
Psychological Outcomes and Quality of Life of Fibromyalgia Patients with Vitamin D Supplementation—A Meta-Analysis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
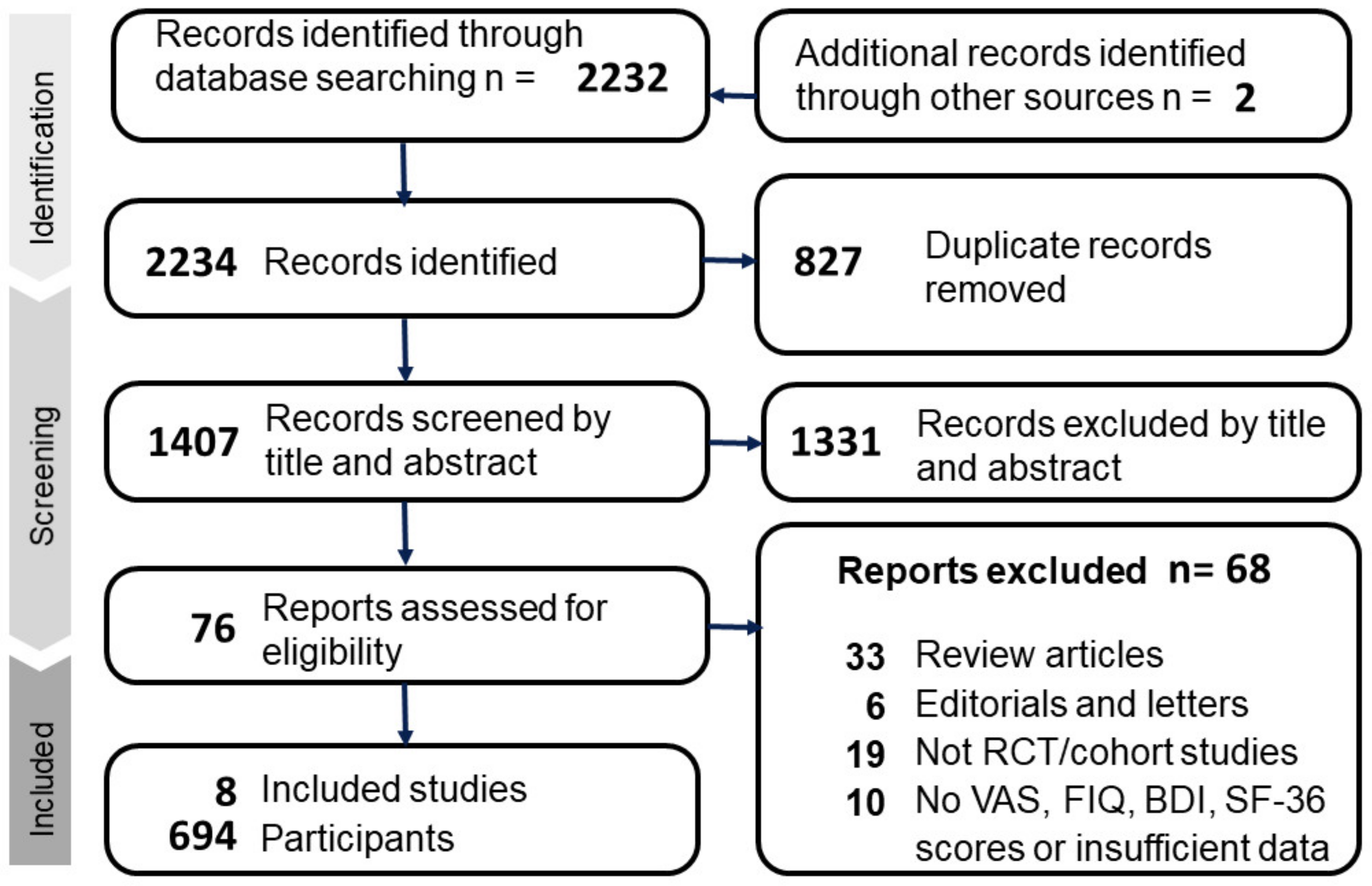
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
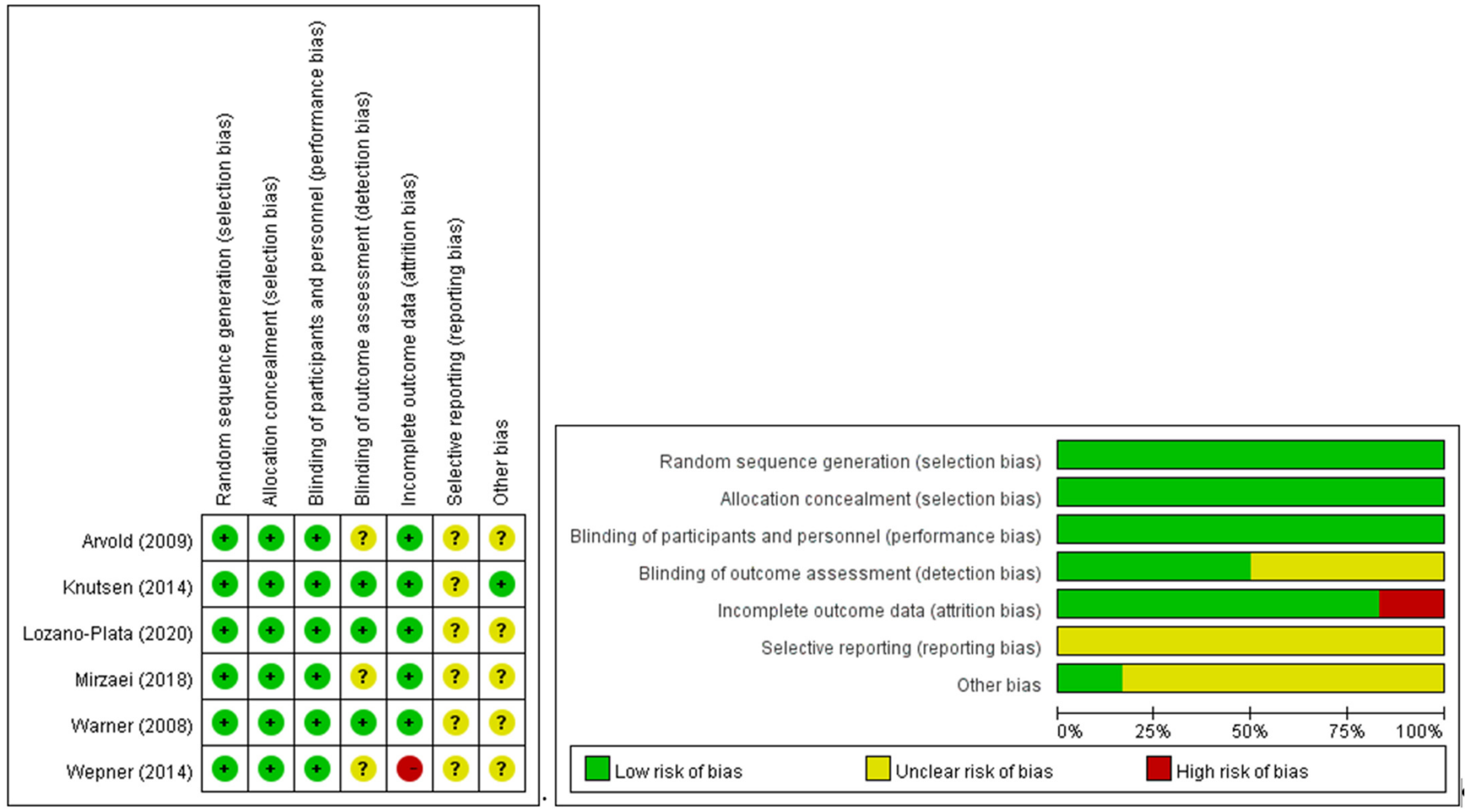
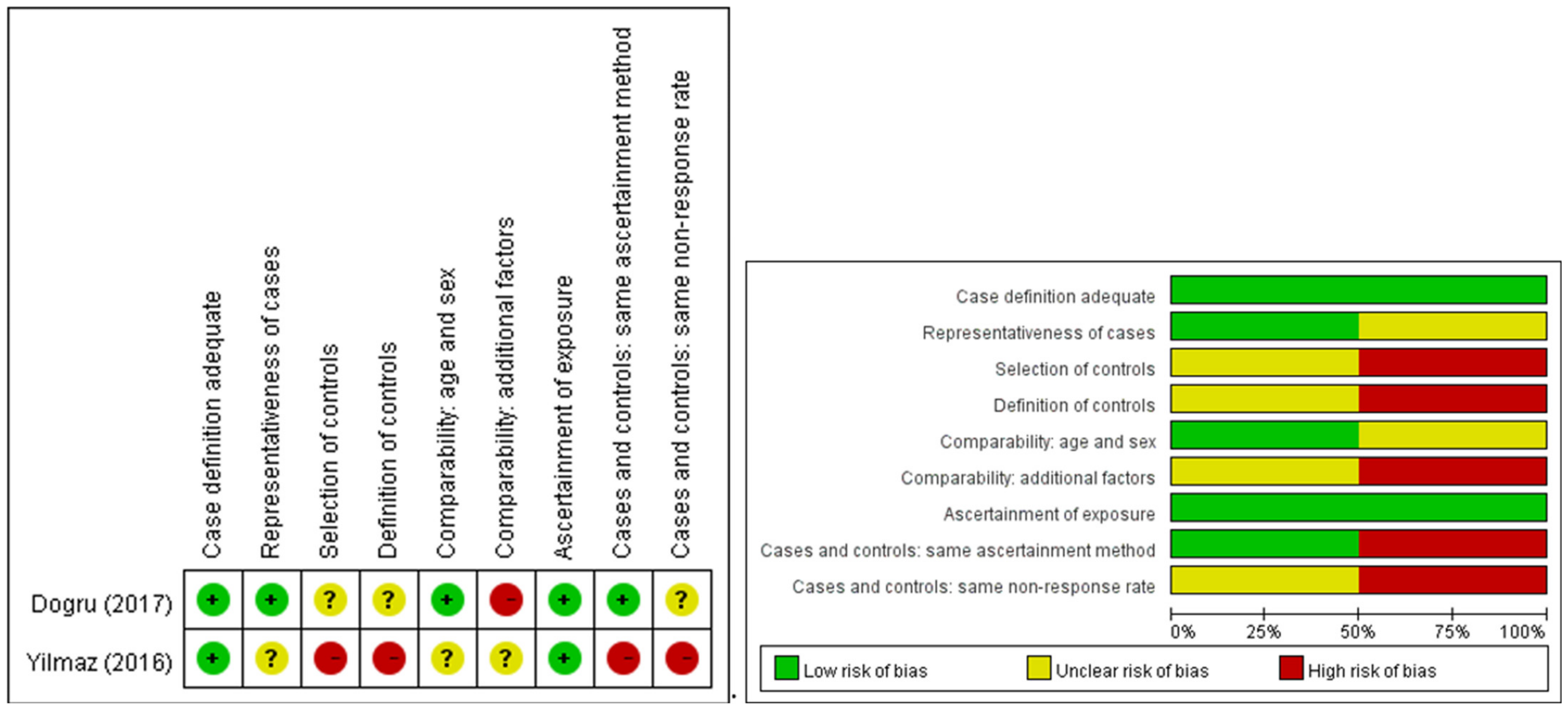
2.3. Data Extraction and Quality Appraisal
2.4. Outcomes Assessments
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Included Studies
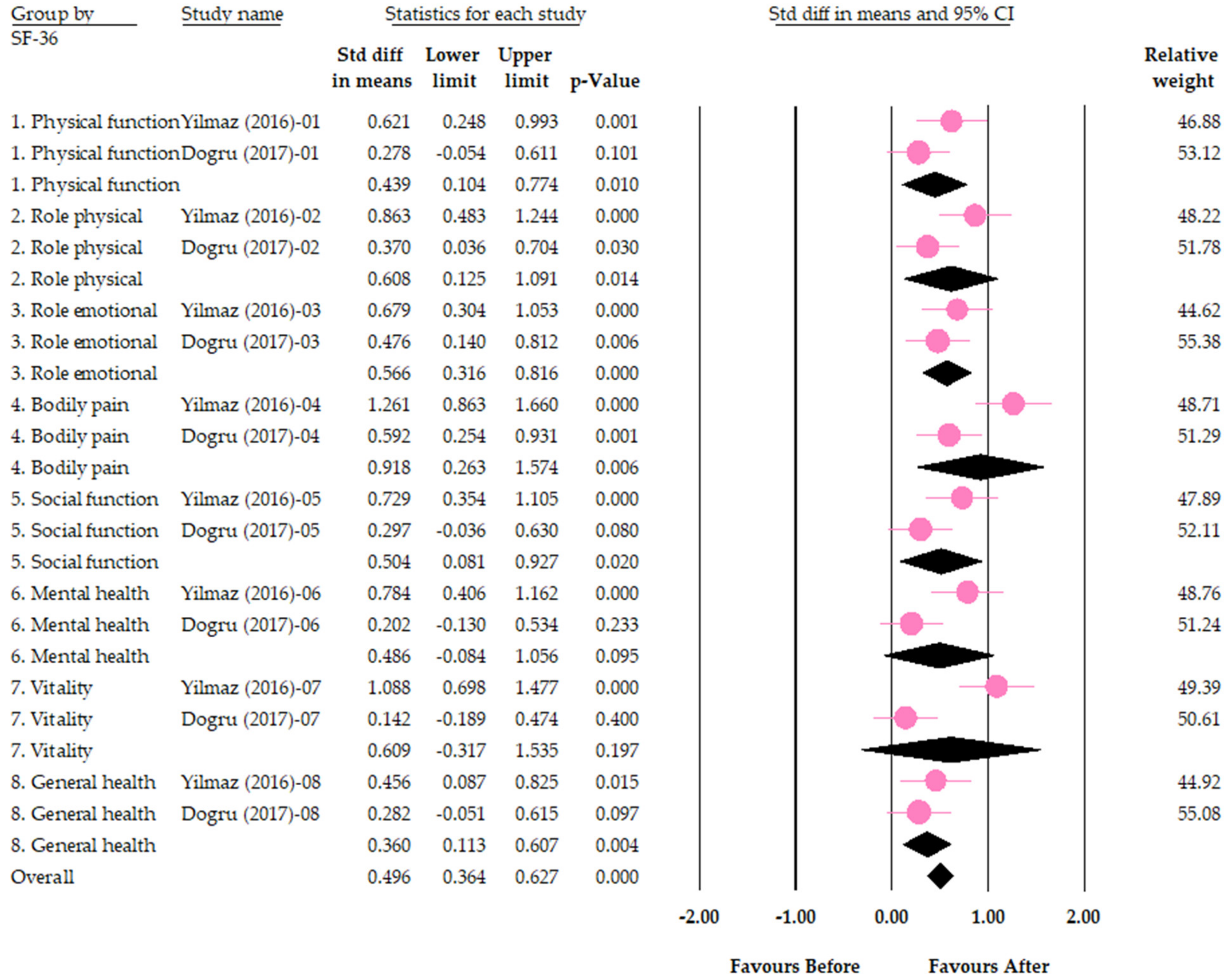
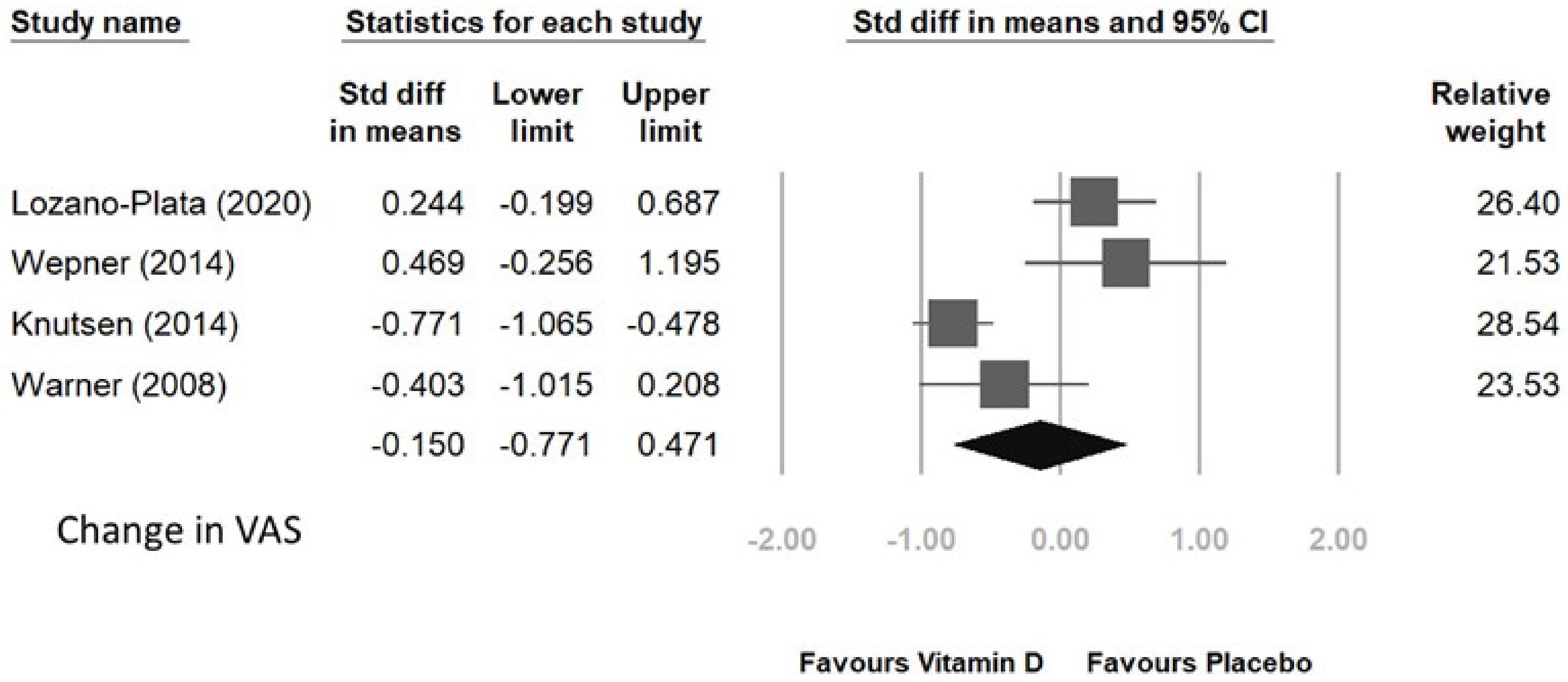
3.2. Psychological Effects of Vitamin D Supplementation on Fibromyalgia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Häuser, W. Fibromyalgia diagnosis and diagnostic criteria. Ann. Med. 2011, 43, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; Santo, A.D.S.D.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicras-Mainar, A.; Rejas, J.; Navarro, R.; Blanca, M.; Morcillo, A.; Larios, R.; Velasco, S.; Villarroya, C. Treating patients with fibromyalgia in primary care settings under routine medical practice: A claim database cost and burden of illness study. Thromb. Haemost. 2009, 11, R54. [Google Scholar] [CrossRef] [Green Version]
- Rivera, J.; Rejas, J.; Esteve-Vives, J.; Vallejo, M. Resource utilisation and health care costs in patients diagnosed with fibromyalgia in Spain. Clin. Exp. Rheumatol. 2009, 27, S39–S45. [Google Scholar]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Fitzcharles, M.-A.; Hassett, A.L.; Katz, R.S.; Häuser, W.; Wolfe, F. The Longitudinal Outcome of Fibromyalgia: A Study of 1555 Patients. J. Rheumatol. 2011, 38, 2238–2246. [Google Scholar] [CrossRef]
- Su, K.-P.; Lai, H.-C.; Yang, H.-T.; Su, W.-P.; Peng, C.-Y.; Chang, J.P.-C.; Chang, H.-C.; Pariante, C.M. Omega-3 Fatty Acids in the Prevention of Interferon-Alpha-Induced Depression: Results from a Randomized, Controlled Trial. Biol. Psychiatry 2014, 76, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-Y.; Huang, S.-Y.; Su, K.-P. A Meta-Analytic Review of Polyunsaturated Fatty Acid Compositions in Patients with Depression. Biol. Psychiatry 2010, 68, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Kvæl, L.A.H.; Løchting, I.; Molin, M. Use of Dietary Supplements and Perceived Knowledge among Adults Living with Fibromyalgia in Norway: A Cross-Sectional Study. Nutrients 2021, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and nutrition: Therapeutic possibilities? Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Kiraly, S.J.; Kiraly, M.A.; Hawe, R.D.; Makhani, N. Vitamin D as a Neuroactive Substance: Review. Sci. World J. 2006, 6, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Guida, F.; Boccella, S.; Belardo, C.; Iannotta, M.; Piscitelli, F.; De Filippis, F.; Paino, S.; Ricciardi, F.; Siniscalco, D.; Marabese, I.; et al. Altered gut microbiota and endocannabinoid system tone in vitamin D deficiency-mediated chronic pain. Brain Behav. Immun. 2019, 85, 128–141. [Google Scholar] [CrossRef]
- Wu, Z.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. The association between vitamin D concentration and pain: A systematic review and meta-analysis. Public Heal. Nutr. 2018, 21, 2022–2037. [Google Scholar] [CrossRef] [Green Version]
