
Features of Obstructive Sleep Apnea in Children with and without Comorbidities

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Clinical Protocol
2.3. Diagnostic Procedure
2.4. Patient Groups
2.5. Therapeutic Protocol
2.6. Sample Size Calculation
2.7. Statistical Analysis
2.8. Ethical Aspects
3. Results
3.1. General Results
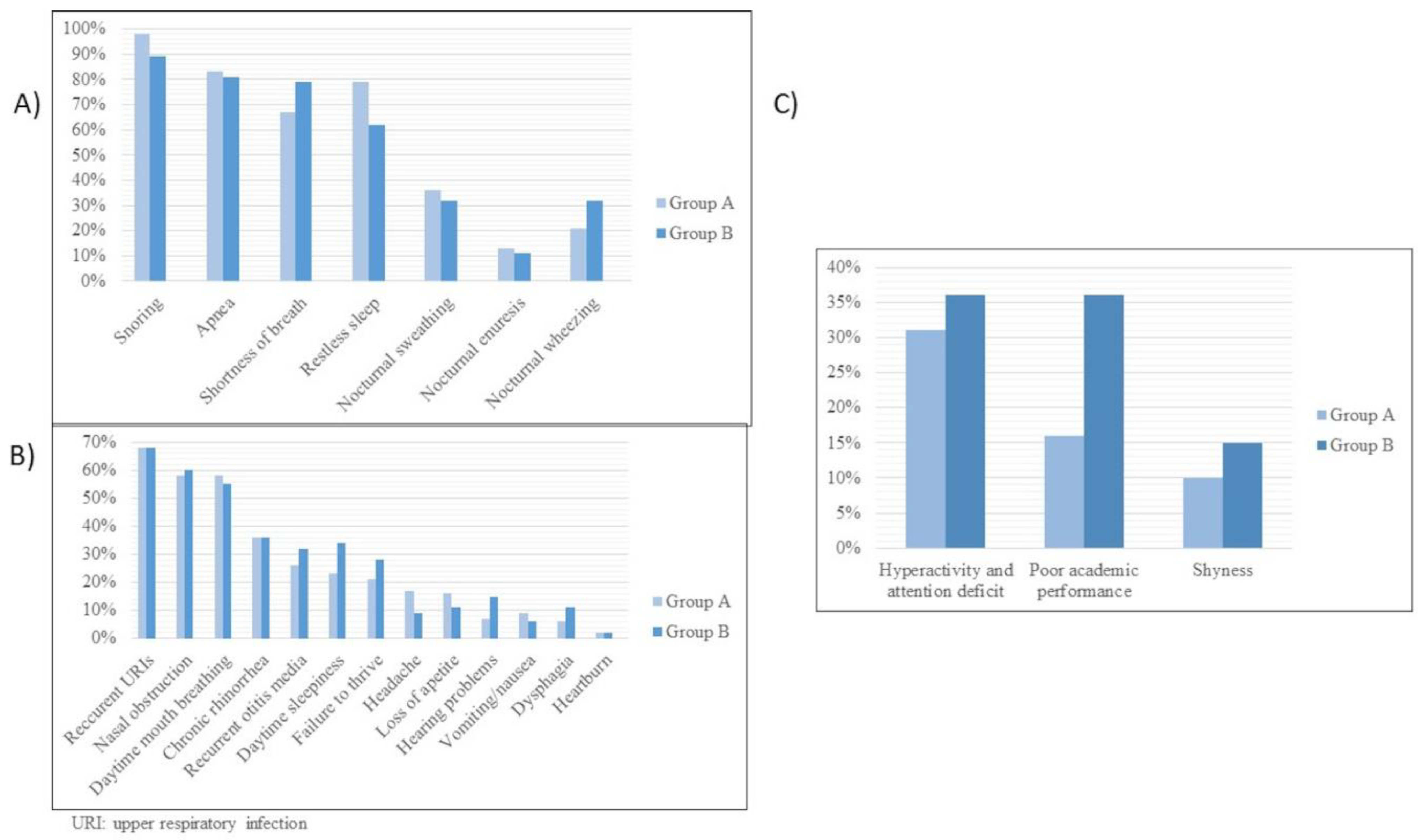
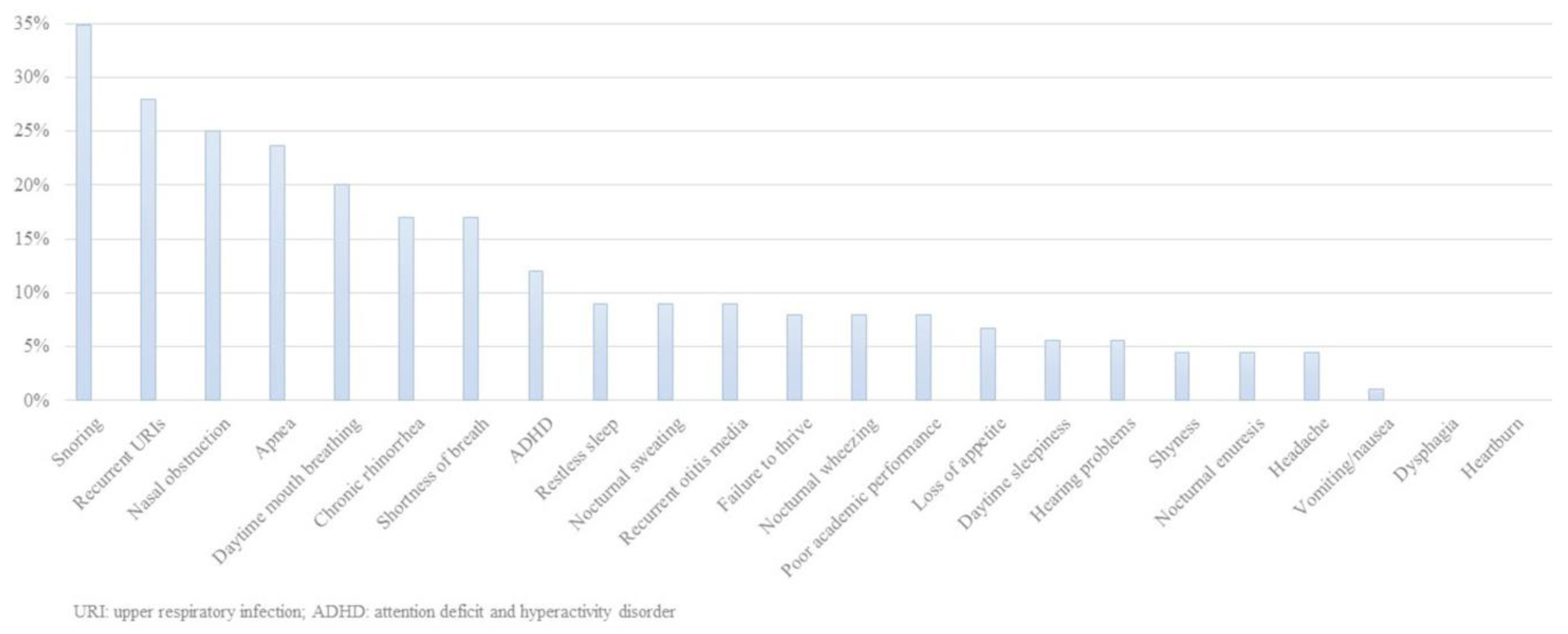
3.2. Clinical Features
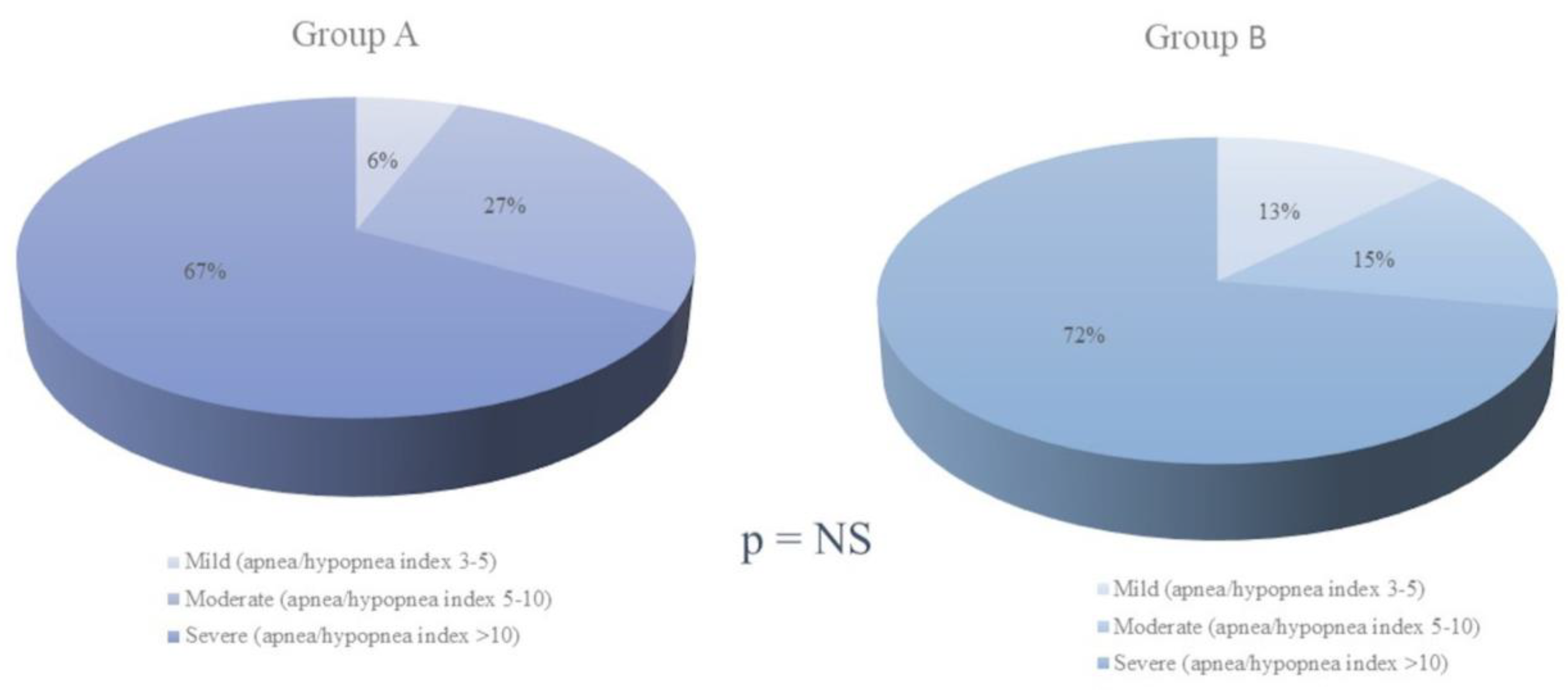
3.3. Polysomnographic Data
3.4. OSA Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hornero, R.; Kheirandish-Gozal, L.; Gutiérrez-Tobal, G.; Philby, M.F.; Alonso-Álvarez, M.L.; Alvarez, D.; Dayyat, E.A.; Xu, Z.; Huang, Y.; Kakazu, M.T.; et al. Consensus document on sleep apnea-hypopnea syndrome in children. Sociedad Española de Sueño. El Área de Sueño de la Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Arch. Bronconeumol. 2011, 47, 2–18. [Google Scholar] [CrossRef]
- Chiner, E.; Sancho-Chust, J.N.; Pérez, P.; Arlandis, M.; Pastor, E.; Martínez-García, M.A. Capítulo 9. SAHS en población infantil. Las amígdalas no son todo. In El Síndrome de Apnea en Poblaciones Especiales; Ed Respira: Barcelona, Spain, 2016; pp. 110–126. [Google Scholar]
- Kaditis, A.G.; Alvarez, M.L.A.; Boudewyns, A.; Abel, F.; Alexopoulos, E.; Ersu, R.; Joosten, K.; Larramona, H.; Miano, S.; Narang, I.; et al. ERS statement on obstructive sleep disordered breathing in 1- to 23-month-old children. Eur. Respir. J. 2017, 50, 1700985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llombart, M.; Chiner, E.; Gómez-Merino, E.; Andreu, A.; Pastor, E.; Senent, C.; Camarasa, A.; Signes-Costa, J. Síndrome de apneas-hipopneas durante el sueño en población infantil: Diferencias en su expresión entre niños con hipertrofia amigdalar y con enfermedad concomitante. Arch. Bronconeumol. 2007, 43, 655–661. [Google Scholar] [CrossRef] [PubMed]
