
The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
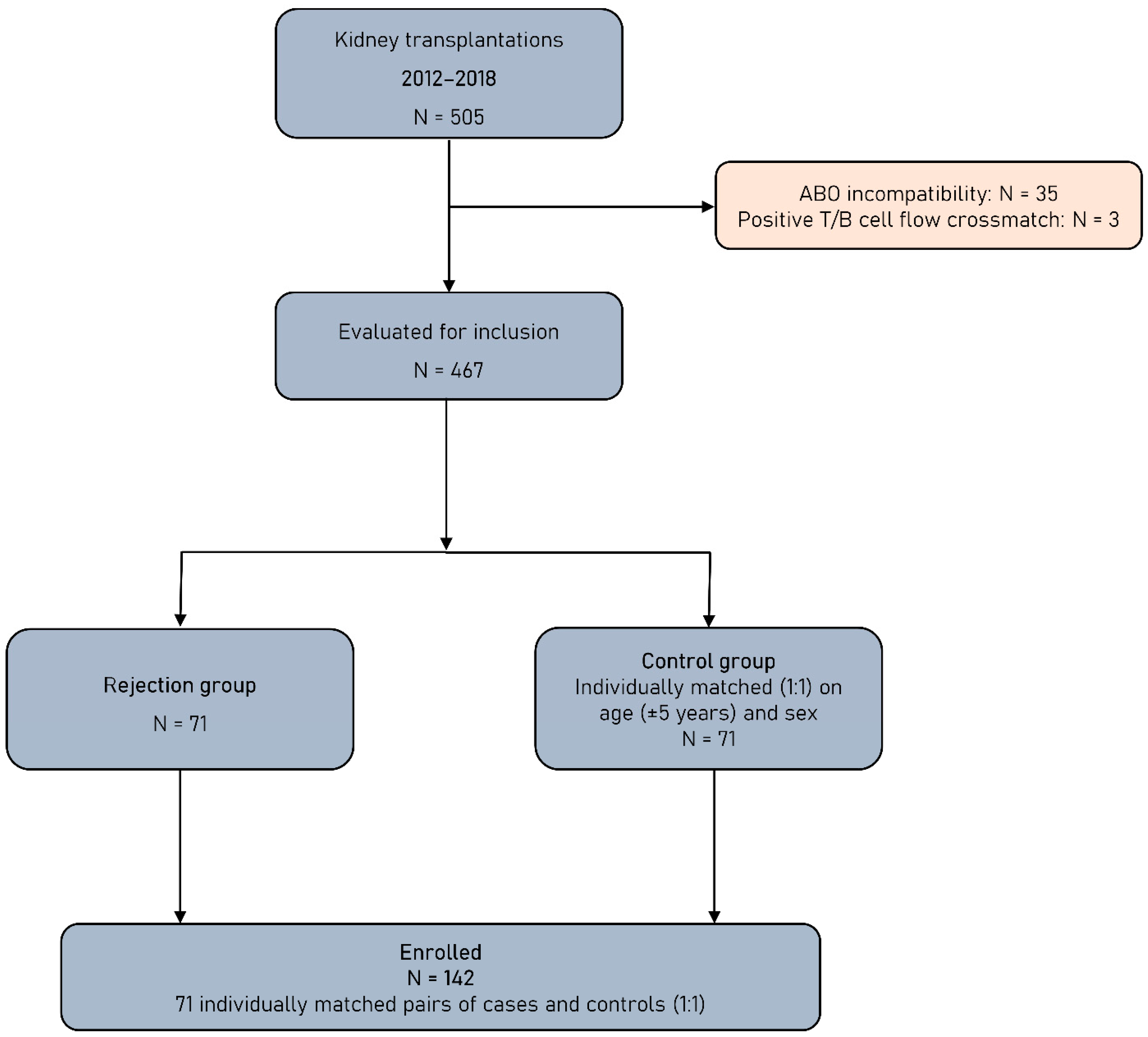
2.1. Study Population
2.2. Immunosuppression
2.3. Serum Collection and Laboratory Evaluations
2.4. Statistical Analysis
3. Results
3.1. Patients and Transplant Characteristics
3.2. Pretransplant Anti-AT1RAbs and HLA-DSAs
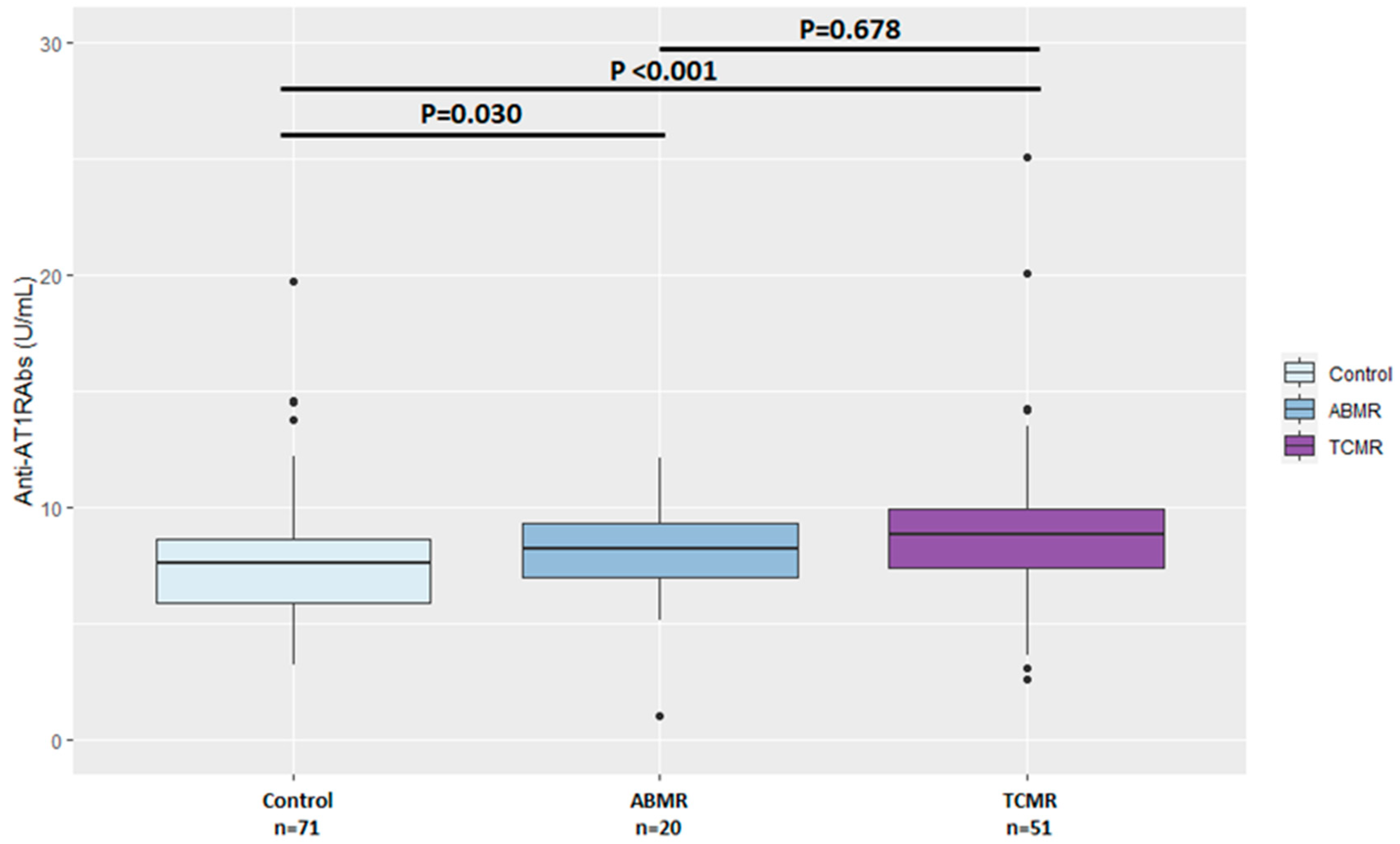
3.3. Anti-AT1RAbs and HLA-DSAs at the Time of Transplant Biopsy
3.4. Anti-AT1RAbs and HLA-DSAs at Follow-Up
3.5. Graft and Patient Outcomes
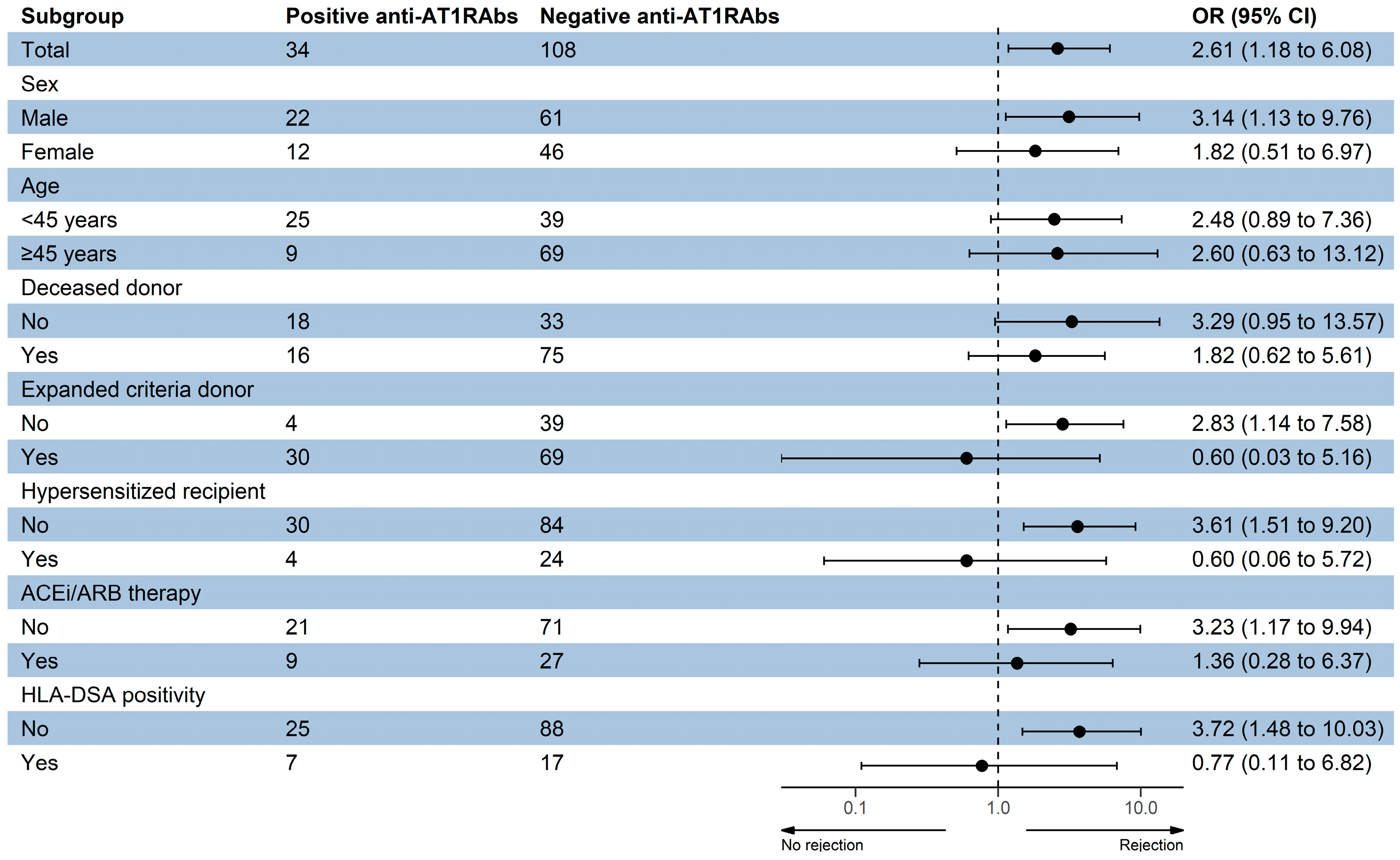
3.6. Anti-AT1RAbs Positivity and Transplant Outcomes
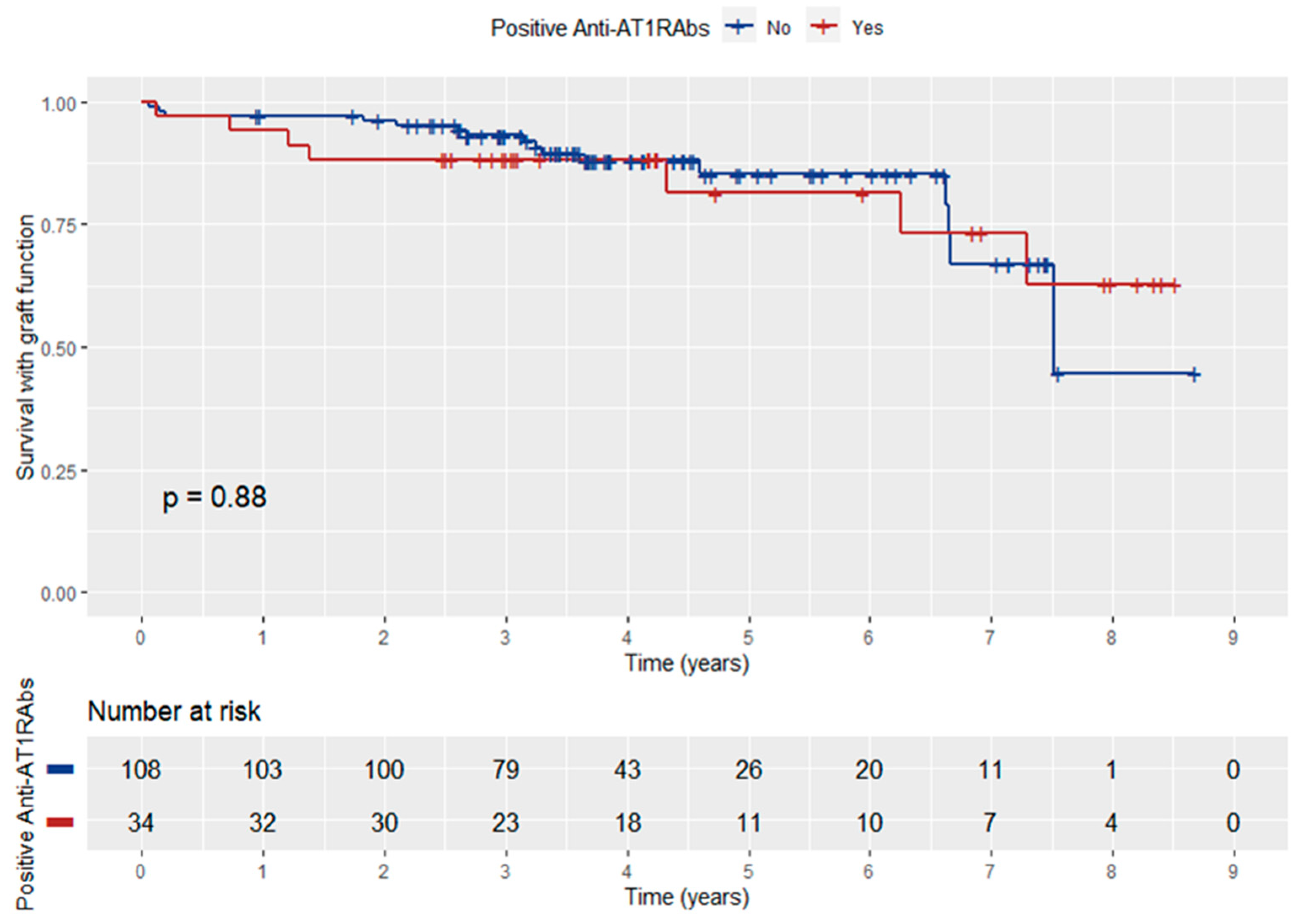
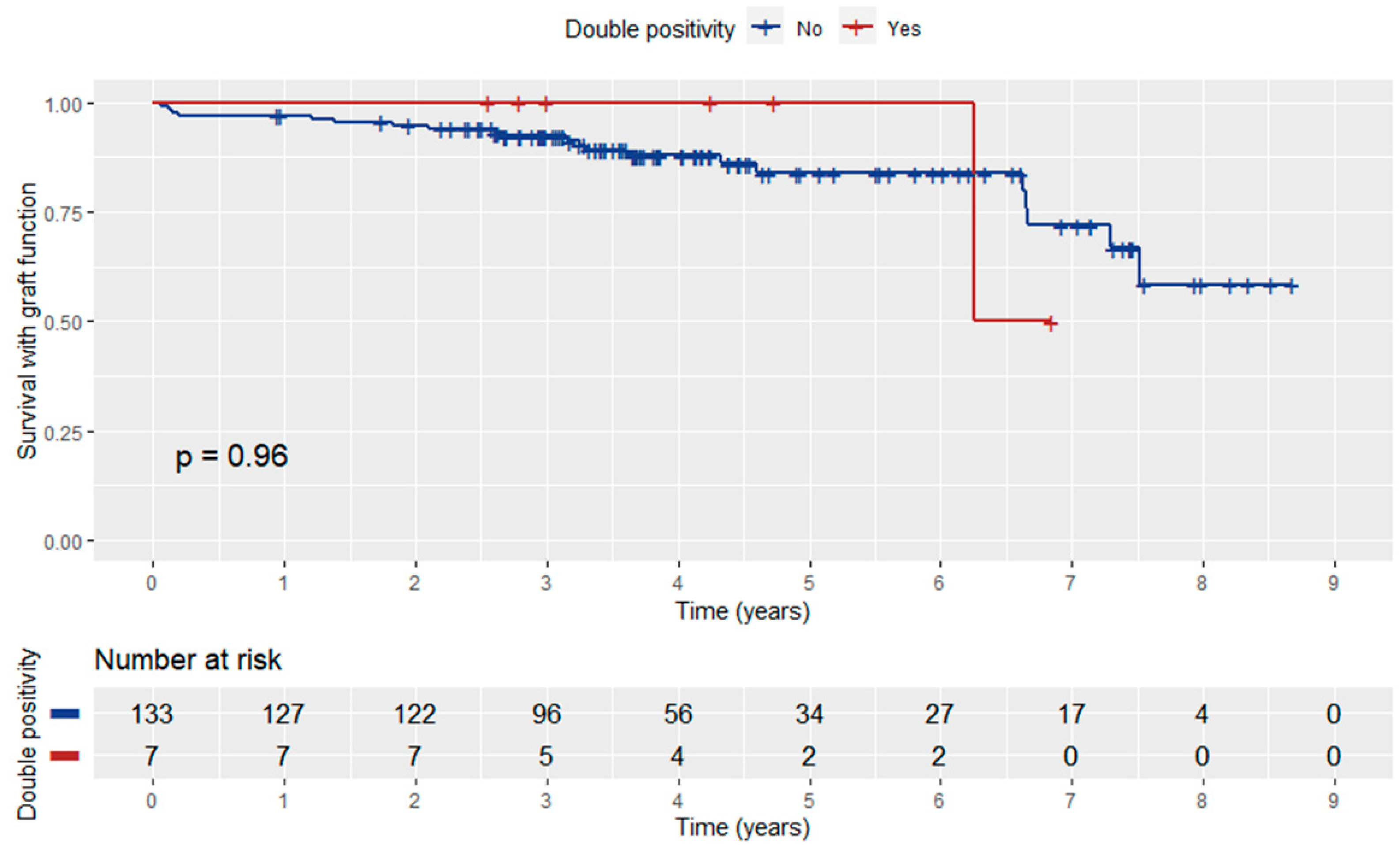
3.7. Graft Function according to Anti-AT1RAbs Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Terasaki, P.I. Deduction of the Fraction of Immunologic and Non-Immunologic Failure in Cadaver Donor Transplants. Clin. Transpl. 2003, 449–452. [Google Scholar]
- Sigdel, T.K.; Sarwal, M.M. Moving beyond HLA: A Review of NHLA Antibodies in Organ Transplantation. Hum. Immunol. 2013, 74, 1486–1490. [Google Scholar] [CrossRef] [PubMed]