- McBeth, J.; Pye, S.; O’Neill, T.; Macfarlane, G.; Tajar, A.; Bartfai, G.; Boonen, S.; Bouillon, R.; Casanueva, F.; Finn, J.D.; et al. Musculoskeletal pain is associated with very low levels of vitamin D in men: Results from the European Male Ageing Study. Ann. Rheum. Dis. 2010, 69, 1448–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Oliveira, D.L.; Hirotsu, C.; Tufik, S.; Andersen, M.L. The interfaces between vitamin D, sleep and pain. J. Endocrinol. 2017, 234, R23–R36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Huang, Y.; Huang, W. The effect of vitamin D supplement on negative emotions: A systematic review and meta-analysis. Depress. Anxiety 2020, 37, 549–564. [Google Scholar] [CrossRef]
- Makrani, A.H.; Afshari, M.; Ghajar, M.; Foroughi, Z.; Moosazadeh, M. Vitamin D and fibromyalgia: A meta-analysis. Korean J. Pain 2017, 30, 250–257. [Google Scholar] [CrossRef]
- Habib, A.M.; Nagi, K.; Thillaiappan, N.B.; Sukumaran, V.; Akhtar, S. Vitamin D and Its Potential Interplay With Pain Signaling Pathways. Front. Immunol. 2020, 11, 820. [Google Scholar] [CrossRef] [PubMed]
- Zanin, E.; Ranjeva, J.; Confort-Gouny, S.; Guye, M.; Denis, D.; Cozzone, P.J.; Girard, N. White matter maturation of normal human fetal brain. An in vivo diffusion tensor tractography study. Brain Behav. 2011, 1, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Zhang, Y.; Wang, T.; Lin, Y.; Yu, J.; Xia, Q.; Zhu, P.; Zhu, D.M. Vitamin D supplementation improves anxiety but not depression symptoms in patients with vitamin D deficiency. Brain Behav. 2020, 10, e01760. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Wang, L.-K.; Hung, K.-C.; Wu, Z.-F.; Chang, C.-Y.; Chen, J.-Y. Patient characteristics and analgesic efficacy of antiviral therapy in postherpetic neuralgia. Med. Hypotheses 2019, 131, 109323. [Google Scholar] [CrossRef]
- Hausmann, J.; Kubesch, A.; Amiri, M.; Filmann, N.; Blumenstein, I. Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2019, 8, 1319. [Google Scholar] [CrossRef] [Green Version]
- Aksan, A.; Tugal, D.; Hein, N.; Boettger, K.; Caicedo-Zea, Y.; Diehl, I.; Schumann, C.; Armbruster, F.-P.; Stein, J. Measuring Vitamin D Status in Chronic Inflammatory Disorders: How does Chronic Inflammation Affect the Reliability of Vitamin D Metabolites in Patients with IBD? J. Clin. Med. 2020, 9, 547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karkeni, E.; Bonnet, L.; Marcotorchino, J.; Tourniaire, F.; Astier, J.; Ye, J.; Landrier, J.-F. Vitamin D limits inflammation-linked microRNA expression in adipocytes in vitro and in vivo: A new mechanism for the regulation of inflammation by vitamin D. Epigenetics 2018, 13, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Staud, R. Fibromyalgia pain: Do we know the source? Curr. Opin. Rheumatol. 2004, 16, 157–163. [Google Scholar] [CrossRef]
- Atherton, K.; Berry, D.J.; Parsons, T.; Macfarlane, G.J.; Power, C.; Hypponen, E. Vitamin D and chronic widespread pain in a white middle-aged British population: Evidence from a cross-sectional population survey. Ann. Rheum. Dis. 2008, 68, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Bjurstrom, M.F.; Giron, S.E.; Griffis, C.A. Cerebrospinal Fluid Cytokines and Neurotrophic Factors in Human Chronic Pain Populations: A Comprehensive Review. Pain Pr. 2014, 16, 183–203. [Google Scholar] [CrossRef]
- Qu, K.; Li, M.-X.; Zhou, Y.-L.; Yu, P.; Dong, M. The efficacy of vitamin D in treatment of fibromyalgia: A meta-analysis of randomized controlled studies and systematic review. Expert Rev. Clin. Pharmacol. 2022, 15, 433–442. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 89, 105906. [Google Scholar]
- Warner, A.E.; Arnspiger, S.A. Diffuse Musculoskeletal Pain Is Not Associated With Low Vitamin D Levels or Improved by Treatment With Vitamin D. Am. J. Clin. Oncol. 2008, 14, 12–16. [Google Scholar] [CrossRef]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Effect of vitamin D supplementation in chronic widespread pain: A systematic review and meta-analysis. Clin. Rheumatol. 2017, 36, 2825–2833. [Google Scholar] [CrossRef]
