1. Introduction
First described by von Graefe in 1866, central serous chorioretinopathy (CSCR) is a disease characterized by a serous neurosensory retinal detachment due to choriocapillaris leakage [
1,
2,
3,
4]. The vast majority of cases of CSCR resolve spontaneously, usually within 3 to 6 months [
5,
6,
7]. However, there is a minority of patients that progress to chronic CSCR, which is often complicated by progressive retinal pigment epithelium (RPE) atrophy, bullous retinal detachment, and choroidal neovascularization (CNV). These sequelae (particularly CNV) offer a poor visual prognosis for patients. Conventionally, the incidence of CNV was estimated to be from 2–18% [
7,
8]. Investigations examining chronic CSCR patients found that roughly one-third will go on to develop CNV [
9,
10]. The advent of optical coherence tomography angiography (OCTA) has demonstrated an incidence closer to 30% [
11]. This is likely due to the increased sensitivity and specificity of OCTA relative to fluorescein angiography and its overall convenience as a non-invasive imaging modality [
11,
12].
OCTA alone, however, may not be sufficient in detecting all cases of CNV in patients with CSCR [
13]. Multimodal imaging often serves as the most comprehensive approach in detecting and characterizing neovascularization in patients with CSCR. The pathophysiologic mechanism for the development of CNV in patients with CSCR is postulated to involve decompensation of the RPE with subsequent disruption of Bruch’s membrane; reminiscent of the proposed mechanism in age-related macular degeneration (ARMD) [
4,
11,
14,
15,
16]. Previously, CNV associated with CSCR has been characterized broadly as a downstream sequela of the disease, with the assumption that all CNV associated with CSCR are similar in their presentation, prognosis, and effective treatment. Some studies have investigated long-term outcomes in patients with CSCR, finding that the majority of patients develop a Type I CNVM, with roughly 69 to 80% requiring either anti-VEGF or PDT [
17,
18,
19].
Our group has recently published a revised classification that functions to standardize the terminology surrounding CSCR, allowing for more nuanced explorations into the diagnosis, management, and prognosis of the disease [
16]. Our classification begins with classifying cases as simple, complex, and atypical based principally on RPE morphology. Simple and complex are differentiated by a size threshold of 2-disc diameters of clinically detectable retinal pigment epitheliopathy. Atypical cases served to include those cases of CSCR in which other retinal pathologies were also present as well as bullous CSCR. In order to further standardize the time course of CSCR, simple and complex cases were further reclassified, based on clinical course, as primary, recurrent, or resolved, and subsequently qualified as a persistent subtype [
20].
Given the poor visual prognosis of patients with CSCR complicated by neovascularization, it is of particular clinical interest to stratify the risk of CNV development in patients with CSCR [
4,
5,
7,
14]. The purpose of this investigation is to establish the incidence of CNV development in relation to our recently described classification system and treatment outcome at one-year follow up for CNV associated with CSCR based on multimodal imaging
2. Materials and Methods
This was a retrospective, multicenter study on patients with a known diagnosis of CSCR. The study adhered to the tenets of the Declaration of Helsinki and ethical clearance was obtained by the Institutional Review Board. Informed consent was obtained from all patients.
Retrospective data were gathered from the Departments of Ophthalmology across multiple centers in the U.S., Italy, India, and Russia from 2015–2020. The charts of all patients with a diagnosis of CSCR were evaluated. Subsequent inclusion criteria were imposed, including (i) availability of demographic, clinical and reliable treatment details; (ii) availability of good quality multimodal imaging including fundus autofluorescence (FAF), spectral domain optical coherence tomography (SD OCT) (B scan), and OCTA or fundus fluorescein angiography (FFA) with indocyanine angiography (ICGA). Importantly, image quality on OCT and OCTA must have exceeded a signal strength of 7/10. With regard to angiographic imaging, patients must have had a full sequence of early, middle, and late phases without motion or lid artifacts. Exclusion criteria included were (i) any other retinal disease such as ARMD or any other cause of macular neovascularization, and (ii) poor quality imaging as discussed earlier.
