
Evaluation of Retinal Nerve Fiber Layer and Macular Ganglion Cell Layer Thickness in Relation to Optic Disc Size

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
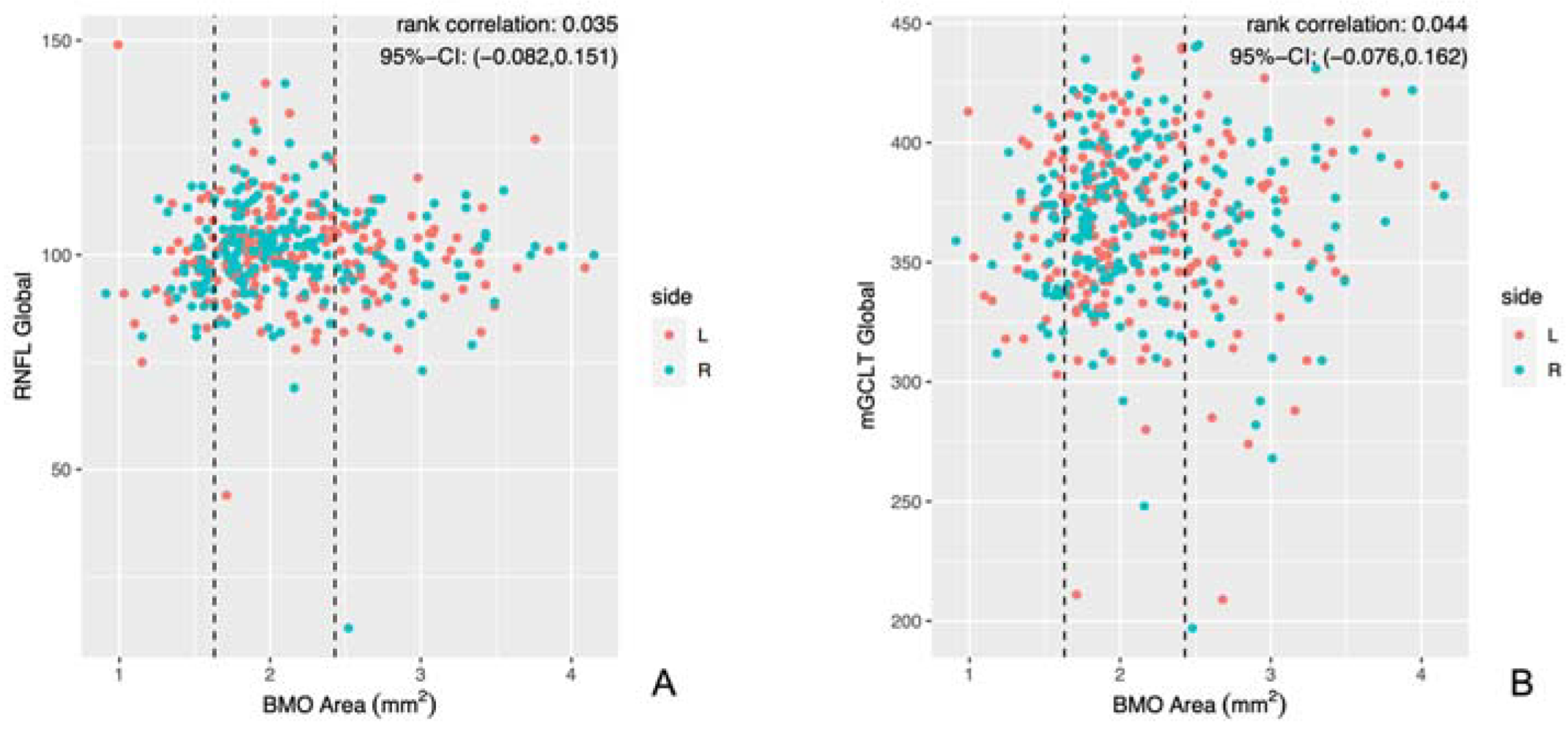
3.1. Correlation Analysis
3.2. Optic Disc Groups (HRT Division)
3.3. Optic Disc Groups (Quantile Division)
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, H.; De Boer, J.F.; Chen, T.C. Diagnostic capability of spectral-domain optical coherence tomography for glaucoma. Am. J. Ophthalmol. 2012, 153, 815–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasia, F.F.; El-Dairi, M.; Freedman, S.F.; Rajani, A.; Asrani, S. Reproducibility of spectral-domain optical coherence tomography measurements in adult and pediatric glaucoma. J. Glaucoma 2015, 24, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kim, S.H.; Kim, T.W.; Park, K.H.; Kim, D.M. Reproducibility of retinal nerve fiber thickness measurements using the test-retest function of spectral OCT/SLO in normal and glaucomatous eyes. J. Glaucoma 2010, 19, 637–642. [Google Scholar] [CrossRef]
- Hood, D.C.; Raza, A.S.; de Moraes, C.G.; Liebmann, J.M.; Ritch, R. Glaucomatous damage of the macula. Prog. Retin. Eye Res. 2013, 32, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Na, J.H.; Sung, K.R.; Baek, S.; Kim, Y.J.; Durbin, M.K.; Lee, H.J.; Kim, H.K.; Sohn, Y.H. Detection of glaucoma progression by assessment of segmented macular thickness data obtained using spectral domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3817–3826. [Google Scholar] [CrossRef]
- Iverson, S.M.; Feuer, W.J.; Shi, W.; Greenfield, D.S. Advanced Imaging for Glaucoma Study Group. Frequency of abnormal retinal nerve fibre layer and ganglion cell layer SDOCT scans in healthy eyes and glaucoma suspects in a prospective longitudinal study. Br. J. Ophthalmol. 2014, 98, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, S.K.; Boey, P.Y.; Yang, H.; Fortune, B.; Burgoyne, C.F.; Demirel, S. Structural Measurements for Monitoring Change in Glaucoma: Comparing Retinal Nerve Fiber Layer Thickness with Minimum Rim Width and Area. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6886–6891. [Google Scholar] [CrossRef]
- Schild, A.M.; Ristau, T.; Fricke, J.; Neugebauer, A.; Kirchhof, B.; Sadda, S.R.; Liakopoulos, S. SDOCT thickness measurements of various retinal layers in patients with autosomal dominant optic atrophy due to OPA1 mutations. Biomed. Res. Int. 2013, 2013, 121398. [Google Scholar] [CrossRef] [Green Version]
- Jonas, J.B.; Schmidt, A.M.; Müller-Bergh, J.A.; Schlötzer-Schrehardt, U.M.; Naumann, G.O. Human optic nerve fiber count and optic disc size. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2012–2018. [Google Scholar]
- Seo, S.; Lee, C.E.; Jeong, J.H.; Park, K.H.; Kim, D.M.; Jeoung, J.W. Ganglion cell-inner plexiform layer and retinal nerve fiber layer thickness according to myopia and optic disc area: A quantitative and three-dimensional analysis. BMC Ophthalmol. 2017, 17, 22. [Google Scholar] [CrossRef] [Green Version]
