
Towards Automation in IVF: Pre-Clinical Validation of a Deep Learning-Based Embryo Grading System during PGT-A Cycles

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
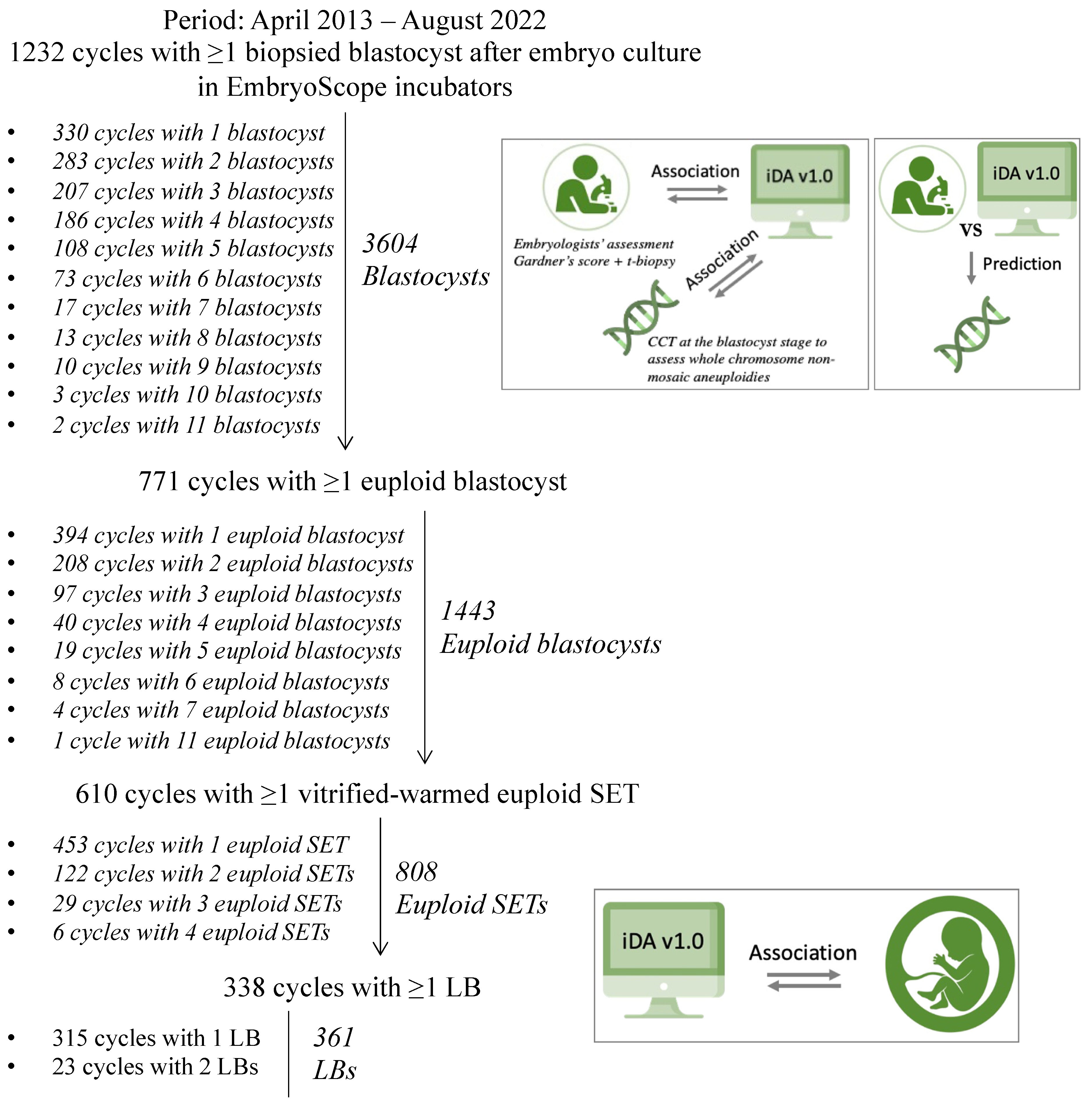
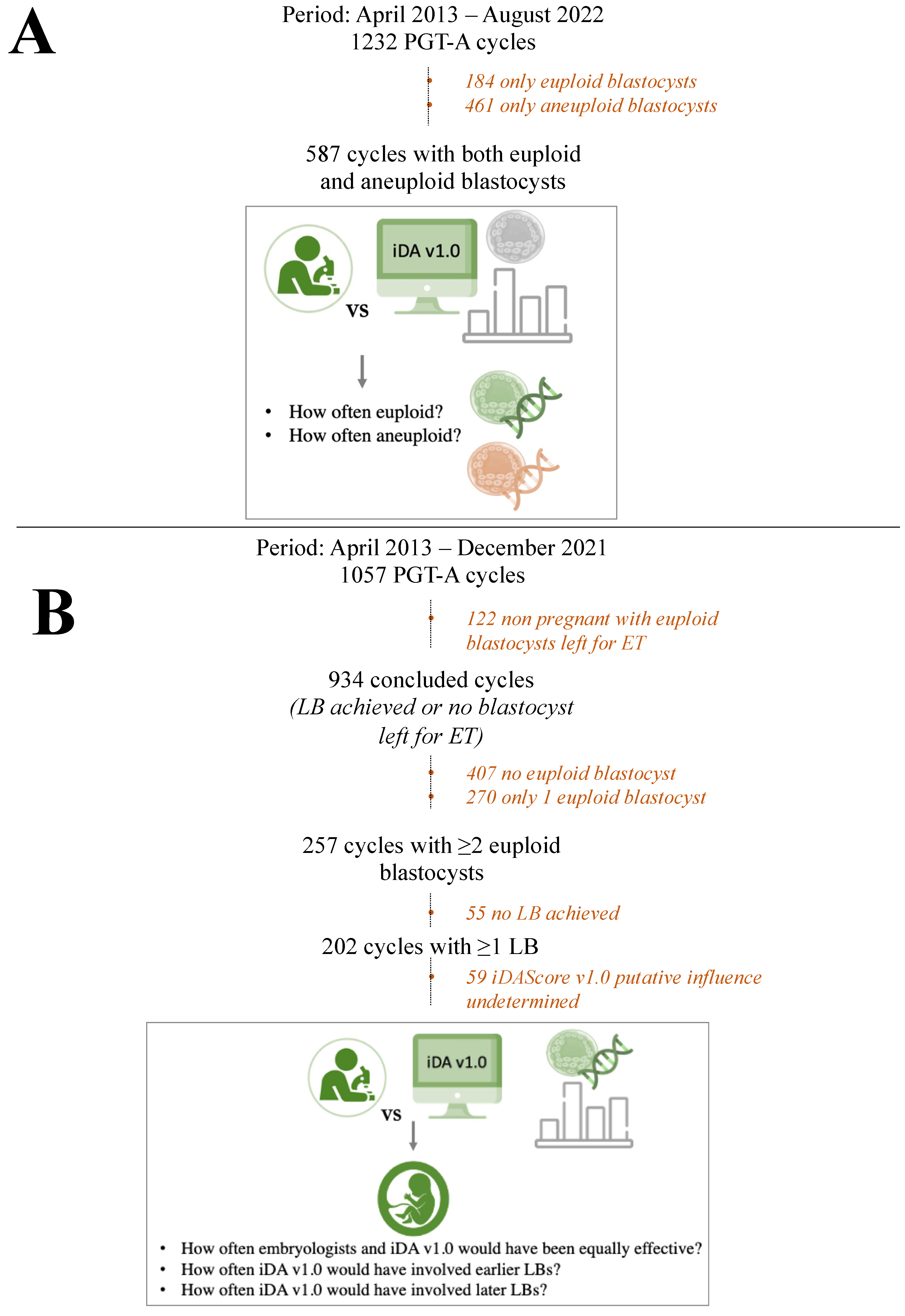
2.1. Study Design
2.2. IVF Protocols
2.3. iDAScore v1.0
2.4. Statistical Analysis
3. Results
3.1. The Patients Included Are Predominantly Poor Prognosis and of Advanced Maternal Age
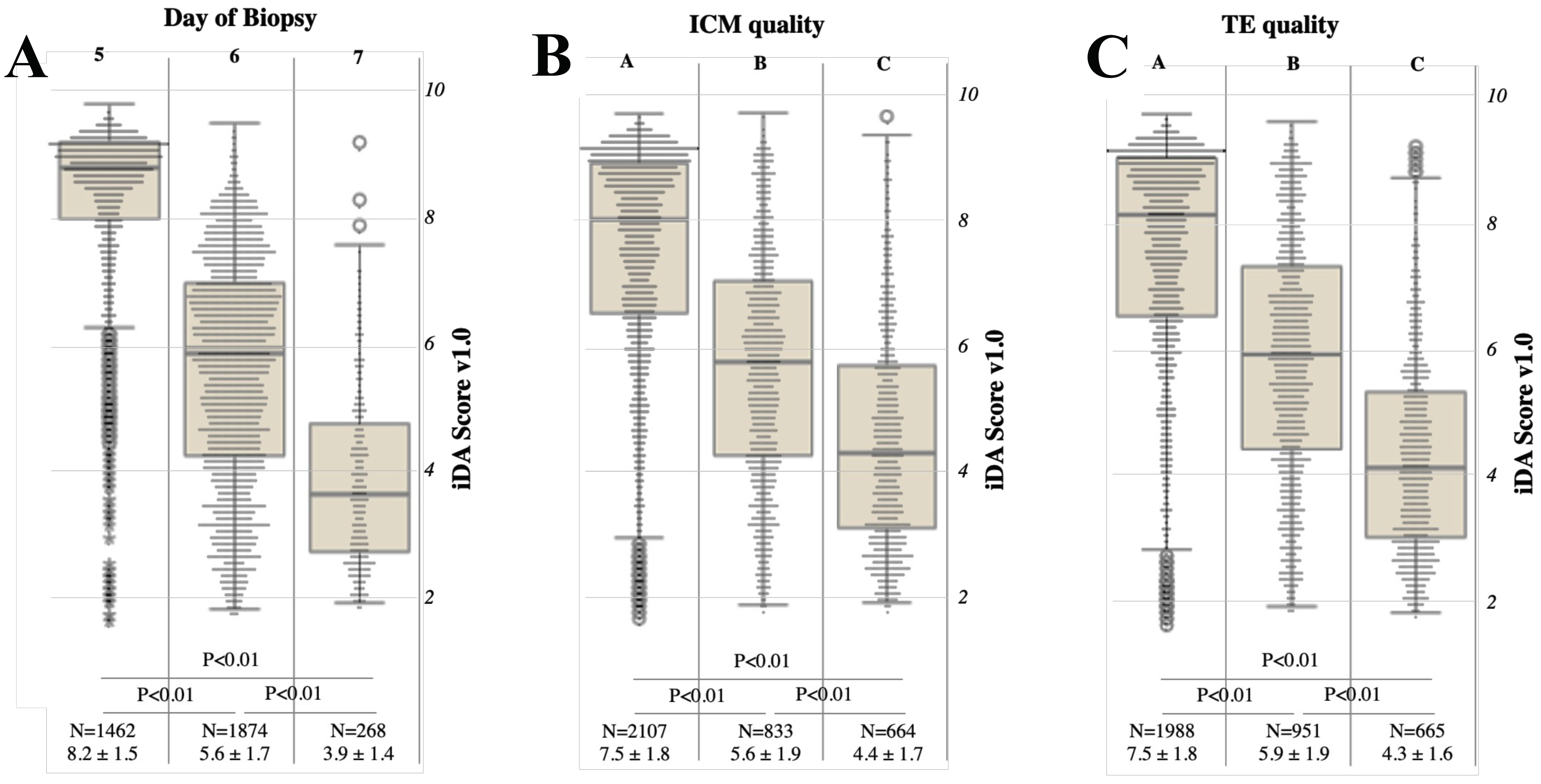
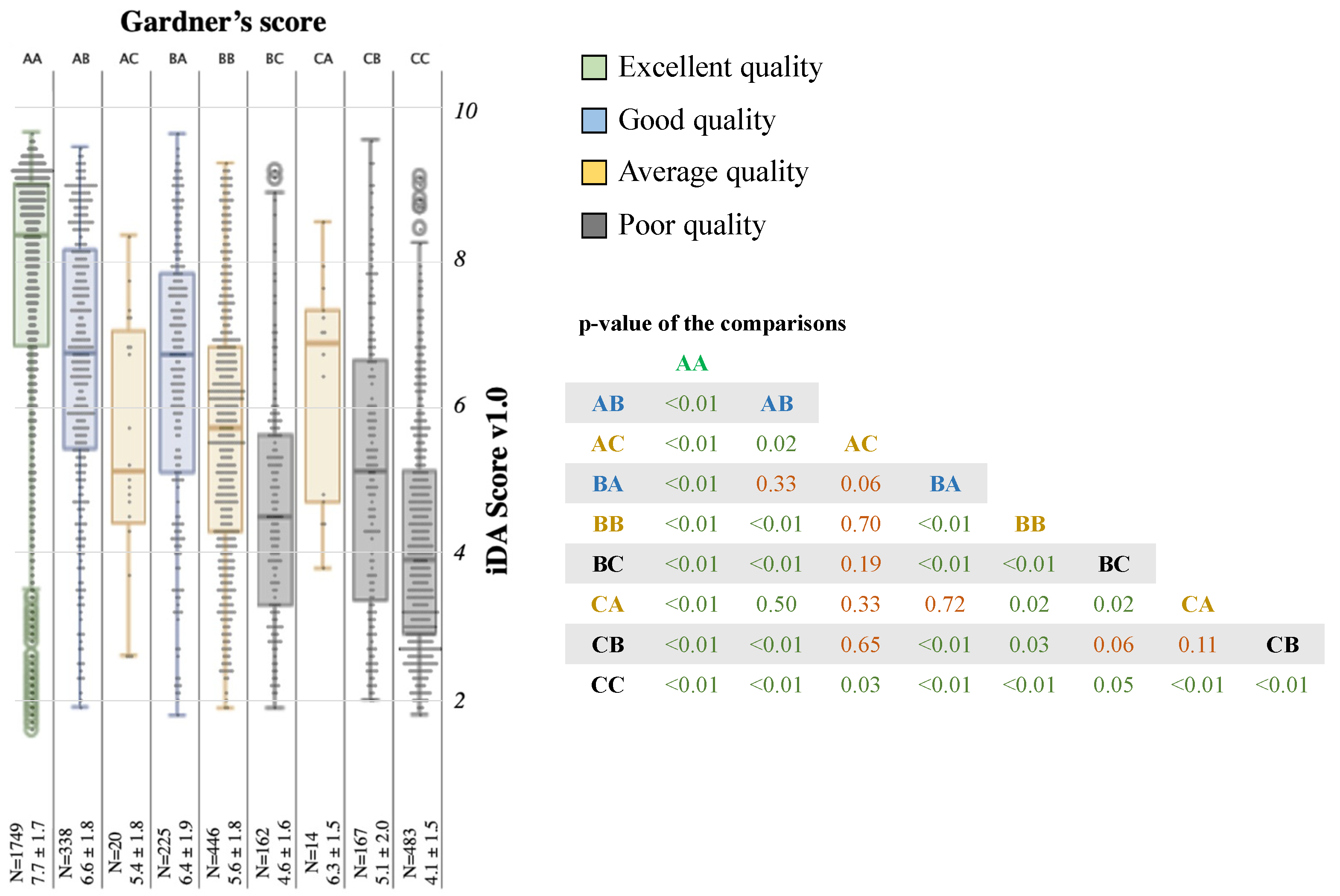
3.2. A Generally Good Association Exists between the Conventional Parameters of Morphological Evaluation and iDAScore v1.0
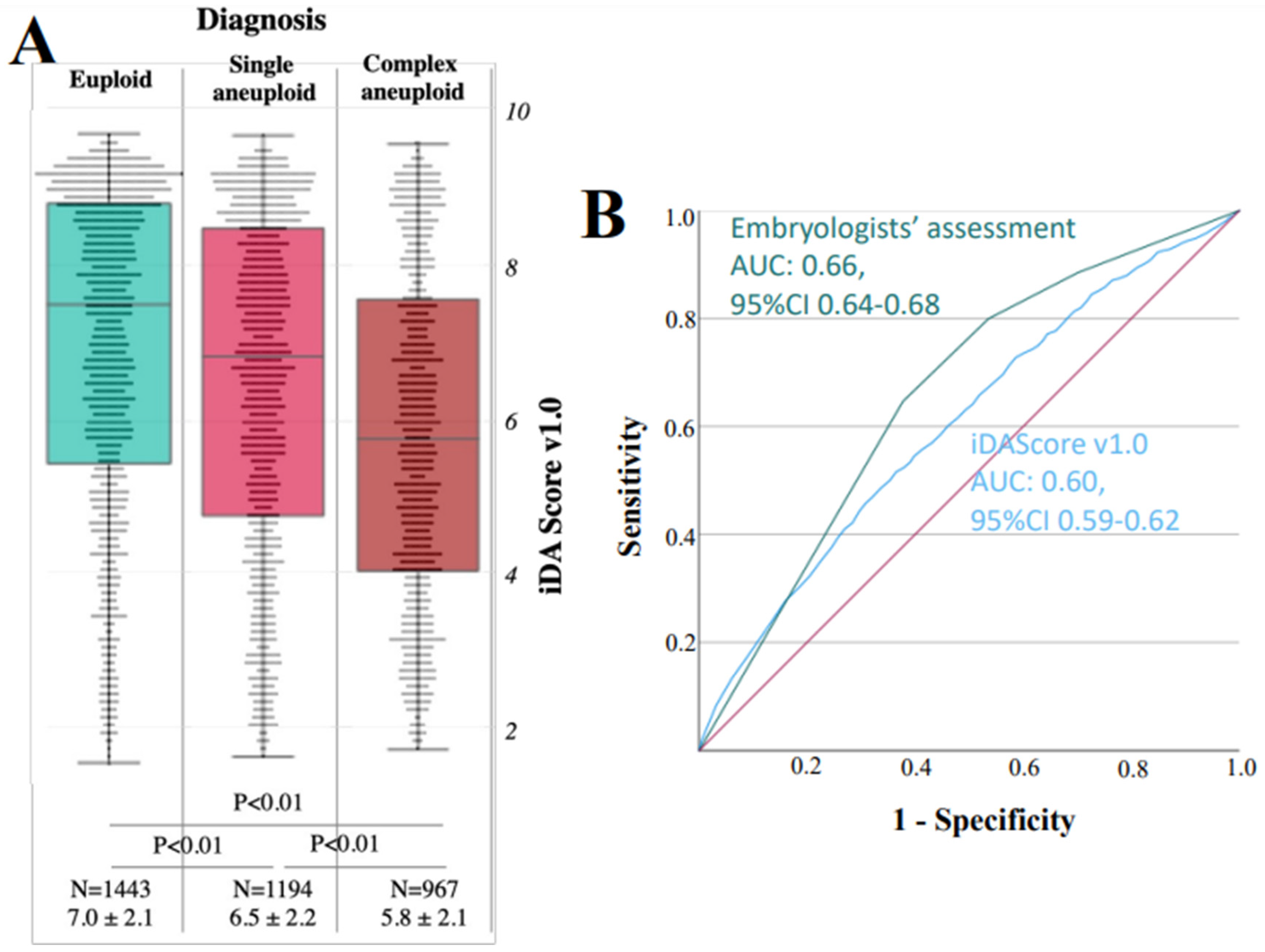
3.3. iDAScore v1.0 Is Significantly Associated with Euploidy, but the AUC Is 0.60
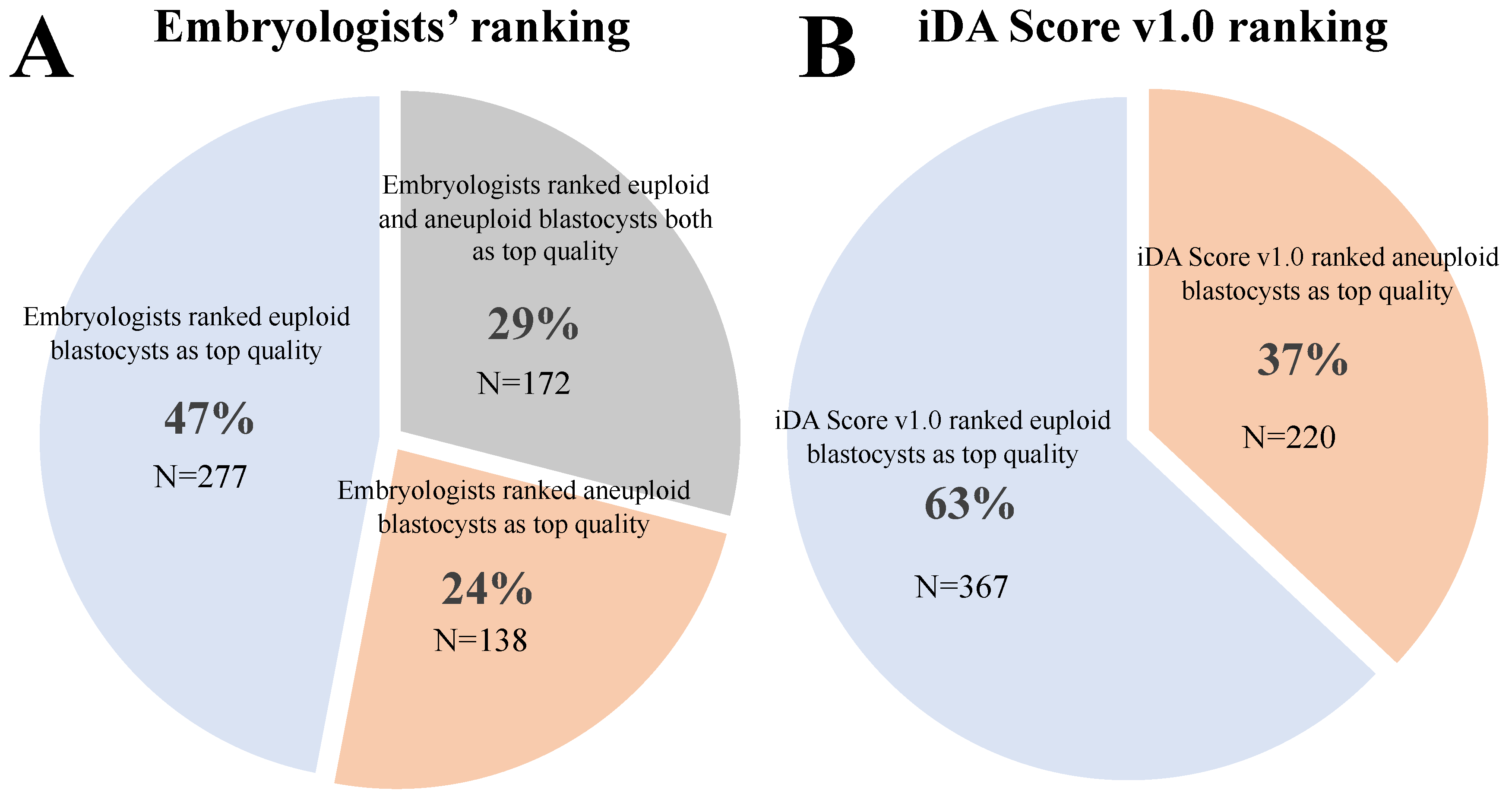
3.4. When Both Euploid and Aneuploid Embryos Were Diagnosed from the Same Cohort, iDAScore v1.0 Ranked the Euploid Blastocyst on Top in 63% of the Cases
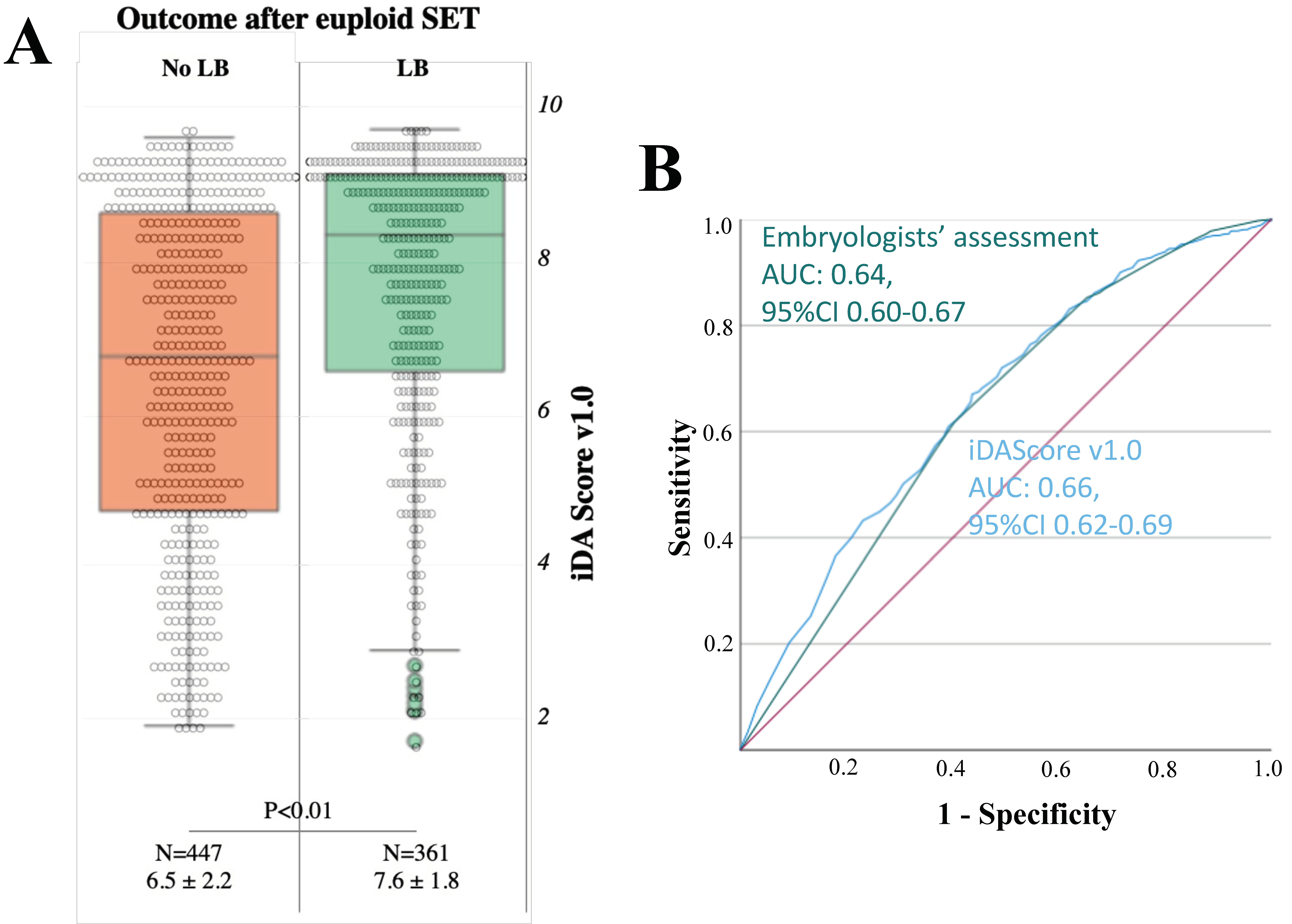
3.5. iDAScore v1.0 Is Significantly Associated with the Achievement of a LB after Euploid Blastocyst SET, with a 0.66 AUC
3.6. When at Least Two Euploid Blastocysts Were Available from the Same Cohort, the Embryologists Would Have often Disagreed with iDAScore v1.0 on Their Ranking
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferraretti, A.; Nygren, K.; Andersen, A.N.; De Mouzon, J.; Kupka, M.; Calhaz-Jorge, C.; Wyns, C.; Gianaroli, L.; Goossens, V.; European IVF-Monitoring Consortium (EIM), for the European Society of Human Reproduction and Embryology (ESHRE); et al. Trends over 15 years in ART in Europe: An analysis of 6 million cycles†. Hum. Reprod. Open 2017, 2017, hox012. [Google Scholar] [CrossRef]
