
Infant Perioperative Risk Factors and Adverse Brain Findings Following Long-Gap Esophageal Atresia Repair
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Brain MRI Acquisition and Structural Analyses
2.3. Underlying Disease Severity Scores and Clinical Parameter Acquisition
2.3.1. Disease Severity Scores
2.3.2. Clinical Care Measures
2.4. Statistical Analysis
2.4.1. Correlation Analysis
2.4.2. Multivariable Linear Regression
3. Results
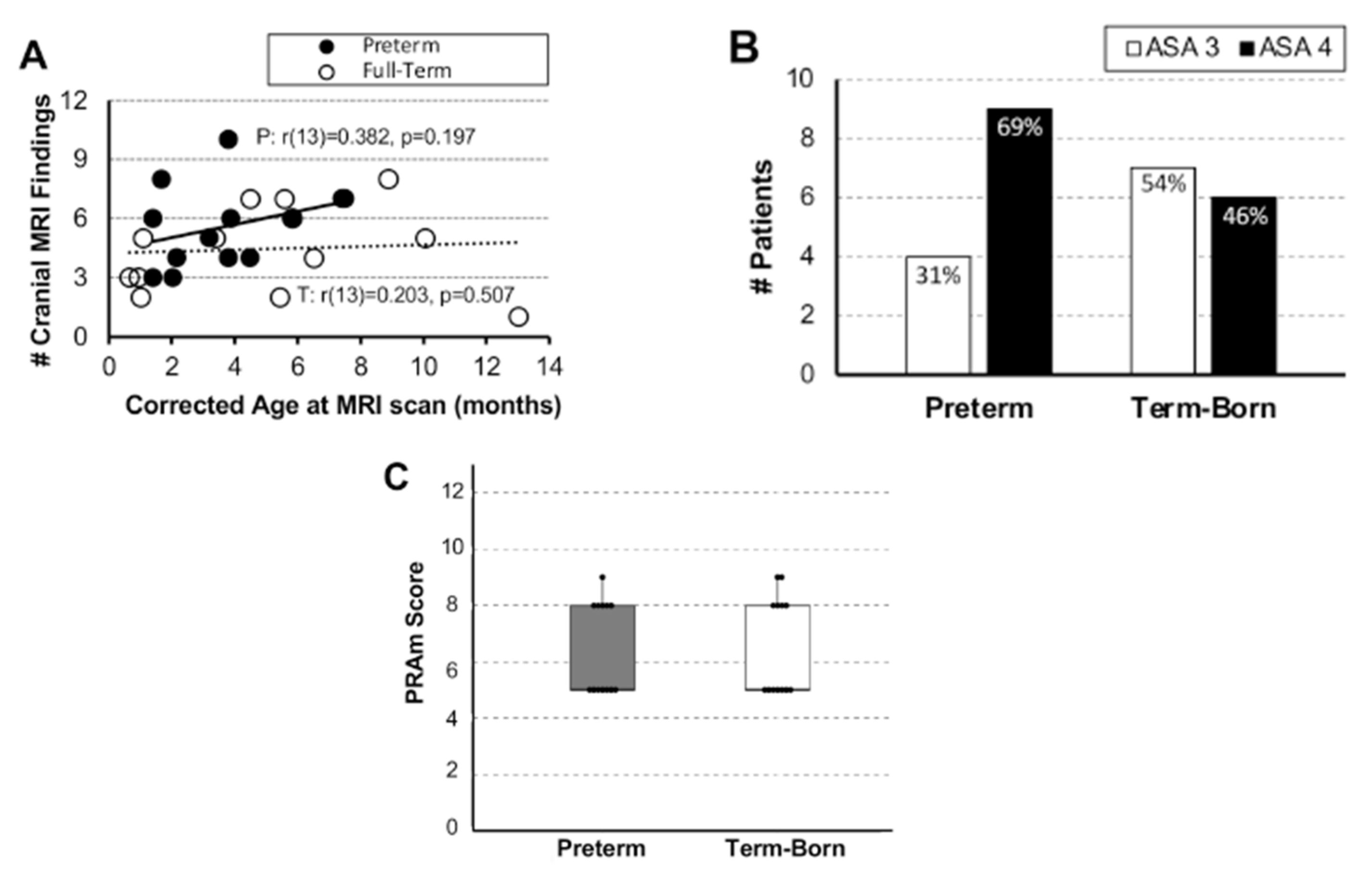
3.1. Brain MRI Measures
3.2. Underlying Disease Severity: American Society of Anesthesiology (ASA) Classification System and Pediatric Risk Assessment (PRAm) Scoring
3.2.1. Disease Severity Score Distribution
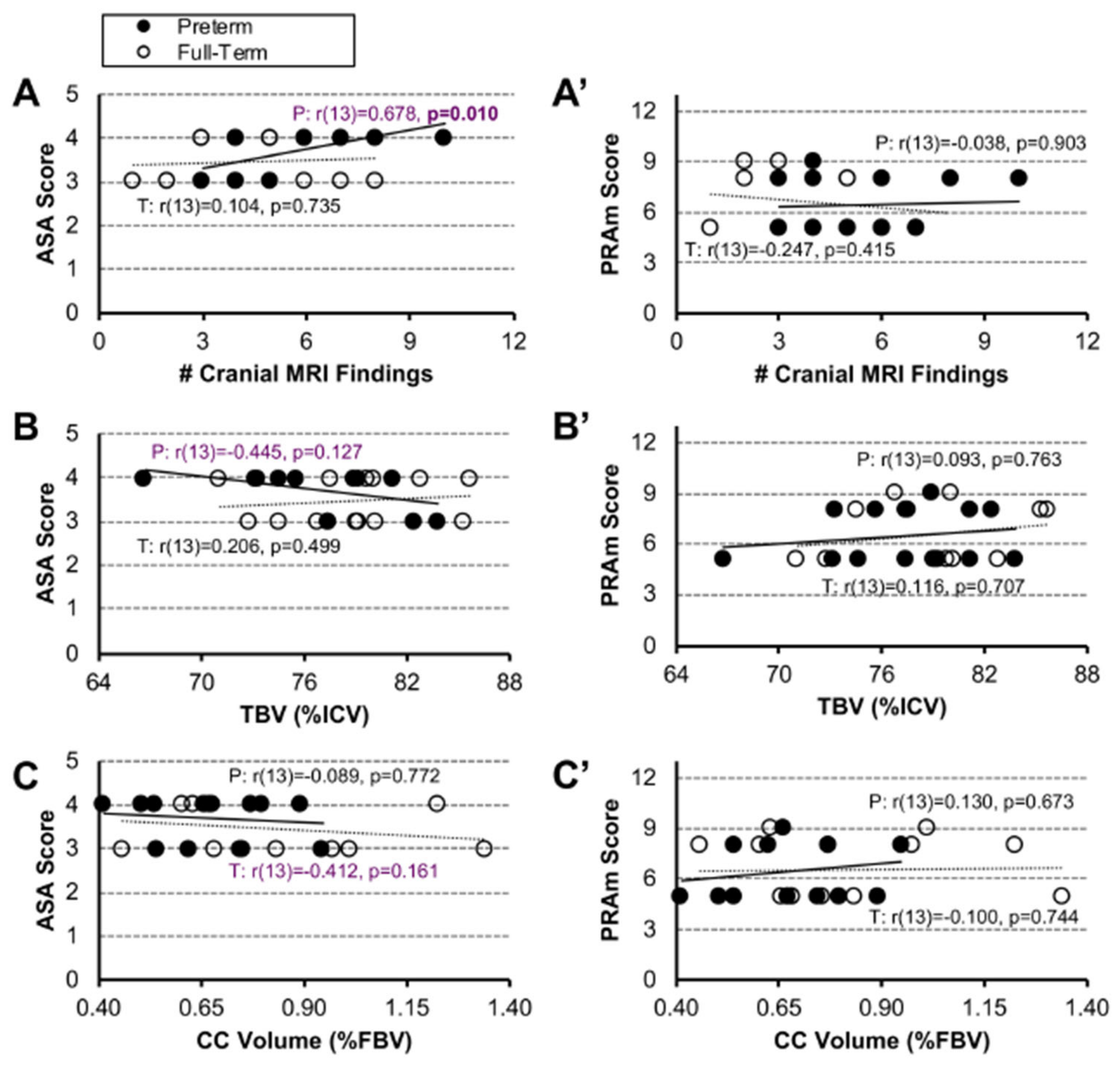
3.2.2. Associations between Disease Severity Scores and Brain MRI Data
3.3. Quantification of Clinical Measures of Care
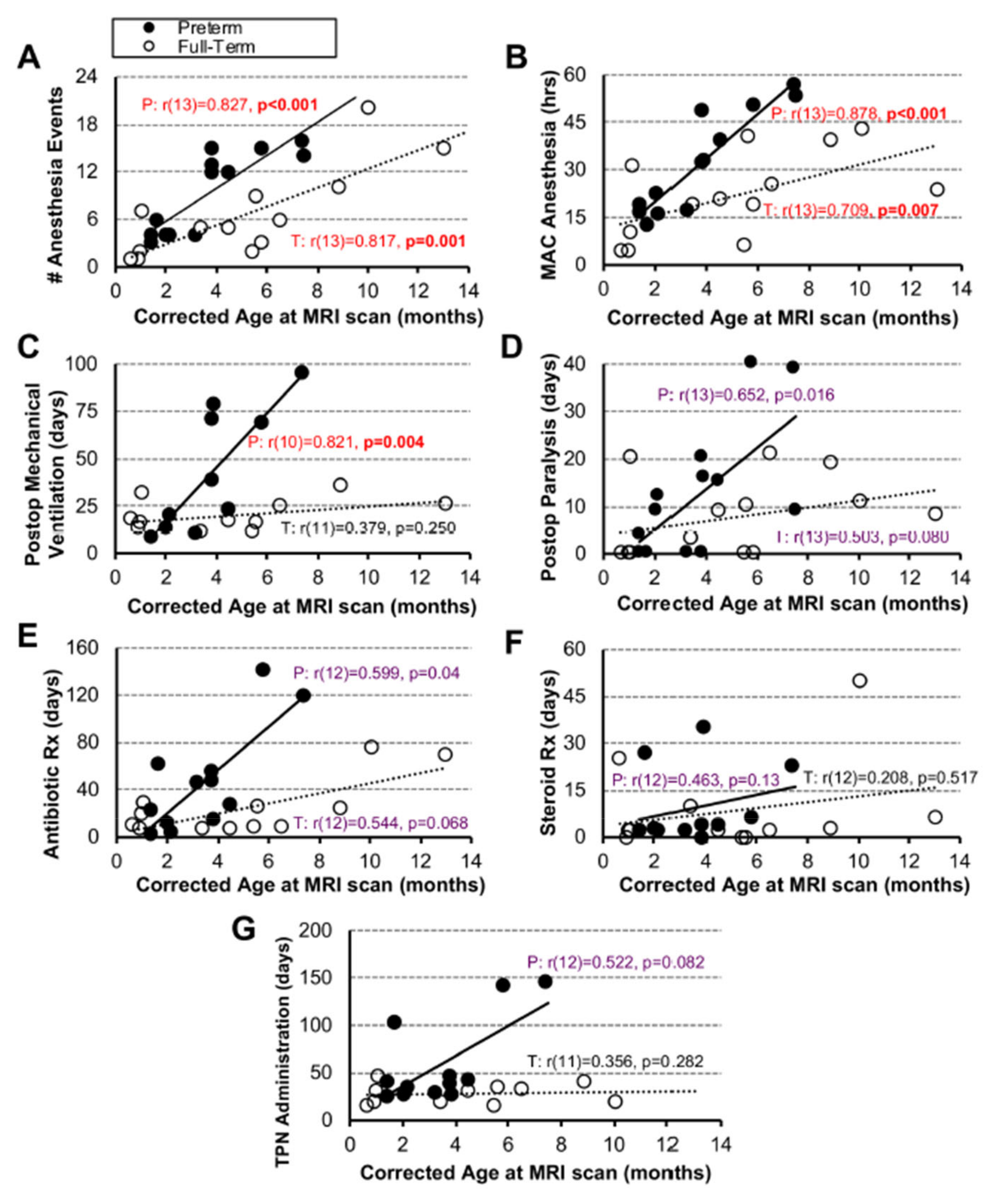
3.3.1. Associations between Clinical Measures and Age
3.3.2. Associations between Clinical Measures and Disease Severity Scores
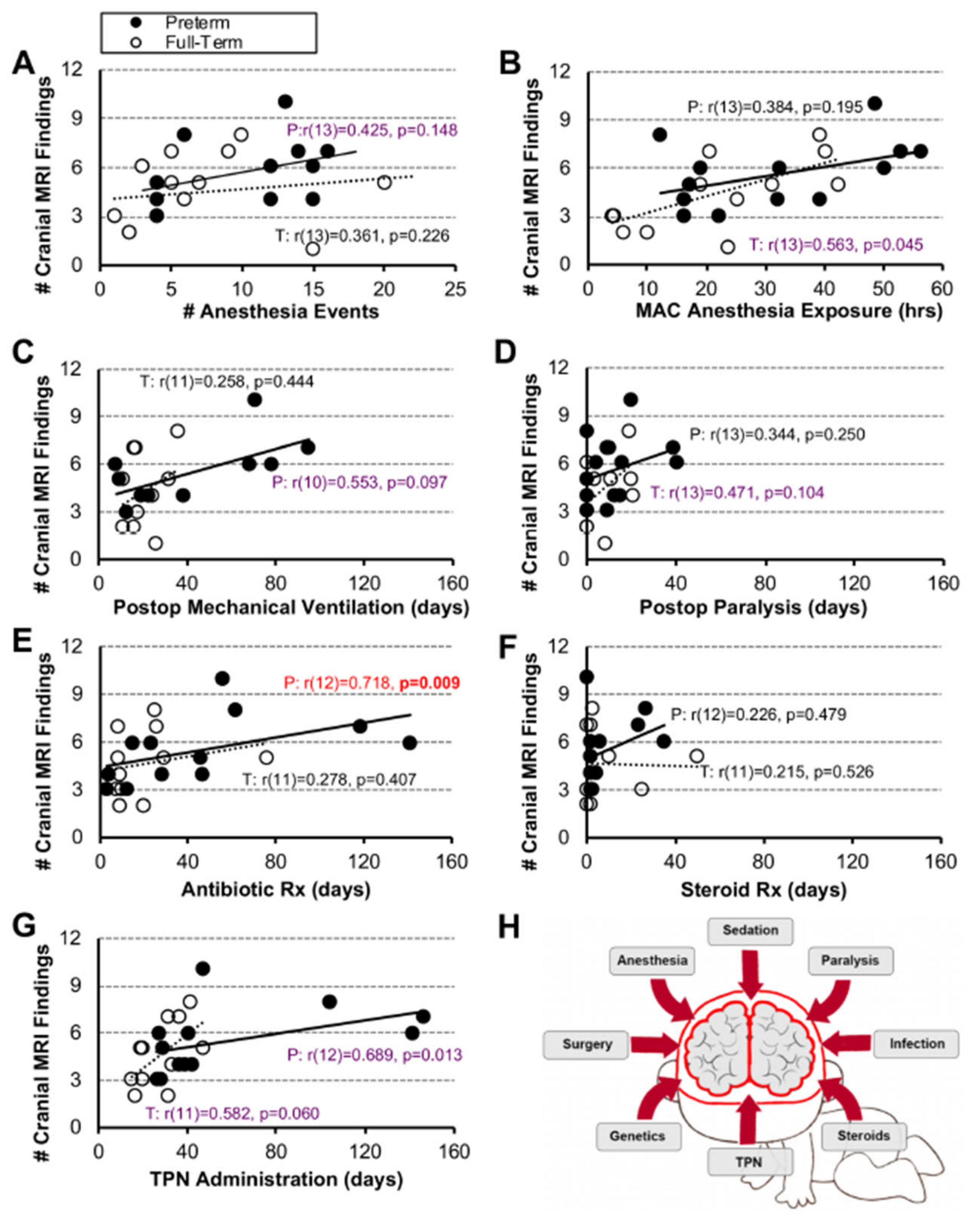
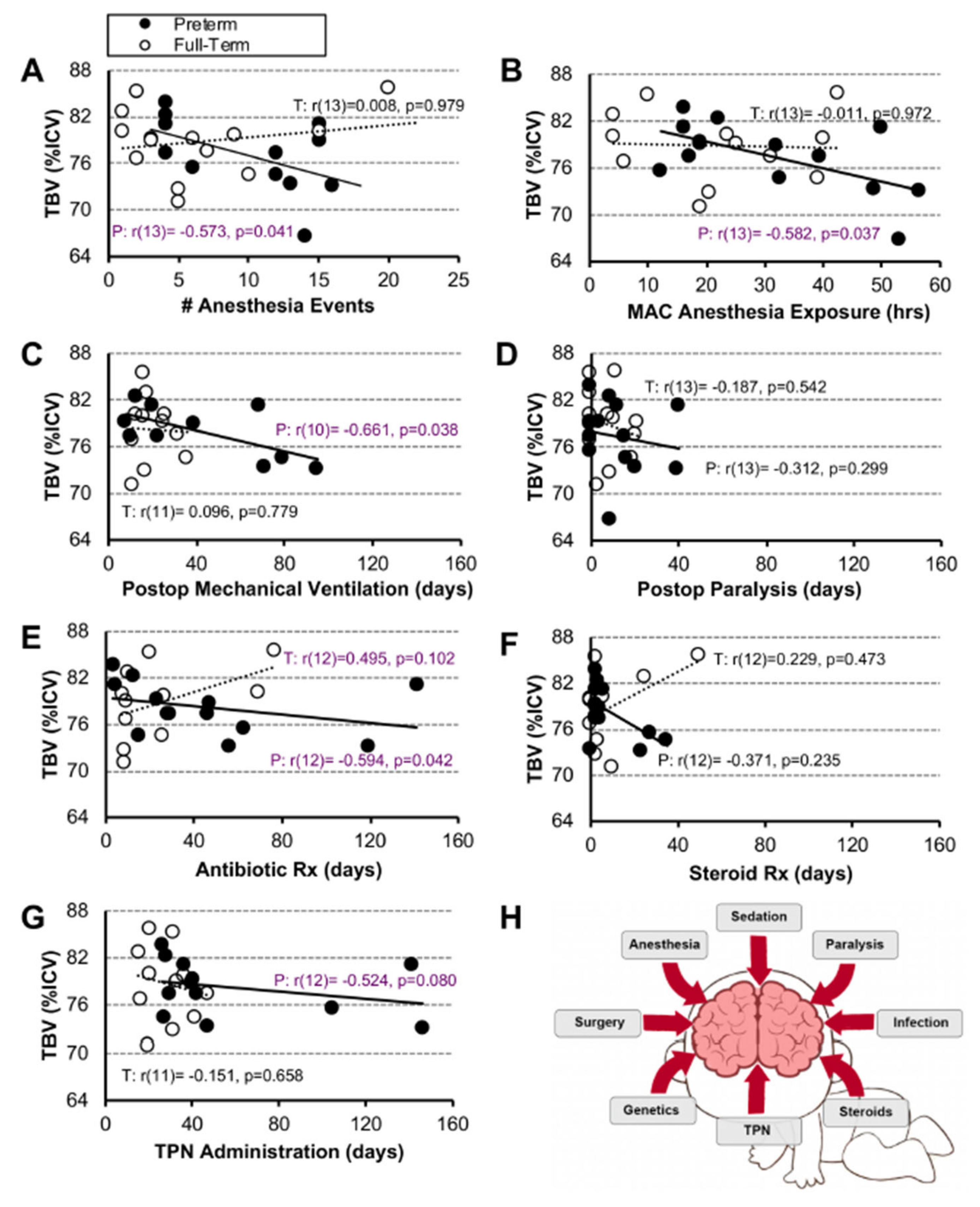
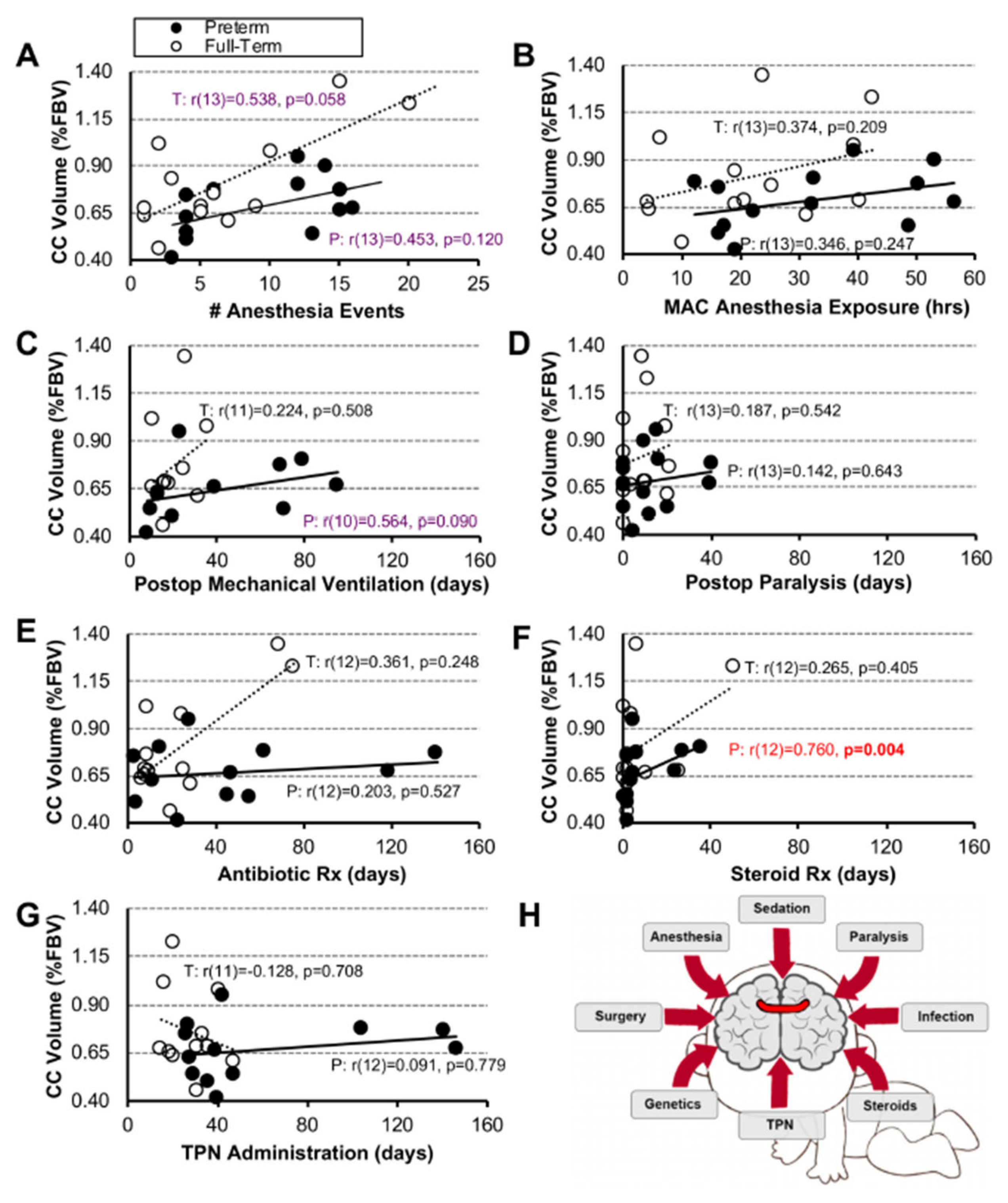
3.3.3. Associations between Clinical Measures and Brain MRI Measures
3.4. Multivariable Linear Regression Models
4. Discussion
4.1. Underlying Disease Severity Scoring Metrics’ Validity for Assessing Brain Findings following Long-Gap Esophageal Atresia Repair
4.2. Validity of Individual and Combined Clinical Parameters as Predictors of Brain Findings
4.3. Long-Term Evaluation and Neurodevelopmental Outcomes
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| LGEA | long-gap esophageal atresia |
| MAC | minimal alveolar concentration |
| MRI | magnetic resonance imaging |
| PRAm | Pediatric Risk Assessment |
| r | Spearman Rho test |
| SGA/IUGR | small for gestational age/intrauterine growth restriction |
| TEF | tracheo-esophageal fistula |
| TIVA | total intravenous anesthesia |
| TPN | total parenteral nutrition |
| VIF | variance inflation factor |
References
- Sfeir, R.; Michaud, L.; Salleron, J.; Gottrand, F. Epidemiology of esophageal atresia. Dis. Esophagus 2013, 26, 354–355. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Persaud, T.V.N.; Torchia, M.G. The Developing Human, Clinically Oriented Embryology, 10th ed.; Elsevier: Philadelphia, PA, USA, 2015. [Google Scholar]
- Van der Zee, D.C.; van Herwaarden, M.Y.; Tytgat, S.H.; Maffi, M.; Lima, M. Esophageal Atresia and Tracheoesophageal Fistula. In Neonatal Surgery; Lima, M., Reinberg, O., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Bairdain, S.; Zurakowski, D.; Vargas, S.O.; Stenquist, N.; McDonald, M.; Towne, M.C.; Miller, D.T.; Jennings, R.W.; Kantor, D.B.; Agrawal, P.B. Long-Gap Esophageal Atresia Is a Unique Entity within the Esophageal Atresia Defect Spectrum. Neonatology 2017, 111, 140–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holland, A.J.; Fitzgerald, D.A. Oesophageal