Baseline data collected from patients included age, sex, best corrected visual acuity (BCVA), duration of complaints, reliable history of any previous such episodes, previous retinal treatment, or steroid use.
FAF, fundus photographs, FFA, and ICGA were obtained from Spectralis HRA + OCT (Heidelberg Engineering, Heidelberg, Germany) or F-10 scanning laser ophthalmoscope (NIDEK, Gamagori, Japan). OCTA examinations were performed with the RTVue-XR Avanti (Optovue, Fremont, CA, USA) or Spectralis HRA + OCT. For each eye, horizontal raster pattern scan through the center of the macula was obtained. OCTA examination including a 6 × 6 mm (2 orthogonal volumes with 400 × 400 A scans) pattern centered in the center of the fovea was performed with RTVue-XR Avanti.
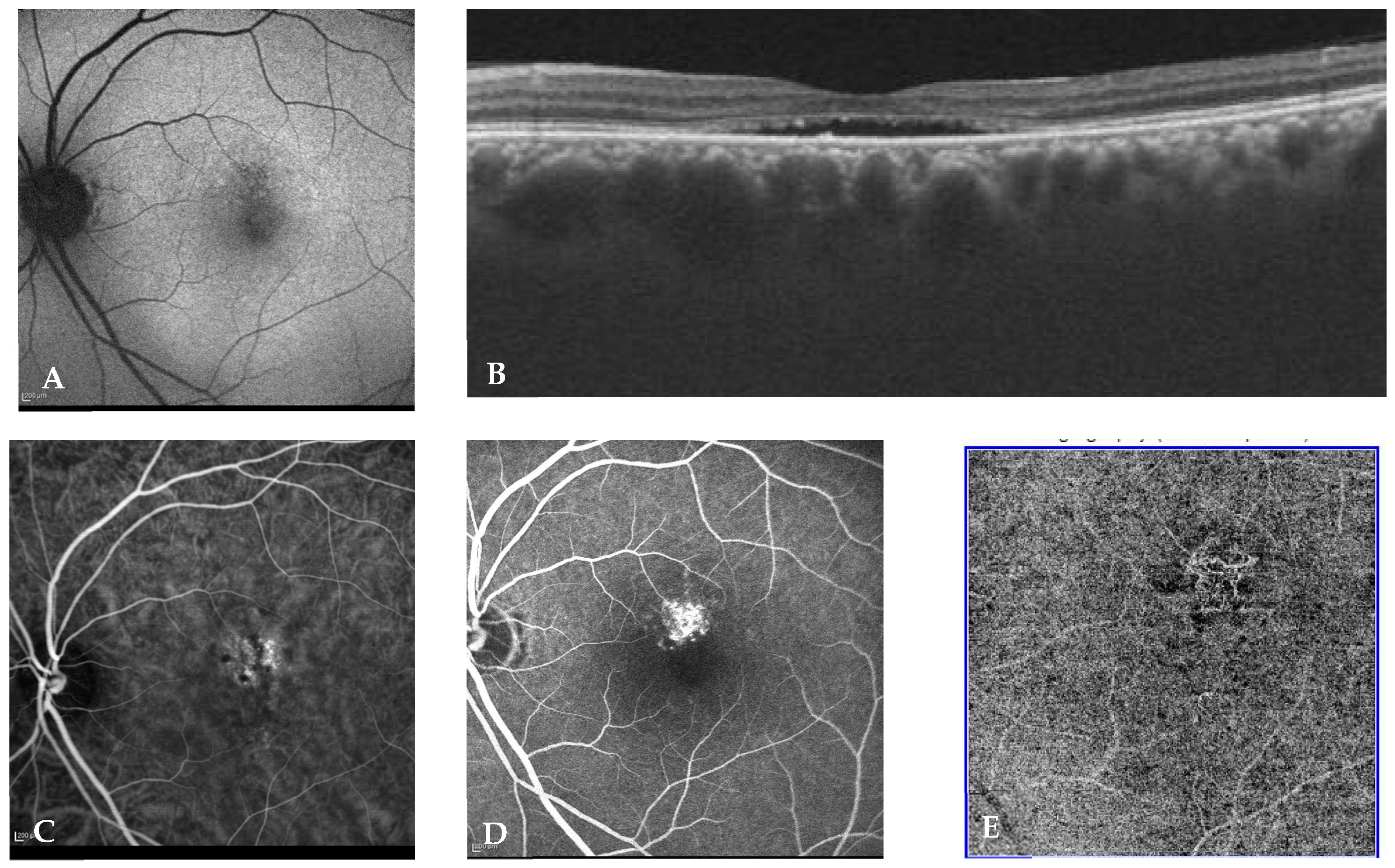
