
Resistance Training Increases White Matter Density in Frail Elderly Women
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Study Design
2.3. MRI
2.4. Voxel Based Morphometry (VBM)
2.5. Cortical Thickness Analysis
2.6. DTI and Tract-Based Spatial Statistics (TBSS)
2.7. Positron Emission Tomography (PET)—Brain and Skeletal Muscle Glucose Uptake during Clamp
2.8. Cognitive Assessments
2.9. Biochemical Analysis
2.10. Statistical Analysis
2.11. Correlations
3. Results
3.1. Comparison between Frail (F) and Non-Frail Control (CTR) Elderly Women
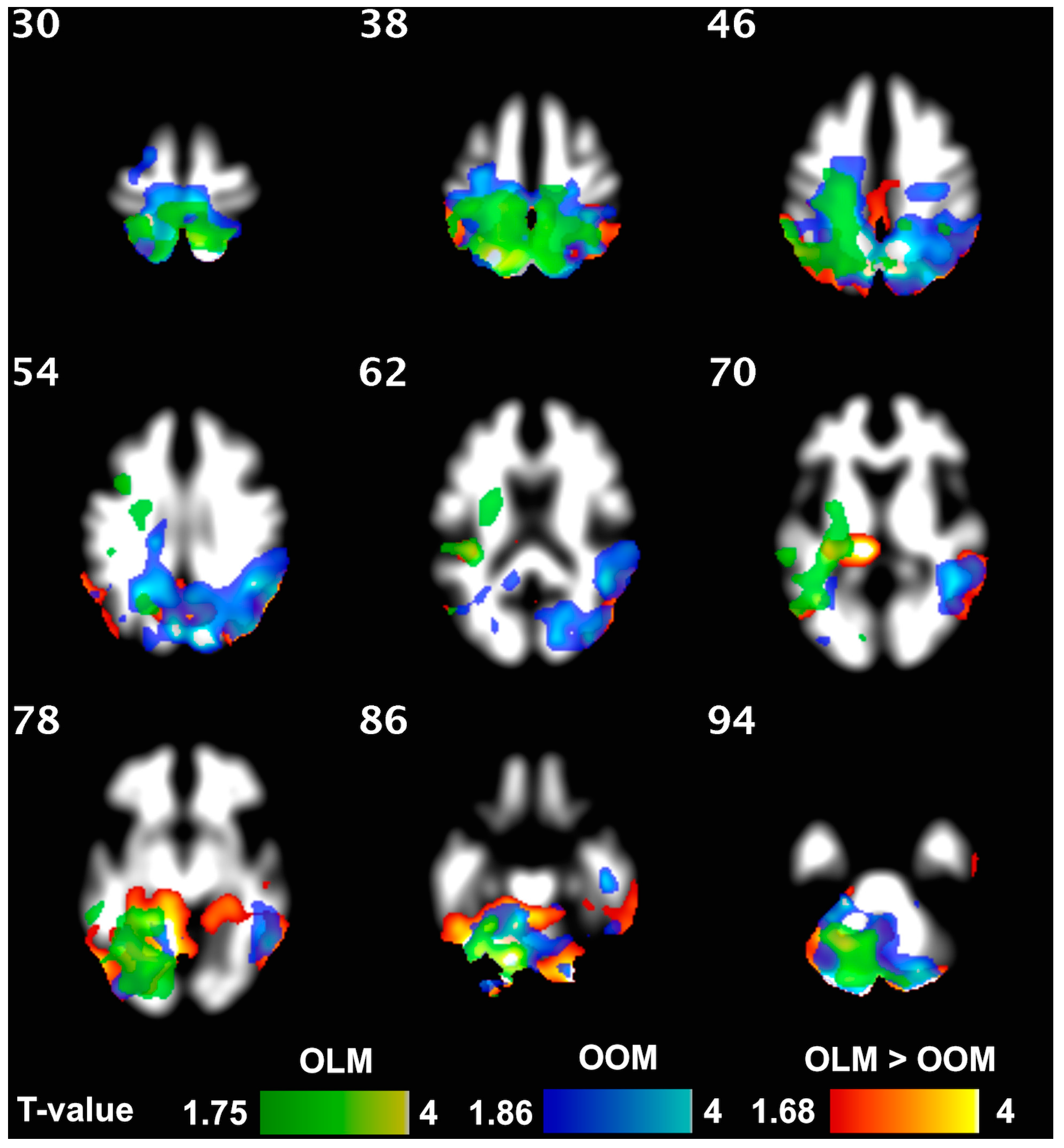
3.2. Comparison between Offspring of Lean Mothers (OLM) and Offspring of Obese Mothers (OOM) (and CTR): The Role of Maternal Obesity
3.3. Effect of Resistance Training on the Brain Structure of Frail Elderly Women
3.4. Cognitive Functioning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, J.A.; Greenhaff, P.L.; Bartlett, D.B.; Jackson, T.A.; Duggal, N.A.; Lord, J.M. Multisystem physiological perspective of human frailty and its modulation by physical activity. Physiol. Rev. 2023, 103, 1137–1191. [Google Scholar] [CrossRef] [PubMed]
- Kanai, R.; Rees, G. The structural basis of inter-individual differences in human behaviour and cognition. Nat. Rev. Neurosci. 2011, 12, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Abe, O.; Hagiwara, A.; Fujita, S.; Kamagata, K.; Hori, M.; Aoki, S.; Osada, T.; Konishi, S.; Masutani, Y.; et al. Advantages of Using Both Voxel- and Surface-based Morphometry in Cortical Morphology Analysis: A Review of Various Applications. Magn. Reson. Med. Sci. 2022, 21, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Farokhian, F.; Yang, C.; Beheshti, I.; Matsuda, H.; Wu, S. Age-Related Gray and White Matter Changes in Normal Adult Brains. Aging Dis. 2017, 8, 899–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry—The methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Bishop, N.A.; Lu, T.; Yankner, B.A. Neural mechanisms of ageing and cognitive decline. Nature 2010, 464, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Wang, L.; Geng, Z.; Zhu, Q.; Song, Z.; Chang, R.; Lv, H. A voxel-based morphometric study of age- and sex-related changes in white matter volume in the normal aging brain. Neuropsychiatr. Dis. Treat. 2016, 12, 453–465. [Google Scholar]
- Jernigan, T.L.; Archibald, S.L.; Fennema-Notestine, C.; Gamst, A.C.; Stout, J.C.; Bonner, J.; Hesselink, J.R. Effects of age on tissues and regions of the cerebrum and cerebellum. Neurobiol. Aging 2001, 22, 581–594. [Google Scholar] [CrossRef] [Green Version]
- Catalano, P.M.; Presley, L.; Minium, J.; Hauguel-de Mouzon, S. Fetuses of obese mothers develop insulin resistance in utero. Diabetes Care 2009, 32, 1076–1080. [Google Scholar] [CrossRef] [Green Version]
- Iozzo, P.; Holmes, M.; Schmidt, M.V.; Cirulli, F.; Guzzardi, M.A.; Berry, A.; Balsevich, G.; Andreassi, M.G.; Wesselink, J.J.; Liistro, T.; et al. Developmental ORIgins of Healthy and Unhealthy AgeiNg: The role of maternal obesity—Introduction to DORIAN. Obes. Facts 2014, 7, 130–151. [Google Scholar] [CrossRef] [PubMed]