- Angaswamy, N.; Tiriveedhi, V.; Sarma, N.J.; Subramanian, V.; Klein, C.; Wellen, J.; Shenoy, S.; Chapman, W.C.; Mohanakumar, T. Interplay between Immune Responses to HLA and Non-HLA Self-Antigens in Allograft Rejection. Hum. Immunol. 2013, 74, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Reed, E.F. The Importance of Non-HLA Antibodies in Transplantation. Nat. Rev. Nephrol. 2016, 12, 484–495. [Google Scholar] [CrossRef]
- Philogene, M.C.; Johnson, T.; Vaught, A.J.; Zakaria, S.; Fedarko, N. Antibodies against Angiotensin II Type 1 and Endothelin A Receptors: Relevance and Pathogenicity. Hum. Immunol. 2019, 80, 561–567. [Google Scholar] [CrossRef]
- Reinsmoen, N.L. Role of Angiotensin II Type 1 Receptor-Activating Antibodies in Solid Organ Transplantation. Hum. Immunol. 2013, 74, 1474–1477. [Google Scholar] [CrossRef] [PubMed]
- Sorohan, B.M.; Ismail, G.; Leca, N.; Tacu, D.; Obrișcă, B.; Constantinescu, I.; Baston, C.; Sinescu, I. Angiotensin II Type 1 Receptor Antibodies in Kidney Transplantation: An Evidence-Based Comprehensive Review. Transplant. Rev. 2020, 34, 100573. [Google Scholar] [CrossRef]
