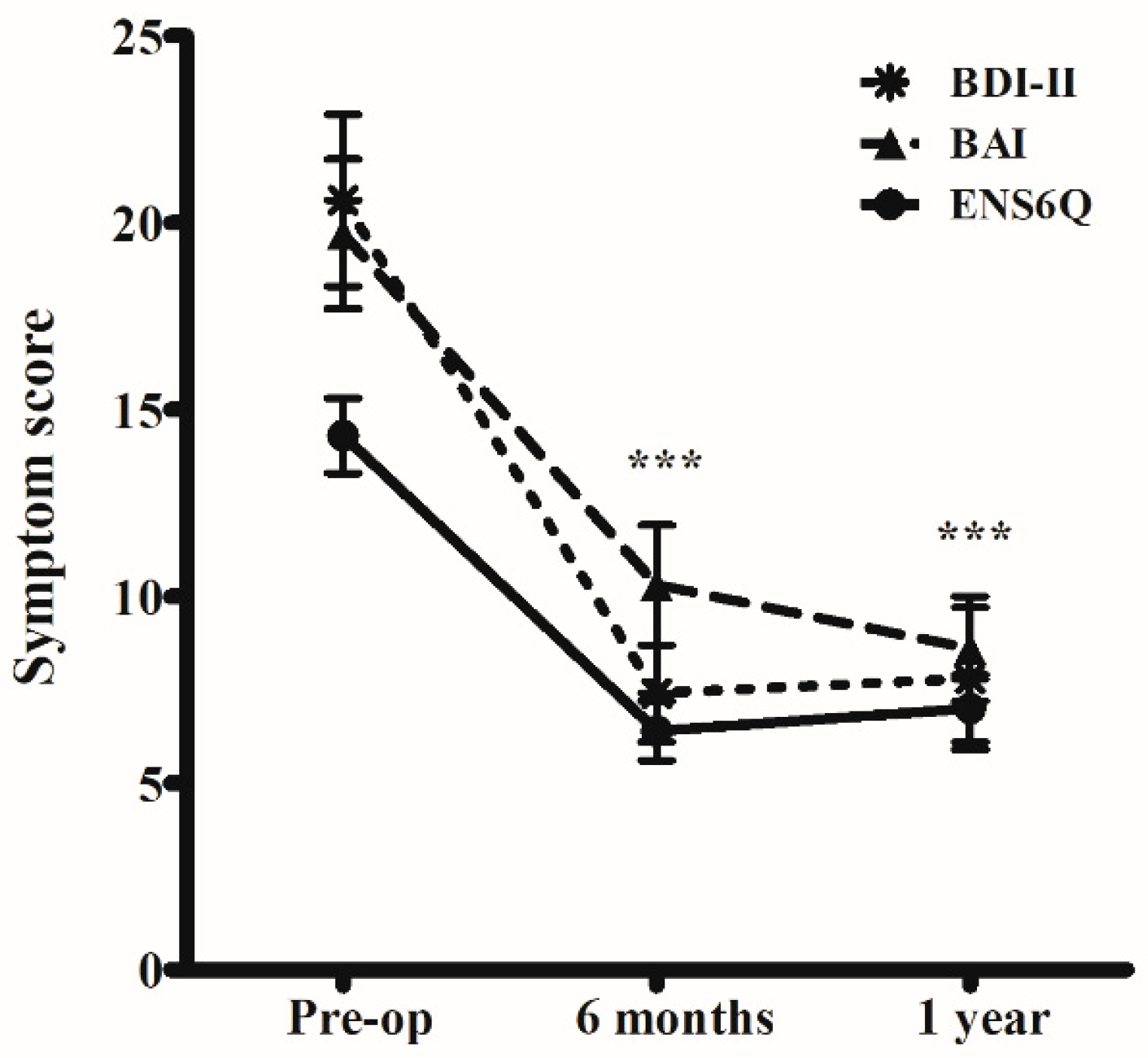
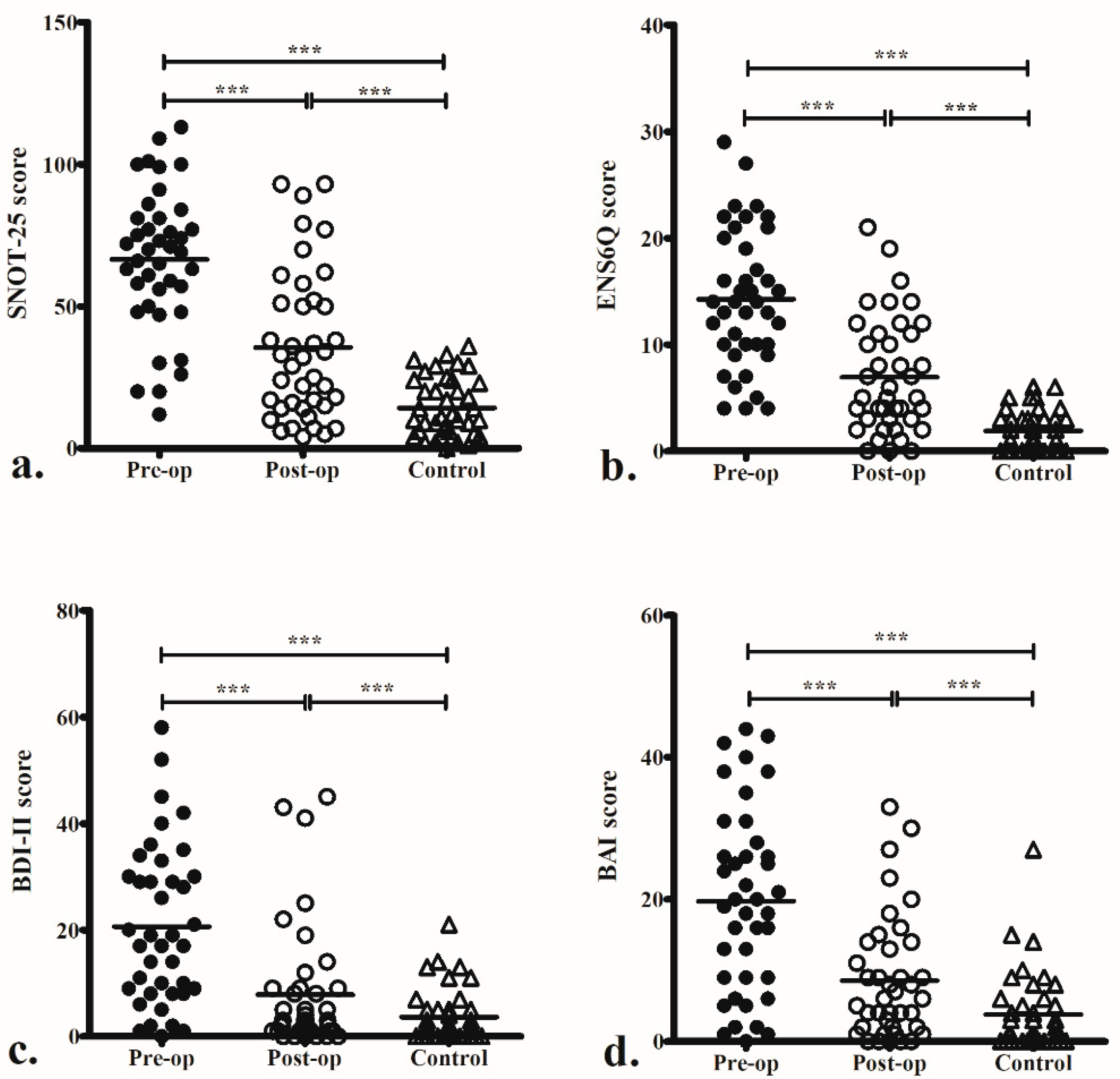
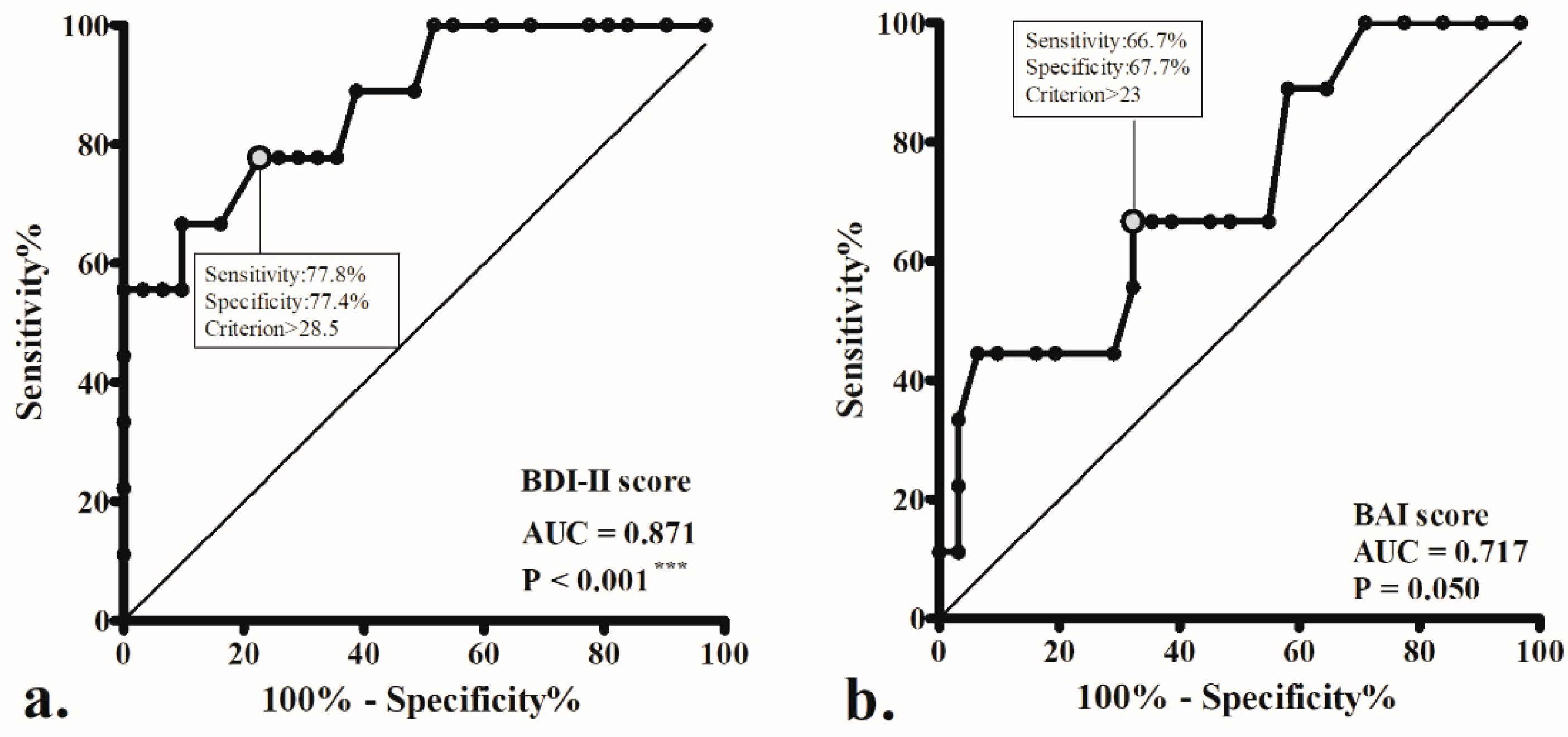
3.2. Questionnaire Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheithauer, M.O. Surgery of the turbinates and “empty nose” syndrome. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2010, 9, Doc03. [Google Scholar] [PubMed]
- Moore, E.J.; Kern, E.B. Atrophic rhinitis: A review of 242 cases. Am. J. Rhinol. 2001, 15, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.H.; Jang, Y.J. Factors affecting the complication rate of septoplasty: Analysis of 1506 consecutive cases of single surgeon. Facial Plast. Surg. 2023. [Google Scholar] [CrossRef]
- Sozansky, J.; Houser, S.M. Pathophysiology of empty nose syndrome. Laryngoscope 2015, 125, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Kanjanawasee, D.; Campbell, R.G.; Rimmer, J.; Alvarado, R.; Kanjanaumporn, J.; Snidvongs, K.; Kalish, L.; Harvey, R.J.; Sacks, R. Empty Nose Syndrome Pathophysiology: A Systematic Review. Otolaryngol. Head Neck Surg. 2022, 167, 434–451. [Google Scholar] [CrossRef]
- Chhabra, N.; Houser, S.M. The diagnosis and management of empty nose syndrome. Otolaryngol. Clin. N. Am. 2009, 42, 311–330. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Blacker, K.; Luo, Y.; Bryant, B.; Jiang, J. Perceiving nasal patency through mucosal cooling rather than air temperature or nasal resistance. PLoS ONE 2011, 6, e24618. [Google Scholar] [CrossRef]
- Li, C.; Farag, A.A.; Maza, G.; McGhee, S.; Ciccone, M.A.; Deshpande, B.; Pribitkin, E.A.; Otto, B.A.; Zhao, K. Investigation of the abnormal nasal aerodynamics and trigeminal functions among empty nose syndrome patients. Int. Forum Allergy Rhinol. 2018, 8, 444–452. [Google Scholar] [CrossRef]