- Abou-Raya, S.; Abou-Raya, A.; Helmii, M. THU0327 Efficacy of Vitamin D Supplementation in the Treatment of Fibromyalgia: Randomized Controlled Trial. Ann. Rheum. Dis. 2014, 73, 295. [Google Scholar] [CrossRef]
- Al-Allaf, A.W.; Mole, P.A.; Paterson, C.R.; Pullar, T. Fibromyalgia, bone density and vitamin D deficiency. J. Bone Miner. Res. 2002, 17, 1333. [Google Scholar]
- Al-Allaf, A.W.; Mole, P.A.; Paterson, C.R.; Pullar, T. Fibromyalgia, bone density and vitamin D deficiency. Ann. Rheum. Dis. 2003, 62, 307. [Google Scholar]
- Al-Dabbagh, T.Q. The relation between vitamin D deficiency and fibromyalgia syndrome. Saudi Med. J. 2012, 33, 331. [Google Scholar] [PubMed]
- Aldaoseri, H.A.; Zubairi, M.B. Vitamin D deficiency and treatment in Iraqi patients with primary fibromyalgia syndrome. Egypt. Rheumatol. 2020, 42, 47–50. [Google Scholar] [CrossRef]
- Ali, O.M.E. Prevalence of Vitamin D Deficiency and Its Relationship with Clinical Outcomes in Patients with Fibromyalgia: A Systematic Review of the Literature. SN Compr. Clin. Med. 2022, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Balkarli, A.; Akyol, M.; Tepeli, E.; Balkarli, H.; Temel, S.; Cobankara, V. Haplotypes of vitamin d receptor gene: Both risky and protective for fibromiyalgia (FMS). Ann. Rheum. Dis. 2016, 75, 391–392. [Google Scholar] [CrossRef]
- Block, S.R. Vitamin D deficiency is not associated with nonspecific musculoskeletal pain syndromes including fibromyalgia. Mayo Clin Proc 2004, 79, 1585–1586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, A.L.; Rooney, T.W.; Brown, J. Fibromyalgia and vitamin D deficiency: Is there a correlation. Arthritis Rheum. 2004, 50, S306–S307. [Google Scholar]
- De Carvalho, J.F.; da Rocha Araújo, F.A.G.; da Mota, L.M.A.; Aires, R.B.; de Araujo, R.P. Vitamin D Supplementation Seems to Improve Fibromyalgia Symptoms: Preliminary Results. Isr. Med. Assoc. J. 2018, 20, 379–381. [Google Scholar] [PubMed]
- Cassisi, G.; Ceccherelli, F.; Atzeni, F.; Sarzi-Puttini, P. Complementary and alternative medicine in fibromyalgia: A practical clinical debate of agreements and contrasts. Clin. Exp. Rheumatol. 2013, 31, S134–S152. [Google Scholar]
- Daniel, D.; Pirotta, M.V. Fibromyalgia—Should we be testing and treating for vitamin D deficiency? Aust. Fam. Physician 2011, 40, 712–716. [Google Scholar] [PubMed]
- Dogru, A.; Balkarli, A.; Çobankara, V.; Sahin, M.; Tunc, S. Effects of vitamin d therapy on quality of life in patients with fibromyalgia [Conference Object]. Ann. Rheum. Dis. 2016. [Google Scholar]
- D’Souza, R.S.; Lin, G.; Oh, T.; Vincent, A.; Orhurhu, V.; Jiang, L.; Mauck, W.D.; Qu, W. Fibromyalgia Symptom Severity and Psychosocial Outcomes in Fibromyalgia Patients with Hypovitaminosis D: A Prospective Questionnaire Study. Pain Med. 2020, 21, 3470–3478. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.D.; Kelly, S.T.; Shurlock, J.H.; Hepburn, A.L.N. The role of vitamin D testing and replacement in fibromyalgia: A systematic literature review. BMC Rheumatol. 2018, 2, 28. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, M.Y.; Hung, C.Y.; Chang, K.V.; Han, D.S.; Wang, T.G. Is serum hypovitaminosis D associated with chronic widespread pain including fibromyalgia? A meta-analysis of observational studies. Pain Physician 2015, 18, E877–E887. [Google Scholar]
