
Evaluation of Different Contrast Agents for Regional Lung Perfusion Measurement Using Electrical Impedance Tomography: An Experimental Pilot Study


Abstract
:1. Introduction
2. Animals and Methods
2.1. Animal Preparation and Ethics
2.2. Measurement and Data Acquisition
2.2.1. Electrical Impedance Tomography
2.2.2. Contrast Agents
- NaCl 5.85%; ready-to-use hypertonic (1 mmol/mL) sodium-chloride solution, clinically used for the substitution of sodium (Natriumchlorid 5.85% Braun Mpc, B. Braun Melsungen AG, Melsungen, Germany).
- NaBic (sodium-bicarbonate) 8.4%, ready-to-use hypertonic buffer solution, clinically used for correction of the acid-base balance (Natriumhydrogencarbonat 8.4%, B. Braun Melsungen AG, Melsungen, Germany).
- Jonosteril; ready-to-use iso-tonic, balanced crystalloid solution, clinically used for intravascular volume replacement (Jonosteril®, Fresenius Kabi, Bad Homburg, Germany).
- Glucose 5%; ready-to-use ion-free isotonic glucose solution, clinically used as carrier solution for intravenous drug administration (Glucose 5%, B. Braun Melsungen AG, Melsungen, Germany).
- Iomeprol 400 mg/mL; ready-to-use non-ionic but iodinated X-ray contrast medium, clinically used for angiography (Imeron® 400 MCT, Bracco Imaging Deutschland GmbH, Konstanz, Germany).
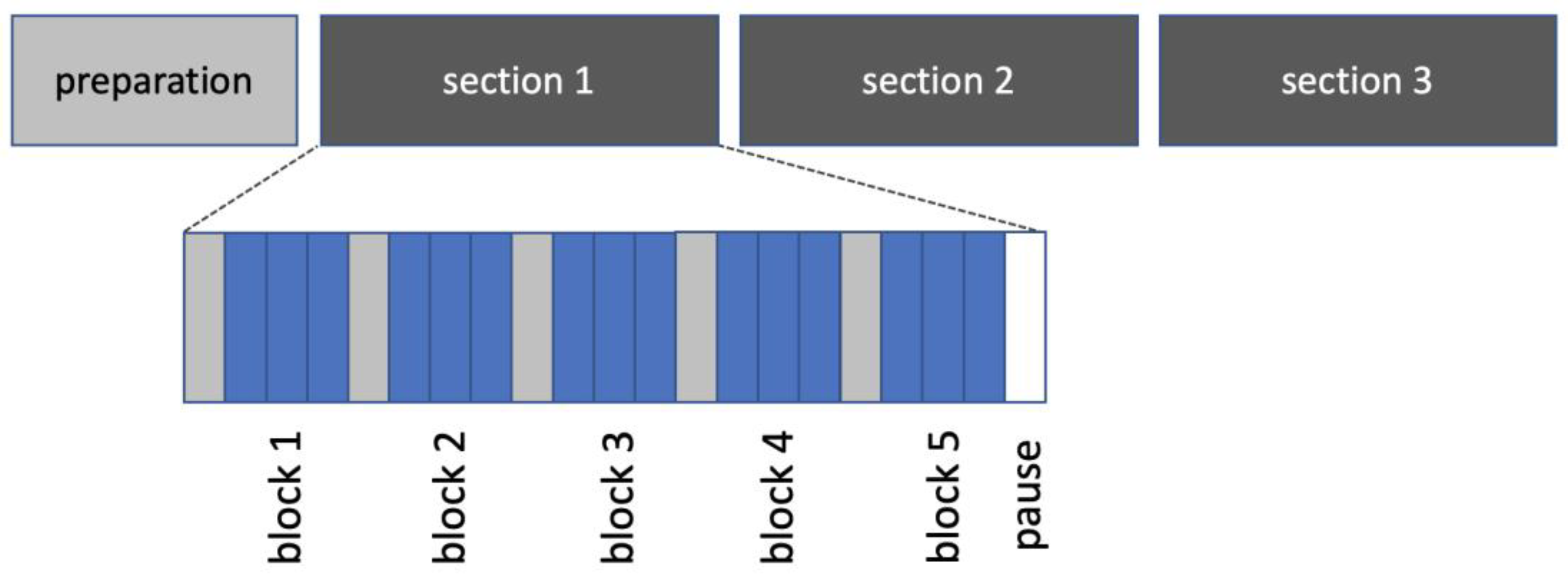
2.2.3. Experimental Protocol
2.3. Data Processing and Analyses
2.3.1. Extraction of Regional Perfusion Images
2.3.2. Success Rate
2.3.3. Regional Signal Strength
2.3.4. Image Quality
2.4. Statistical Analyses
3. Results
3.1. Success Rate of Perfusion Image Extraction
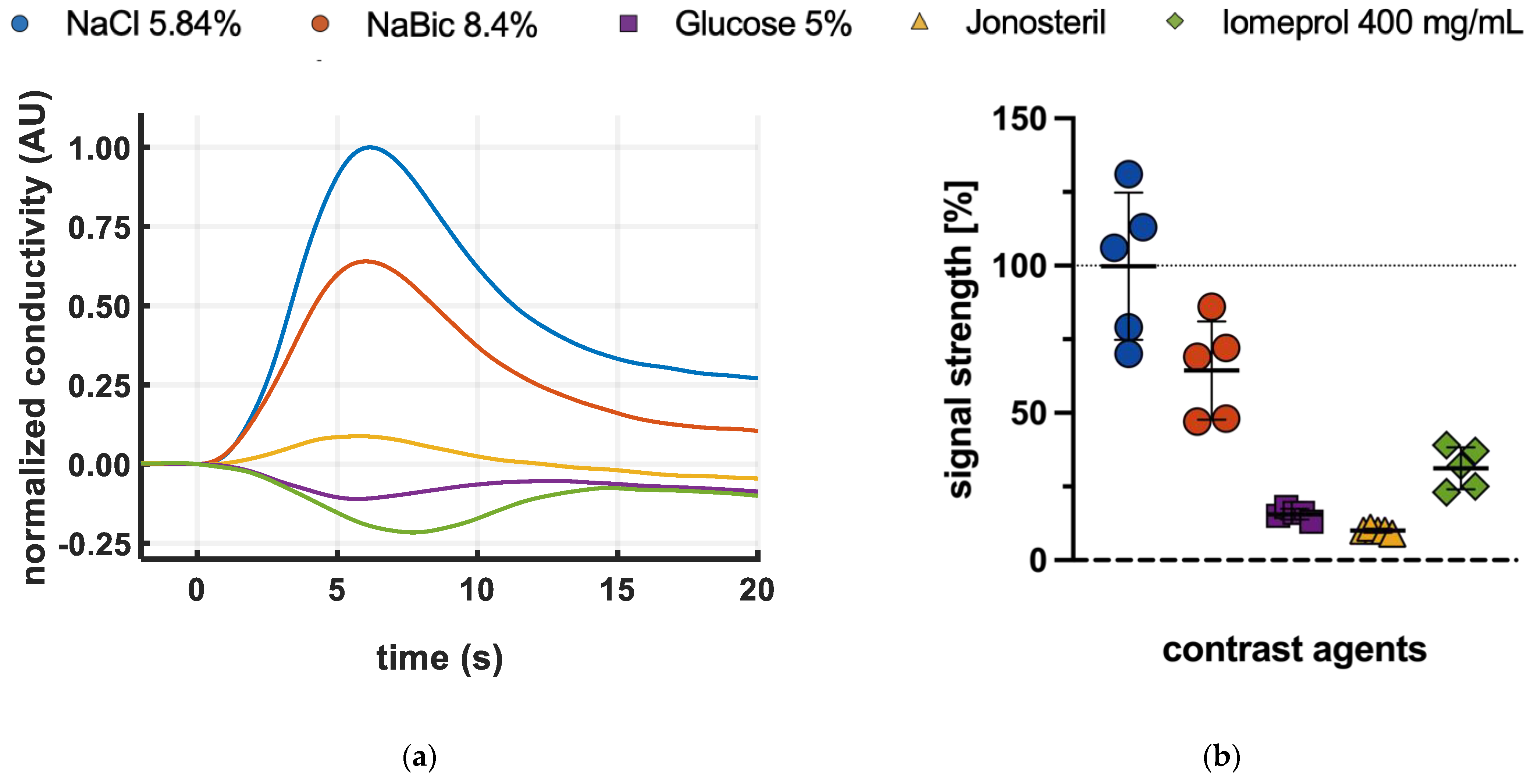