- Giral, M.; Foucher, Y.; Dufay, A.; Van Huyen, J.P.D.; Renaudin, K.; Moreau, A.; Philippe, A.; Hegner, B.; Dechend, R.; Heidecke, H.; et al. Pretransplant Sensitization against Angiotensin II Type 1 Receptor Is a Risk Factor for Acute Rejection and Graft Loss. Am. J. Transplant. 2013, 13, 2567–2576. [Google Scholar] [CrossRef]
- Taniguchi, M.; Rebellato, L.M.; Cai, J.; Hopfield, J.; Briley, K.P.; Haisch, C.E.; Catrou, P.G.; Bolin, P.; Parker, K.; Kendrick, W.T.; et al. Higher Risk of Kidney Graft Failure in the Presence of Anti-Angiotensin II Type-1 Receptor Antibodies. Am. J. Transplant. 2013, 13, 2577–2589. [Google Scholar] [CrossRef]
- Dragun, D.; Müller, D.N.; Bräsen, J.H.; Fritsche, L.; Nieminen-Kelhä, M.; Dechend, R.; Kintscher, U.; Rudolph, B.; Hoebeke, J.; Eckert, D.; et al. Angiotensin II Type 1–Receptor Activating Antibodies in Renal-Allograft Rejection. N. Engl. J. Med. 2005, 352, 558–569. [Google Scholar] [CrossRef]