- Rienzi, L.; Cimadomo, D.; Vaiarelli, A.; Gennarelli, G.; Holte, J.; Livi, C.; Masip, M.A.; Uher, P.; Fabozzi, G.; Ubaldi, F.M. Measuring success in IVF is a complex multidisciplinary task: Time for a consensus? Reprod. Biomed. Online 2021, 43, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Alpha Scientists in Reproductive Medicine; ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum. Reprod. 2011, 26, 1270–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, D.K.; Schoolcraft, B. In Vitro Culture of Human Blastocysts, toward Reproductive Certainty: Fertility and Genetics Beyond; Parthenon Publishing London: London, UK, 1999; pp. 378–388. [Google Scholar]
- Glujovsky, D.; Farquhar, C.; Retamar, A.M.Q.; Sedo, C.R.A.; Blake, D. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Syst. Rev. 2016, 5, CD002118. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Q.; Sierra, E.; Malmsten, J.; Ye, Z.; Rosenwaks, Z.; Zaninovic, N. Blastocyst score, a blastocyst quality ranking tool, is a predictor of blastocyst ploidy and implantation potential. F&S Rep. 2020, 1, 133–141. [Google Scholar] [CrossRef]
- Shear, M.A.; Vaughan, D.A.; Modest, A.M.; Seidler, E.A.; Leung, A.Q.; Hacker, M.R.; Sakkas, D.; Penzias, A.S. Blasts from the past: Is morphology useful in PGT-A tested and untested frozen embryo transfers? Reprod. Biomed. Online 2020, 41, 981–989. [Google Scholar] [CrossRef]
- Bamford, T.; Barrie, A.; Montgomery, S.; Dhillon-Smith, R.; Campbell, A.; Easter, C.; Coomarasamy, A. Morphological and morphokinetic associations with aneuploidy: A systematic review and meta-analysis. Hum. Reprod. Update 2022, 28, 656–686. [Google Scholar] [CrossRef]
- Storr, A.; Venetis, C.; Cooke, S.; Kilani, S.; Ledger, W. Inter-observer and intra-observer agreement between embryologists during selection of a single Day 5 embryo for transfer: A multicenter study. Hum. Reprod. 2017, 32, 307–314. [Google Scholar] [CrossRef]
- Paternot, G.; Devroe, J.; Debrock, S.; D’Hooghe, T.M.; Spiessens, C. Intra- and inter-observer analysis in the morphological assessment of early-stage embryos. Reprod. Biol. Endocrinol. 2009, 7, 105. [Google Scholar] [CrossRef] [Green Version]