- Savini, G.; Zanini, M.; Carelli, V.; Sadun, A.A.; Ross-Cisneros, F.N.; Barboni, P. Correlation between retinal nerve fibre layer thickness and optic nerve head size: An optical coherence tomography study. Br. J. Ophthalmol. 2005, 89, 489–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resch, H.; Deak, G.; Vass, C. Influence of optic-disc size on parameters of retinal nerve fibre analysis as measured using GDx VCC and ECC in healthy subjects. Br. J. Ophthalmol. 2010, 94, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Chopra, V.; Lu, A.T.; Tan, O.; Francis, B.; Varma, R. Advanced Imaging for Glaucoma Study-AIGS Group: Does optic nerve head size variation affect circumpapillary retinal nerve fiber layer thickness measurement by optical coherence tomography? Investig. Ophthalmol. Vis. Sci. 2012, 53, 4990–4997. [Google Scholar] [CrossRef] [Green Version]
- Arnold, A.C. Pathogenesis of nonarteritic anterior ischemic optic neuropathy. J. Neuroophthalmol. 2003, 23, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Cazana, I.M.; Böhringer, D.; Reinhard, T.; Evers, C.; Engesser, D.; Anton, A.; Lübke, J. A comparison of optic disc area measured by confocal scanning laser tomography versus Bruch’s membrane opening area measured using optical coherence tomography. BMC Ophthalmol. 2021, 21, 31. [Google Scholar] [CrossRef]
- Enders, P.; Adler, W.; Schaub, F.; Hermann, M.M.; Dietlein, T.; Cursiefen, C.; Heindl, L.M. Novel Bruch’s Membrane Opening Minimum Rim Area Equalizes Disc Size Dependency and Offers High Diagnostic Power for Glaucoma. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6596–6603. [Google Scholar] [CrossRef] [Green Version]
- Reis, A.S.; Sharpe, G.P.; Yang, H.; Nicolela, M.T.; Burgoyne, C.F.; Chauhan, B.C. Optic disc margin anatomy in patients with glaucoma and normal controls with spectral domain optical coherence tomography. Ophthalmology 2012, 119, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Rosner, B.; Glynn, R.J. Interval estimation for rank correlation coefficients based on the probit transformation with extension to measurement error correction of correlated ranked data. Stat. Med. 2007, 26, 633–646. [Google Scholar] [CrossRef]
- Rosner, B.; Glynn, R.J.; Lee, M.L. Extension of the rank sum test for clustered data: Two-group comparisons with group membership defined at the subunit level. Biometrics 2006, 62, 1251–1259. [Google Scholar] [CrossRef]
- Jiang, Y.; Lee, M.-L.T.; He, X.; Rosner, B.; Yan, J. Wilcoxon Rank-Based Tests for Clustered Data with R Package clusrank. J. Stat. Softw. 2020, 96, 1–26. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: https://www.R-project.org/ (accessed on 5 October 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2.tidyverse.org/ (accessed on 5 October 2022).
