
Prognostic Value of Absolute Lymphocyte Count in Patients with Advanced Renal Cell Carcinoma Treated with Nivolumab Plus Ipilimumab
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Statistical Analysis
2.3. Ethical Approval
3. Results
3.1. Patient Characteristics
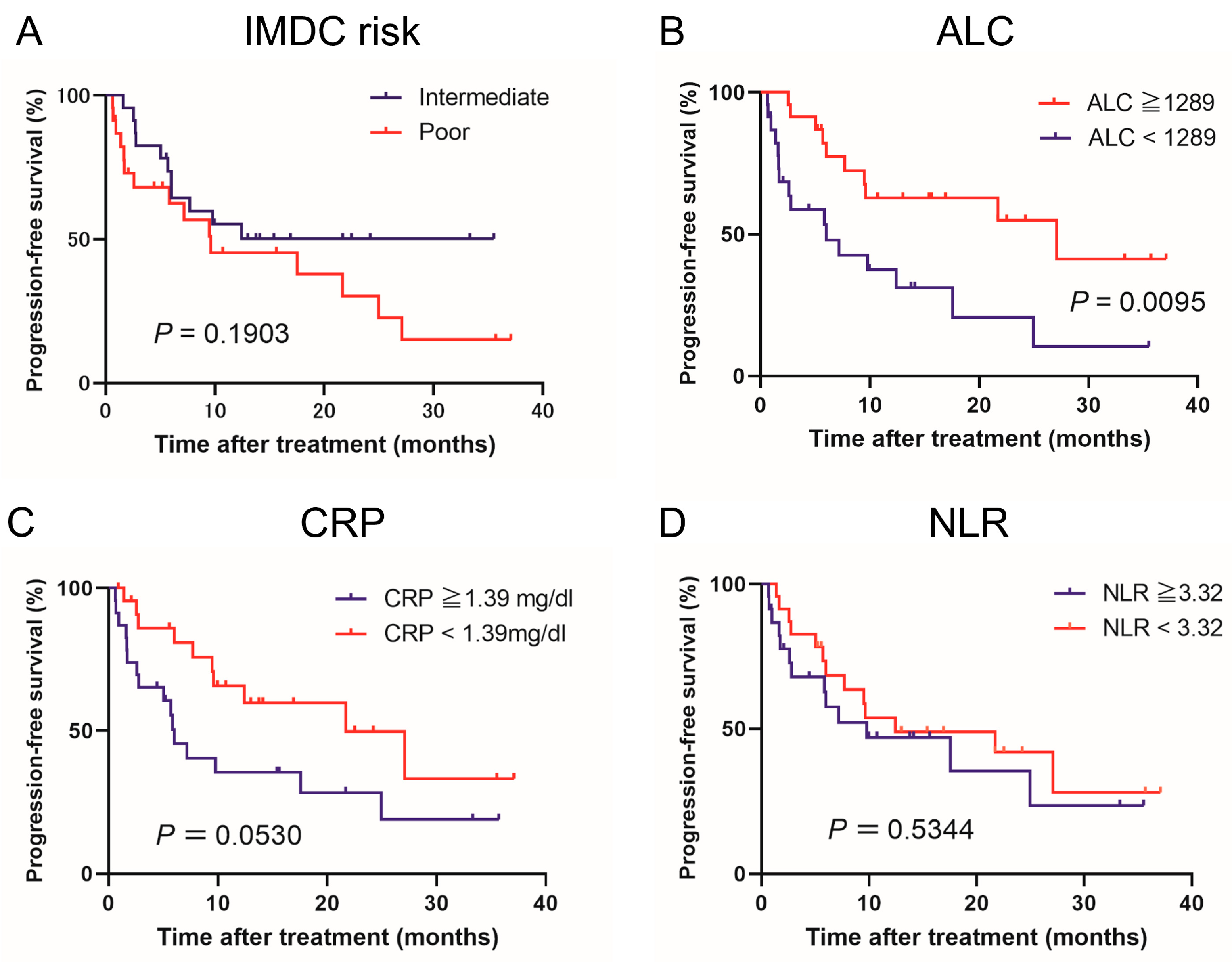
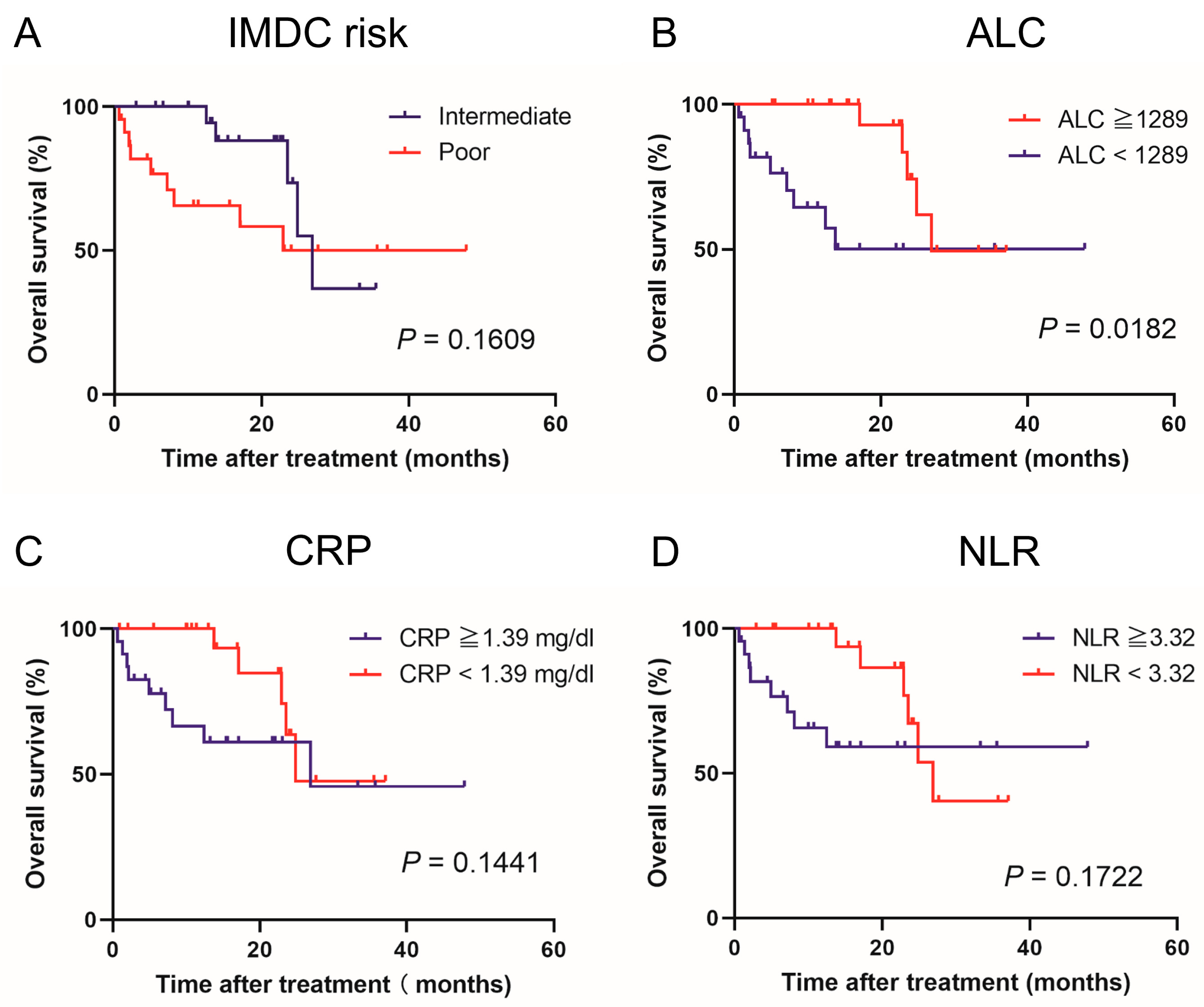
3.2. Clinical Course According to IMDC Risk Classification and Pretreatment Peripheral Inflammatory Biomarkers
3.3. Univariate and Multivariate Analyses of Pretreatment Prognostic Factors
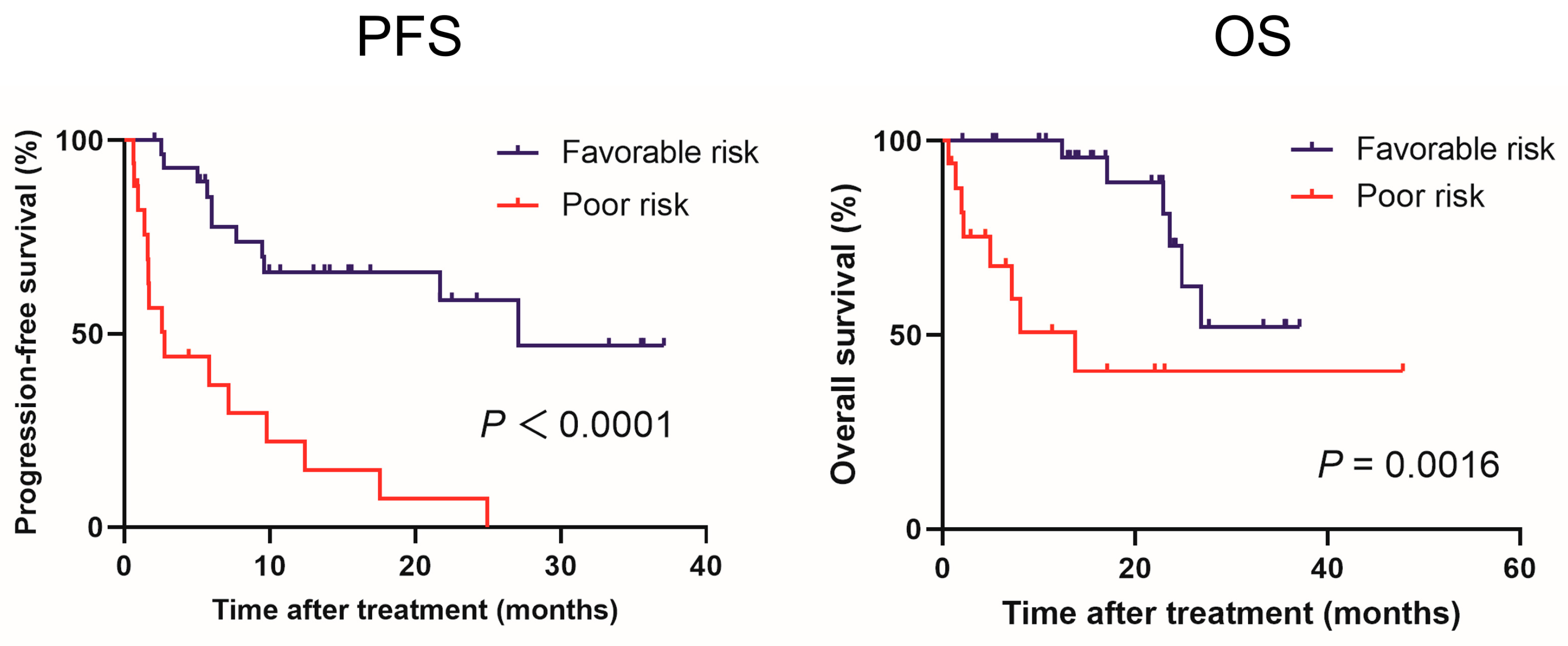
3.4. Prognostic Model Using Prior Nephrectomy and ALC (ALNx Model)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ernst, M.S.; Navani, V.; Wells, J.C.; Donskov, F.; Basappa, N.; Labaki, C.; Pal, S.K.; Meza, L.; Wood, L.A.; Ernst, D.S.; et al. Outcomes for International Metastatic Renal Cell Carcinoma Database Consortium Prognostic Groups in Contemporary First-line Combination Therapies for Metastatic Renal Cell Carcinoma. Eur. Urol. 2023, in press. [Google Scholar] [CrossRef]
- Rathmell, W.K.; Rumble, R.B.; Van Veldhuizen, P.J.; Al-Ahmadie, H.; Emamekhoo, H.; Hauke, R.J.; Louie, A.V.; Milowsky, M.I.; Molina, A.M.; Rose, T.L.; et al. Management of Metastatic Clear Cell Renal Cell Carcinoma: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2957–2995. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Suekane, S.; Kurose, H.; Ito, N.; Ogasawara, N.; Hiroshige, T.; Chikui, K.; Ejima, K.; Uemura, K.; Nakiri, M.; et al. Improved survival of real-world Japanese patients with advanced renal cell carcinoma treated with immuno-oncology combination therapy. Anticancer Res. 2022, 42, 4573–4580. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Ueda, K.; Suekane, S.; Kurose, H.; Ito, N.; Ogasawara, N.; Hiroshige, T.; Chikui, K.; Ejima, K.; Uemura, K.; Nakiri, M.; et al. Immune-related adverse events are clinical biomarkers to predict favorable outcomes in advanced renal cell carcinoma treated with nivolumab plus ipilimumab. Jpn. J. Clin. Oncol. 2022, 52, 479–485. [Google Scholar] [CrossRef]