- Cimadomo, D.; Sosa Fernandez, L.; Soscia, D.; Fabozzi, G.; Benini, F.; Cesana, A.; Dal Canto, M.B.; Maggiulli, R.; Muzzi, S.; Scarica, C.; et al. Inter-centre reliability in embryo grading across several IVF clinics is limited: Implications for embryo selection. Reprod. Biomed. Online 2021, 44, 39–48. [Google Scholar] [CrossRef]
- Coticchio, G.; Barrie, A.; Lagalla, C.; Borini, A.; Fishel, S.; Griffin, D.; Campbell, A. Plasticity of the human preimplantation embryo: Developmental dogmas, variations on themes and self-correction. Hum. Reprod. Update 2021, 27, 848–865. [Google Scholar] [CrossRef]
- Capalbo, A.; Rienzi, L.; Cimadomo, D.; Maggiulli, R.; Elliott, T.; Wright, G.; Nagy, Z.P.; Ubaldi, F.M. Correlation between standard blastocyst morphology, euploidy and implantation: An observational study in two centers involving 956 screened blastocysts. Hum. Reprod. 2014, 29, 1173–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimadomo, D.; Soscia, D.; Casciani, V.; Innocenti, F.; Trio, S.; Chiappetta, V.; Albricci, L.; Maggiulli, R.; Erlich, I.; Ben-Meir, A.; et al. How slow is too slow? A comprehensive portrait of Day 7 blastocysts and their clinical value standardized through artificial intelligence. Hum. Reprod. 2022, 37, 1134–1147. [Google Scholar] [CrossRef] [PubMed]
- Cimadomo, D.; Soscia, D.; Vaiarelli, A.; Maggiulli, R.; Capalbo, A.; Ubaldi, F.M.; Rienzi, L. Looking past the appearance: A comprehensive description of the clinical contribution of poor-quality blastocysts to increase live birth rates during cycles with aneuploidy testing. Hum. Reprod. 2019, 34, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Kemper, J.M.; Liu, Y.; Afnan, M.; Hammond, E.R.; Morbeck, D.E.; Mol, B.W.J. Should we look for a low-grade threshold for blastocyst transfer? A scoping review. Reprod. Biomed. Online 2021, 42, 709–716. [Google Scholar] [CrossRef]