- Mahmoudinezhad, G.; Mohammadzadeh, V.; Martinyan, J.; Edalati, K.; Zhou, B.; Yalzadeh, D.; Amini, N.; Caprioli, J.; Nouri-Mahdavi, K. Comparison of Ganglion Cell Layer and Ganglion Cell/Inner Plexiform Layer Measures for Detection of Early Glaucoma. Ophthalmol. Glaucoma 2023, 6, 58–67. [Google Scholar] [CrossRef]
- Peng, P.H.; Lin, H.S. Retinal nerve fiber layer thickness measured by optical coherence tomography in non-glaucomatous Taiwanese. J. Formos. Med. Assoc. 2008, 107, 627–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, J.H.; Lee, S.Y. The effects of optic disc factors on retinal nerve fiber layer thickness measurement in children. Korean J. Ophthalmol. 2008, 22, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampougeris, G.; Spyropoulos, D.; Mitropoulou, A.; Zografou, A.; Kosmides, P. Peripapillary retinal nerve fibre layer thickness measurement with SD-OCT in normal and glaucomatous eyes: Distribution and correlation with age. Int. J. Ophthalmol. 2013, 6, 662–665. [Google Scholar] [CrossRef]
- Yoo, Y.C.; Lee, C.M.; Park, J.H. Changes in peripapillary retinal nerve fiber layer distribution by axial length. Optom. Vis. Sci. 2012, 89, 4–11. [Google Scholar] [CrossRef]
- Leung, C.K.; Mohamed, S.; Leung, K.S.; Cheung, C.Y.; Chan, S.L.; Cheng, D.K.; Lee, A.K.; Leung, G.Y.; Rao, S.K.; Lam, D.S. Retinal nerve fiber layer measurements in myopia: An optical coherence tomography study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 5171–5176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.H.; Hong, S.W.; Im, S.K.; Lee, S.H.; Ahn, M.D. Effect of myopia on the thickness of the retinal nerve fiber layer measured by Cirrus HD optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4075–4083. [Google Scholar] [CrossRef] [Green Version]
- Rauscher, F.M.; Sekhon, N.; Feuer, W.J.; Budenz, D.L. Myopia affects retinal nerve fiber layer measurements as determined by optical coherence tomography. J. Glaucoma 2009, 18, 501–505. [Google Scholar] [CrossRef] [Green Version]
- Alasil, T.; Wang, K.; Keane, P.A.; Lee, H.; Baniasadi, N.; de Boer, J.F.; Chen, T.C. Analysis of normal retinal nerve fiber layer thickness by age, sex, and race using spectral domain optical coherence tomography. J. Glaucoma 2013, 22, 532–541. [Google Scholar] [CrossRef]
- Invernizzi, A.; Pellegrini, M.; Acquistapace, A.; Benatti, E.; Erba, S.; Cozzi, M.; Cigada, M.; Viola, F.; Gillies, M.; Staurenghi, G. Normative Data for Retinal-Layer Thickness Maps Generated by Spectral-Domain OCT in a White Population. Ophthalmol. Retin. 2018, 2, 808.e1–815.e1. [Google Scholar] [CrossRef]
- Koh, V.T.; Tham, Y.C.; Cheung, C.Y.; Wong, W.L.; Baskaran, M.; Saw, S.M.; Wong, T.Y.; Aung, T. Determinants of ganglion cell-inner plexiform layer thickness measured by high-definition optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5853–5859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Littmann, H. Determination of the real size of an object on the fundus of the living eye. Klinische Monatsblatter fur Augenheilkunde 1982, 180, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Crowston, J.G.; Hopley, C.R.; Healey, P.R.; Lee, A.; Mitchell, P. Blue Mountains Eye Study. The effect of optic disc diameter on vertical cup to disc ratio percentiles in a population based cohort: The Blue Mountains Eye Study. Br. J. Ophthalmol. 2004, 88, 766–770. [Google Scholar] [CrossRef] [Green Version]