3.2. Global Conductivity Changes and Regional Signal Strength
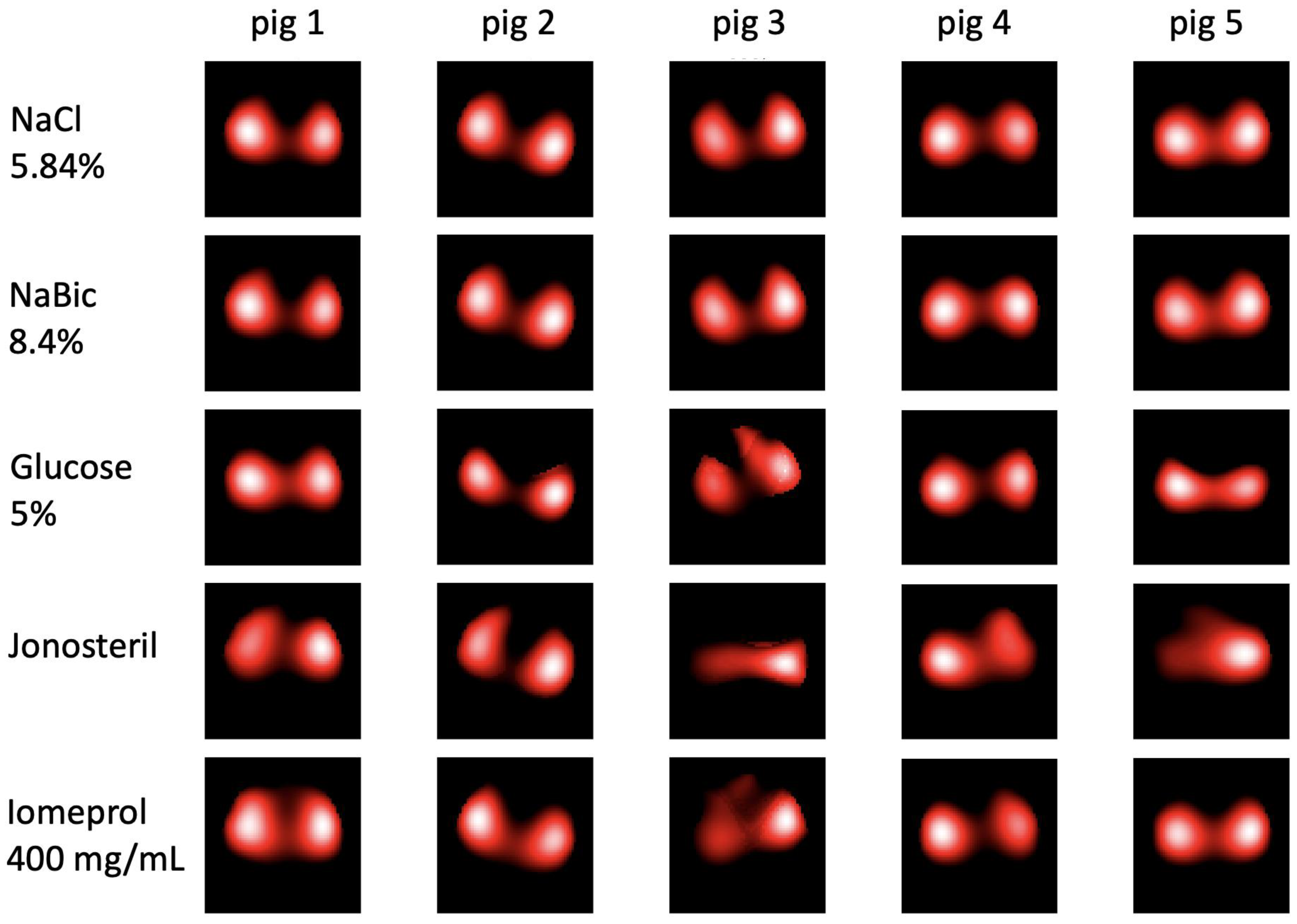
3.3. Regional Perfusion Images
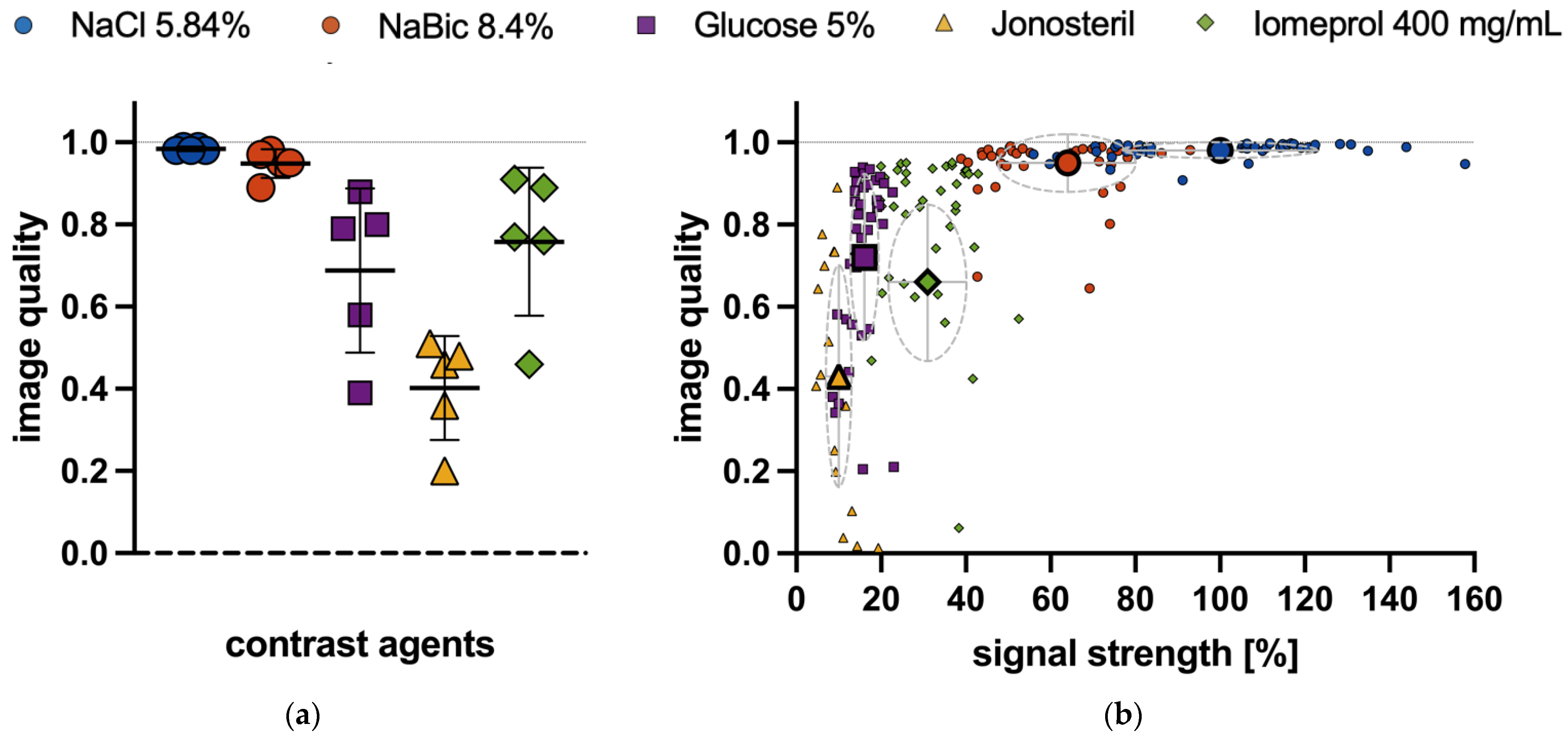
3.4. Quality of Regional Perfusion Images
4. Discussion
- Blood resistivity results predominantly from the electrical resistance of the erythrocytes and is therefore dependent on the hematocrit. Each bolus injection of an erythrocyte-free solution causes hematocrit dilution and consequently a reduced resistivity according to an increased conductivity (conductivity = 1/resistivity) [20]. This effect is enhanced by the use of a hyperosmolar fluid, as intravascular water shift increases hematocrit dilution [20].
- Blood conductivity is linearly related to ion concentration [20]. Injection of hypertonic ion solution increases blood conductivity, whereas conductivity is decreased by hypotonic or ion-free indicators.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersson, J.; Glenny, R.W. Gas Exchange and Ventilation-Perfusion Relationships in the Lung. Eur. Respir. J. 2014, 44, 1023–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, A.R.; Burrowes, K.S.; Tawhai, M.H. Ventilation/Perfusion Matching: Of Myths, Mice, and Men. Physiology 2019, 34, 419–429. [Google Scholar] [CrossRef]
- Suárez-Sipmann, F.; Villar, J.; Ferrando, C.; Sánchez-Giralt, J.A.; Tusman, G. Monitoring Expired CO2 Kinetics to Individualize Lung-Protective Ventilation in Patients with the Acute Respiratory Distress Syndrome. Front. Physiol. 2021, 12, 785014. [Google Scholar] [CrossRef]
- Bitker, L.; Talmor, D.; Richard, J.-C. Imaging the Acute Respiratory Distress Syndrome: Past, Present and Future. Intensive Care Med. 2022, 48, 995–1008. [Google Scholar] [CrossRef]