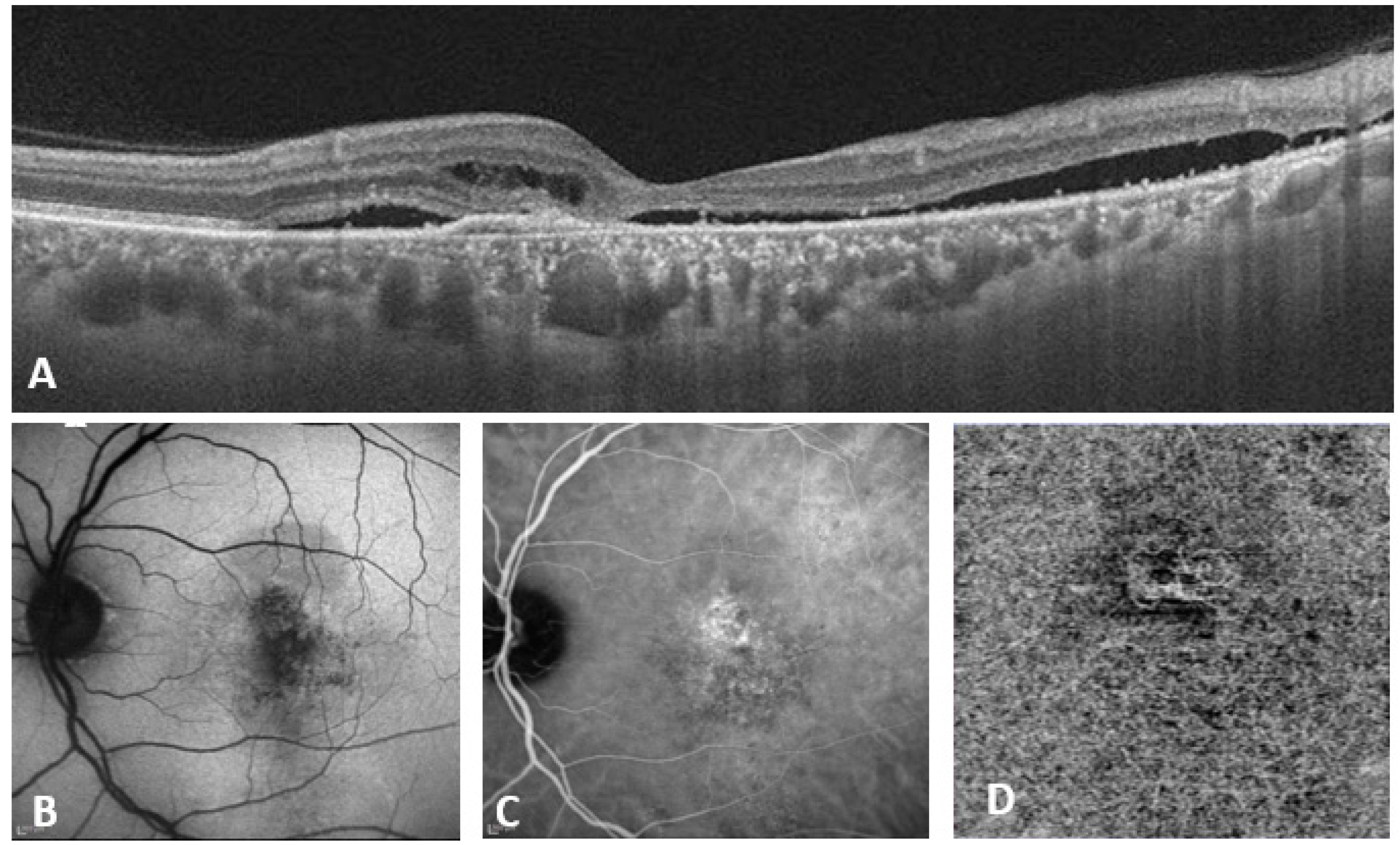
Double blind classification was performed by two retinal experts [SA and DM] as per the new multimodal imaging-based classification system of CSCR. In cases of non-consensus, senior investigator (JC) was consulted. All images were made available by SC for all graders with images deidentified and randomly assigned by numeric generator to either expert. Eyes were classified as per the multimodal imaging-based classification of CSCR at baseline into (i) simple/complex CSCR, (ii) primary episode/recurrent/resolved CSCR, (iii) persistent SRF (>6 months) or not, (iv) outer retinal atrophy (ORA) presence or absence, (v) foveal involvement presence or absence, (vi) CNV presence or absence. Representative cases of simple and complex CSCR are illustrated in
Figure 1 and
Figure 2, respectively.