- Huisman, A.M.; White, K.P.; Algra, A.; Harth, M.; Vieth, R.; Jacobs, J.W.G.; Bijlsma, J.W.J.; Bell, D.A. Vitamin D in female systemic lupus erythematosus and fibromyalgia patients. Arthritis Rheum. 2000, 43, S248. [Google Scholar]
- Ibáñez-Vera, A.J.; Alvero-Cruz, J.R.; García-Romero, J.C. Therapeutic physical exercise and supplements to treat fibromyalgia. Apunt. Med. l’Esport 2018, 53, 33–41. [Google Scholar] [CrossRef]
- Jesus, C.A.S.; Feder, D.; Peres, M.F.P. The Role of Vitamin D in Pathophysiology and Treatment of Fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 1–7. [Google Scholar] [CrossRef]
- Kadayifci, F.Z.; Bradley, M.J.; Onat, A.M.; Shi, H.N.; Zheng, S.S. Review of nutritional approaches to fibromyalgia. Nutr. Rev 2022, 80, 2260–2274. [Google Scholar] [CrossRef]
- Karras, S.; Rapti, E.; Matsoukas, S.; Kotsa, K. Vitamin D in fibromyalgia: A causative or confounding biological interplay? Nutrients 2016, 8, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Sukumaran, S.; Apostolos, V. Early replacement of vitamin D in vitamin D-deficient fibromyalgia patients improves reported pain and number of tender points. Rheumatology 2016, 55, 181. [Google Scholar]
- Lewis, J.M.; Coley, J.L.B.; Fontrier, T.H. Fibromyalgia syndrome and Vitamin D. J. Musculoskelet. Pain 2011, 19, 164–166. [Google Scholar] [CrossRef]
- Lombardo, M.; Feraco, A.; Ottaviani, M.; Rizzo, G.; Camajani, E.; Caprio, M.; Armani, A. The Efficacy of Vitamin D Supplementation in the Treatment of Fibromyalgia Syndrome and Chronic Musculoskeletal Pain. Nutrients 2022, 14, 3010. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.L.; Tian, X.Y.; Wang, Y.Q.; Zhang, H.F.; Zhang, L. Vitamin D supplementation prevents placental ischemia induced endothelial dysfunction by downregulating placental soluble FMS-like tyrosine kinase-1. DNA Cell Biol. 2017, 36, 1134–1141. [Google Scholar] [CrossRef]
- Maraslı, E.; Ozdolap, S.; Sarıkaya, S. Relationship between FokI polymorphism in the vitamin D receptor gene and fibromyalgia syndrome. Int. J. Rheum. Dis. 2016, 19, 1063–1068. [Google Scholar] [CrossRef]
- Martin, L.; Kaplan, B.J. Potential clinical benefit of nutritional supplements in the management of fibromyalgia. J. Musculoskelet. Pain 1999, 7, 125–130. [Google Scholar] [CrossRef]
- Martins, Y.A.; Cardinali, C.A.E.F.; Ravanelli, M.I.; Brunaldi, K. Is hypovitaminosis D associated with fibromyalgia? A systematic review. Nutr. Rev. 2020, 78, 115–133. [Google Scholar] [CrossRef] [PubMed]
- Matthana, M.H. The relation between vitamin D deficiency and fibromyalgia syndrome in women. Saudi Med. J. 2011, 32, 925–929. [Google Scholar] [PubMed]
- Matthana, M.H. The relation between vitamin D deficiency and fibromyalgia syndrome Reply. Saudi Med. J. 2012, 33, 331–332. [Google Scholar]
- Miao, E.Y. How do you treat fibromyalgia in your practice? Med. Acupunct. 2008, 20, 143. [Google Scholar] [CrossRef]
- Moreno García, M.S.; Del Río-Martínez, P.S.; Baltanás Rubio, P. Fibromyalgia and vitamin D levels. Rev. La Soc. Esp. Dolor 2017, 24, E877–E887. [Google Scholar] [CrossRef]
- Motley, C.P.; Maxwell, M.L. Fibromyalgia: Helping your patient while maintaining your sanity. Prim. Care Clin. Off. Pract. 2010, 37, 743–755. [Google Scholar] [CrossRef] [PubMed]
- Mytton, J.; Frater, A.P.; Oakley, G.; Murphy, E.; Barber, M.J.; Jahfar, S. Vitamin D deficiency in multicultural primary care: A case series of 299 patients. Br. J. Gen. Pract. 2007, 57, 577–579. [Google Scholar] [PubMed]
- NCT. Valuation of Efficacy and Safety of Vitamin D3 Use in 80 Women Diagnosed With Fibromyalgia. Using FIQ Score and VAS. 2017. Available online: https://clinicaltrials.gov/show/NCT03369379 (accessed on 7 March 2023).