- di Palmo, E.; Filice, E.; Cavallo, A.; Caffarelli, C.; Maltoni, G.; Miniaci, A.; Ricci, G.; Pession, A. Childhood Obesity and Respiratory Diseases: Which Link? Children 2021, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Weihrauch-Blüher, S.; Wiegand, S. Risk Factors and Implications of Childhood Obesit. Curr. Obes. Rep. 2018, 7, 254–259. [Google Scholar] [CrossRef]
- DelRosso, L.; Mogavero, M.; Ferri, R. Effect of Sleep Disorders on Blood Pressure and Hypertension in Children. Curr. Hypertens. Rep. 2020, 22, 88. [Google Scholar] [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Ward, S.D.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Lehmann, C.; Schechter, M.S.; Sheldon, S.; et al. American Academy of Pediatrics. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef] [Green Version]
- Kirk, V.; Baughn, J.; D’Andrea, L.; Friedman, N.; Galion, A.; Garetz, S.; Hassan, F.; Wrede, J.; Harrod, C.G.; Malhotra, R.K. American Academy of Sleep Medicine Position Paper for the Use of Home Sleep Apnea Test for the Diagnosis of OSA in Children. J. Clin. Sleep Med. 2017, 13, 1199–1203. [Google Scholar] [CrossRef]
- Reckley, L.K.; Fernandez-Salvador, C.; Camacho, M. The effect of tonsillectomy on obstructive sleep apnea: An overview of systematic reviews. Nat. Sci. Sleep 2018, 10, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Gozal, D.; Hui-Leng, T.; Kheirandish-Gozal, L. Treatment of Obstructive Sleep Apnea in Children: Handling the Unknown with Precision. J. Clin. Med. 2020, 9, 888. [Google Scholar] [CrossRef] [Green Version]
- Imanguli, M.; Ulualp, S.O. Risk factors for residual obstructive sleep apnea after adenotonsillectomy in children. Laryngoscope 2016, 126, 2624–2629. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; De Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Guilleminault, C.; Li, K.; Khramitsov, A.; Palombini, I.; Pelayo, R. Breathing patterns in pre-pubertal children with sleep disordered breathing. Arch. Pediatr. Adolesc. Med. 2004, 158, 153–161. [Google Scholar] [CrossRef]