All patients selected by the above criteria were classified as previously published by our group [
20]. Parameters evaluated at baseline, 3 months, 6 months, and 12 months included BCVA, subfoveal choroidal thickness (SFCT), and central macular thickness (CMT). Presence of CNV and treatment instituted for each of the above time intervals was also noted. Statistical analysis, including baseline characteristics of CNV and predictors, were evaluated with one-way analysis of variance (ANOVA), chi-square test, and odds ratio calculation via Microsoft Excel.
3. Results
Included in this analysis were 134 eyes from 132 patients with six eyes having non-consensus requiring consultation of senior investigator JC. The median age of patients was 48 years (range: 23–67). There was a strong male gender predisposition with 84.6% being male. Seven eyes had previous histories of treatment at presentation: five eyes with focal laser, one eye with photodynamic therapy (PDT), and one patient on Eplerenone.
Of the 134 eyes with CSCR, CNV was present in 32.8% (
n = 44), and demographic data for this group is summarized in
Table 1. Of all patients with CNV, 15% were detected primarily by OCT-A, though ICG-A and FA showed suspicious lesions. Of the 44 patients with CNV, 32 had complex CSCR (72.7%), 10 had simple CSCR (22.7%), and 2 had atypical CSCR (4.5%). Demographic breakdown and visual acuity per each CSCR subtype in patients with CNV is summarized in
Table 2. Among the 90 patients without CNV, 50 had simple CSCR (55.6%) and 40 had complex CSCR (44.4%). There was no statistically significant difference in the prevalence of simple CSCR between patients with CNV and those without (
p = 0.08). Patients with complex CSCR were 2.72 times more likely to have CNV than patients with simple CSCR (95% CI 1.199 to 6.166;
p = 0.016).
Table 3 summarizes the incidence of CNV among CSCR subtypes.
Patients with simple CSCR with CNV had better baseline BCVA than those with complex CSCR (0.72 vs. 0.49, p = 0.03) without differences in age (mean 59 vs. 59 years, p = 0.76), SFCT 393 vs. 390 μm, (p = 0.997), and reported duration of symptoms (median 6 vs. 18 weeks, p = 0.38).
Based on presentation, there was an equal incidence of CNV in both primary and recurrent cases (
n = 20, 45.5% each) with the remainder of CNV found in resolved cases (9.1%,
n = 4). Data is summarized in
Table 4. There was no age-related, statistically significant difference between primary, recurrent, and resolved cohorts, with the mean age being 58 ± 10.8, 61 ± 9.8, and 62 ± 10.8, respectively (
p = 0.27). BCVA was also not statistically significantly different among primary, recurrent, and resolved cases of CSCR with mean BCVA Snellen equivalent(logMAR) of 20/73 (0.56, standard deviation [SD] 0.29), 20/63 (0.50, SD 0.31) and 20/89 (0.65, SD 0.33), respectively (
p = 0.66). Demographic and visual acuity data are summarized in
Table 3. SFCT did not differ among these cohort as well with their mean values as 414 ± SD, 383 ± SD, and 329 ± SD μ, respectively (
p = 0.55). Differences in overall duration among the three cohorts were not statistically significant with median values of 7 and 30 months, respectively (
p = 0.42). A summary of duration in months across various sub-groups is listed in
Table 5.