atresia and tracheo-oesophageal fistula: Current management strategies and complications. Paediatr. Respir. Rev. 2010, 11, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Hunt, R.W.; Perkins, E.J.; King, S. Peri-operative management of neonates with oesophageal atresia and tracheo-oesophageal fistula. Paediatr. Respir. Rev. 2016, 19, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Foker, J.E.; Kendall Krosch, T.C.; Catton, K.; Munro, F.; Khan, K.M. Long-gap esophageal atresia treated by growth induction: The biological potential and early follow-up results. Semin. Pediatr. Surg. 2009, 18, 23–29. [Google Scholar] [CrossRef]
- Kunisaki, S.M.; Foker, J.E. Surgical advances in the fetus and neonate: Esophageal atresia. Clin. Perinatol. 2012, 39, 349–361. [Google Scholar] [CrossRef]
- Bairdain, S.; Hamilton, T.E.; Smithers, C.J.; Manfredi, M.; Ngo, P.; Gallagher, D.; Zurakowski, D.; Foker, J.E.; Jennings, R.W. Foker process for the correction of long gap esophageal atresia: Primary treatment versus secondary treatment after prior esophageal surgery. J. Pediatr. Surg. 2015, 50, 933–937. [Google Scholar] [CrossRef]
- Mongerson, C.R.L.; Wilcox, S.L.; Goins, S.M.; Pier, D.B.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Infant brain structural MRI analysis in the context of thoracic noncardiac surgery and critical care. Front. Pediatr. 2019, 7, 315. [Google Scholar] [CrossRef] [Green Version]
- Hodkinson, D.J.; Mongerson, C.R.L.; Jennings, R.W.; Bajic, D. Neonatal functional brain maturation in the context of perioperative critical care and pain management: A case report. Heliyon 2019, 5, e02350. [Google Scholar] [CrossRef] [Green Version]
- Liszewski, M.C.; Bairdain, S.; Buonomo, C.; Jennings, R.W.; Taylor, G.A. Imaging of long gap esophageal atresia and the Foker process: Expected findings and complications. Pediatr. Radiol. 2014, 44, 467–475. [Google Scholar] [CrossRef]
- Anand, K.J.; Barton, B.A.; McIntosh, N.; Lagercrantz, H.; Pelausa, E.; Young, T.E.; Vasa, R. Analgesia and sedation in preterm neonates who require ventilatory support: Results from the NOPAIN trial. Neonatal Outcome and Prolonged Analgesia in Neonates. Arch. Pediatr. Adolesc. Med. 1999, 153, 331–338. [Google Scholar] [CrossRef]
- Dewey, W.L. Various factors which affect the rate of development of tolerance and physical dependence to abused drugs. NIDA Res. Monogr. 1984, 54, 39–49. [Google Scholar]
- Solodiuk, J.C.; Jennings, R.W.; Bajic, D. Evaluation of Postnatal Sedation in Full-Term Infants. Brain Sci. 2019, 9, 114. [Google Scholar] [CrossRef] [Green Version]
- Stolwijk, L.J.; Keunen, K.; de Vries, L.S.; Groenendaal, F.; van der Zee, D.C.; van Herwaarden, M.Y.A.; Lemmers, P.M.A.; Benders, M. Neonatal Surgery for Noncardiac Congenital Anomalies: Neonates at Risk of Brain Injury. J. Pediatr. 2017, 182, 335–341. [Google Scholar] [CrossRef]