- Konstantinidis, I.; Tsakiropoulou, E.; Chatziavramidis, A.; Ikonomidis, C.; Markou, K. Intranasal trigeminal function in patients with empty nose syndrome. Laryngoscope 2017, 127, 1263–1267. [Google Scholar] [CrossRef]
- Wu, C.L.; Fu, C.H.; Lee, T.J. Distinct Histopathology Characteristics in Empty Nose Syndrome. Laryngoscope 2021, 131, E14–E18. [Google Scholar]
- Jiang, C.; Wong, F.; Chen, K.; Shi, R. Assessment of surgical results in patients with empty nose syndrome using the 25-item sino-nasal outcome test evaluation. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasquez, N.; Thamboo, A.; Habib, A.R.; Huang, Z.; Nayak, J.V. The Empty Nose Syndrome 6-Item Questionnaire (ENS6Q): A validated 6-item questionnaire as a diagnostic aid for empty nose syndrome patients. Int. Forum Allergy Rhinol. 2017, 7, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Manji, J.; Nayak, J.V.; Thamboo, A. The functional and psychological burden of empty nose syndrome. Int. Forum Allergy Rhinol. 2018, 8, 707–712. [Google Scholar] [CrossRef]
- Lee, T.J.; Fu, C.H.; Wu, C.L.; Tam, Y.Y.; Huang, C.C.; Chang, P.H.; Chen, Y.W.; Wu, M.H. Evaluation of depression and anxiety in empty nose syndrome after surgical treatment. Laryngoscope 2016, 126, 1284–1289. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Wu, P.W.; Fu, C.H.; Huang, C.C.; Chang, P.H.; Wu, C.L.; Lee, T.J. What drives depression in empty nose syndrome? A Sinonasal Outcome Test-25 subdomain analysis. Rhinology 2019, 57, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Lamb, M.; Bacon, D.R.; Zeatoun, A.; Onourah, P.; Thorp, B.D.; Abramowitz, J.; Ebert, C.S., Jr.; Kimple, A.J.; Senior, B.A. Mental health burden of empty nose syndrome compared to chronic rhinosinusitis and chronic rhinitis. Int. Forum Allergy Rhinol. 