- Amr, F.; Shereen, E.; Morsy, A. A Sleep Scoring System Using EEG Combined Spectral and Detrended Fluctuation Analysis Features. J. Biomed. Sci. Eng. 2014, 7. [Google Scholar] [CrossRef] [Green Version]
- Novelli, L.; Ferri, R.; Bruni, O. Sleep classification according to AASM and Rechtschaffen and Kales: Effects on sleep scoring parameters of children and adolescents. J. Sleep Res. 2010, 19, 238–247. [Google Scholar] [CrossRef]
- Rana, M.; August, J.; Levi, J.; Parsi, G.; Motro, M.; DeBassio, W. Alternative approaches to adenotonsillectomy and continuous positive airway pressure (CPAP) for the management of pediatric obstructive sleep apnea (OSA): A review. Sleep Disorders. 2020, 7987208. [Google Scholar] [CrossRef]
- Wu, C.-R.; Tu, Y.-K.; Chuang, L.-P.; Gordon, C.; Chen, N.-H.; Chen, P.-Y.; Hasan, F.; Kurniasari, M.D.; Susanty, S.; Chiu, H.-Y. Diagnostic meta-analysis of the Pediatric Sleep Questionnaire, OSA-18, and pulse oximetry in detecting pediatric obstructive sleep apnea syndrome. Sleep Med. Rev. 2020, 54, 101355. [Google Scholar] [CrossRef] [PubMed]
- Nixon, G.M.; Brouillette, R.T. Sleep. 8: Paediatric obstructive sleep apnoea. Thorax 2005, 60, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nixon, G.M.; Hwang, B.-F.; Lee, Y.-L.; Lin, Y.-C.; Jaakkola, J.J.K.; Guo, Y.L. Evaluation of children with chronic cough including obstructive sleep apnea: A single-center experience. Eur. J. Pediatr. 2019, 178, 189–197. [Google Scholar] [CrossRef]
- Ekici, A.; Ekici, M.; Kurtipek, E.; Keles, H.; Kara, T.; Tunckol, M.; Kocyigit, P. Association of asthma-related symptoms with snoring and apnea and effect on health-related quality of life. Chest 2005, 128, 3358–3363. [Google Scholar] [CrossRef] [Green Version]
- Sulit, L.G.; Storfer-Isser, A.; Rosen, C.L.; Kirchner, H.L.; Redline, S. Associations of obesity, sleep-disordered breathing, and wheezing in children. Am. J. Respir. Crit. Care Med. 2005, 171, 659–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiner, E.; Cánovas, C.; Molina, V.; Sancho-Chust, J.N.; Vañes, S.; Pastor, E.; Martinez-Garcia, M.A. Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome. J. Clin. Med. 2020, 9, 2067. [Google Scholar] [CrossRef] [PubMed]