- Stolwijk, L.J.; Lemmers, P.M.; Harmsen, M.; Groenendaal, F.; de Vries, L.S.; van der Zee, D.C.; Benders, M.J.; van Herwaarden-Lindeboom, M.Y. Neurodevelopmental Outcomes After Neonatal Surgery for Major Noncardiac Anomalies. Pediatrics 2016, 137, e20151728. [Google Scholar] [CrossRef] [Green Version]
- Rudisill, S.S.; Wang, J.T.; Jaimes, C.; Mongerson, C.R.L.; Hansen, A.R.; Jennings, R.W.; Bajic, D. Neurologic injury and brain growth in the setting of long-gap esophageal atresia perioperative critical care: A pilot study. Brain Sci. 2019, 9, 383. [Google Scholar] [CrossRef] [Green Version]
- Mongerson, C.R.L.; Jaimes, C.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Infant Corpus Callosum Size After Surgery and Critical Care for Long-Gap Esophageal Atresia: Qualitative and Quantitative MRI. Sci. Rep. 2020, 10, 6408. [Google Scholar] [CrossRef] [Green Version]
- Mongerson, C.R.L.; Jennings, R.W.; Zurakowski, D.; Bajic, D. Quantitative MRI study of infant regional brain size following surgery for long-gap esophageal atresia requiring prolonged critical care. Int. J. Dev. Neurosci. 2019, 79, 11–20. [Google Scholar] [CrossRef]
- Bajic, D.; Rudisill, S.S.; Jennings, R.W. Head circumference in infants undergoing Foker process for long-gap esophageal atresia repair: Call for attention. J. Pediatr. Surg. 2021, 59, 1564–1569. [Google Scholar] [CrossRef]
- Doyle, D.J.; Goyal, A.; Bansal, P.; Garmon, E.H. American Society of Anesthesiologists Classification. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Nasr, V.G.; DiNardo, J.A.; Faraoni, D. Development of a Pediatric Risk Assessment Score to Predict Perioperative Mortality in Children Undergoing Noncardiac Surgery. Anesth. Analg. 2017, 124, 1514–1519. [Google Scholar] [CrossRef]
- Quinn, J.A.; Munoz, F.M.; Gonik, B.; Frau, L.; Cutland, C.; Mallett-Moore, T.; Kissou, A.; Wittke, F.; Das, M.; Nunes, T.; et al. Preterm birth: Case definition & guidelines for data collection, analysis, and presentation of immunisation safety data. Vaccine 2016, 34, 6047–6056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svetanoff, W.J.; Zendejas, B.; Hernandez, K.; Davidson, K.; Ngo, P.; Manfredi, M.; Hamilton, T.E.; Jennings, R.; Smithers, C.J. Contemporary outcomes of the Foker process and evolution of treatment algorithms for long-gap esophageal atresia. J. Pediatr. Surg. 2021, 56, 2180–2191. [Google Scholar] [CrossRef] [PubMed]
- Kamran, A.; Zendejas, B.; Jennings, R.W. Long-Gap Esophageal Atresia. In Fundamentals of Pediatric Surgery; Springer: Cham, Switzerland, 2022; pp. 497–508. [Google Scholar]
- Vet, N.J.; Kleiber, N.; Ista, E.; de Hoog, M.; de Wildt, S.N. Sedation in Critically Ill Children with Respiratory Failure. Front. Pediatr. 2016, 4, 89. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Shastri, S.; Farahbakhsh, N.; Sharma, P. Intrauterine growth restriction—Part 1. J. Matern. Fetal Neonatal. Med. 2016, 29, 3977–3987. [Google Scholar] [CrossRef] [PubMed]