- Paderi, A.; Giorgione, R.; Giommoni, E.; Mela, M.M.; Rossi, V.; Doni, L.; Minervini, A.; Carini, M.; Pillozzi, S.; Antonuzzo, L. Association between immune related adverse events and outcome in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors. Cancers 2021, 13, 860. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Hussaini, S.; Chehade, R.; Boldt, R.G.; Raphael, J.; Blanchette, P.; Maleki Vareki, S.; Fernandes, R. Association between immune-related side effects and efficacy and benefit of immune checkpoint inhibitors—A systematic review and meta-analysis. Cancer Treat. Rev. 2021, 92, 102134. [Google Scholar] [CrossRef]
- Anker, J.; Miller, J.; Taylor, N.; Kyprianou, N.; Tsao, C.K. From bench to bedside: How the tumor microenvironment is impacting the future of immunotherapy for renal cell carcinoma. Cells 2021, 10, 3231. [Google Scholar] [CrossRef]
- Ueda, K.; Suekane, S.; Kurose, H.; Ogasawara, N.; Hiroshige, T.; Chikui, K.; Uemura, K.; Nakiri, M.; Nishihara, K.; Matsuo, M.; et al. Absolute lymphocyte count is an independent predictor of survival in patients with metastatic renal cell carcinoma treated with nivolumab. Jpn. J. Clin. Oncol. 2022, 52, 179–186. [Google Scholar] [CrossRef]
- Inoue, H.; Shiozaki, A.; Fujiwara, H.; Konishi, H.; Kiuchi, J.; Ohashi, T.; Shimizu, H.; Arita, T.; Yamamoto, Y.; Morimura, R.; et al. Absolute lymphocyte count and C-reactive protein-albumin ratio can predict prognosis and adverse events in patients with recurrent esophageal cancer treated with nivolumab therapy. Oncol. Lett. 2022, 24, 257. [Google Scholar] [CrossRef]
- Ho, W.J.; Yarchoan, M.; Hopkins, A.; Mehra, R.; Grossman, S.; Kang, H. Association between pretreatment lymphocyte count and response to PD1 inhibitors in head and neck squamous cell carcinomas. J. Immunother. Cancer 2018, 6, 84. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Choueiri, T.K.; McDermott, D.F.; Powles, T.; Vano, Y.A.; Gupta, S.; Yao, J.; Han, C.; Ammar, R.; Papillon-Cavanagh, S.; et al. Biomarker analysis from CheckMate 214: Nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma. J. Immunother. Cancer 2022, 10, e004316. [Google Scholar] [CrossRef] [PubMed]