- Padidela, R.; Nilsson, O.; Makitie, O.; Beck-Nielsen, S.; Ariceta, G.; Schnabel, D.; Brandi, M.L.; Boot, A.; Levtchenko, E.; Smyth, M.; et al. The international X-linked hypophosphataemia (XLH) registry (NCT03193476): Rationale for and description of an international, observational study. Orphanet. J. Rare. Dis. 2020, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Giangrandi, I.; Dinu, M.; Sofi, F.; Colombini, B. Nutritional Interventions in the Management of Fibromyalgia Syndrome. Nutrients 2020, 12, 2525. [Google Scholar] [CrossRef] [PubMed]
- Parvez, S.; Fatima, G.; Mehdi, F.; Hadi, N.R.; Fedacko, J. Relationship Between Vitamin D Receptor Gene BsmI Polymorphism and Fibromyalgia Syndrome. Cureus 2022, 14, e27113. [Google Scholar] [CrossRef]
- Plotnikoff, G.A. Vitamin D deficiency is not associated with nonspecific musculoskeletal pain syndromes including fibromyalgia—Reply. Mayo Clin. Proc. 2004, 79, 1586–1587. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Di Lollo, A.C.; Guzzo, M.P.; Giacomelli, C.; Atzeni, F.; Bazzichi, L.; Di Franco, M. Fibromyalgia and nutrition: What news? Clin. Exp. Rheumatol. 2015, 33, S117–S125. [Google Scholar]
- Scheuer, R. Fibromyalgia: Could vitamin D help? Int. J. Clin. Rheumatol. 2014, 9, 237–239. [Google Scholar] [CrossRef]
- Shanmuganandan, K.; Kartik, S. Vitamin D deficiency: A ‘Blindspot’ for clinicians and a veritable ‘Ray’ of hope for patients with chronic musculoskeletal pains? Indian J. Rheumatol. 2012, 7, 189–190. [Google Scholar] [CrossRef]
- Siracusa, R.; Di Paola, R.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, mechanisms, diagnosis and treatment options update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef]
- Sousa, H.; Pinto, A.S.; Ferreira, J.F. Vitamin D supplementation in fibromyalgia: A systematic review. Ann. Rheum. Dis. 2022, 81, 1721–1722. [Google Scholar] [CrossRef]
- Spaeth, M. Fibromyalgia syndrome review. J. Musculoskelet. Pain 2007, 15, 55–62. [Google Scholar] [CrossRef]
- Straube, S.; Moore, R.A.; Derry, S.; McQuay, H.J. Vitamin D and chronic pain. Pain 2009, 141, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Straube, S.; Derry, S.; Straube, C.; Moore, R.A. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst. Rev. 2015, 2015, CD007771. [Google Scholar] [CrossRef]
- Talotta, R.; Bazzichi, L.; Di Franco, M.; Casale, R.; Batticciotto, A.; Gerardi, M.C.; Sarzi-Puttini, P. One year in review 2017: Fibromyalgia. Clin. Exp. Rheumatol. 2017, 35, 6–12. [Google Scholar] [PubMed]
- Türkyilmaz, A.K.; Yalçinkaya, E.Y.; Öneş, K. The effects of bone mineral density and level of serum vitamin-D on pain and quality of life in fibromialgia patients. Osteoporoz Dunya. 2010, 16, 53–57. [Google Scholar]
- Vasquez, A. Neuroinflammation in fibromyalgia and CRPS is multifactorial. Nat. Rev. Rheumatol. 2016, 12, 242. [Google Scholar] [CrossRef] [PubMed]
- Velozo, E.; Recalde, M.C.; Burgos, L.; Rafaelli, S.; Rosa, J.; Soriano, E.; Catoggio, L.; Plantalech, L. Vitamin D levels on patients with Fibromyalgia. Bone 2008, 43, S131. [Google Scholar] [CrossRef]
- Venkatesan, N.; Gyawali, M.; Botleroo, R.A.; Ahmed, R.; Kareem, R.; Ogeyingbo, O.D.; Bhandari, R.; Elshaikh, A.O. Efficacy of Vitamin D Supplementation in the Improvement of Clinical Status in Pa-tients Diagnosed with Fibromyalgia Syndrome: A Systematic Review. Curr. Rheumatol. Rev. 2022, 18, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Vittorio, S.; Erica, S.; Cinzia, C.; Alvise, M.; Elena, M.; Alessandro, P.; Enrico, P.; Katia, D.; Teresa, V.M.; Luca, D.C. Comparison between Acupuncture and Nutraceutical Treatment with Migratens((R)) in Patients with Fibromyalgia Syndrome: A Prospective Randomized Clinical Trial. Nutrients 2020, 12, 821. [Google Scholar] [CrossRef] [Green Version]