- Deane, S.; Thomson, A. Obesity and the pulmonologist. Arch. Dis. Child. 2006, 9, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Abijay, C.A.; Tomkies, A.; Rayasam, S.; Johnson, R.F.; Mitchell, R.B. Children with Down Syndrome and Obstructive Sleep Apnea: Outcomes After Tonsillectomy. Otolaryngol. Head Neck. Surg. 2021, 13, 1945998211023102. [Google Scholar] [CrossRef]
- O’Donoghue, F.; Camfferman, D.; Kennedy, J.; Martin, A.; Couper, T.; Lack, L.; Lushington, K.; McEvoy, D. Sleep-disordered breathing in Prader-Willi syndrome and its association with neurobehavioral abnormalities. J. Pediatr. 2005, 147, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, D.; Isaiah, A. Towards Patient-centered Diagnosis of Pediatric Obstructive Sleep Apnea. Review of Biomedical Engineering Strategies. Expert Rev. Med. Devices 2019, 16, 617–629. [Google Scholar] [CrossRef]
- Alonso-Álvarez, M.L.; Terán-Santos, J.; Carbajo, E.O.; Cordero-Guevara, J.A.; Navazo-Egüia, A.I.; Kheirandish-Gozal, L.; Gozal, D. Reliability of home respiratory polygraphy for the diagnosis of sleep apnea in children. Chest 2015, 147, 1020–1028. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.L.; Kheirandish-Gozal, L.; Gozal, D. Pediatric home sleep apnea testing; slowly getting there! Chest 2015, 148, 1382–1395. [Google Scholar] [CrossRef] [Green Version]
- Friedman, M.; Wilson, M.; Lin, H.C.; Chang, H.W. Updated systematic review of tonsi-llectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol. Head Neck. Surg. 2009, 140, 800–808. [Google Scholar] [CrossRef]