2022, 12, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Lee, C.C.; Wei, P.W.; Chuang, C.C.; Lee, Y.S.; Chang, P.H.; Huang, C.C.; Fu, C.H.; Lee, T.J. Sleep impairment in patients with empty nose syndrome. Rhinology 2023, 61, 47–53. [Google Scholar] [CrossRef]
- Huang, C.C.; Wu, P.W.; Fu, C.H.; Huang, C.C.; Chang, P.H.; Lee, T.J. Impact of Psychologic Burden on Surgical Outcome in Empty Nose Syndrome. Laryngoscope 2021, 131, E694–E701. [Google Scholar] [CrossRef]
- Huang, C.C.; Wu, P.W.; Lee, C.C.; Chang, P.H.; Huang, C.C.; Lee, T.J. Suicidal thoughts in patients with empty nose syndrome. Laryngoscope Investig. Otolaryngol. 2022, 7, 22–28. [Google Scholar] [CrossRef]
- Huang, C.C.; Wu, P.W.; Lee, C.C.; Huang, C.C.; Fu, C.H.; Chang, P.H.; Lee, T.J. Comparison of SNOT-25 and ENS6Q in evaluating patients with empty nose syndrome. Laryngoscope Investig. Otolaryngol. 2022, 7, 342–348. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corp.: San Antonio, TX, USA, 1996. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometirc properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Tian, P.; Hu, J.; Ma, Y.; Zhou, C.; Liu, X.; Dang, H.; Zou, H. The clinical effect of psychosomatic interventions on empty nose syndrome secondary to turbinate-sparing techniques: A prospective self-controlled study. Int. Forum Allergy Rhinol. 