In comparing patients with primary CSCR with CNV to those without CNV, the mean age was 58 years (SD 10 years) as compared to 47 years (SD 10 years) with a p-value of 0.00003. The mean BCVA logMAR (Snellen fraction) was 0.75 (20/112) as compared to 0.56 (20/73) with a p-value of 0.01. The average duration was 7 months as compared to 1 month (p = 0.0002).
When comparing patients with recurrent CSCR with CNV to those without, there was no statistically significant difference in mean logMAR BCVA (0.50 vs. 0.61, p = 0.31), duration (median 7 vs. 2 months, p = 0.32), and mean SFCT (383 ± 75 vs. 424 ± 85 μm, p = 0.21). An exception to this trend of similarity between the two groups is in the mean age of presentation, which was 60.7-years-old in patients with recurrent CSCR with CNV and 52-years-old in recurrent CSCR patients without CNV (p = 0.003).
Forty-three out of the forty-four patients with CNV had foveal involvement, compared to the eighty-five out of ninety patients without CNV, which was not statistically significant (p = 0.38). In comparing foveal involvement between patients with CNV and patients without CNV, there was no statistically significant difference. Regarding ORA, among all CSCR patients with CNV, 36 (78%) had ORA as opposed to 29 (32%) among CSCR patients without CNV (p < 0.01).
4. Discussion
Our investigation yields several key risk factors for the development of CNV in patients with CSCR. Patients with complex CSCR were at a significantly higher risk for CNV with an odds ratio of 2.72. In both primary and recurrent CSCR, there was a significant difference in age of presentation when comparing patients that developed CNV with those who did not. Specifically, in both primary and complex CSCR, older patients were more likely to develop CNV. Our data also intuitively demonstrate that primary CSCR patients with CNV are predisposed to longer courses when compared to patients without CNV. The relative higher incidence of CNV in patients with primary CSCR compared to prior published data implies that a lower threshold should exist for use of OCTA or FA to evaluate for CNV in CSCR patients with SRF on initial presentation. Counterintuitively, our data did not support statistically significant differences in duration of disease course between primary, recurrent and atypical CSCR. This finding supports the idea that recurrence functions as a secondary measure more so than a primary prognostic measure.
The positive correlation between age upon presentation and the incidence of CNV can serve as an important determinant of pre-test probability for the development of CNV when evaluating patients with CSCR on initial work-up. These findings are in line with other studies of CSCR which found older patients with higher incidence of CNV and worse visual acuity [
7,
21].
Multimodal imaging-based classification provides objective approach to associate disease severity with CNV formation and progression. More broadly, increased CNV in patients with complex CSCR when taken in conjunction with our findings of increased ORA in patients with CNV, reinforce the notion of complex CSCR as retinal pigment epitheliopathy. The co-occurrence of ORA with CNV has been validated by other groups as well [
22]. The importance of the association between CNV and complex CSCR has several important implications beyond elucidation of underlying pathophysiology. In the affected eye, CNV has been shown previously to be associated with cystoid macular degeneration, a marker of progressive CSCR damage [
15]. Given that CSCR has been frequently demonstrated to progress to bilateral disease, it is reasonable that in patients with unilateral neovascular CSCR, there is a risk of CNV secondary to CSCR in the fellow eye. Previously published work by our group has shown that the fellow eye in patients with unilateral CSCR complicated by CNV can have early signs of neovascularization as detected by OCTA [
14].
CSCR often takes an uncomplicated, self-resolving course, however, in patients in which this does not occur, morbidity and visual prognosis can be poor. Our data point towards a model of CSCR management in which early classification can allow for appropriate risk stratification with regard to the development of CNV and consequently appropriate screening via multi-modal imaging. The rise of OCTA, taken together with ICGA, FFA, and OCT allow for a layered approach to the early diagnosis of CNV in both the affected eye and the fellow eye, with early treatment mitigating complications of long-standing CSCR such as cystoid macular degeneration.