- Marcus, C.L.; Rosen, G.; Ward, S.L.D.; Halbower, A.C.; Sterni, L.; Lutz, J.; Stading, P.J.; Bolduc, D.; Gordon, N. Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics 2006, 117, e442–e451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, K.A.; Chawla, J.; Harris, M.A.; Heussler, H.; Black, R.J.; Cheng, A.T. Cognition After Early Tonsillectomy for Mild OSA. Pediatrics 2020, 145, e20191450. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.L.; Kaditis, A.G. Phenotypic variance in pediatric obstructive sleep apnea. Pediatr. Pulmonol. 2021, 56, 1754–1762. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | p Value | |
|---|---|---|---|
| Age (years, mean ± SD) | 6 ± 3 | 9 ± 4 | <0.001 |
| Anthropometric measurements (mean ± SD) | |||
| Weight (kg) | 28 ± 16 | 37 ± 21 | <0.01 |
| Height (cm) | 120 ± 20 | 130 ± 20 | <0.01 |
| BMI (kg/m2) | 18 ± 4 | 20 ± 7 | <0.05 |
| BMI percentile | 66 ± 35 | 68 ± 42 | NS |
| Neck circumference (cm) | 28 ± 4 | 30 ± 5 | <0.05 |
| Predisposing factors (%) | |||
| Tonsillar hypertrophy | 93 | 62 | <0.001 |
| Adenoid hypertrophy | 49 | 43 | NS |
| High-arched palate | 12 | 17 | NS |
| Macroglossia | 1 | 11 | <0.01 |
| Facial abnormalities | 10 | 34 | <0.001 |
| Micrognathism | 3 | 21 | <0.001 |
| Prognathism | 0 | 4 | <0.05 |
| Retrognathia | 8 | 21 | <0.05 |
| Dental malocclusion | 3 | 11 | NS |
| Dolichocephaly | 2 | 11 | <0.01 |
| Obesity | 17 | 30 | <0.05 |
| Previous tonsillectomy | 3 | 11 | <0.05 |
| Group A (Mean ± SD) | Group B (Mean ± SD) | p Value | |
|---|---|---|---|
| Duration of recording (minutes) | 490 ± 64 | 496 ± 62 | NS |
| Sleep efficiency (%) | 87 ± 8 | 85 ± 9 | NS |
| Stage 1 (%) | 13 ± 9 | 14 ± 10 | NS |
| Stage 2 (%) | 30 ± 11 | 30 ± 13 | NS |
| Stages 3 and 4 (%) | 31 ± 14 | 31 ± 19 | NS |
| REM stage (%) | 26 ± 12 | 23 ± 15 | NS |
| Stage 1 latency | 10 ± 23 | 11 ± 35 | NS |
| Stage 2 latency | 12 ± 12 | 8 ± 7 | NS |
| Stage 3 and 4 latency | 138 ± 181 | 200 ± 196 | NS |
| REM stage latency | 70 ± 57 | 56 ± 50 | NS |
| Microarousal index | 14 ± 8 | 21 ± 18 | <0.05 |
| Apnea/hypopnea index | 15 ± 9 | 22 ± 21 | <0.05 |
| Oxygen desaturation index | 7 ± 8 | 16 ± 23 | <0.05 |
| Baseline oxygen saturation (%) | 97 ± 1 | 95 ± 4 | <0.01 |