- Muders, T.; Luepschen, H.; Meier, T.; Reske, A.W.; Zinserling, J.; Kreyer, S.; Pikkemaat, R.; Maripu, E.; Leonhardt, S.; Hedenstierna, G.; et al. Individualized Positive End-Expiratory Pressure and Regional Gas Exchange in Porcine Lung Injury. Anesthesiology 2020, 132, 808–824. [Google Scholar] [CrossRef] [PubMed]
- Putensen, C.; Hentze, B.; Muenster, S.; Muders, T. Electrical Impedance Tomography for Cardio-Pulmonary Monitoring. J. Clin. Med. 2019, 8, 1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frerichs, I.; Amato, M.B.P.; van Kaam, A.H.; Tingay, D.G.; Zhao, Z.; Grychtol, B.; Bodenstein, M.; Gagnon, H.; Böhm, S.H.; Teschner, E.; et al. Chest Electrical Impedance Tomography Examination, Data Analysis, Terminology, Clinical Use and Recommendations: Consensus Statement of the TRanslational EIT DevelopmeNt StuDy Group. Thorax 2016, 72, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Brown, B.H.; Leathard, A.D.; Sinton, A.; McArdle, F.J.; Smith, R.W.; Barber, D.C. Blood Flow Imaging Using Electrical Impedance Tomography. Clin. Phys. Physiol. Meas. 1992, 13, 175–179. [Google Scholar] [CrossRef]
- Frerichs, I.; Hinz, J.; Herrmann, P.; Weisser, G.; Hahn, G.; Quintel, M.; Hellige, G. Regional Lung Perfusion as Determined by Electrical Impedance Tomography in Comparison with Electron Beam CT Imaging. IEEE Trans. Med. Imaging 2002, 21, 646–652. [Google Scholar] [CrossRef]
- Hentze, B.; Muders, T.; Luepschen, H.; Maripuu, E.; Hedenstierna, G.; Putensen, C.; Walter, M.; Leonhardt, S. Regional Lung Ventilation and Perfusion by Electrical Impedance Tomography Compared to Single-Photon Emission Computed Tomography. Physiol. Meas. 2018, 39, 065004. [Google Scholar] [CrossRef]