While our study provides nuance to the progression and prognosis of patients with CNV, it is limited by a relatively small sample size and retrospective nature. Studies of CSCR are often limited by the relatively low incidence. Our study’s retrospective nature precludes an ability to assess patients at a long-term follow-up. This can create bias in the data towards patients that may develop CNV later in their course. Additionally, while efforts were made to ensure randomization of patient images for classification, the retrospective nature of this study provides an inherent limitation to the completeness of randomization. It is also important to note that CSCR with CNV is often confounded by the presence of pachychoroid neovasculopathy; this element may confound interpretation of patient presentation.
The investigation and subsequent data presented tie our previously published classification system to objective, discrete outcomes in patients with CSCR, specifically, the development of CNV. Age upon presentation and complex CSCR phenotype serve as early prognostic indicators to the development of CNV and consequently poorer visual outcomes. The importance of these findings is their purported role in driving more targeted treatment for patients with CSCR. Further studies will be conducted to prospectively evaluate patients’ treatment response and to further explore the relative distribution of different types of CNV across different CSCR classifications.
Author Contributions
For conceptualization, S.C., J.C. and T.S. For data curation, resources and methodology, S.A., D.S.M., S.R.S., N.K.S., D.P., A.N.K., C.I., F.T., R.G., R.V., N.G.R., R.S., E.P. and M.L. For data analysis, S.C., J.C. and T.S. For Writing—original draft S.C. For writing—review and editing S.C., J.C. and S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhao, M.; Celerier, I.; Bousquet, E.; Jeanny, J.C.; Jonet, L.; Savoldelli, M.; Offret, O.; Curan, A.; Farman, N.; Jaisser, F.; et al. Mineralocorticoid receptor is involved in rat and human ocular chorioretinopathy. J. Clin. Investig. 2012, 122, 2672–2679. [Google Scholar] [CrossRef]
- Michael, J.C.; Pak, J.; Pulido, J.; de Venecia, G. Central serous chorioretinopathy associated with administration of sympathomimetic agents. Am. J. Ophthalmol. 2003, 136, 182–185. [Google Scholar] [CrossRef]
- Reiner, A.; Fitzgerald, M.E.C.; Del Mar, N.; Li, C. Neural control of choroidal blood flow. Prog. Retin. Eye Res. 2018, 64, 96–130. [Google Scholar] [CrossRef]
- Chhablani, J. Central Serous Chorioretinopathy; Academic Press: Cambridge, MA, USA, 2019; p. 662. [Google Scholar]
- Liegl, R.; Ulbig, M.W. Central serous chorioretinopathy. Ophthalmologica 2014, 232, 65–76. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Munch, I.C.; Hasler, P.W.; Prunte, C.; Larsen, M. Central serous chorioretinopathy. Acta Ophthalmol. 2008, 86, 126–145. [Google Scholar] [CrossRef]
- Spaide, R.F.; Campeas, L.; Haas, A.; Yannuzzi, L.A.; Fisher, Y.L.; Guyer, D.R.; Slakter, J.S.; Sorenson, J.A.; Orlock, D.A. Central serous chorioretinopathy in younger and older adults. Ophthalmology 1996, 103, 2070–2080. [Google Scholar] [CrossRef]
- Loo, R.H.; Scott, I.U.; Flynn, H.W., Jr.; Gass, J.D.; Murray, T.G.; Lewis, M.L.; Rosenfeld, P.J.; Smiddy, W.E. Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina 2002, 22, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Savastano, M.C.; Rispoli, M.; Lumbroso, B. The Incidence of Neovascularization in Central Serous Chorioretinopathy by Optical Coherence Tomography Angiography. Retina 2021, 41, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sulzbacher, F.; Schutze, C.; Burgmuller, M.; Vecsei-Marlovits, P.V.; Weingessel, B. Clinical evaluation of neovascular and non-neovascular chronic central serous chorioretinopathy (CSC) diagnosed by swept source optical coherence tomography angiography (SS OCTA). Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1581–1590. [Google Scholar] [CrossRef]