- Schlabritz-Loutsevitch, N.; Jauregui, M.; Jain, B. Comment on the Recent Publication in the “New England Journal of Medicine”: “Trends in Mental Health Care among Children and Adolescents” (Olfson et al., 2015). J. Depress. Anxiety 2015, 4, 1000193. [Google Scholar]
- Eriksson, J.G.; Sandboge, S.; Salonen, M.K.; Kajantie, E.; Osmond, C. Long-term consequences of maternal overweight in pregnancy on offspring later health: Findings from the Helsinki Birth Cohort Study. Ann. Med. 2014, 46, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Van Lieshout, R.J.; Taylor, V.H.; Boyle, M.H. Pre-pregnancy and pregnancy obesity and neurodevelopmental outcomes in offspring: A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, e548–e559. [Google Scholar] [CrossRef] [PubMed]
- Bale, T.L. Epigenetic and transgenerational reprogramming of brain development. Nat. Rev. Neurosci. 2015, 16, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Heikura, U.; Taanila, A.; Hartikainen, A.L.; Olsen, P.; Linna, S.L.; von Wendt, L.; Jarvelin, M.R. Variations in prenatal sociodemographic factors associated with intellectual disability: A study of the 20-year interval between two birth cohorts in northern Finland. Am. J. Epidemiol. 2008, 167, 169–177. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Schieve, L.A.; Stein, A.D.; Swan, D.W.; Ramakrishnan, U.; Sharma, A.J. Associations between maternal prepregnancy body mass index and child neurodevelopment at 2 years of age. Int. J. Obes. 2012, 36, 1312–1319. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Yu, X.; Keim, S.; Li, L.; Zhang, L.; Zhang, J. Maternal prepregnancy obesity and child neurodevelopment in the Collaborative Perinatal Project. Int. J. Epidemiol. 2014, 43, 783–792. [Google Scholar] [CrossRef] [Green Version]
- Tanda, R.; Salsberry, P.J.; Reagan, P.B.; Fang, M.Z. The impact of prepregnancy obesity on children’s cognitive test scores. Matern. Child. Health J. 2013, 17, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Madden, D.J.; Bennett, I.J.; Burzynska, A.; Potter, G.G.; Chen, N.K.; Song, A.W. Diffusion tensor imaging of cerebral white matter integrity in cognitive aging. Biochim. Biophys. Acta 2012, 1822, 386–400. [Google Scholar] [CrossRef] [Green Version]
- Ou, X.; Thakali, K.M.; Shankar, K.; Andres, A.; Badger, T.M. Maternal adiposity negatively influences infant brain white matter development. Obesity 2015, 23, 1047–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, H.K.; Lipsitz, L.A. Cerebral white matter changes and geriatric syndromes: Is there a link? J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 818–826. [Google Scholar] [CrossRef]