| Minimum oxygen saturation (%) | 79 ± 13 | 74 ± 17 | <0.05 |
| CT90 (%) | 4 ± 10 | 12 ± 20 | <0.05 |
| Before Treatment (Mean ± SD) | After Treatment (Mean ± SD) | p Value | |
|---|---|---|---|
| Group A | |||
| Weight (kg) | 27 ± 13 | 31 ± 14 | <0.001 |
| Height (cm) | 1.0 ± 0.2 | 1.2 ± 0.2 | <0.001 |
| BMI (kg/m2) | 18 ± 4 | 19 ± 4 | <0.01 |
| Neck circumference (cm) | 28 ± 3 | 29 ± 3 | <0.001 |
| Apnea/hypopnea index | 17 ± 9 | 8 ± 7 | <0.001 |
| Oxygen desaturation index | 7 ± 9 | 3.7 ± 4 | <0.01 |
| Baseline oxygen saturation | 97 ± 2 | 97 ± 1 | <0.05 |
| Minimum oxygen saturation | 79 ± 15 | 83 ± 14 | NS |
| CT90 (%) | 4 ± 6 | 7 ± 19 | NS |
| Group B | |||
| Weight (kg) | 34 ± 16 | 36 ± 16 | <0.01 |
| Height (cm) | 1.2 ± 0.2 | 1.3 ± 0.2 | <0.01 |
| BMI (kg/m2) | 20 ± 5 | 20 ± 5 | NS |
| Neck circumference (cm) | 29 ± 5 | 30 ± 5 | <0.05 |
| Apnea/hypopnea index | 23 ± 19 | 12 ± 15 | <0.05 |
| Oxygen desaturation index | 21 ± 24 | 7 ± 10 | <0.05 |
| Baseline oxygen saturation | 94 ± 4 | 96 ± 2 | <0.05 |
| Minimum oxygen saturation | 71 ± 17 | 76 ± 14 | NS |
| CT90 (%) | 16 ± 21 | 7 ± 10 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiner, E.; Sancho-Chust, J.N.; Pastor, E.; Esteban, V.; Boira, I.; Castelló, C.; Celis, C.; Vañes, S.; Torba, A. Features of Obstructive Sleep Apnea in Children with and without Comorbidities. J. Clin. Med. 2023, 12, 2418. https://doi.org/10.3390/jcm12062418
Chiner E, Sancho-Chust JN, Pastor E, Esteban V, Boira I, Castelló C, Celis C, Vañes S, Torba A. Features of Obstructive Sleep Apnea in Children with and without Comorbidities. Journal of Clinical Medicine. 2023; 12(6):2418. https://doi.org/10.3390/jcm12062418
Chicago/Turabian StyleChiner, Eusebi, Jose N. Sancho-Chust, Esther Pastor, Violeta Esteban, Ignacio Boira, Carmen Castelló, Carly Celis, Sandra Vañes, and Anastasiya Torba. 2023. "Features of Obstructive Sleep Apnea in Children with and without Comorbidities" Journal of Clinical Medicine 12, no. 6: 2418. https://doi.org/10.3390/jcm12062418