- Yano, Y.; Ohno, T.; Komura, K.; Fukuokaya, W.; Uchimoto, T.; Adachi, T.; Hirasawa, Y.; Hashimoto, T.; Yoshizawa, A.; Yamazaki, S.; et al. Serum C-reactive protein level predicts overall survival for clear cell and non-clear cell renal cell carcinoma treated with ipilimumab plus nivolumab. Cancers 2022, 14, 5659. [Google Scholar] [CrossRef]
- Iinuma, K.; Enomoto, T.; Kawada, K.; Fujimoto, S.; Ishida, T.; Takagi, K.; Nagai, S.; Ito, H.; Kawase, M.; Nakai, C.; et al. Utility of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and systemic immune inflammation index as prognostic, predictive biomarkers in patients with metastatic renal cell carcinoma treated with nivolumab and ipilimumab. J. Clin. Med. 2021, 10, 5325. [Google Scholar] [CrossRef] [PubMed]
- Pham, F.; Belkaid, S.; Maillet, D.; Confavreux, C.B.; Dalle, S.; Péron, J. Impact of bone metastases on patients with renal cell carcinoma or melanoma treated with Combotherapy ipilimumab plus nivolumab. Biomedicines 2022, 10, 2758. [Google Scholar] [CrossRef]
- Tucker, M.D.; Brown, L.C.; Chen, Y.W.; Kao, C.; Hirshman, N.; Kinsey, E.N.; Ancell, K.K.; Beckermann, K.E.; Davis, N.B.; McAlister, R.; et al. Association of baseline neutrophil-to-eosinophil ratio with response to nivolumab plus ipilimumab in patients with metastatic renal cell carcinoma. Biomark. Res. 2021, 9, 80. [Google Scholar] [CrossRef]
- Yasuda, Y.; Saito, K.; Yuasa, T.; Uehara, S.; Kawamura, N.; Yokoyama, M.; Ishioka, J.; Matsuoka, Y.; Yamamoto, S.; Okuno, T.; et al. Early response of C-reactive protein as a predictor of survival in patients with metastatic renal cell carcinoma treated with tyrosine kinase inhibitors. Int. J. Clin. Oncol. 2017, 22, 1081–1086. [Google Scholar] [CrossRef]