- Warner, A.E.; Amspiger, S.A. Treatment with vitamin D does not reduce pain in fibromyalgia patients with low vitamin D levels. Arthritis Rheum. 2005, 52, S517. [Google Scholar]
- Wu, Z.Q.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.M.; Scragg, R. Effect of Vitamin D Supplementation on Pain: A Systematic Review and Meta-analysis. Pain Physician 2016, 19, 415–427. [Google Scholar]
- Zabihiyeganeh, M. Effects of vitamin D on quality of life in fibromyalgia patients: A randomized controlled trial. Osteoporos. Int. 2015, 26, S108–S109. [Google Scholar] [CrossRef]
- Zdebik, N.; Zdebik, A.; Boguslawska, J.; Przezdziecka-Dolyk, J.; Turno-Krecicka, A. Fibromyalgia syndrome and the eye-A review. Surv. Ophthalmol. 2021, 66, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar] [CrossRef]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Arvold, D.S.; Odean, M.J.; Dornfeld, M.P.; Regal, R.R.; Arvold, J.G.; Karwoski, G.C.; Mast, D.J.; Sanford, P.B.; Sjoberg, R.J. Correlation of Symptoms with Vitamin D Deficiency and Symptom Response to Cholecalciferol Treatment: A Randomized Controlled Trial. Endocr. Pr. 2009, 15, 203–212. [Google Scholar] [CrossRef]
- Wepner, F.; Scheuer, R.; Schuetz-Wieser, B.; Machacek, P.; Pieler-Bruha, E.; Cross, H.S.; Hahne, J.; Friedrich, M. Effects of vitamin D on patients with fibromyalgia syndrome: A randomized placebo-controlled trial. Pain 2014, 155, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, A.; Zabihiyeganeh, M.; Jahed, S.A.; Khiabani, E.; Nojomi, M.; Ghaffari, S. Effects of vitamin D optimization on quality of life of patients with fibromyalgia: A randomized controlled trial. Med J. Islam. Repub. Iran 2018, 32, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Lozano-Plata, L.I.; Vega-Morales, D.; Esquivel-Valerio, J.A.; Garza-Elizondo, M.A.; Galarza-Delgado, D.A.; Silva-Luna, K.; Serna-Peña, G.; Sifuentes-Ramírez, J.; Garza-Guerra, A.D.J.; de Rivera, R.D.-N. Efficacy and safety of weekly vitamin D3 in patients with fibromyalgia: 12-week, double-blind, randomized, controlled placebo trial. Clin. Rheumatol. 2021, 40, 3257–3264. [Google Scholar] [CrossRef]
- Knutsen, K.V.; Madar, A.A.; Brekke, M.; Meyer, H.E.; Natvig, B.; Mdala, I.; Lagerlv, P. Effect of vitamin D on musculoskeletal pain and headache: A randomized, double-blind, placebo-controlled trial among adult ethnic minorities in Norway. Pain 2014, 155, 2591–2598. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, R.; Salli, A.; Cingoz, H.T.; Kucuksen, S.; Ugurlu, H. Efficacy of vitamin D replacement therapy on patients with chronic nonspecific widespread musculoskeletal pain with vitamin D deficiency. Int. J. Rheum. Dis. 2016, 19, 1255–1262. [Google Scholar] [CrossRef] [Green Version]
- Dogru, A.; Balkarli, A.; Cobankara, V.; Tunc, S.E.; Sahin, M. Effects of Vitamin D Therapy on Quality of Life in Patients with Fibromyalgia. Eurasian J. Med. 2017, 49, 113–117. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Hauser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia Criteria and Severity Scales for Clinical and Epidemiological Studies: A Modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Von Hippel, P.T. The heterogeneity statistic I2 can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes Del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B. SF-36 Health Survey. Manual and Interpretation Guide; The Health Institute: Boston, MA, USA, 1993. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar]