- Hentze, B.; Muders, T.; Antink, C.H.; Putensen, C.; Larsson, A.; Hedenstierna, G.; Walter, M.; Leonhardt, S. A Model-Based Source Separation Algorithm for Lung Perfusion Imaging Using Electrical Impedance Tomography. Physiol. Meas. 2021, 42, 084001. [Google Scholar] [CrossRef] [PubMed]
- Bluth, T.; Kiss, T.; Kircher, M.; Braune, A.; Bozsak, C.; Huhle, R.; Scharffenberg, M.; Herzog, M.; Roegner, J.; Herzog, P.; et al. Measurement of Relative Lung Perfusion with Electrical Impedance and Positron Emission Tomography: An Experimental Comparative Study in Pigs. Br. J. Anaesth. 2019, 123, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Borges, J.B.; Suarez-Sipmann, F.; Bohm, S.H.; Tusman, G.; Melo, A.; Maripuu, E.; Sandström, M.; Park, M.; Costa, E.L.V.; Hedenstierna, G.; et al. Regional Lung Perfusion Estimated by Electrical Impedance Tomography in a Piglet Model of Lung Collapse. J. Appl. Physiol. 2012, 112, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Kircher, M.; Elke, G.; Stender, B.; Hernandez Mesa, M.; Schuderer, F.; Dossel, O.; Fuld, M.K.; Halaweish, A.F.; Hoffman, E.A.; Weiler, N.; et al. Regional Lung Perfusion Analysis in Experimental ARDS by Electrical Impedance and Computed Tomography. IEEE Trans. Med. Imaging 2021, 40, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Fossali, T.; Pavlovsky, B.; Ottolina, D.; Colombo, R.; Basile, M.C.; Castelli, A.; Rech, R.; Borghi, B.; Ianniello, A.; Flor, N.; et al. Effects of Prone Position on Lung Recruitment and Ventilation-Perfusion Matching in Patients with COVID-19 Acute Respiratory Distress Syndrome: A Combined CT Scan/Electrical Impedance Tomography Study. Crit. Care Med. 2022, 50, 723. [Google Scholar] [CrossRef]
