
Τhe Impact of Pre-Transplant Kidney Biopsy on the Evaluation of Prospective Living Kidney Donors
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
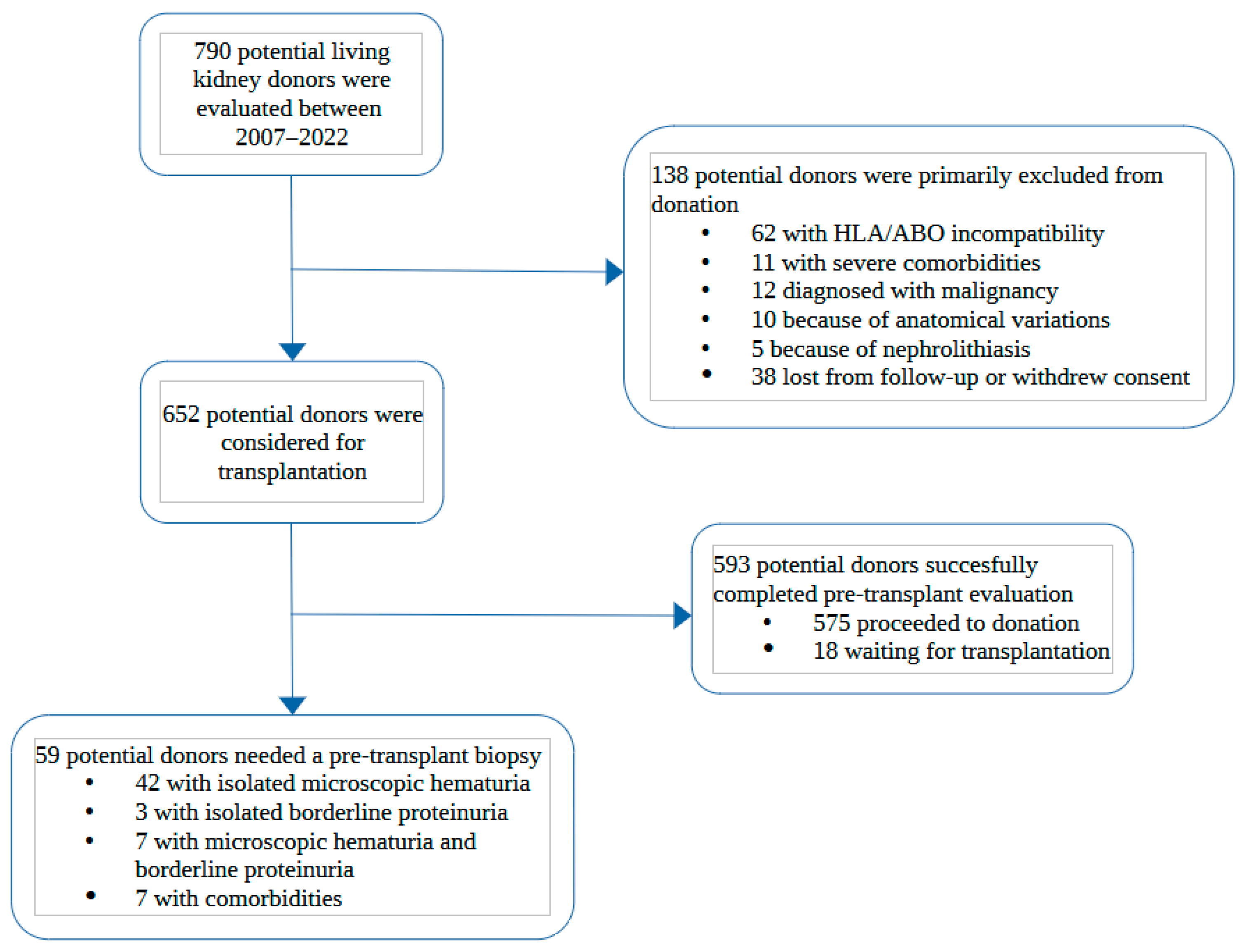
3.1. Characteristics of Potential Living Kidney Donors and Pre-Transplant Biopsy Indications
3.2. Biopsy Results and Exclusion from Donation
3.3. Post-Donation Follow-Up of Living Kidney Donors Who Underwent a Pre-Transplant Biopsy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared With Dialysis in Clinically Relevant Outcomes. Am. J. Transplant. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Diabetes and Digestive and Kidney Diseases. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health: Betehsda, MD, USA, 2022.