- Morbeck, D.E. Blastocyst culture in the Era of PGS and FreezeAlls: Is a ‘C’ a failing grade? Hum. Reprod. Open 2017, 2017, hox017. [Google Scholar] [CrossRef] [Green Version]
- Cimadomo, D.; Rienzi, L.; Capalbo, A.; Rubio, C.; Innocenti, F.; Garcia-Pascual, C.M.; Ubaldi, F.M.; Handyside, A. The dawn of the future: 30 years from the first biopsy of a human embryo. The detailed history of an ongoing revolution. Hum. Reprod. Update 2020, 26, 453–473. [Google Scholar] [CrossRef]
- Scott, R.T., Jr.; Upham, K.M.; Forman, E.J.; Zhao, T.; Treff, N.R. Cleavage-stage biopsy significantly impairs human embryonic implantation potential while blastocyst biopsy does not: A randomized and paired clinical trial. Fertil. Steril. 2013, 100, 624–630. [Google Scholar] [CrossRef]
- Tiegs, A.W.; Tao, X.; Zhan, Y.; Whitehead, C.; Kim, J.; Hanson, B.; Osman, E.; Kim, T.J.; Patounakis, G.; Gutmann, J.; et al. A multicenter, prospective, blinded, nonselection study evaluating the predictive value of an aneuploid diagnosis using a targeted next-generation sequencing-based preimplantation genetic testing for aneuploidy assay and impact of biopsy. Fertil. Steril. 2020, 115, 627–637. [Google Scholar] [CrossRef]
- Dahdouh, E.M.; Balayla, J.; Garcia-Velasco, J.A. Comprehensive chromosome screening improves embryo selection: A meta-analysis. Fertil. Steril. 2015, 104, 1503–1512. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Wei, S.; Hu, J.; Quan, S. Can Comprehensive Chromosome Screening Technology Improve IVF/ICSI Outcomes? A Meta-Analysis. PLoS ONE 2015, 10, e0140779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apter, S.; Ebner, T.; Freour, T.; Guns, Y.; Kovacic, B.; Le Clef, N.; Marques, M.; Meseguer, M.; Montjean, D.; Sfontouris, I.; et al. Eshre Working group on Time-lapse technology: Good practice recommendations for the use of time-lapse technology. Hum. Reprod. Open 2020, 2020, hoaa008. [Google Scholar] [CrossRef] [PubMed]