- Alachkar, N.; Gupta, G.; Montgomery, R.A. Angiotensin Antibodies and Focal Segmental Glomerulosclerosis. N. Engl. J. Med. 2013, 368, 971–973. [Google Scholar] [CrossRef]
- Deltombe, C.; Gillaizeau, F.; Anglicheau, D.; Morelon, E.; Trébern-Launay, K.; Le Borgne, F.; Rimbert, M.; Guérif, P.; Malard-Castagnet, S.; Foucher, Y.; et al. Is Pre-Transplant Sensitization against Angiotensin II Type 1 Receptor Still a Risk Factor of Graft and Patient Outcome in Kidney Transplantation in the Anti-HLA Luminex Era? A Retrospective Study. Transpl. Int. 2017, 30, 1150–1160. [Google Scholar] [CrossRef]
- Haas, M.; Sis, B.; Racusen, L.C.; Solez, K.; Glotz, D.; Colvin, R.B.; Castro, M.C.R.; David, D.S.R.; David-Neto, E.; Bagnasco, S.M.; et al. Banff 2013 Meeting Report: Inclusion of C4d-Negative Antibody-Mediated Rejection and Antibody-Associated Arterial Lesions. Am. J. Transplant. 2014, 14, 272–283. [Google Scholar] [CrossRef]
- Sis, B.; Mengel, M.; Haas, M.; Colvin, R.B.; Halloran, P.F.; Racusen, L.C.; Solez, K.; Baldwin III, W.M.; Bracamonte, E.R.; Broecker, V.; et al. Banff ’09 Meeting Report: Antibody Mediated Graft Deterioration and Implementation of Banff Working Groups. Am. J. Transplant. 2010, 10, 464–471. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef]
- Metzger, R.A.; Delmonico, F.L.; Feng, S.; Port, F.K.; Wynn, J.J.; Merion, R.M. Expanded criteria donors for kidney transplantation. Am. J. Transplant. 2003, 3, 114–125. [Google Scholar] [CrossRef]
- Vittoraki, A.; Ioannou, S.; Vallindra, H.; Siorenta, A.; Milonas, A.; Seimenis, N.; Apostolaki, M.; Iniotaki, A. Treating sera with ethylenediaminetetraacetic acid: A promising technical solution for the complement-mediated prozone effect in anti-HLA antibody detection by single antigen bead assay. Hum. Immunol. 2015, 76, 65. [Google Scholar] [CrossRef]
- Therneau, T. A Package for Survival Analysis in R; R Package Version 3.5-5; Springer: New York, NY, USA, 2023; Available online: https://CRAN.R-project.org/package=survival (accessed on 16 February 2023).
- Kassambara, A.; Kosinski, M.; Biecek, P. Drawing Survival Curves Using “ggplot2”; R Package Survminer Version 0.4.8; 2020; Available online: https://CRAN.R-project.org/package=survminer (accessed on 16 February 2023).