- Cunnane, S.; Nugent, S.; Roy, M.; Courchesne-Loyer, A.; Croteau, E.; Tremblay, S.; Castellano, A.; Pifferi, F.; Bocti, C.; Paquet, N.; et al. Brain fuel metabolism, aging, and Alzheimer’s disease. Nutrition 2011, 27, 3–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mergenthaler, P.; Lindauer, U.; Dienel, G.A.; Meisel, A. Sugar for the brain: The role of glucose in physiological and pathological brain function. Trends Neurosci. 2013, 36, 587–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucci, M.; Huovinen, V.; Guzzardi, M.A.; Koskinen, S.; Raiko, J.R.; Lipponen, H.; Ahsan, S.; Badeau, R.M.; Honka, M.J.; Koffert, J.; et al. Resistance training improves skeletal muscle insulin sensitivity in elderly offspring of overweight and obese mothers. Diabetologia 2016, 59, 77–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brucher, N.; Mandegaran, R.; Filleron, T.; Wagner, T. Measurement of inter- and intra-observer variability in the routine clinical interpretation of brain 18-FDG PET-CT. Ann. Nucl. Med. 2015, 29, 233–239. [Google Scholar] [CrossRef]
- Boecker, H.; Drzezga, A. A perspective on the future role of brain pet imaging in exercise science. Neuroimage 2016, 131, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.P.; Barber, S.E.; Young, J.B.; Forster, A.; Iliffe, S.J. Do home-based exercise interventions improve outcomes for frail older people? Findings from a systematic review. Rev. Clin. Gerontol. 2012, 22, 68–78. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.M.; van Ravensberg, C.D.; Hobbelen, J.S.; Olde Rikkert, M.G.; Staal, J.B.; Nijhuis-van der Sanden, M.W. Effects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: A meta-analysis. Ageing Res. Rev. 2012, 11, 136–149. [Google Scholar] [CrossRef]
- Theou, O.; Stathokostas, L.; Roland, K.P.; Jakobi, J.M.; Patterson, C.; Vandervoort, A.A.; Jones, G.R. The effectiveness of exercise interventions for the management of frailty: A systematic review. J. Aging Res. 2011, 2011, 569194. [Google Scholar] [CrossRef] [Green Version]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef]
- Yu, R.; Tong, C.; Ho, F.; Woo, J. Effects of a Multicomponent Frailty Prevention Program in Prefrail Community-Dwelling Older Persons: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, e291–e294. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients during Acute Hospitalization: A Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.N.; White, S.M.; et al. Plasticity of brain networks in a randomized intervention trial of exercise training in older adults. Front. Aging Neurosci. 2010, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Tamura, M.; Nemoto, K.; Kawaguchi, A.; Kato, M.; Arai, T.; Kakuma, T.; Mizukami, K.; Matsuda, H.; Soya, H.; Asada, T. Long-term mild-intensity exercise regimen preserves prefrontal cortical volume against aging. Int. J. Geriatr. Psychiatry 2015, 30, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Syddall, H.; Cooper, C.; Martin, F.; Briggs, R.; Aihie Sayer, A. Is grip strength a useful single marker of frailty? Age Ageing 2003, 32, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbatecola, A.M.; Paolisso, G. Is there a relationship between insulin resistance and frailty syndrome? Curr. Pharm. Des. 2008, 14, 405–410. [Google Scholar]
- Yliharsila, H.; Kajantie, E.; Osmond, C.; Forsen, T.; Barker, D.J.; Eriksson, J.G. Birth size, adult body composition and muscle strength in later life. Int. J. Obes. 2007, 31, 1392–1399. [Google Scholar] [CrossRef] [Green Version]