- Ciray, H.N.; Campbell, A.; Agerholm, I.E.; Aguilar, J.; Chamayou, S.; Esbert, M.; Sayed, S.; Time-Lapse User, G. Proposed guidelines on the nomenclature and annotation of dynamic human embryo monitoring by a time-lapse user group. Hum. Reprod. 2014, 29, 2650–2660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, S.; Bhide, P.; Jordan, V.; Pacey, A.; Farquhar, C. Time-lapse systems for embryo incubation and assessment in assisted reproduction. Cochrane Database Syst. Rev. 2018, 5, CD011320. [Google Scholar] [CrossRef]
- Pribenszky, C.; Nilselid, A.M.; Montag, M. Time-lapse culture with morphokinetic embryo selection improves pregnancy and live birth chances and reduces early pregnancy loss: A meta-analysis. Reprod. Biomed. Online 2017, 35, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Zaninovic, N.; Irani, M.; Meseguer, M. Assessment of embryo morphology and developmental dynamics by time-lapse microscopy: Is there a relation to implantation and ploidy? Fertil. Steril. 2017, 108, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Rienzi, L.; Capalbo, A.; Stoppa, M.; Romano, S.; Maggiulli, R.; Albricci, L.; Scarica, C.; Farcomeni, A.; Vajta, G.; Ubaldi, F.M. No evidence of association between blastocyst aneuploidy and morphokinetic assessment in a selected population of poor-prognosis patients: A longitudinal cohort study. Reprod. Biomed. Online 2015, 30, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Swain, J.; VerMilyea, M.T.; Meseguer, M.; Ezcurra, D.; Fertility, A.I.F.G. AI in the treatment of fertility: Key considerations. J. Assist. Reprod. Genet. 2020, 37, 2817–2824. [Google Scholar] [CrossRef]
- Riegler, M.A.; Stensen, M.H.; Witczak, O.; Andersen, J.M.; Hicks, S.A.; Hammer, H.L.; Delbarre, E.; Halvorsen, P.; Yazidi, A.; Holst, N.; et al. Artificial intelligence in the fertility clinic: Status, pitfalls and possibilities. Hum. Reprod. 2021, 36, 2429–2442. [Google Scholar] [CrossRef]