- Templeton, A.J.; Knox, J.J.; Lin, X.; Simantov, R.; Xie, W.; Lawrence, N.; Broom, R.; Fay, A.P.; Rini, B.; Donskov, F.; et al. Change in neutrophil-to-lymphocyte ratio in response to targeted therapy for metastatic renal cell carcinoma as a prognosticator and biomarker of efficacy. Eur. Urol. 2016, 70, 358–364. [Google Scholar] [CrossRef]
- Patel, S.H.; Derweesh, I.H.; Saito, K.; Patil, D.; Meagher, M.F.; Bindayi, A.; Eldefrawy, A.; Patel, D.N.; Nasseri, R.; Yasuda, Y.; et al. Preoperative elevation of C-reactive protein is a predictor for adverse oncologic survival outcomes for renal cell carcinoma: Analysis from the international marker consortium renal cancer (INMARC). Clin. Genitourin. Cancer 2021, 19, e206–e215. [Google Scholar] [CrossRef]
- Ishihara, H.; Tachibana, H.; Takagi, T.; Kondo, T.; Fukuda, H.; Yoshida, K.; Iizuka, J.; Kobayashi, H.; Okumi, M.; Ishida, H.; et al. Predictive impact of peripheral blood markers and C-reactive protein in nivolumab therapy for metastatic renal cell carcinoma. Target. Oncol. 2019, 14, 453–463. [Google Scholar] [CrossRef]
- Cho, Y.; Park, S.; Byun, H.K.; Lee, C.G.; Cho, J.; Hong, M.H.; Kim, H.R.; Cho, B.C.; Kim, S.; Park, J.; et al. Impact of treatment-related lymphopenia on immunotherapy for advanced non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Bi, Y.; Xue, J.; Liu, Y.; Zhu, J.; Qin, S. Prognostic value of absolute lymphocyte count in patients with advanced esophageal cancer treated with immunotherapy: A retrospective analysis. Ann. Transl. Med. 2022, 10, 744. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Chasalow, S.D.; Kuk, D.; Panageas, K.S.; Cheng, M.L.; Yuan, J.; Wolchok, J.D. Absolute lymphocyte count as a prognostic biomarker for overall survival in patients with advanced melanoma treated with ipilimumab. Melanoma Res. 2020, 30, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.J.; Xie, W.; Kroeger, N.; Lee, J.L.; Rini, B.I.; Knox, J.J.; Bjarnason, G.A.; Srinivas, S.; Pal, S.K.; Yuasa, T.; et al. The International Metastatic Renal Cell Carcinoma Database Consortium model as a prognostic tool in patients with metastatic renal cell carcinoma previously treated with first-line targeted therapy: A population-based study. Lancet Oncol. 