- Ashburner, J. A fast diffeomorphic image registration algorithm. NeuroImage 2007, 38, 95–113. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage 2004, 23 (Suppl. S1), S208–S219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oguz, I.; Farzinfar, M.; Matsui, J.; Budin, F.; Liu, Z.; Gerig, G.; Johnson, H.J.; Styner, M. DTIPrep: Quality control of diffusion-weighted images. Front. Neuroinform. 2014, 8, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Rinne-Albers, M.A.; van der Werff, S.J.; van Hoof, M.J.; van Lang, N.D.; Lamers-Winkelman, F.; Rombouts, S.A.; Vermeiren, R.R.; van der Wee, N.J. Abnormalities of white matter integrity in the corpus callosum of adolescents with PTSD after childhood sexual abuse: A DTI study. Eur. Child. Adolesc. Psychiatry 2016, 25, 869–878. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Tobin, J.D.; Andres, R. Glucose clamp technique: A method for quantifying insulin secretion and resistance. Am. J. Physiol. 1979, 237, E214–E223. [Google Scholar] [CrossRef]
- Gjedde, A. Calculation of cerebral glucose phosphorylation from brain uptake of glucose analogs in vivo: A re-examination. Brain Res. 1982, 257, 237–274. [Google Scholar] [CrossRef]
- Heinonen, K.; Eriksson, J.G.; Lahti, J.; Kajantie, E.; Pesonen, A.K.; Tuovinen, S.; Osmond, C.; Raikkonen, K. Late preterm birth and neurocognitive performance in late adulthood: A birth cohort study. Pediatrics 2015, 135, e818–e825. [Google Scholar] [CrossRef] [Green Version]
- Good, C.D.; Johnsrude, I.S.; Ashburner, J.; Henson, R.N.; Friston, K.J.; Frackowiak, R.S. A voxel-based morphometric study of ageing in 465 normal adult human brains. NeuroImage 2001, 14, 21–36. [Google Scholar] [CrossRef] [Green Version]
- Heise, D.R. Separating reliability and stability in test-retest correlation. Am. Sociol. Rev. 1969, 34, 93–101. [Google Scholar] [CrossRef]
- Chen, W.T.; Chou, K.H.; Liu, L.K.; Lee, P.L.; Lee, W.J.; Chen, L.K.; Wang, P.N.; Lin, C.P. Reduced cerebellar gray matter is a neural signature of physical frailty. Hum. Brain Mapp. 2015, 36, 3666–3676. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Kant, I.M.J.; de Bresser, J.; van Montfort, S.J.T.; Aarts, E.; Verlaan, J.J.; Zacharias, N.; Winterer, G.; Spies, C.; Slooter, A.J.C.; Hendrikse, J.; et al. The association between brain volume, cortical brain infarcts, and physical frailty. Neurobiol. Aging 2018, 70, 247–253. [Google Scholar] [CrossRef]
- Mosconi, L. Glucose metabolism in normal aging and Alzheimer’s disease: Methodological and physiological considerations for PET studies. Clin. Transl. Imaging 2013, 1, 217–233. [Google Scholar] [CrossRef] [Green Version]
- Rebelos, E.; Bucci, M.; Karjalainen, T.; Oikonen, V.; Bertoldo, A.; Hannukainen, J.C.; Virtanen, K.A.; Latva-Rasku, A.; Hirvonen, J.; Heinonen, I.; et al. Insulin Resistance Is Associated with Enhanced Brain Glucose Uptake during Euglycemic Hyperinsulinemia: A Large-Scale PET Cohort. Diabetes Care 2021, 44, 788–794. [Google Scholar] [CrossRef]