- Department of Medical Informatics. ERA Registry: ERA Registry Annual Report 2020; UMC, location AMC: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.-T.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101, S7. [Google Scholar] [CrossRef] [Green Version]
- Bolenz, C.; Schröppel, B.; Eisenhardt, A.; Schmitz-Dräger, B.J.; Grimm, M.O. The Investigation of Hematuria. Dtsch. Arztebl. Int. 2018, 115, 801–807. [Google Scholar]
- Chadban, S.J.; Briganti, E.M.; Kerr, P.G.; Dunstan, D.W.; Welborn, T.A.; Zimmet, P.Z.; Atkins, R.C. Prevalence of Kidney Damage in Australian Adults: The AusDiab Kidney Study. J. Am. Soc. Nephrol. 2003, 14, S131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, P.A.; Burnapp, L. British Transplantation Society/Renal Association UK Guidelines for Living Donor Kidney Transplantation 2018. Transplantation 2018, 102, e307. [Google Scholar] [CrossRef] [PubMed]
- Hassan, E.A.; Ali, T.Z.; Abdulbaki, A.; Ibrahim, I.A.; Almanae, H.M.; Aleid, H.A. Histopathologic Findings of Potential Kidney Donors With Asymptomatic Microscopic Hematuria: Impact on Donation. Transplant. Proc. 2017, 49, 1729–1732. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, M.; Sakai, K.; Suzuki, T.; Nobori, S.; Ushigome, H.; Sakamoto, S.; Urasaki, K.; Mori, Y.; Akioka, K.; Daimon, S.; et al. Histopathologic Evaluation of Living Kidney Donor Candidates by Pre-Operative Kidney Biopsy. Clin. Transplant. 2009, 23, 58–61. [Google Scholar] [CrossRef]
- Choi, S.R.; Sun, I.O.; Hong, Y.A.; Kim, H.G.; Park, H.S.; Chung, B.H.; Choi, B.S.; Park, C.W.; Kim, Y.S.; Yang, C.W. The Role of Kidney Biopsy to Determine Donation from Prospective Kidney Donors with Asymptomatic Urinary Abnormalities. Transplant. Proc. 2012, 44, 11–13. [Google Scholar] [CrossRef]
- Koushik, R.; Garvey, C.; Manivel, J.C.; Matas, A.J.; Kasiske, B.L. Persistent, Asymptomatic, Microscopic Hematuria in Prospective Kidney Donors. Transplantation 2005, 80, 1425–1429. [Google Scholar] [CrossRef]
- Kido, R.; Shibagaki, Y.; Iwadoh, K.; Nakajima, I.; Fuchinoue, S.; Fujita, T.; Teraoka, S. Persistent Glomerular Hematuria in Living Kidney Donors Confers a Risk of Progressive Kidney Disease in Donors After Heminephrectomy. Am. J. Transplant. 2010, 10, 1597–1604. [Google Scholar] [CrossRef]
- Van der Weijden, J.; van Londen, M.; Pol, R.A.; Sanders, J.-S.F.; Navis, G.; Nolte, I.M.; de Borst, M.H.; Berger, S.P. Microscopic Hematuria at Kidney Donor Screening and Post-Donation Kidney Outcomes. J. Clin. Med. 2022, 11, 6281. [Google Scholar] [CrossRef]
- Bonani, M.; Seeger, H.; Weber, N.; Lorenzen, J.M.; Wüthrich, R.P.; Kistler, A.D. Safety of Kidney Biopsy When Performed as an Outpatient Procedure. Kidney Blood Press. Res. 2021, 46, 310–322. [Google Scholar] [CrossRef]