- Jonas, J.B.; Gusek, G.C.; Naumann, G.O. Optic disc, cup and neuroretinal rim size, configuration and correlations in normal eyes. Investig. Ophthalmol. Vis. Sci. 1988, 29, 1151–1158. [Google Scholar]
- Lee, E.J.; Lee, K.M.; Kim, H.; Kim, T.W. Glaucoma Diagnostic Ability of the New Circumpapillary Retinal Nerve Fiber Layer Thickness Analysis Based on Bruch’s Membrane Opening. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4194–4204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheuble, P.; Petrak, M.; Brinkmann, C.K. Glaucoma Diagnostic Testing: The Influence of Optic Disc Size. Klinische Monatsblatter fur Augenheilkunde 2022, 239, 1043–1051. [Google Scholar] [CrossRef]
- Palazon-Cabanes, A.; Palazon-Cabanes, B.; Rubio-Velazquez, E.; Lopez-Bernal, M.D.; Garcia-Medina, J.J.; Villegas-Perez, M.P. Normative Database for All Retinal Layer Thicknesses Using SD-OCT Posterior Pole Algorithm and the Effects of Age, Gender and Axial Lenght. J. Clin. Med. 2020, 9, 3317. [Google Scholar] [CrossRef] [PubMed]
- Ooto, S.; Hangai, M.; Tomidokoro, A.; Saito, H.; Araie, M.; Otani, T.; Kishi, S.; Matsushita, K.; Maeda, N.; Shirakashi, M.; et al. Effects of age, sex, and axial length on the three-dimensional profile of normal macular layer structures. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8769–8779. [Google Scholar] [CrossRef]
- Najeeb, S.; Ganne, P.; Damagatla, M.; Chaitanya, G.; Krishnappa, N.C. Mapping the thickness of retinal layers using Spectralis spectral domain optical coherence tomography in Indian eyes. Indian J. Ophthalmol. 2022, 70, 2990–2997. [Google Scholar] [CrossRef]
- Choovuthayakorn, J.; Chokesuwattanaskul, S.; Phinyo, P.; Hansapinyo, L.; Pathanapitoon, K.; Chaikitmongkol, V.; Watanachai, N.; Kunavisarut, P.; Patikulsila, D. Reference Database of Inner Retinal Layer Thickness and Thickness Asymmetry in Healthy Thai Adults as Measured by the Spectralis Spectral-Domain Optical Coherence Tomography. Ophthalmic Res. 2022, 65, 668–677. [Google Scholar] [CrossRef]
- Sung, M.S.; Heo, M.Y.; Heo, H.; Park, S.W. Bruch’s membrane opening enlargement and its implication on the myopic optic nerve head. Sci. Rep. 2019, 9, 19564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budenz, D.L.; Anderson, D.R.; Varma, R.; Schuman, J.; Cantor, L.; Savell, J.; Greenfield, D.S.; Patella, V.M.; Quigley, H.A.; Tielsch, J. Determinants of normal retinal nerve fiber layer thickness measured by Stratus OCT. Ophthalmology 2007, 114, 1046–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, D.D.; Mauschitz, M.M.; Bönniger, M.M.; Merten, N.; Finger, R.P.; Breteler, M.M.B. Association of retinal layer measurements and adult cognitive function: A population-based study. Neurology 2020, 95, e1144–e1152. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Xiao, H.; Lai, K.; Guo, X.; Luo, J.; Liu, X. Determinants of macular ganglion cell-inner plexiform layer thickness in normal Chinese adults. BMC Ophthalmol. 2021, 21, 267. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (Eyes) | 501 (100%) |