- Bonini Filho, M.A.; de Carlo, T.E.; Ferrara, D.; Adhi, M.; Baumal, C.R.; Witkin, A.J.; Reichel, E.; Duker, J.S.; Waheed, N.K. Association of Choroidal Neovascularization and Central Serous Chorioretinopathy With Optical Coherence Tomography Angiography. JAMA Ophthalmol. 2015, 133, 899–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, R.; Dogra, M.; Mulkutkar, S.; Katoch, D.; Singh, R.; Gupta, V.; Dogra, M.R.; Gupta, A. Optical coherence tomography angiography versus fluorescein angiography in diagnosing choroidal neovascularization in chronic central serous chorioretinopathy. Indian J. Ophthalmol. 2019, 67, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.S.; Ho, M.; Chen, L.J.; Yip, F.L.; Teh, W.M.; Zhou, L.; Mohamed, S.; Tsang, C.W.; Brelen, M.E.; Chen, H.; et al. Optical Coherence Tomography Angiography Compared with Multimodal Imaging for Diagnosing Neovascular Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2021, 232, 70–82. [Google Scholar] [CrossRef]
- Mandadi, S.K.R.; Singh, S.R.; Sahoo, N.K.; Mishra, S.B.; Sacconi, R.; Iovino, C.; Berger, L.; Munk, M.R.; Querques, G.; Peiretti, E.; et al. Optical coherence tomography angiography findings in fellow eyes of choroidal neovascularisation associated with central serous chorioretinopathy. Br. J. Ophthalmol. 2021, 105, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, N.K.; Mishra, S.B.; Iovino, C.; Singh, S.R.; Munk, M.R.; Berger, L.; Peiretti, E.; Chhablani, J. Optical coherence tomography angiography findings in cystoid macular degeneration associated with central serous chorioretinopathy. Br. J. Ophthalmol. 2019, 103, 1615–1618. [Google Scholar] [CrossRef]
- Chhablani, J.; Cohen, F.B.; Aymard, P.; Beydoun, T.; Bousquet, E.; Daruich-Matet, A.; Zweifel, S. Multimodal Imaging-Based Central Serous Chorioretinopathy Classification. Ophthalmol. Retin. 2020, 4, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Hagag, A.M.; Chandra, S.; Khalid, H.; Lamin, A.; Keane, P.A.; Lotery, A.J.; Sivaprasad, S. Multimodal Imaging in the Management of Choroidal Neovascularization Secondary to Central Serous Chorioretinopathy. J. Clin. Med. 2020, 9, 1934. [Google Scholar] [CrossRef]
- Moussa, M.; Leila, M.; Khalid, H.; Lolah, M. Detection of Silent Type I Choroidal Neovascular Membrane in Chronic Central Serous Chorioretinopathy Using En Face Swept-Source Optical Coherence Tomography Angiography. J. Ophthalmol. 2017, 2017, 6913980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.Y.; Ma, G.J.; Park, W.K.; Kim, M.; Park, Y.G.; Park, Y.H. Clinical course after the onset of choroidal neovascularization in eyes with central serous chorioretinopathy. Medicine 2021, 100, e26980. [Google Scholar] [CrossRef]
- Arora, S.; Kulikov, A.N.; Maltsev, D.S. Implementation of the new multimodal imaging-based classification of central serous chorioretinopathy. Eur. J. Ophthalmol. 2021, 32, 1044–1049. [Google Scholar] [CrossRef]
- Zhou, X.; Komuku, Y.; Araki, T.; Terasaki, H.; Miki, A.; Kuwayama, S.; Nishi, T.; Kinoshita, T.; Gomi, F. Risk factors and characteristics of central serous chorioretinopathy with later development of macular neovascularisation detected on OCT angiography: A retrospective multicentre observational study. BMJ Open Ophthalmol. 2022, 7, e000976. [Google Scholar] [CrossRef]
- Borrelli, E.; Battista, M.; Sacconi, R.; Gelormini, F.; Querques, L.; Grosso, D.; Vella, G.; Bandello, F.; Querques, G. OCT Risk Factors for 3-Year Development of Macular Complications in Eyes With “Resolved” Chronic Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2021, 223, 129–139. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}