- Kincaid-Smith, P.; Fairley, K. The Investigation of Hematuria. Semin. Nephrol. 2005, 25, 127–135. [Google Scholar] [CrossRef]
- Vadivel, N.; Stankovic, A.; Rennke, H.G.; Singh, A.K. Accepting Prospective Kidney Donors with Asymptomatic Urinary Abnormalities: Are We Shooting in the Dark? Kidney Int. 2007, 71, 173–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, G. Natural History of Idiopathic IgA Nephropathy and Factors Predictive of Disease Outcome. Semin. Nephrol. 2004, 24, 179–196. [Google Scholar] [CrossRef]
- Gross, O.; Weber, M.; Fries, J.W.U.; Müller, G.-A. Living Donor Kidney Transplantation from Relatives with Mild Urinary Abnormalities in Alport Syndrome: Long-Term Risk, Benefit and Outcome. Nephrol. Dial. Transplant. 2009, 24, 1626–1630. [Google Scholar] [CrossRef] [Green Version]
- Choi, C.; Ahn, S.; Min, S.-K.; Ha, J.; Ahn, C.; Kim, Y.; Lee, H.; Min, S. Midterm Outcome of Kidney Transplantation From Donors With Thin Basement Membrane Nephropathy. Transplantation 2018, 102, e180–e184. [Google Scholar] [CrossRef] [PubMed]
- Thorner, P.S. Alport Syndrome and Thin Basement Membrane Nephropathy. Nephron Clin. Pract. 2007, 106, c82–c88. [Google Scholar] [CrossRef] [PubMed]
- Savige, J.; Rana, K.; Tonna, S.; Buzza, M.; Dagher, H.; Wang, Y.Y. Thin Basement Membrane Nephropathy. Kidney Int. 2003, 64, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Matthaiou, A.; Poulli, T.; Deltas, C. Prevalence of Clinical, Pathological and Molecular Features of Glomerular Basement Membrane Nephropathy Caused by COL4A3 or COL4A4 Mutations: A Systematic Review. Clin. Kidney J. 2020, 13, 1025–1036. [Google Scholar] [CrossRef] [Green Version]
- Savige, J.; Lipska-Zietkiewicz, B.S.; Watson, E.; Hertz, J.M.; Deltas, C.; Mari, F.; Hilbert, P.; Plevova, P.; Byers, P.; Cerkauskaite, A.; et al. Guidelines for Genetic Testing and Management of Alport Syndrome. Clin. J. Am. Soc. Nephrol. 2022, 17, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, Y.; Okumi, M.; Kanzawa, T.; Unagami, K.; Iizuka, J.; Takagi, T.; Ishida, H.; Tanabe, K. Impact of Donor-Related Arteriosclerosis in Pretransplant Biopsy on Long-Term Outcome of Living-Kidney Transplantation: A Propensity Score-Matched Cohort Study. Int. J. Urol. 2020, 27, 423–430. [Google Scholar] [CrossRef]
- Merzkani, M.A.; Mullan, A.; Denic, A.; D’Costa, M.; Iverson, R.; Kremers, W.; Alexander, M.P.; Textor, S.C.; Taler, S.J.; Stegall, M.D.; et al. Renal Function Outcomes and Kidney Biopsy Features of Living Kidney Donors with Hypertension. Clin. Transplant. 2021, 35, e14293. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, L.M.; Massie, A.B.; Muzaale, A.D.; Bagnasco, S.M.; Orandi, B.J.; Alejo, J.L.; Boyarsky, B.J.; Anjum, S.K.; Montgomery, R.A.; Dagher, N.N.; et al. Long-Term Renal Function in Living Kidney Donors Who Had Histological Abnormalities at Donation. Transplantation 2016, 100, 1294–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Potential Donors N = 59 | Individuals with Isolated Microscopic Hematuria N = 42 | Individuals with Borderline Proteinuria ± Hematuria Ν = 10 | Individuals with Comorbidities N = 7 | |
|---|---|---|---|---|
| Gender (male) | 10 (16.9) | 4 (9.5) | 5 (50) | 1 (14.3) |
| Age (years) | 58 (51–63) | 56.5 (50.3–61) | 62.5 (56.7–67) | 64 (52–67) |
| Older than 60 years old | 23 (39) | 12 (28.6) | 6 (60) | 5 (71.4) |
| Hypertension | 21 (35.6) | 8 (19) | 7 (70) | 6 (85.7) |
On antihypertensive medication
| 21 (35.6) 16 (27.1) 4 (6.8) 1 (1.7) | 8 (19) 7 (16.7) 1 (2.4) | 7 (70) 4 (40) 2 (20) 1 (10) | 6 (85.7) 5 (71.4) 1 (14.3) |
| BMI (kg/m2) | 27 (24.6–29.1) | 26 (24–27.5) | 27.3 (25.9–29.7) | 29.4 (28.3–31.5) |
| BMI > 30 (kg/m2) | 7 (11.9) | 2 (4.8) | 2 (20) | 3 (42.9) |
| Smoking | 17 (28.8) | 9 (21.4) | 4 (40) | 4 (57.1) |
| Abnormal OGTT | 3 (5.1) | 0 (0) | 2 (20) | 1 (14.3) |
| Creatinine (mg/mL) | 0.76 (±0.14) | 0.74 (±0.13) | 0.87 (±0.15) | 0.81 (±0.16) |
| eGFR (mL/min/1.73 m2) | 90.8 (±13.6) | 93 (±11.9) | 82.2 (±13.1) | 88.7 (±14.9) |
| eGFR < 80 mL/min/1.73 m2 | 11 (18.6) | 6 (14.3) | 4 (40) | 1 (14.3) |
| mGFR (mL/min/1.73 m2) | 90.3 (±17.5) | 92.2 (±18.8) | 81.4 (±14.9) | 86.7 (±15.2) |
| mGFR < 80 mL/min/1.73 m2 | 11 (18.6) | 6 (14.3) | 4 (40) | 1 (14.3) |
| Diagnosis: | ||||
| 32 (54.2) | 22 (52.4) | 4 (40) | 6 (85.7) |
| 8 (13.6) | 6 (14.3) | 2 (20) | 0 (0) |
| 10 (16.9) | 10 (23.8) | 0 (0) | 0 (0) |
| 9 (15.3) | 4 (9.5) | 4 (40) | 1 (14.3) |
| Total Potential Donors N = 59 | Individuals Accepted for Donation N = 32 | Individuals Diagnosed with IgA Nephropathy Ν = 8 | Individuals Diagnosed with TBMN N = 10 | Individuals Diagnosed with Secondary FSGS-Increased Chronicity N = 9 | |
|---|---|---|---|---|---|
| Gender (male) | 10 (16.9) | 4 (12.5) | 2 (25) | 0 (0) | 4 (44.4) |
| Age (years) | 58 (51–63) | 60.5 (50–65.3) | 53.5 (51–55) | 59.5 (47.3–60.8) | 58 (57–63) |
| Older than 60 years old | 23 (39) | 15 (46.7) | 1 (12.5) | 4 (40) | 3 (33.3) |
| Hypertension | 21 (35.6) | 12 (37.5) | 3 (37.5) | 1 (10) | 3 (37.5) |
On antihypertensive medication
| 21 (35.6) 16 (27.1) 4 (6.8) 1 (1.7) | 12 (37.5) 9 (28.1) 3 (9.4) | 3 (37.5) 3 (37.5) | 1 (10) 1 (10) | 5 (55.5) 3 (33.3) 1 (11.1) 1 (11.1) |
| BMI (kg/m2) | 27 (24.6–29.1) | 27 (24.8–29) | 26 (25.5–27.1) | 24.4 (23.8–25.3) | 29.5 (27.3–30.9) |
| BMI > 30 (kg/m2) | 7 (11.9) | 4 (12.5) | 0 (0) | 1 (10) | 2 (22.2) |
| Smoking | 17 (28.8) | 9 (28.1) | 2 (25) | 2 (20) | 4 (44.4) |
| Abnormal OGTT | 3 (5.1) | 2 (6.3) | 0 (0) | 0 (0) | 1 (11.1) |