- Tsudo, M.; Uchiyama, T.; Takatsuki, K.; Uchino, H.; Yodoi, J. Modulation of Tac antigen on activated human T cells by anti-Tac monoclonal antibody. J. Immunol. 1982, 129, 592–595. [Google Scholar] [CrossRef]
- Kagan, M.S.; Mongerson, C.R.L.; Zurakowski, D.; Bajic, D. Impact of Infant Thoracic Non-cardiac Perioperative Critical Care on Homotopic-Like Corpus Callosum and Forebrain Sub-regional Volumes. Front. Pain Res. 2022, 3, 788903. [Google Scholar] [CrossRef]
- Beare, R.J.; Chen, J.; Kelly, C.E.; Alexopoulos, D.; Smyser, C.D.; Rogers, C.E.; Loh, W.Y.; Matthews, L.G.; Cheong, J.L.; Spittle, A.J.; et al. Neonatal Brain Tissue Classification with Morphological Adaptation and Unified Segmentation. Front. Neuroinform. 2016, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Schober, P.; Vetter, T.R. Correlation Analysis in Medical Research. Anesth. Analg. 2020, 130, 332. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Curtin, F.; Schulz, P. Multiple correlations and Bonferroni’s correction. Biol. Psychiatry 1998, 44, 775–777. [Google Scholar] [CrossRef]
- Herrup, E.A.; Wieczorek, B.; Kudchadkar, S.R. Characteristics of postintensive care syndrome in survivors of pediatric critical illness: A systematic review. World J. Crit. Care Med. 2017, 6, 124–134. [Google Scholar] [CrossRef]
- Valencia, E.; Staffa, S.J.; Faraoni, D.; DiNardo, J.A.; Nasr, V.G. Prospective External Validation of the Pediatric Risk Assessment Score in Predicting Perioperative Mortality in Children Undergoing Noncardiac Surgery. Anesth. Analg. 2019, 129, 1014–1020. [Google Scholar] [CrossRef]
- Symington, A.; Pinelli, J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst. Rev. 2003, 4, CD001814. [Google Scholar] [CrossRef]
- Hickey, L.; Burnett, A.; Spittle, A.J.; Roberts, G.; Anderson, P.; Lee, K.; Doyle, L.W.; Cheong, J.L.Y.; Victorian Infant Collaborative Study, G. Extreme prematurity, growth and neurodevelopment at 8 years: A cohort study. Arch. Dis. Child. 2021, 106, 160–166. [Google Scholar] [CrossRef]
- Pollack, M.M.; Ruttimann, U.E.; Getson, P.R. Pediatric risk of mortality (PRISM) score. Crit. Care Med. 1988, 16, 1110–1116. [Google Scholar] [CrossRef]
- Leteurtre, S.; Duhamel, A.; Salleron, J.; Grandbastien, B.; Lacroix, J.; Leclerc, F.; Groupe Francophone de Reanimation et d’Urgences, P. PELOD-2: An update of the PEdiatric logistic organ dysfunction score. Crit. Care Med. 2013, 41, 1761–1773. [Google Scholar] [CrossRef]
- Graciano, A.L.; Balko, J.A.; Rahn, D.S.; Ahmad, N.; Giroir, B.P. The Pediatric Multiple Organ Dysfunction Score (P-MODS): Development and validation of an objective scale to measure the severity of multiple organ dysfunction in critically ill children. Crit. Care Med. 2005, 33, 1484–1491. [Google Scholar] [CrossRef]