2015, 16, 293–300. [Google Scholar] [CrossRef]
- Escudier, B.; Motzer, R.J.; Tannir, N.M.; Porta, C.; Tomita, Y.; Maurer, M.A.; McHenry, M.B.; Rini, B.I. Efficacy of Nivolumab plus Ipilimumab According to Number of IMDC Risk Factors in ChechMate 214. Eur. Urol. 2022, 77, 449–453. [Google Scholar] [CrossRef]
- Méjean, A.; Ravaud, A.; Thezenas, S.; Colas, S.; Beauval, J.B.; Bensalah, K.; Geoffrois, L.; Thiery-Vuillemin, A.; Cormier, L.; Lang, H.; et al. Sunitinib Alone or after Nephrectomy in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 417–427. [Google Scholar] [CrossRef]
- Bex, A.; Mulders, P.; Jewett, M.; Wagstaff, J.; van Thienen, J.V.; Blank, C.U.; van Velthoven, R.; Del Pilar Laguna, M.; Wood, L.; van Melick, H.H.E.; et al. Nephrectomy in Patients with Synchronous Metastatic Renal Cell Carcinoma Receiving Sunitinib: The SURTIME Randomized Clinical Trial. JAMA Oncol. 2019, 5, 164–170. [Google Scholar] [CrossRef]
- Tanaka, T.; Hatakeyama, S.; Numakura, K.; Kido, K.; Noro, D.; Oikawa, M.; Hosogoe, S.; Tokui, N.; Yamamoto, H.; Narita, S.; et al. Efficacy and safety of first-line nivolumab plus ipilimumab in patients with metastatic renal cell carcinoma: A multicenter retrospective study. Int. J. Urol. 2020, 27, 1095–1100. [Google Scholar] [CrossRef]
- Kato, T.; Fujita, K.; Minami, T.; Nagahara, A.; Hyashi, Y.; Nakata, W.; Matsuzaki, K.; Nakano, K.; Hatano, K.; Kawashima, A.; et al. Real-world efficacy and safety of nivolumab plus ipilimumab in untreated metastatic renal cell carcinoma, and the impact of previous nephrectomy on clinical outcome: Japanese multi-institutional retrospective study. Int. J. Clin. Oncol. 2022, 27, 1596–1604. [Google Scholar] [CrossRef]