- Berntsen, J.; Rimestad, J.; Lassen, J.T.; Tran, D.; Kragh, M.F. Robust and generalizable embryo selection based on artificial intelligence and time-lapse image sequences. PLoS ONE 2022, 17, e0262661. [Google Scholar] [CrossRef]
- Khosravi, P.; Kazemi, E.; Zhan, Q.; Malmsten, J.E.; Toschi, M.; Zisimopoulos, P.; Sigaras, A.; Lavery, S.; Cooper, L.A.D.; Hickman, C.; et al. Deep learning enables robust assessment and selection of human blastocysts after in vitro fertilization. NPJ Digit. Med. 2019, 2, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavez-Badiola, A.; Flores-Saiffe-Farias, A.; Mendizabal-Ruiz, G.; Drakeley, A.J.; Cohen, J. Embryo Ranking Intelligent Classification Algorithm (ERICA): Artificial intelligence clinical assistant predicting embryo ploidy and implantation. Reprod. Biomed. Online 2020, 41, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Kragh, M.F.; Rimestad, J.; Berntsen, J.; Karstoft, H. Automatic grading of human blastocysts from time-lapse imaging. Comput. Biol. Med. 2019, 115, 103494. [Google Scholar] [CrossRef] [PubMed]
- Coticchio, G.; Ezoe, K.; Lagalla, C.; Shimazaki, K.; Ohata, K.; Ninomiya, M.; Wakabayashi, N.; Okimura, T.; Uchiyama, K.; Kato, K.; et al. Perturbations of morphogenesis at the compaction stage affect blastocyst implantation and live birth rates. Hum. Reprod. 2021, 36, 918–928. [Google Scholar] [CrossRef]
- Coticchio, G.; Mignini Renzini, M.; Novara, P.V.; Lain, M.; De Ponti, E.; Turchi, D.; Fadini, R.; Dal Canto, M. Focused time-lapse analysis reveals novel aspects of human fertilization and suggests new parameters of embryo viability. Hum. Reprod. 2018, 33, 23–31. [Google Scholar] [CrossRef]
- Kragh, M.F.; Karstoft, H. Embryo selection with artificial intelligence: How to evaluate and compare methods? J Assist Reprod Genet 2021, 38, 1675–1689. [Google Scholar] [CrossRef]