- Casavant, S.G.; Cong, X.; Fitch, R.H.; Moore, J.; Rosenkrantz, T.; Starkweather, A. Allostatic Load and Biomarkers of Stress in the Preterm Infant: An Integrative Review. Biol. Res. Nurs. 2019, 21, 210–223. [Google Scholar] [CrossRef]
- Guidi, J.; Lucente, M.; Sonino, N.; Fava, G.A. Allostatic Load and Its Impact on Health: A Systematic Review. Psychother. Psychosom. 2021, 90, 11–27. [Google Scholar] [CrossRef]
- Wilder, R.T.; Flick, R.P.; Sprung, J.; Katusic, S.K.; Barbaresi, W.J.; Mickelson, C.; Gleich, S.J.; Schroeder, D.R.; Weaver, A.L.; Warner, D.O. Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology 2009, 110, 796–804. [Google Scholar] [CrossRef] [Green Version]
- Flick, R.P.; Katusic, S.K.; Colligan, R.C.; Wilder, R.T.; Voigt, R.G.; Olson, M.D.; Sprung, J.; Weaver, A.L.; Schroeder, D.R.; Warner, D.O. Cognitive and behavioral outcomes after early exposure to anesthesia and surgery. Pediatrics 2011, 128, e1053–e1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ing, C.; DiMaggio, C.; Whitehouse, A.; Hegarty, M.K.; Brady, J.; von Ungern-Sternberg, B.S.; Davidson, A.; Wood, A.J.; Li, G.; Sun, L.S. Long-term differences in language and cognitive function after childhood exposure to anesthesia. Pediatrics 2012, 130, e476–e485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oztan, M.O.; Soyer, T.; Oztorun, C.I.; Firinci, B.; Durakbasa, C.U.; Dokumcu, Z.; Gollu, G.; Akkoyun, I.; Demirel, D.; Karaman, A.; et al. Outcome of Very Low and Low Birth Weight Infants with Esophageal Atresia: Results of the Turkish Esophageal Atresia Registry. Eur. J. Pediatr. Surg. 2021, 31, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Van der Zee, D.C.; van Herwaarden, M.Y.A.; Hulsker, C.C.C.; Witvliet, M.J.; Tytgat, S.H.A. Esophageal Atresia and Upper Airway Pathology. Clin. Perinatol. 2017, 44, 753–762. [Google Scholar] [CrossRef]
- Harrington, A.W.; Riebold, J.; Hernandez, K.; Staffa, S.J.; Svetanoff, W.J.; Zurakowski, D.; Hamilton, T.; Jennings, R.; Mehta, N.M.; Zendejas, B. Nutrition delivery and growth outcomes in infants with long-gap esophageal atresia who undergo the Foker process. J. Pediatr. Surg. 2021, 56, 2133–2139. [Google Scholar] [CrossRef]
- Evanovich, D.M.; Wang, J.T.; Zendejas, B.; Jennings, R.W.; Bajic, D. From the Ground Up: Esophageal Atresia Types, Disease Severity Stratification and Survival Rates at a Single Institution. Front. Surg. 2022, 9, 799052. [Google Scholar] [CrossRef]
- Spitz, L.; Kiely, E.M.; Morecroft, J.A.; Drake, D.P. Oesophageal atresia: At-risk groups for the 1990s. J. Pediatr. Surg. 1994, 29, 723–725. [Google Scholar] [CrossRef]
- Waterston, D.J.; Carter, R.E.; Aberdeen, E. Oesophageal atresia: Tracheo-oesophageal fistula. A study of survival in 218 infants. Lancet 1962, 1, 819–822. [Google Scholar] [CrossRef]
- Van Hoorn, C.E.; Ten Kate, C.A.; Rietman, A.B.; Toussaint-Duyster, L.C.C.; Stolker, R.J.; Wijnen, R.M.H.; de Graaff, J.C. Long-term neurodevelopment in children born with esophageal atresia: A systematic review. Dis. Esophagus 2021, 34, doab054. [Google Scholar] [CrossRef]