- Walker, E.A.; Katon, W.J.; Jemelka, R.P.; Roy-Byrne, P.P. Comorbidity of gastrointestinal complaints, depression, and anxiety in the epidemiologic catchment area (ECA) study. Am. J. Med. 1992, 92, S26–S30. [Google Scholar] [CrossRef]
- McWilliams, L.; Cox, B.J.; Enns, M.W. Mood and anxiety disorders associated with chronic pain: An examination in a nationally representative sample. Pain 2003, 106, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Gureje, O.; Akinpelu, A.O.; Uwakwe, R.; Udofia, O.; Wakil, A. Comorbidity and Impact of Chronic Spinal Pain in Nigeria. Spine 2007, 32, E495–E500. [Google Scholar] [CrossRef]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Leuk. Res. 2014, 43, 476–493. [Google Scholar] [CrossRef] [Green Version]
- Ishak, W.W.; Wen, R.Y.; Naghdechi, L.; Vanle, B.; Dang, J.; Knosp, M.; Dascal, J.; Marcia, L.; Gohar, Y.; Eskander, L.; et al. Pain and Depression: A Systematic Review. Harv. Rev. Psychiatry 2018, 26, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M.; Browne, M.A.O.; McGee, M.A.; Wells, J.E. For The New Zealand Mental Health Survey Research Team Mental-Physical Comorbidity in Te Rau Hinengaro: The New Zealand Mental Health Survey. Aust. New Zealand J. Psychiatry 2006, 40, 882–888. [Google Scholar] [CrossRef]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and Pain Comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loggia, M.L.; Berna, C.; Kim, J.; Cahalan, C.M.; Gollub, R.L.; Wasan, A.D.; Harris, R.E.; Edwards, R.R.; Napadow, V. Disrupted Brain Circuitry for Pain-Related Reward/Punishment in Fibromyalgia. Arthritis Rheumatol. 2013, 66, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Martikainen, I.K.; Nuechterlein, E.B.; Peciña, M.; Love, T.M.; Cummiford, C.M.; Green, C.R.; Stohler, C.S.; Zubieta, J.-K. Chronic Back Pain Is Associated with Alterations in Dopamine Neurotransmission in the Ventral Striatum. J. Neurosci. 2015, 35, 9957–9965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, S.K.; Wood, C.S.; Lombard, C.M.; Lee, C.S.; Zhang, X.-Y.; Finnell, J.E.; Valentino, R.J. Inflammatory Factors Mediate Vulnerability to a Social Stress-Induced Depressive-like Phenotype in Passive Coping Rats. Biol. Psychiatry 2014, 78, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, A.K.; Kavelaars, A.; Heijnen, C.J.; Dantzer, R. Neuroinflammation and Comorbidity of Pain and Depression. Pharmacol. Rev. 2013, 66, 80–101. [Google Scholar] [CrossRef] [Green Version]
- Roughan, W.H.; Campos, A.I.; García-Marín, L.M.; Cuéllar-Partida, G.; Lupton, M.K.; Hickie, I.B.; Medland, S.E.; Wray, N.R.; Byrne, E.M.; Ngo, T.T.; et al. Comorbid Chronic Pain and Depression: Shared Risk Factors and Differential Antidepressant Effectiveness. Front. Psychiatry 2021, 12, 643609. [Google Scholar] [CrossRef]
- Uguz, F.; Çiçek, E.; Salli, A.; Karahan, A.Y.; Albayrak, I.; Kaya, N.; Uğurlu, H. Axis I and Axis II psychiatric disorders in patients with fibromyalgia. Gen. Hosp. Psychiatry 2010, 32, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Hudson, J.I.; Keck, P.E.; Auchenbach, M.B.; Javaras, K.N.; Hess, E.V. Comorbidity of Fibromyalgia and Psychiatric Disorders. J. Clin. Psychiatry 2006, 67, 1219–1225. [Google Scholar] [CrossRef]
- Aguglia, A.; Salvi, V.; Maina, G.; Rossetto, I.; Aguglia, E. Fibromyalgia syndrome and depressive symptoms: Comorbidity and clinical correlates. J. Affect. Disord. 2011, 128, 262–266. [Google Scholar] [CrossRef]