- Spinelli, E.; Kircher, M.; Stender, B.; Ottaviani, I.; Basile, M.C.; Marongiu, I.; Colussi, G.; Grasselli, G.; Pesenti, A.; Mauri, T. Unmatched Ventilation and Perfusion Measured by Electrical Impedance Tomography Predicts the Outcome of ARDS. Crit. Care 2021, 25, 192. [Google Scholar] [CrossRef]
- Mauri, T.; Spinelli, E.; Scotti, E.; Colussi, G.; Basile, M.C.; Crotti, S.; Tubiolo, D.; Tagliabue, P.; Zanella, A.; Grasselli, G.; et al. Potential for Lung Recruitment and Ventilation-Perfusion Mismatch in Patients with the Acute Respiratory Distress Syndrome from Coronavirus Disease 2019. Crit. Care Med. 2020, 48, 1129–1134. [Google Scholar] [CrossRef]
- Kien, N.D.; Kramer, G.C. Cardiac Performance Following Hypertonic Saline. Braz. J. Med. Biol. Res. 1989, 22, 245–248. [Google Scholar]
- Pfortmueller, C.A.; Uehlinger, D.; von Haehling, S.; Schefold, J.C. Serum Chloride Levels in Critical Illness—The Hidden Story. Intensive Care Med. Exp. 2018, 6, 10. [Google Scholar] [CrossRef]
- Hellige, N.C.; Meyer, B.; Rodt, T.; Vogel-Claussen, J.; Hahn, G.; Hellige, G. In-Vitro Evaluation of Contrast Media for Assessment of Regional Perfusion Distribution by Electrical Impedance Tomography (EIT). Biomed. Eng./Biomed. Technol. 2012, 57, 525–528. [Google Scholar] [CrossRef]
- Muders, T.; Hentze, B.; Simon, P.; Girrbach, F.; Doebler, M.R.G.; Leonhardt, S.; Wrigge, H.; Putensen, C. A Modified Method to Assess Tidal Recruitment by Electrical Impedance Tomography. J. Clin. Med. 2019, 8, 1161. [Google Scholar] [CrossRef] [Green Version]