- McCann, M.E.; de Graaff, J.C.; Dorris, L.; Disma, N.; Withington, D.; Bell, G.; Grobler, A.; Stargatt, R.; Hunt, R.W.; Sheppard, S.J.; et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): An international, multicentre, randomised, controlled equivalence trial. Lancet 2019, 393, 664–677. [Google Scholar] [CrossRef]
- Curley, M.A.; Wypij, D.; Watson, R.S.; Grant, M.J.; Asaro, L.A.; Cheifetz, I.M.; Dodson, B.L.; Franck, L.S.; Gedeit, R.G.; Angus, D.C.; et al. Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: A randomized clinical trial. JAMA 2015, 313, 379–389. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.J.; Disma, N.; de Graaff, J.C.; Withington, D.E.; Dorris, L.; Bell, G.; Stargatt, R.; Bellinger, D.C.; Schuster, T.; Arnup, S.J.; et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): An international multicentre, randomised controlled trial. Lancet 2016, 387, 239–250. [Google Scholar] [CrossRef] [Green Version]
- Disma, N.; Veyckemans, F.; Virag, K.; Hansen, T.G.; Becke, K.; Harlet, P.; Vutskits, L.; Walker, S.M.; de Graaff, J.C.; Zielinska, M.; et al. Morbidity and mortality after anaesthesia in early life: Results of the European prospective multicentre observational study, neonate and children audit of anaesthesia practice in Europe (NECTARINE). Br. J. Anaesth. 2021, 126, 1157–1172. [Google Scholar] [CrossRef]
- Kussman, B.D.; Wypij, D.; Laussen, P.C.; Soul, J.S.; Bellinger, D.C.; DiNardo, J.A.; Robertson, R.; Pigula, F.A.; Jonas, R.A.; Newburger, J.W. Relationship of intraoperative cerebral oxygen saturation to neurodevelopmental outcome and brain magnetic resonance imaging at 1 year of age in infants undergoing biventricular repair. Circulation 2010, 122, 245–254. [Google Scholar] [CrossRef]
- Sadhwani, A.; Cheng, H.; Stopp, C.; Rollins, C.K.; Jolley, M.A.; Dunbar-Masterson, C.; Wypij, D.; Newburger, J.; Ware, J.; Thiagarajan, R.R. Early Neurodevelopmental Outcomes in Children Supported with ECMO for Cardiac Indications. Pediatr. Cardiol. 2019, 40, 1072–1083. [Google Scholar] [CrossRef]
- Meuwly, E.; Feldmann, M.; Knirsch, W.; von Rhein, M.; Payette, K.; Dave, H.; Tuura, R.O.G.; Kottke, R.; Hagmann, C.; Latal, B.; et al. Postoperative brain volumes are associated with one-year neurodevelopmental outcome in children with severe congenital heart disease. Sci. Rep. 2019, 9, 10885. [Google Scholar] [CrossRef] [Green Version]
- Garcia Guerra, G.; Robertson, C.M.; Alton, G.Y.; Joffe, A.R.; Dinu, I.A.; Nicholas, D.; Ross, D.B.; Rebeyka, I.M.; Western Canadian Complex Pediatric Therapies Follow-up Group. Quality of life 4 years after complex heart surgery in infancy. J. Thorac. Cardiovasc. Surg. 2013, 145, 482–488. [Google Scholar] [CrossRef] [Green Version]