- Heaney, R.P. Vitamin D—Baseline Status and Effective Dose. New Engl. J. Med. 2012, 367, 77–78. [Google Scholar] [CrossRef] [Green Version]
- Spedding, S. Vitamin D and Depression: A Systematic Review and Meta-Analysis Comparing Studies with and without Biological Flaws. Nutrients 2014, 6, 1501–1518. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Kahlon, A.S.; Irving, K.; Hampson, G.; Garrood, T. 279. Association Between Vitamin D and Multiple Symptom Domains in Fibromyalgia. Rheumatology 2015, 54, i158. [Google Scholar] [CrossRef] [Green Version]
- Ozkan, A.; Kocyigit, H.; Askin, A. Relationship between seasonal serum 25-hydroxyvitamin d levels and disease activity in patients with ankylosing spondylitis, osteoarthritis and fibromyalgia syndrome. J. Clin. Anal. Med. 2017, 8, 523–528. [Google Scholar]
- Özcan, D.S.; Aras, M.; Koseoglu, B.F. Vitamin D Levels in Women with Fibromyalgia and Relationship between Pain, Depression, and Sleep. Turk. J. Phys. Med. Rehabil. 2014, 60, 329–334. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Study Design | FMS Diagnostic Criteria | Participants (N) | Age | Dose of Vitamin D | Assessment | Major Findings | Duration |
|---|---|---|---|---|---|---|---|---|---|---|
| Tx/Placebo | Mean (SD) | Weeks | ||||||||
| Warner [31] | 2008 | USA | RCT | 1990 ACR criteria | 22/20 | 57.4 (9.3) | 50,000 IU/week | VAS | No difference in the VAS | 12 |
| Arvold [92] | 2009 | USA | RCT | Not mentioned | 48/42 | 59.7 (14.0) | 50,000 IU/week | FIQ | The treatment group showed mild short-term improvement in the overall FIQ | 8 |
| Wepner [93] | 2014 | Austria | RCT | 1990 or 2010 ACR criteria | 15/15 | 48.4 (5.3) | 50,000 IU/week | VAS, FIQ, SF-36 | Treatment group showed marked reduction in VAS, with better physical functioning scale in SF-36 | 20 |
| Knutsen [96] | 2014 | Norway | RCT | Not mentioned | 144/71 | 36 (3) | 1000 IU/day | VAS | Treatment group showed improved pain scores and headache scores | 16 |
| Mirzaei [94] | 2018 | Iran | RCT | 2010 ACR criteria | 37/37 | 42.1 (10.8) | 50,000 IU/week | FIQ, SF-36, WPI, PSQI | Improvement in FIQ, WPI, PSQI scores in both groups; (patients of both groups took Trazodone 25 mg before sleep) | 8 |
| Lozano-Plata [95] | 2020 | Mexico | RCT | 1990 or 2010 ACR criteria | 39/40 | 50.3 (11.9) | 50,000 IU/week | VAS, FIQ | No difference in the VAS or FIQ | 12 |
| Yilmaz [97] | 2016 | Turkey | Prospective | 1990 ACR criteria | 58/0 | 36.9 (9.2) | 50,000 IU/week | VAS, SF-36, BDI | Reduced in VAS, BDI, improved in some subgroups of SF-36 | 12 |
| Dogru [98] | 2017 | Turkey | Prospective | 2010 ACR criteria | 70/0 | 38.7 (5.2) | 50,000 IU/week | VAS, FIQ, SF-36, BDI | No difference in VAS, FIQ, BDI, improved in overall SF-36 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.-C.; Tsai, S.-T.; Ting, B.; Cheng, Y.-C.; Wang, C.-K.; Chang, J.P.-C.; Su, K.-P. Psychological Outcomes and Quality of Life of Fibromyalgia Patients with Vitamin D Supplementation—A Meta-Analysis. J. Clin. Med. 2023, 12, 2750. https://doi.org/10.3390/jcm12072750
Yang C-C, Tsai S-T, Ting B, Cheng Y-C, Wang C-K, Chang JP-C, Su K-P. Psychological Outcomes and Quality of Life of Fibromyalgia Patients with Vitamin D Supplementation—A Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2750. https://doi.org/10.3390/jcm12072750
Chicago/Turabian StyleYang, Chia-Chun, Sheng-Ta Tsai, Berne Ting, Ying-Chih Cheng, Chin-Kun Wang, Jane Pei-Chen Chang, and Kuan-Pin Su. 2023. "Psychological Outcomes and Quality of Life of Fibromyalgia Patients with Vitamin D Supplementation—A Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2750. https://doi.org/10.3390/jcm12072750