|---|---|
| n (patients) | 287 (100%) |
| age (years) | 35 (16; 56) |
| gender (M:F) | 210 (42%):291 (58%) |
| n (eyes) according to optic disc size (HRT division): | |
| large (2.43–4.15 mm2) | 123 (25%) |
| medium (1.63–2.42 mm2) | 298 (59%) |
| small (0.91–1.62 mm2) | 80 (16%) |
| n (eyes) according to optic disc size (quantile division): | |
| largest (3.30–4.15 mm2) | 25 (5%) |
| intermediate (1.41–3.30 mm2) | 451 (90%) |
| smallest (0.91–1.40 mm2) | 25 (5%) |
| study eye (R:L) | 249 (50%):252 (50%) |
| median visual acuity (logMAR) | 0.10 (0.00; 0.20) |
| median spherical equivalent: | 0.00 (−0.75; 0.63) |
| per group (HRT division) | |
| large | 0.00 (−1.13; 0.63) |
| medium | 0.00 (−0.75; 0.63) |
| small | 0.00 (−0.38; 0.66) |
| per group (quantile division) | |
| large | −0.25 (−1.25; 0.13) |
| medium | 0.00 (−0.63; 0.69) |
| small | 0.00 (−1.50; 1.50) |
| Estimate | Lower 95% CI | Upper 95% CI | |
|---|---|---|---|
| RNFL global | 0.04 | −0.08 | 0.15 |
| mGCLT global | 0.04 | −0.08 | 0.16 |
| RNFL | Estimate | Lower 95% CI Bound | Upper 95% CI Bound |
|---|---|---|---|
| NS | −0.04 | −0.15 | 0.08 |
| N | 0.02 | −0.09 | 0.14 |
| NI | 0.05 | −0.07 | 0.16 |
| TI | 0.06 | −0.06 | 0.17 |
| T | −0.02 | −0.14 | 0.10 |
| TS | 0.09 | −0.02 | 0.21 |
| mGCLT | |||
| C | 0.11 | 0.00 | 0.23 |
| IN | 0.02 | −0.09 | 0.14 |
| ON | −0.07 | −0.18 | 0.05 |
| II | 0.06 | −0.05 | 0.18 |
| OI | 0.00 | −0.12 | 0.11 |
| IT | 0.09 | −0.03 | 0.20 |
| OT | 0.05 | −0.07 | 0.16 |
| IS | 0.03 | −0.08 | 0.15 |
| OS | 0.01 | −0.11 | 0.13 |
| Small vs. Medium | Medium vs. Large | Small vs. Large | Median Thickness Small | Median Thickness Medium | Median Thickness Large | |
|---|---|---|---|---|---|---|
| RNFL Global | <0.01 | 0.05 | 0.42 | 96.50 | 102.00 | 100.00 |
| mGCLT Global | 0.08 | 1.00 | 0.94 | 40.11 | 41.22 | 40.89 |
| Smallest vs. Intermediate | Intermediate vs. Largest | Smallest vs. Largest | Median Thickness Smallest | Median Thickness Intermediate | Median Thickness Largest | |
|---|---|---|---|---|---|---|
| RNFL Global | 0.05 | 1.00 | 0.37 | 91.00 | 101.00 | 101.00 |
| mGCLT Global | 0.83 | 0.25 | 0.23 | 37.00 | 38.00 | 38.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Storp, J.J.; Storp, N.H.; Danzer, M.F.; Eter, N.; Biermann, J. Evaluation of Retinal Nerve Fiber Layer and Macular Ganglion Cell Layer Thickness in Relation to Optic Disc Size. J. Clin. Med. 2023, 12, 2471. https://doi.org/10.3390/jcm12072471
Storp JJ, Storp NH, Danzer MF, Eter N, Biermann J. Evaluation of Retinal Nerve Fiber Layer and Macular Ganglion Cell Layer Thickness in Relation to Optic Disc Size. Journal of Clinical Medicine. 2023; 12(7):2471. https://doi.org/10.3390/jcm12072471
Chicago/Turabian StyleStorp, Jens Julian, Nils Hendrik Storp, Moritz Fabian Danzer, Nicole Eter, and Julia Biermann. 2023. "Evaluation of Retinal Nerve Fiber Layer and Macular Ganglion Cell Layer Thickness in Relation to Optic Disc Size" Journal of Clinical Medicine 12, no. 7: 2471. https://doi.org/10.3390/jcm12072471