- Albiges, L.; Tannir, N.M.; Burotto, M.; McDermott, D.; Plimack, E.R.; Barthélémy, P.; Porta, C.; Powles, T.; Donskov, F.; George, S.; et al. First-Line Nivolumab Plus Ipilimumab versus Sunitinib in Patients without Nephrectomy and with an Evaluable Primary Renal Tumor in the CheckMate 214 Trial. Eur. Urol. 2022, 81, 266–271. [Google Scholar] [CrossRef]
- Okadome, K.; Baba, Y.; Yagi, T.; Kiyozumi, Y.; Ishimoto, T.; Iwatsuki, M.; Miyamoto, Y.; Yoshida, N.; Watanabe, M.; Baba, H. Prognostic nutritional index, Tumor-infiltrating Lymphocytes, and Prognosis in Patients with Esophageal Cancer. Ann. Surg. 2020, 271, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kim, E.Y.; Yun, J.S.; Park, Y.L.; Do, S.I.; Chae, S.W.; Park, C.H. The prognostic and predictive value of tumor-infiltrating lymphocytes and hematologic parameters in patients with breast cancer. BMC Cancer 2018, 18, 938. [Google Scholar] [CrossRef] [PubMed]
- Rappold, P.M.; Vuong, L.; Leibold, J.; Chakiryan, N.H.; Curry, M.; Kuo, F.; Sabio, E.; Jiang, H.; Nixon, B.G.; Liu, M.; et al. A Targetable Myeloid Inflammatory State Governs Disease Recurrence in Clear-Cell Renal Cell Carcinoma. Cancer Discov. 2022, 12, 2308–2329. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Feature | Total (n = 46) | ALC ≥ 1289 (n = 23) | ALC < 1289 (n = 23) | p | |
|---|---|---|---|---|---|
| Age, years, range | 66.5 (42–80) | 67 (42–80) | 66.5 (48–80) | 0.5974 | |
| Sex, n (%) | Male | 39 (84.8) | 21 (91.3) | 18 (78.3) | 0.2118 |
| Female | 7 (15.2) | 2 (8.7) | 5 (21.7) | ||
| BMI (kg/m2), median | 22.7 | 24.6 | 21.4 | 0.0098 | |
| Prior nephrectomy, n (%) | Yes | 17 (37.0) | 11 (47.8) | 6 (26.1) | 0.1246 |
| No | 29 (63.0) | 12 (52.2) | 17 (73.9) | ||
| Performance status, n (%) | 0, 1 | 39 (84.8) | 19 (82.6) | 20 (87.0) | 0.6810 |
| ≥2 | 7 (15.2) | 4 (17.4) | 3 (13.0) | ||
| Histological subtype, n (%) | CCRCC | 37 (80.4) | 20 (87.0) | 17 (73.9) | 0.4557 |
| Non-CCRCC | 7 (15.2) | 2 (8.7) | 5 (21.7) | ||
| Unknown | 2 (4.3) | 1 (4.3) | 1 (4.3) | ||