- Garcia Guerra, G.; Joffe, A.R.; Robertson, C.M.; Atallah, J.; Alton, G.; Sauve, R.S.; Dinu, I.A.; Ross, D.B.; Rebeyka, I.M.; Western Canadian Complex Pediatric Therapies Follow-up Group. Health-related quality of life experienced by children with chromosomal abnormalities and congenital heart defects. Pediatr. Cardiol. 2014, 35, 536–541. [Google Scholar] [CrossRef]
- Ricci, M.F.; Andersen, J.C.; Joffe, A.R.; Watt, M.J.; Moez, E.K.; Dinu, I.A.; Garcia Guerra, G.; Ross, D.B.; Rebeyka, I.M.; Robertson, C.M. Chronic Neuromotor Disability After Complex Cardiac Surgery in Early Life. Pediatrics 2015, 136, e922–e933. [Google Scholar] [CrossRef] [Green Version]
- Garcia Guerra, G.; Zorzela, L.; Robertson, C.M.; Alton, G.Y.; Joffe, A.R.; Moez, E.K.; Dinu, I.A.; Ross, D.B.; Rebeyka, I.M.; Lequier, L.; et al. Survival and neurocognitive outcomes in pediatric extracorporeal-cardiopulmonary resuscitation. Resuscitation 2015, 96, 208–213. [Google Scholar] [CrossRef]
- Andropoulos, D.B.; Ahmad, H.B.; Haq, T.; Brady, K.; Stayer, S.A.; Meador, M.R.; Hunter, J.V.; Rivera, C.; Voigt, R.G.; Turcich, M.; et al. The association between brain injury, perioperative anesthetic exposure, and 12-month neurodevelopmental outcomes after neonatal cardiac surgery: A retrospective cohort study. Paediatr. Anaesth. 2014, 24, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Garcia Guerra, G.; Robertson, C.M.; Alton, G.Y.; Joffe, A.R.; Cave, D.A.; Yasmin, F.; Dinu, I.A.; Creighton, D.E.; Ross, D.B.; Rebeyka, I.M.; et al. Neurotoxicity of sedative and analgesia drugs in young infants with congenital heart disease: 4-year follow-up. Paediatr. Anaesth. 2014, 24, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, V.A.; Carpenter, J.L.; Zurakowski, D.; Reitz, J.G.; Tague, L.; Donofrio, M.T.; Murnick, J.; Axt-Fliedner, R.; Limperopoulos, C.; Yerebakan, C. Determinants of neurological outcome in neonates with congenital heart disease following heart surgery. Pediatr. Res. 2021, 89, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Morgan, T.M.; Case, L.D. Conservative Sample Size Determination for Repeated Measures Analysis of Covariance. Ann. Biom. Biostat. 2013, 1, 1002. [Google Scholar]
- Staffa, S.J.; Zurakowski, D. Statistical power and sample size calculations: A primer for pediatric surgeons. J. Pediatr. Surg. 2019, 55, 1173–1179. [Google Scholar] [CrossRef]
- Staffa, S.J.; Zurakowski, D. Five Steps to Successfully Implement and Evaluate Propensity Score Matching in Clinical Research Studies. Anesth. Analg. 2018, 127, 1066–1073. [Google Scholar] [CrossRef]
- Zacharia, A.; Zimine, S.; Lovblad, K.O.; Warfield, S.; Thoeny, H.; Ozdoba, C.; Bossi, E.; Kreis, R.; Boesch, C.; Schroth, G.; et al. Early assessment of brain maturation by MR imaging segmentation in neonates and premature infants. AJNR Am. J. Neuroradiol. 2006, 27, 972–977. [Google Scholar]