- Institute of Laboratory Animal Resources; National Research Council (Eds.) Guide for the Care and Use of Laboratory Animals, 6th ed.; National Acad. Press: Washington, DC, USA, 1996; ISBN 978-0-309-05377-8. [Google Scholar]
- Adler, A.; Lionheart, W.R.B. Uses and Abuses of EIDORS: An Extensible Software Base for EIT. Physiol. Meas. 2006, 27, S25–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, M.; Ong, V.; Florence, T.J.; Mozaffari, K.; Mahgerefteh, N.; Rana, S.; Duong, C.; Plurad, D.S.; Yang, I. Hypertonic Saline Treatment in Traumatic Brain Injury: A Systematic Review. World Neurosurg. 2022, 162, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Suarez, J.I.; Qureshi, A.I.; Bhardwaj, A.; Williams, M.A.; Schnitzer, M.S.; Mirski, M.; Hanley, D.F.; Ulatowski, J.A. Treatment of Refractory Intracranial Hypertension with 23.4% Saline. Crit. Care Med. 1998, 26, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-J.; Chang, L.; Han, Y.-Y.; Lee, Y.-C.; Tu, Y.-K. Efficacy and Safety of Hypertonic Saline Solutions in the Treatment of Severe Head Injury. Surg. Neurol. 2006, 65, 539–546. [Google Scholar] [CrossRef]
- Suetrong, B.; Pisitsak, C.; Boyd, J.H.; Russell, J.A.; Walley, K.R. Hyperchloremia and Moderate Increase in Serum Chloride Are Associated with Acute Kidney Injury in Severe Sepsis and Septic Shock Patients. Crit. Care 2016, 20, 315. [Google Scholar] [CrossRef] [Green Version]