| IMDC risk classification, n (%) | Intermediate | 23 (50.0) | 14 (60.9) | 9 (39.1) | 0.1388 |
| Poor | 23 (50.0) | 9 (39.1) | 14 (60.9) | ||
| Liver metastasis, n (%) | No | 42 (91.3) | 21 (91.3) | 21 (91.3) | 1.0000 |
| Yes | 4 (8.7) | 2 (8.7) | 2 (8.7) | ||
| Bone metastasis, n (%) | No | 33 (71.7) | 17 (73.9) | 16 (69.6) | 0.7432 |
| Yes | 13 (28.3) | 6 (26.1) | 7 (30.4) | ||
| Charlson comorbidity score, n (%) | ≤2 | 44 (95.7) | 22 (95.7) | 22 (95.7) | 1.0000 |
| ≥3 | 2 (4.3) | 1 (4.3) | 1 (4.3) | ||
| Monocyte count, median (range) | 399.5 (128.7–620.0) | 396.5 (255.0–600.6) | 402.1 (128.7–620.0) | 0.8519 | |
| NLR, median (range) | 3.32 (1.03–11.51) | 2.30 (1.03–4.16) | 4.99 (2.65–11.51) | <0.0001 | |
| CRP, mg/dL, median (range) | 1.39 (0.08–18.58) | 0.62 (0.08–7.36) | 3.27 (0.32–18.58) | 0.0081 |
| Progression-Free Survival (n = 46) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | HR | p-Value | HR | p-Value |
| Age (≥70 years) | 0.815 (0.342–1.940) | 0.6434 | ||
| Sex (female) | 2.016 (0.748–5.436) | 0.1657 | ||
| Prior nephrectomy (no) | 4.162 (1.554–11.148) | 0.0046 | 3.854 (1.433–10.359) | 0.0075 |
| Performance status (≥2) | 1.393 (0.474–4.090) | 0.5467 | ||
| IMDC risk classification (poor) | 1.678 (0.766–3.675) | 0.1957 | ||
| Liver metastasis (yes) | 1.175 (0.276–5.012) | 0.8271 | ||
| Bone metastasis (yes) | 1.546 (0.686–3.484) | 0.2934 | ||
| CRP (mg/dL) (≥1.39) | 2.149 (0.971–4.756) | 0.0591 | ||
| ALC (<1289) | 2.762 (1.241–6.149) | 0.0128 | 2.513 (1.119–5.648) | 0.0257 |
| Monocyte count (≥399.5) | 1.419 (0.653–3.084) | 0.3768 | ||
| Anemia (yes) | 4.971 (0.672–36.785) | 0.1164 | ||
| Calcium (upper limit over) | 1.712 (0.753–3.888) | 0.1993 | ||
| Neutrophil count (upper limit over) | 1.970 (0.671–5.783) | 0.2169 | ||
| Platelet count (upper limit over) | 1.349 (0.507–3.587) | 0.5486 | ||
| Overall Survival (n = 46) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | HR | p-Value | HR | p-Value |
| Age (≥70 years) | 0.385 (0.086–1.723) | 0.2118 | ||