- Sanguinetti, E.; Liistro, T.; Mainardi, M.; Pardini, S.; Salvadori, P.A.; Vannucci, A.; Burchielli, S.; Iozzo, P. Maternal high-fat feeding leads to alterations of brain glucose metabolism in the offspring: Positron emission tomography study in a porcine model. Diabetologia 2016, 59, 813–821. [Google Scholar] [CrossRef] [Green Version]
- Jordan, N.; Gvalda, M.; Cody, R.; Galante, O.; Haywood, C.; Yates, P. Frailty, MRI, and FDG-PET Measures in an Australian Memory Clinic Cohort. Front. Med. 2020, 7, 578243. [Google Scholar] [CrossRef] [PubMed]
- Rajasilta, O.; Häkkinen, S.; Björnsdotter, M.; Scheinin, N.M.; Lehtola, S.J.; Saunavaara, J.; Parkkola, R.; Lähdesmäki, T.; Karlsson, L.; Karlsson, H.; et al. Maternal pre-pregnancy BMI associates with neonate local and distal functional connectivity of the left superior frontal gyrus. Sci. Rep. 2021, 11, 19182. [Google Scholar] [CrossRef]
- Poulakis, K.; Reid, R.I.; Przybelski, S.A.; Knopman, D.S.; Graff-Radford, J.; Lowe, V.J.; Mielke, M.M.; Machulda, M.M.; Jack, C.R.; Petersen, R.C.; et al. Longitudinal deterioration of white-matter integrity: Heterogeneity in the ageing population. Brain Commun. 2021, 3, fcaa238. [Google Scholar] [CrossRef]
- Gine-Garriga, M.; Roque-Figuls, M.; Coll-Planas, L.; Sitja-Rabert, M.; Salva, A. Physical exercise interventions for improving performance-based measures of physical function in community-dwelling, frail older adults: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 753–769 e753. [Google Scholar] [CrossRef]
- Honka, M.J.; Bucci, M.; Andersson, J.; Huovinen, V.; Guzzardi, M.A.; Sandboge, S.; Savisto, N.; Salonen, M.K.; Badeau, R.M.; Parkkola, R.; et al. Resistance training enhances insulin suppression of endogenous glucose production in elderly women. J. Appl. Physiol. 2016, 120, 633–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, H.; Ishii, K.; Makizako, H.; Ishiwata, K.; Oda, K.; Suzukawa, M. Effects of exercise on brain activity during walking in older adults: A randomized controlled trial. J. Neuroeng. Rehabil. 2017, 14, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, A.G.; Dennis, A.; Bandettini, P.A.; Johansen-Berg, H. The effects of aerobic activity on brain structure. Front. Psychol. 2012, 3, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intzandt, B.; Vrinceanu, T.; Huck, J.; Vincent, T.; Montero-Odasso, M.; Gauthier, C.J.; Bherer, L. Comparing the effect of cognitive vs. exercise training on brain MRI outcomes in healthy older adults: A systematic review. Neurosci. Biobehav. Rev. 2021, 128, 511–533. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; Tang, Y.; Bennett, D.A. Frailty is associated with incident Alzheimer’s disease and cognitive decline in the elderly. Psychosom. Med. 2007, 69, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Spencer, F.H.; Bornholt, L.J.; Ouvrier, R.A. Test reliability and stability of children’s cognitive functioning. J. Child. Neurol. 2003, 18, 5–11. [Google Scholar] [CrossRef]