- Abeysekera, W. Sooriyarachchi Use of Schoenfeld’s Global Test to Test the Proportional Hazards Assumption in the Cox Proportional Hazards Model: An Application to a Clinical Study. J. Natl. Sci. Found. Sri Lanka 2009, 37, 41–51. [Google Scholar] [CrossRef]
- Reinsmoen, N.L.; Lai, C.-H.; Heidecke, H.; Haas, M.; Cao, K.; Ong, G.; Naim, M.; Wang, Q.; Mirocha, J.; Kahwaji, J.; et al. Anti-Angiotensin Type 1 Receptor Antibodies Associated with Antibody Mediated Rejection in Donor HLA Antibody Negative Patients. Transplantation 2010, 90, 1473–1477. [Google Scholar] [CrossRef] [PubMed]
- Malheiro, J.; Tafulo, S.; Dias, L.; Martins, L.S.; Fonseca, I.; Beirão, I.; Castro-Henriques, A.; Cabrita, A. Deleterious Effect of Anti-Angiotensin II Type 1 Receptor Antibodies Detected Pretransplant on Kidney Graft Outcomes Is Both Proper and Synergistic with Donor-Specific Anti-HLA Antibodies. Nephrology 2019, 24, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Huh, H.J.; Lee, K.W.; Park, J.B.; Kim, S.-J.; Huh, W.; Jang, H.R.; Kwon, G.Y.; Moon, H.H.; Kang, E.-S. Pre-Transplant Angiotensin II Type 1 Receptor Antibodies and Anti-Endothelial Cell Antibodies Predict Graft Function and Allograft Rejection in a Low-Risk Kidney Transplantation Setting. Ann. Lab. Med. 2020, 40, 398–408. [Google Scholar] [CrossRef]
- Gareau, A.J.; Wiebe, C.; Pochinco, D.; Gibson, I.W.; Ho, J.; Rush, D.N.; Nickerson, P.W. Pre-Transplant AT1R Antibodies Correlate with Early Allograft Rejection. Transpl. Immunol. 2018, 46, 29–35. [Google Scholar] [CrossRef]
- Banasik, M.; Boratyńska, M.; Kościelska-Kasprzak, K.; Kamińska, D.; Bartoszek, D.; Żabińska, M.; Myszka, M.; Zmonarski, S.; Protasiewicz, M.; Nowakowska, B.; et al. The Influence of Non-HLA Antibodies Directed against Angiotensin II Type 1 Receptor (AT1R) on Early Renal Transplant Outcomes. Transpl. Int. 2014, 27, 1029–1038. [Google Scholar] [CrossRef]
- Amico, P.; Hönger, G.; Bielmann, D.; Lutz, D.; Garzoni, D.; Steiger, J.; Mihatsch, M.J.; Dragun, D.; Schaub, S. Incidence and Prediction of Early Antibody-Mediated Rejection Due to Non-Human Leukocyte Antigen-Antibodies. Transplantation 2008, 85, 1557–1563. [Google Scholar] [CrossRef]
- Min, J.W.; Lee, H.; Choi, B.S.; Park, C.W.; Yang, C.W.; Kim, Y.-S.; Choi, Y.J.; Oh, E.-J.; Chung, B.H. Clinical Impact of Pre-Transplant Antibodies Against Angiotensin II Type I Receptor and Major Histocompatibility Complex Class I-Related Chain A in Kidney Transplant Patients. Ann. Lab. Med. 2018, 38, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Pearl, M.H.; Zhang, Q.; Palma Diaz, M.F.; Grotts, J.; Rossetti, M.; Elashoff, D.; Gjertson, D.W.; Weng, P.; Reed, E.F.; Tsai Chambers, E. Angiotensin II Type 1 Receptor Antibodies Are Associated with Inflammatory Cytokines and Poor Clinical Outcomes in Pediatric Kidney Transplantation. Kidney Int. 2018, 93, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Philogene, M.C.; Zhou, S.; Lonze, B.E.; Bagnasco, S.; Alasfar, S.; Montgomery, R.A.; Kraus, E.; Jackson, A.M.; Leffell, M.S.; Zachary, A.A. Pre-Transplant Screening for Non-HLA Antibodies: Who Should Be Tested? Hum. Immunol. 2018, 79, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Méndez, E.A.; Arreola-Guerra, J.M.; Morales-Buenrostro, L.E.; Ramírez, J.B.; Calleja, S.; Castelán, N.; Salcedo, I.; Vilatobá, M.; Contreras, A.G.; Gabilondo, B.; et al. Pre-transplant angiotensin II type 1 receptor antibodies: A risk factor for decreased kidney graft function in the early post-transplant period? Clin. Transpl. 2013, 343–350. [Google Scholar]
- Cuevas, E.; Arreola-Guerra, J.M.; Hernández-Méndez, E.A.; Salcedo, I.; Castelán, N.; Uribe-Uribe, N.O.; Vilatobá, M.; Contreras-Saldívar, A.G.; Sánchez-Cedillo, A.I.; Ramírez, J.B.; et al. Pretransplant Angiotensin II Type 1-Receptor Antibodies Are a Risk Factor for Earlier Detection of de Novo HLA Donor-Specific Antibodies. Nephrol. Dial. Transplant. 2016, 31, 1738–1745. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Viglietti, D.; Bouatou, Y.; Philippe, A.; Pievani, D.; Aubert, O.; Duong Van Huyen, J.-P.; Taupin, J.-L.; Glotz, D.; Legendre, C.; et al. Non-HLA Agonistic Anti-Angiotensin II Type 1 Receptor Antibodies Induce a Distinctive Phenotype of Antibody-Mediated Rejection in Kidney Transplant Recipients. Kidney Int. 2019, 96, 189–201. [Google Scholar] [CrossRef]