| Sex (female) | 4.093 (1.211–13.835) | 0.0233 | 3.659 (1.055–12.687) | 0.0409 |
| Prior nephrectomy (no) | 3.078 (0.854–11.089) | 0.0856 | ||
| Performance status (≥2) | 3.814 (1.138–12.790) | 0.0301 | ||
| IMDC risk classification (poor) | 2.156 (0.718–6.476) | 0.1709 | ||
| Liver metastasis (yes) | 0.675 (0.087–5.210) | 0.7059 | ||
| Bone metastasis (yes) | 1.408 (0.468–4.238) | 0.5424 | ||
| CRP (mg/dL) (≥1.39) | 2.455 (0.834–7.225) | 0.1029 | ||
| ALC (<1289) | 3.564 (1.166–10.896) | 0.0258 | 3.367 (1.075–10.541) | 0.0371 |
| Monocyte count (≥399.5) | 2.789 (0.868–8.962) | 0.0851 | ||
| Anemia (yes) | 1.955 (0.255–14.980) | 0.5188 | ||
| Calcium (upper limit over) | 1.116 (0.342–3.639) | 0.8551 | ||
| Neutrophil count (upper limit over) | 3.013 (0.831–10.930) | 0.0934 | ||
| Platelet count (upper limit over) | 2.995 (0.924–9.706) | 0.0675 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, K.; Ogasawara, N.; Ito, N.; Ohnishi, S.; Suekane, H.; Kurose, H.; Hiroshige, T.; Chikui, K.; Uemura, K.; Nishihara, K.; et al. Prognostic Value of Absolute Lymphocyte Count in Patients with Advanced Renal Cell Carcinoma Treated with Nivolumab Plus Ipilimumab. J. Clin. Med. 2023, 12, 2417. https://doi.org/10.3390/jcm12062417
Ueda K, Ogasawara N, Ito N, Ohnishi S, Suekane H, Kurose H, Hiroshige T, Chikui K, Uemura K, Nishihara K, et al. Prognostic Value of Absolute Lymphocyte Count in Patients with Advanced Renal Cell Carcinoma Treated with Nivolumab Plus Ipilimumab. Journal of Clinical Medicine. 2023; 12(6):2417. https://doi.org/10.3390/jcm12062417
Chicago/Turabian StyleUeda, Kosuke, Naoyuki Ogasawara, Naoki Ito, Satoshi Ohnishi, Hiroki Suekane, Hirofumi Kurose, Tasuku Hiroshige, Katsuaki Chikui, Keiichiro Uemura, Kiyoaki Nishihara, and et al. 2023. "Prognostic Value of Absolute Lymphocyte Count in Patients with Advanced Renal Cell Carcinoma Treated with Nivolumab Plus Ipilimumab" Journal of Clinical Medicine 12, no. 6: 2417. https://doi.org/10.3390/jcm12062417