2021, 11, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Dholakia, S.; Spector, B.M.; Yang, A.; Kim, D.; Borchard, N.A.; Thamboo, A.; Zhao, K.; Nayak, J.V. Inferior meatus augmentation procedure (IMAP) normalizes nasal airflow patterns in empty nose syndrome patients via computational fluid dynamics (CFD) modeling. Int. Forum Allergy Rhinol. 2021, 11, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Li, C.; Maza, G.; Farag, A.A.; Krebs, J.P.; McGhee, S.; Zappitelli, G.; Deshpande, B.; Otto, B.A.; Zhao, K. Computational fluid dynamic analysis of aggressive turbinate reductions: Is it a culprit of empty nose syndrome? Int. Forum Allergy Rhinol. 2019, 9, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Berking, M.; Wupperman, P. Emotion regulation and mental health: Recent findings, current challenges, and future directions. Curr. Opin. Psychiatry 2012, 25, 128–134. [Google Scholar] [CrossRef]
- Freund, W.; Wunderlich, A.P.; Stöcker, T.; Schmitz, B.L.; Scheithauer, M.O. Empty nose syndrome: Limbic system activation observed by functional magnetic resonance imaging. Laryngoscope 2011, 121, 2019–2025. [Google Scholar] [CrossRef]
- Mangin, D.; Bequignon, E.; Zerah-Lancner, F.; Isabey, D.; Louis, B.; Adnot, S.; Papon, J.F.; Coste, A.; Boyer, L.; Devars du Mayne, M. Investigating hyperventilation syndrome in patients suffering from empty nose syndrome. Laryngoscope 2017, 127, 1983–1988. [Google Scholar] [CrossRef]
- Thamboo, A.; Velasquez, N.; Habib, A.R.; Zarabanda, D.; Paknezhad, H.; Nayak, J.V. Defining surgical criteria for empty nose syndrome: Validation of the office-based cotton test and clinical interpretability of the validated Empty Nose Syndrome 6-Item Questionnaire. Laryngoscope 2017, 127, 1746–1752. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ENS | Control | p Value † | |
|---|---|---|---|