- Carroll, R.P.; Riceman, M.; Hope, C.M.; Zeng, A.; Deayton, S.; Bennett, G.D.; Coates, P.T. Angiotensin II Type-1 Receptor Antibody (AT1Rab) Associated Humoral Rejection and the Effect of Peri Operative Plasma Exchange and Candesartan. Hum. Immunol. 2016, 77, 1154–1158. [Google Scholar] [CrossRef]
- Philogene, M.C.; Bagnasco, S.; Kraus, E.S.; Montgomery, R.A.; Dragun, D.; Leffell, M.S.; Zachary, A.A.; Jackson, A.M. Anti-Angiotensin II Type 1 Receptor and Anti-Endothelial Cell Antibodies: A Cross-Sectional Analysis of Pathological Findings in Allograft Biopsies. Transplantation 2017, 101, 608–615. [Google Scholar] [CrossRef]
- Lee, J.; Huh, K.H.; Park, Y.; Park, B.G.; Yang, J.; Jeong, J.C.; Lee, J.; Park, J.B.; Cho, J.-H.; Lee, S.; et al. The Clinicopathological Relevance of Pretransplant Anti-Angiotensin II Type 1 Receptor Antibodies in Renal Transplantation. Nephrol. Dial. Transplant. 2017, 32, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Gimferrer, I.; Warner, P.; Nelson, K.; Sibulesky, L.; Bakthavatsalam, R.; Leca, N. Preformed Angiotensin II Type-1 Receptor Antibodies Are Associated With Rejection After Kidney Transplantation: A Single-Center, Cohort Study. Transplant. Proc. 2018, 50, 3467–3472. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.-Y.; Liu, C.; Liu, W.; Li, D.-H. Effect of Anti-Angiotensin II Type 1 Receptor Antibodies on the Outcomes of Kidney Transplantation: A Systematic Review and Meta-Analysis. Nephrol. Dial. Transplant. 2022, 37, 1171–1180. [Google Scholar] [CrossRef]
- Arnold, M.-L.; Ntokou, I.-S.; Doxiadis, I.I.N.; Spriewald, B.M.; Boletis, J.N.; Iniotaki, A.G. Donor-Specific HLA Antibodies: Evaluating the Risk for Graft Loss in Renal Transplant Recipients with Isotype Switch from Complement Fixing IgG1/IgG3 to Noncomplement Fixing IgG2/IgG4 Anti-HLA Alloantibodies. Transpl. Int. 2014, 27, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Lukitsch, I.; Kehr, J.; Chaykovska, L.; Wallukat, G.; Nieminen-Kelhä, M.; Batuman, V.; Dragun, D.; Gollasch, M. Renal Ischemia and Transplantation Predispose to Vascular Constriction Mediated by Angiotensin II Type 1 Receptor-Activating Antibodies. Transplantation 2012, 94, 8–13. [Google Scholar] [CrossRef]
- Delville, M.; Lamarthée, B.; Pagie, S.; See, S.B.; Rabant, M.; Burger, C.; Gatault, P.; Giral, M.; Thaunat, O.; Arzouk, N.; et al. Early Acute Microvascular Kidney Transplant Rejection in the Absence of Anti-HLA Antibodies Is Associated with Preformed IgG Antibodies against Diverse Glomerular Endothelial Cell Antigens. J. Am. Soc. Nephrol. 2019, 30, 692–709. [Google Scholar] [CrossRef]
- Zorn, E.; See, S.B. Is There a Role for Natural Antibodies in Rejection Following Transplantation? Transplantation 2019, 103, 1612–1619. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients (n = 142) | Rejection Group (n = 71) | Control Group (n = 71) | p-Value |
|---|---|---|---|---|
| Age at transplantation | 45.8 ± 13.0 | 42.8 ± 12.9 | 48.8 ± 12.5 | 0.005 |
| Male sex | 83 (58.5%) | 44 (62.0%) | 39 (54.9%) | 0.496 |
| Donor age | 54.8 ± 13.9 | 54.6 ± 12.6 | 54.9 ± 15.3 | 0.890 |
| Donor male sex | 56 (39.4%) | 26 (36.6%) | 30 (42.2%) | 0.607 |
| Deceased donor | 91 (64.1%) | 40 (56.3%) | 51 (71.8%) | 0.080 |
| Expanded criteria donor | 43 (30.3%) | 15 (21.1%) | 28 (39.4%) | 0.131 |
| Cold ischemia time (h) | 17 [15–20.6] | 17.5 [16–19.5] | 17 [14.8–20.8] | 0.316 |
| Time on dialysis (years) | 6.3 [2.1–9.5] | 4.2 [1.8–8.2] | 6.9 [2.6–10.0] | 0.103 |
| Primary renal disease | ||||
| Diabetes mellitus | 4 (2.8%) | 3 (4.2%) | 1 (1.4%) | 0.085 |
| Hypertension | 8 (5.6%) | 1 (1.4%) | 7 (9.8%) | |
| Glomerulonephritis | 33 (23.2%) | 18 (25.3%) | 15 (21.1%) | |
| Polycystic kidney disease | 21 (14.7%) | 8 (11.2) | 13 (18.3%) | |
| Obstructive uropathy/Reflux nephropathy/Interstitial nephritis | 18 (12.6%) | 13 (18.3%) | 5 (7.0%) | |
| Unknown | 50 (35.2%) | 25 (35.2%) | 25 (35.2%) | |
| Other | 8 (5.6%) | 3 (4.2%) | 5 (7.0%) | |