- Yunos, N.M.; Bellomo, R.; Hegarty, C.; Story, D.; Ho, L.; Bailey, M. Association Between a Chloride-Liberal vs Chloride-Restrictive Intravenous Fluid Administration Strategy and Kidney Injury in Critically Ill Adults. JAMA 2012, 308, 1566. [Google Scholar] [CrossRef] [Green Version]
- Commereuc, M.; Nevoret, C.; Radermacher, P.; Katsahian, S.; Asfar, P.; Schortgen, F. HYPER2S investigators Hyperchloremia Is Not Associated with AKI or Death in Septic Shock Patients: Results of a Post Hoc Analysis of the “HYPER2S” Trial. Ann. Intensive Care 2019, 9, 95. [Google Scholar] [CrossRef] [Green Version]
- Huet, O.; Chapalain, X.; Vermeersch, V.; Moyer, J.-D.; Lasocki, S.; Cohen, B.; Dahyot-Fizelier, C.; Chalard, K.; Seguin, P.; Hourmant, Y.; et al. Impact of Continuous Hypertonic (NaCl 20%) Saline Solution on Renal Outcomes after Traumatic Brain Injury (TBI): A Post Hoc Analysis of the COBI Trial. Crit. Care 2023, 27, 42. [Google Scholar] [CrossRef]
- Fujii, T.; Udy, A.; Licari, E.; Romero, L.; Bellomo, R. Sodium Bicarbonate Therapy for Critically Ill Patients with Metabolic Acidosis: A Scoping and a Systematic Review. J. Crit. Care 2019, 51, 184–191. [Google Scholar] [CrossRef]
- Yagi, K.; Fujii, T. Management of Acute Metabolic Acidosis in the ICU: Sodium Bicarbonate and Renal Replacement Therapy. Crit. Care 2021, 25, 314. [Google Scholar] [CrossRef] [PubMed]
- Coppola, S.; Caccioppola, A.; Froio, S.; Chiumello, D. Sodium Bicarbonate in Different Critically Ill Conditions: From Physiology to Clinical Practice. Anesthesiology 2021, 134, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Bracco Imaging S.p.A. Available online: https://www.bracco.com/sites/default/files/2022-11/germany-imeron-spc-april-2022.pdf; (accessed on 4 April 2023).