- Reignier, A.; Lammers, J.; Barriere, P.; Freour, T. Can time-lapse parameters predict embryo ploidy? A systematic review. Reprod. Biomed. Online 2018, 36, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Rienzi, L.; Ubaldi, F.M.; Iacobelli, M.; Minasi, M.G.; Romano, S.; Ferrero, S.; Sapienza, F.; Baroni, E.; Litwicka, K.; Greco, E. Significance of metaphase II human oocyte morphology on ICSI outcome. Fertil. Steril. 2008, 90, 1692–1700. [Google Scholar] [CrossRef]
- Ubaldi, F.M.; Capalbo, A.; Colamaria, S.; Ferrero, S.; Maggiulli, R.; Vajta, G.; Sapienza, F.; Cimadomo, D.; Giuliani, M.; Gravotta, E.; et al. Reduction of multiple pregnancies in the advanced maternal age population after implementation of an elective single embryo transfer policy coupled with enhanced embryo selection: Pre- and post-intervention study. Hum. Reprod. 2015, 30, 2097–2106. [Google Scholar] [CrossRef] [Green Version]
- Cimadomo, D.; Capalbo, A.; Dovere, L.; Tacconi, L.; Soscia, D.; Giancani, A.; Scepi, E.; Maggiulli, R.; Vaiarelli, A.; Rienzi, L.; et al. Leave the past behind: Women’s reproductive history shows no association with blastocysts’ euploidy and limited association with live birth rates after euploid embryo transfers. Hum. Reprod. 2021, 36, 929–940. [Google Scholar] [CrossRef]
- Maggiulli, R.; Cimadomo, D.; Fabozzi, G.; Papini, L.; Dovere, L.; Ubaldi, F.M.; Rienzi, L. The effect of ICSI-related procedural timings and operators on the outcome. Hum. Reprod. 2020, 35, 32–43. [Google Scholar] [CrossRef]
- Maggiulli, R.; Giancani, A.; Cimadomo, D.; Ubaldi, F.M.; Rienzi, L. Human Blastocyst Biopsy and Vitrification. J. Vis. Exp. 2019, 149, e59625. [Google Scholar] [CrossRef] [Green Version]