| Re-transplantation | 17 (12.0%) | 12 (16.9%) | 5 (7.0%) | 0.119 |
| Hypersensitized recipient | 29 (20.4%) | 18 (25.3%) | 11 (15.4%) | 0.271 |
| HLA mismatches | 3 [2–4] | 3 [3, 4] | 3 [2–4] | 0.679 |
| Delayed graft function | 79 (55.6%) | 41 (57.7%) | 38 (53.5%) | 0.734 |
| Induction immunosuppression | ||||
| Basiliximab | 133 (93.7%) | 68 (95.8%) | 65 (91.5%) | 0.493 |
| Anti-thymocyte globulin | 9 (6.3%) | 3 (4.2%) | 6 (8.5%) | |
| Maintenance immunosuppression | ||||
| MPA/Tacrolimus | 138 (97.2%) | 68 (95.8%) | 70 (98.6%) | 0.620 |
| MPA/Ciclosporin | 3 (2.1%) | 2 (2.8%) | 1 (1.4% | |
| Tacrolimus/Everolimus | 1 (0.7%) | 1 (1.4%) | 0 (0.0%) | |
| ACEi/ARB pre-KTx | 36/128 (28.1%) | 14/60 (23.3%) | 22/68 (32.4%) | 0.350 |
| ACEi/ARB post-KTx | 52 (36.6%) | 26 (36.6%) | 26 (36.6%) | 1 |
| Follow-up period (years) | 3.7 [2.9–5.2] | 3.4 [2.6–4.8] | 3.7 [3.3–5.5] | 0.059 |
| Time from transplantation to rejection (days) | - | 28 [12–375] | - | N/A |
| Time of follow-up after rejection (years) | - | 2.9 [2–3.9] | - | N/A |
| Parameter | All Patients (n = 142) | Rejection Group (n = 71) | Control Group (n = 71) | p-Value |
|---|---|---|---|---|
| Rejection classification (Banff 2009–2013) | ||||
| ABMR | 20 (14.1%) | 20 (28.2%) | - | |
| Acute/active | 13 (18.3%) | - | ||
| Chronic active | 7 (9.8%) | - | ||
| Borderline changes | 8 (5.6%) | 8 (11.2%) | - | |
| TCMR | 43 (30.3%) | 43 (60.6%) | - | |
| Acute | 38 (53.6%) | - | ||
| Grade IA | 16 | |||
| Grade IB | 10 | |||
| Grade IIA | 6 | |||
| Grade IIB | 6 | |||
| Chronic active | 5 (7.0%) | - | ||
| Anti-AT1RAbs pre-KTx (U/mL) | 8.2 [6.5–9.8] | 9.0 [7.4–11.3] | 7.6 [5.9–8.7] | <0.001 |
| Anti-AT1Rabs pre-KTx ≥ 10 U/mL | 34 (23.9%) | 23 (32.4%) | 11 (15.5%) | 0.031 |
| HLA-DSA pre-KTx (MFI > 1000) | 25 (17.6%) | 19 (26.7%) | 6 (8.4%) | 0.010 |
| First-year serum creatinine (mg/dL) | 1.6 [1.3–2.2] | 1.8 [1.4–2.9] | 1.6 [1.2–2.1] | 0.036 |
| End-of-follow-up serum creatinine (mg/dL) | 1.5 [1.2–2.0] | 1.8 [1.4–2.6] | 1.3 [1.1–1.6] | <0.001 |
| First-year eGFR (CKD-EPI) (mL/min/1.73 m2) | 42 [31–58] | 39 [24.3–58] | 43 [33.5–57] | 0.229 |
| End-of-follow-up eGFR (CKD-EPI) (mL/min/1.73 m2) | 47.5 [34.3–60] | 38 [23–56] | 52 [44.5–65] | <0.001 |
| Graft loss | 14 (9.9%) | 13 (18.3%) | 1 (1.4%) | 0.001 |
| Death | 9 (6.3%) | 7 (9.9%) | 2 (2.8%) | 0.166 |
| Antibodies | Pre-KTx | At Biopsy | ABMR C4d (+) | ABMR C4d (−) | TCMR |
|---|---|---|---|---|---|
| Anti-AT1RAbs (+) HLA-DSA (−) | 18 (25.4%) | 8 (11.2%) | 1 | 0 | 7 |
| Anti-AT1RAbs (−) HLA-DSA (+) | 14 (19.7%) | 22 (31%) | 5 | 7 | 10 |
| Anti-AT1RAbs (+) HLA-DSA (+) | 5 (7.0%) | 7 (9.9%) | 0 | 3 | 4 |
| Anti-AT1RAbs (−) HLA-DSA (−) | 34 (47.9) | 34 (47.9%) | 1 | 3 | 30 |
| Model | Odds Ratio | 95% Confidence Intervals | p-Value |
|---|---|---|---|
| Crude | 2.61 | 1.18–6.08 | 0.021 |
| Model 1 | 1.88 | 0.80–4.57 | 0.153 |
| Model 2 | 1.72 | 0.72–4.21 | 0.227 |
| Model 3 | 1.72 | 0.67–4.51 | 0.258 |
| Model 4 | 1.97 | 0.75–5.38 | 0.174 |
| Model | Hazard Ratio | 95% Confidence Intervals | p-Value |
|---|---|---|---|
| Crude | 1.07 | 0.43–2.69 | 0.878 |
| Model 1 | 0.79 | 0.31–2.02 | 0.619 |
| Model 2 | 0.82 | 0.32–2.14 | 0.690 |
| Model 3 | 0.43 | 0.12–1.36 | 0.215 |
| Model 4 | 0.49 | 0.13–1.89 | 0.302 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filiopoulos, V.; Vittoraki, A.; Vallianou, K.; Bellos, I.; Markaki, P.; Liapis, G.; Marinaki, S.; Iniotaki, A.; Boletis, I.N. The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study. J. Clin. Med. 2023, 12, 3112. https://doi.org/10.3390/jcm12093112
Filiopoulos V, Vittoraki A, Vallianou K, Bellos I, Markaki P, Liapis G, Marinaki S, Iniotaki A, Boletis IN. The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study. Journal of Clinical Medicine. 2023; 12(9):3112. https://doi.org/10.3390/jcm12093112
Chicago/Turabian StyleFiliopoulos, Vassilis, Angeliki Vittoraki, Kalliopi Vallianou, Ioannis Bellos, Pavlina Markaki, George Liapis, Smaragdi Marinaki, Aliki Iniotaki, and Ioannis N. Boletis. 2023. "The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study" Journal of Clinical Medicine 12, no. 9: 3112. https://doi.org/10.3390/jcm12093112