| Case number, n (%) | 40 | 40 | |
| Age (year) | 45.0 ± 13.0 | 44.7 ± 12.6 | 0.862 |
| Female: male, n | 10:30 | 10:30 | 1.000 |
| Smoker, n (%) | 9 (22.5) | 7 (17.5) | 0.781 |
| Previous nasal surgery: | |||
| Inferior turbinate surgery, n (%) | 40 (100) | 0 (0) | |
| Nasal septal surgery, n (%) | 26 (65.0) | 0 (0) | |
| Endoscopic sinus surgery, n (%) | 13 (32.5) | 0 (0) | |
| Caldwell–Luc operation, n (%) | 2 (5.0) | 0 (0) |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Age | 0.98 (0.92–1.04) | 0.415 | ||
| Gender | 0.82 (0.14–4.80) | 0.827 | ||
| Pre-op SNOT-25 | 1.03 (0.99–1.06) | 0.150 | ||
| Pre-op ENS6Q | 1.10 (0.97–1.25) | 0.122 | ||
| Pre-op BDI-II | 1.14 (1.04–1.25) | 0.004 ** | 1.17 (1.03–1.33) | 0.013 * |
| Pre-op BAI | 1.08 (1.01–1.15) | 0.033 * | 0.96 (0.86–1.08) | 0.505 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Wu, P.-W.; Huang, C.-C.; Chang, P.-H.; Fu, C.-H.; Lee, T.-J. Identifying Residual Psychological Symptoms after Nasal Reconstruction Surgery in Patients with Empty Nose Syndrome. J. Clin. Med. 2023, 12, 2635. https://doi.org/10.3390/jcm12072635
Huang C-C, Wu P-W, Huang C-C, Chang P-H, Fu C-H, Lee T-J. Identifying Residual Psychological Symptoms after Nasal Reconstruction Surgery in Patients with Empty Nose Syndrome. Journal of Clinical Medicine. 2023; 12(7):2635. https://doi.org/10.3390/jcm12072635
Chicago/Turabian StyleHuang, Chien-Chia, Pei-Wen Wu, Chi-Che Huang, Po-Hung Chang, Chia-Hsiang Fu, and Ta-Jen Lee. 2023. "Identifying Residual Psychological Symptoms after Nasal Reconstruction Surgery in Patients with Empty Nose Syndrome" Journal of Clinical Medicine 12, no. 7: 2635. https://doi.org/10.3390/jcm12072635