- Gischler, S.J.; Mazer, P.; Duivenvoorden, H.J.; van Dijk, M.; Bax, N.M.; Hazebroek, F.W.; Tibboel, D. Interdisciplinary structural follow-up of surgical newborns: A prospective evaluation. J. Pediatr. Surg. 2009, 44, 1382–1389. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Qualitative MRI Findings |
# PRETERM (n = 13) |
# TERM-BORN (n = 13) |
Total # Anomalies |
|---|---|---|---|
| Brain Abnormalities | |||
| Increased extra-axial space | 11 | 7 | 18 |
| Widened sylvian fissures | 5 | 5 | 10 |
| Enlarged/Prominent Ventricles | 11 | 9 | 20 |
| Low cerebellar volume | 0 | 0 | 0 |
| Low brainstem volume | 0 | 0 | 0 |
| Chronic blood products (e.g., hemosiderin) | 0 | 2 | 2 |
| Mass or cyst | 1 | 2 | 3 |
| Narrowing of cerebral aqueduct | 1 | 0 | 1 |
| Incomplete rotation of hippocampi | 2 | 0 | 2 |
| White Matter Abnormalities | |||
| Low cerebral white matter volume | 1 | 0 | 1 |
| Abnormal signal in white matter | 2 | 4 | 6 |
| Corpus callosum abnormalities | 12 | 10 | 22 |
| Grey Matter Abnormalities | |||
| Low cerebral grey matter volume | 0 | 1 | 1 |
| Abnormal signal in grey matter | 0 | 0 | 0 |
| Vasculature Abnormalities/Hemorrhage | |||
| Intraventricular Hemorrhage | 1 | 0 | 1 |
| Subdural hemorrhage | 3 | 0 | 3 |
| Subdural effusion/collection | 1 | 2 | 3 |
| Arterial ischemic/hemorrhagic stroke | 1 | 0 | 1 |
| Venous hemorrhagic stroke | 0 | 1 | 1 |
| Cerebellar hemorrhage (arterial or venous) stroke | 0 | 1 | 1 |
| Vascular anomaly | 1 | 0 | 1 |
| Possible parturitional hemorrhage | 0 | 1 | 1 |
| Cranial Abnormalities | |||
| Abnormal head shape (e.g., plagiocelphaly) | 3 | 2 | 5 |
| Non-CNS cranial anomaly | 3 | 2 | 5 |
| Clinical Variables | Regression Coefficient | 95% CI | p Value |
|---|---|---|---|
| 1. Group Status (Preterm vs. Term-born) | 0.026 | −1.881 to 1.932 | 0.98 |
| 2. MAC Anesthesia Exposure (hrs) | 0.119 | 0.002 to 0.237 | 0.05 |
| 3. Intubated Sedation (days) | 0.031 | −0.05 to 0.113 | 0.42 |
| 4. Postoperative Paralysis (days) | −0.014 | −0.157 to 0.128 | 0.83 |
| 5. Antibiotic Rx (days) | −0.029 | −0.064 to 0.007 | 0.11 |
| 6. Steroid Rx (days) | −0.039 | −0.166 to 0.088 | 0.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kagan, M.S.; Wang, J.T.; Pier, D.B.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Infant Perioperative Risk Factors and Adverse Brain Findings Following Long-Gap Esophageal Atresia Repair. J. Clin. Med. 2023, 12, 1807. https://doi.org/10.3390/jcm12051807
Kagan MS, Wang JT, Pier DB, Zurakowski D, Jennings RW, Bajic D. Infant Perioperative Risk Factors and Adverse Brain Findings Following Long-Gap Esophageal Atresia Repair. Journal of Clinical Medicine. 2023; 12(5):1807. https://doi.org/10.3390/jcm12051807
Chicago/Turabian StyleKagan, Mackenzie Shea, Jue Teresa Wang, Danielle Bennett Pier, David Zurakowski, Russell William Jennings, and Dusica Bajic. 2023. "Infant Perioperative Risk Factors and Adverse Brain Findings Following Long-Gap Esophageal Atresia Repair" Journal of Clinical Medicine 12, no. 5: 1807. https://doi.org/10.3390/jcm12051807