- Biondi-Zoccai, G.; Lotrionte, M.; Thomsen, H.S.; Romagnoli, E.; D’Ascenzo, F.; Giordano, A.; Frati, G. Nephropathy after Administration of Iso-Osmolar and Low-Osmolar Contrast Media: Evidence from a Network Meta-Analysis. Int. J. Cardiol. 2014, 172, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Grychtol, B.; Lionheart, W.R.B.; Bodenstein, M.; Wolf, G.K.; Adler, A. Impact of Model Shape Mismatch on Reconstruction Quality in Electrical Impedance Tomography. IEEE Trans. Med. Imaging 2012, 31, 1754–1760. [Google Scholar] [CrossRef] [Green Version]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving Bioscience Research Reporting: The ARRIVE Guidelines for Reporting Animal Research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal | NaCl 5.85% | NaBic 8.4% | Glucose 5% | Jonosteril® | Imeron 400 MCT® | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| 1 | 9 | 100 | 9 | 100 | 9 | 100 | 4 | 44 | 8 | 89 |
| 2 | 9 | 100 | 9 | 100 | 9 | 100 | 6 | 67 | 9 | 100 |
| 3 | 9 | 100 | 9 | 100 | 4 | 44 | 2 | 22 | 4 | 44 |
| 4 | 9 | 100 | 9 | 100 | 9 | 100 | 3 | 33 | 9 | 100 |
| 5 | 9 | 100 | 9 | 100 | 9 | 100 | 4 | 44 | 9 | 100 |
| Mean | 9 | 100 | 9 | 100 | 8 | 89 | 3.8 | 42 | 7.8 | 87 |
| SD | 0 | 0 | 0 | 0 | 2.2 | 25 | 1.5 | 16 | 2.1 | 24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muders, T.; Hentze, B.; Leonhardt, S.; Putensen, C. Evaluation of Different Contrast Agents for Regional Lung Perfusion Measurement Using Electrical Impedance Tomography: An Experimental Pilot Study. J. Clin. Med. 2023, 12, 2751. https://doi.org/10.3390/jcm12082751
Muders T, Hentze B, Leonhardt S, Putensen C. Evaluation of Different Contrast Agents for Regional Lung Perfusion Measurement Using Electrical Impedance Tomography: An Experimental Pilot Study. Journal of Clinical Medicine. 2023; 12(8):2751. https://doi.org/10.3390/jcm12082751
Chicago/Turabian StyleMuders, Thomas, Benjamin Hentze, Steffen Leonhardt, and Christian Putensen. 2023. "Evaluation of Different Contrast Agents for Regional Lung Perfusion Measurement Using Electrical Impedance Tomography: An Experimental Pilot Study" Journal of Clinical Medicine 12, no. 8: 2751. https://doi.org/10.3390/jcm12082751