| Creatinine (mg/dL) | 0.76 (±0.14) | 0.73 (±0.14) | 0.79 (±0.08) | 0.7 (±0.08) | 0.92 (±0.13) |
| eGFR (mL/min/1.73 m2) | 90.8 (±13.6) | 91.3 (±13.8) | 94.2 (±9.6) | 97.3 (±11.9) | 80.2 (±11.4) |
| eGFR <80 mL/min/1.73 m2 | 11 (18.6) | 5 (15.6) | 1 (12.5) | 1 (10) | 4 (44.4) |
| mGFR (mL/min/1.73 m2) | 90.3 (±17.5) | 91.3 (±18.2) | 91.5 (±15.3) | 93 (±11.2) | 75.3 (±13.2) |
| mGFR < 80 mL/min/1.73 m2 | 11 (18.6) | 5 (15.6) | 1 (12.5) | 1 (10) | 4 (44.4) |
| Glomerular hematuria | 42 (71.1) | 22 (68.8) | 6 (60) | 10 (100) | 4 (44.4) |
| Borderline proteinuria (150–300 mg/d) | 3 (5.1) | 2 (6.3) | 0 (0) | 0 (0) | 1 (11.1) |
| Hematuria and borderline proteinuria | 7 (11.9) | 2 (6.3) | 2 (25) | 0 (0) | 3 (33.3) |
| Donors Accepted without a Pre-Transplant Biopsy N = 128 | Donors Who Underwent a Pre-Transplant Biopsy N = 32 | p-Value | |
|---|---|---|---|
| Gender (male) | 16 (12.5) | 4 (12.5) | 0.863 |
| Age (years) | 61 (50.5–66) | 60.5 (50–65.3) | 0.628 |
| Hypertension | 24 (18.7) | 12 (37.5) | 0.003 |
| BMI (kg/m2) | 26.1 (24–28.1) | 27 (24.8–29) | 0.139 |
| Smoking | 24 (18.8) | 9 (28.1) | 0.202 |
| Abnormal OGTT | 7 (5.5) | 2 (6.3) | 0.511 |
| Creatinine (mg/dL) | 0.7 (±0.16) | 0.73 (±0.13) | 0.537 |
| eGFR (mL/min/1.73 m2) | 96.2 (±17.1) | 91.3 (±13.8) | 0.103 |
| Glomerular hematuria | 0 (0) | 24 (75) | <0.001 |
| Borderline proteinuria (150–300 mg/d) | 0 (0) | 4 (12.5) | <0.001 |
| Follow up (months) | 80 (34–116) | 79 (36–114) | 0.725 |
| Creatinine at follow-up (mg/dL) | 1.08 (±0.18) | 1.08 (±0.14) | 0.736 |
| eGFR at follow-up (mL/min/1.72 m2) | 61.9 (±13.8) | 61.3 (±10.4) | 0.866 |
| Proteinuria at follow-up (mg/d) | 88.5 (75–99) | 77 (62–164) | 0.549 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marinaki, S.; Vallianou, K.; Darema, M.; Mantios, E.; Kapsia, E.; Melexopoulou, C.; Filiopoulos, V.; Liapis, G.; Boletis, I.N. Τhe Impact of Pre-Transplant Kidney Biopsy on the Evaluation of Prospective Living Kidney Donors. J. Clin. Med. 2023, 12, 2685. https://doi.org/10.3390/jcm12072685
Marinaki S, Vallianou K, Darema M, Mantios E, Kapsia E, Melexopoulou C, Filiopoulos V, Liapis G, Boletis IN. Τhe Impact of Pre-Transplant Kidney Biopsy on the Evaluation of Prospective Living Kidney Donors. Journal of Clinical Medicine. 2023; 12(7):2685. https://doi.org/10.3390/jcm12072685
Chicago/Turabian StyleMarinaki, Smaragdi, Kalliopi Vallianou, Maria Darema, Evangelos Mantios, Eleni Kapsia, Christina Melexopoulou, Vassilis Filiopoulos, George Liapis, and Ioannis N. Boletis. 2023. "Τhe Impact of Pre-Transplant Kidney Biopsy on the Evaluation of Prospective Living Kidney Donors" Journal of Clinical Medicine 12, no. 7: 2685. https://doi.org/10.3390/jcm12072685