- Willis, S.L.U.; Schaie, K.W. Cognitive functioning in baby boomers: Longitudinal and cohort effects. In The Baby Boomers Grow Up: Contemporary Perspectives on Midlife; Whitbourne, S.K., Willis, S.L.U., Eds.; Taylor & Francis: Abingdon, UK, 2014; pp. 205–234. [Google Scholar]
- Liao, Y.Y.; Chen, I.H.; Hsu, W.C.; Tseng, H.Y.; Wang, R.Y. Effect of exergaming versus combined exercise on cognitive function and brain activation in frail older adults: A randomised controlled trial. Ann. Phys. Rehabil. Med. 2021, 64, 101492. [Google Scholar] [CrossRef]
- Filley, C.M.; Fields, R.D. White matter and cognition: Making the connection. J. Neurophysiol. 2016, 116, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Walther, K.; Birdsill, A.C.; Glisky, E.L.; Ryan, L. Structural brain differences and cognitive functioning related to body mass index in older females. Hum. Brain Mapp. 2010, 31, 1052–1064. [Google Scholar] [CrossRef]
- Ryan, L.; Walther, K. White matter integrity in older females is altered by increased body fat. Obesity 2014, 22, 2039–2046. [Google Scholar] [CrossRef] [Green Version]
- Borkowski, K.; Krzyżak, A.T. Analysis and correction of errors in DTI-based tractography due to diffusion gradient inhomogeneity. J. Magn. Reson. 2018, 296, 5–11. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Controls (n = 9) | Frails (n = 37) | p | OLM (n = 20) | OOM (n = 17) | p | |
|---|---|---|---|---|---|---|
| Age (years) | 71.7 ± 1.0 | 71.8 ± 0.5 | 0.98 ^ | 72.2 ± 0.6 | 71.5 ± 0.9 | 0.27 ^ |
| BMI (kg/m2) | 27.8 ± 1.4 | 27.2 ± 0.8 | 0.70 | 26.6 ± 1.1 | 27.9 ± 1.1 | 0.40 |
| fP-Glucose (mmol/L) | 6.4 ± 0.3 | 6.0 ± 0.1 | 0.21 ^ | 6.0 ± 0.2 | 5.9 ± 0.2 | 0.99 ^ |
| fP-Insulin (mU/I) | 10.7 ± 2.2 | 9.5 ± 0.9 | 0.60 ^ | 9.6 ± 1.4 | 9.4 ± 1.2 | 0.78 ^ |
| Offspring of Lean Mothers | Offspring of Obese Mothers | |||||
|---|---|---|---|---|---|---|
| Baseline (n = 20) | Treatment (n = 19) | p | Baseline (n = 17) | Treatment (n = 16) | p | |
| BMI (kg/m2) | 26.6 ± 1.1 | 27.1 ± 1.1 | 0.52 | 27.9 ± 1.1 | 27.6 ± 1.2 | 0.92 |
| fP-Glucose (mmol/L) | 6.0 ± 0.2 | 6.1 ± 0.2 | 0.43 | 5.9 ± 0.2 | 5.8 ± 0.2 | 0.92 |
| fP-Insulin (mU/I) | 9.6 ± 1.4 | 9.5 ± 1.1 | 0.70 | 9.4 ± 1.2 | 9.7 ± 1.4 | 0.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bucci, M.; Iozzo, P.; Merisaari, H.; Huovinen, V.; Lipponen, H.; Räikkönen, K.; Parkkola, R.; Salonen, M.; Sandboge, S.; Eriksson, J.G.; et al. Resistance Training Increases White Matter Density in Frail Elderly Women. J. Clin. Med. 2023, 12, 2684. https://doi.org/10.3390/jcm12072684
Bucci M, Iozzo P, Merisaari H, Huovinen V, Lipponen H, Räikkönen K, Parkkola R, Salonen M, Sandboge S, Eriksson JG, et al. Resistance Training Increases White Matter Density in Frail Elderly Women. Journal of Clinical Medicine. 2023; 12(7):2684. https://doi.org/10.3390/jcm12072684
Chicago/Turabian StyleBucci, Marco, Patricia Iozzo, Harri Merisaari, Ville Huovinen, Heta Lipponen, Katri Räikkönen, Riitta Parkkola, Minna Salonen, Samuel Sandboge, Johan Gunnar Eriksson, and et al. 2023. "Resistance Training Increases White Matter Density in Frail Elderly Women" Journal of Clinical Medicine 12, no. 7: 2684. https://doi.org/10.3390/jcm12072684