- Treff, N.R.; Tao, X.; Ferry, K.M.; Su, J.; Taylor, D.; Scott, R.T., Jr. Development and validation of an accurate quantitative real-time polymerase chain reaction-based assay for human blastocyst comprehensive chromosomal aneuploidy screening. Fertil. Steril. 2012, 97, 819–824. [Google Scholar] [CrossRef]
- Garcia-Pascual, C.M.; Navarro-Sanchez, L.; Navarro, R.; Martinez, L.; Jimenez, J.; Rodrigo, L.; Simon, C.; Rubio, C. Optimized NGS Approach for Detection of Aneuploidies and Mosaicism in PGT-A and Imbalances in PGT-SR. Genes 2020, 11, 724. [Google Scholar] [CrossRef] [PubMed]
- Girardi, L.; Serdarogullari, M.; Patassini, C.; Poli, M.; Fabiani, M.; Caroselli, S.; Coban, O.; Findikli, N.; Boynukalin, F.K.; Bahceci, M.; et al. Incidence, Origin, and Predictive Model for the Detection and Clinical Management of Segmental Aneuploidies in Human Embryos. Am. J. Hum. Genet. 2020, 106, 525–534. [Google Scholar] [CrossRef]
- Paulson, R.J.; Treff, N. Isn’t it time to stop calling preimplantation embryos “mosaic”? F&S Rep. 2020, 1, 164–165. [Google Scholar] [CrossRef]
- Forman, E.J. Demystifying "mosaic" outcomes. Fertil. Steril. 2019, 111, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capalbo, A.; Poli, M.; Rienzi, L.; Girardi, L.; Patassini, C.; Fabiani, M.; Cimadomo, D.; Benini, F.; Farcomeni, A.; Cuzzi, J.; et al. Mosaic human preimplantation embryos and their developmental potential in a prospective, non-selection clinical trial. Am. J. Hum. Genet. 2021, 108, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.; Cooke, S.; Illingworth, P.J.; Gardner, D.K. Deep learning as a predictive tool for fetal heart pregnancy following time-lapse incubation and blastocyst transfer. Hum. Reprod. 2019, 34, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Alikani, M.; Go, K.J.; McCaffrey, C.; McCulloh, D.H. Comprehensive evaluation of contemporary assisted reproduction technology laboratory operations to determine staffing levels that promote patient safety and quality care. Fertil. Steril. 2014, 102, 1350–1356. [Google Scholar] [CrossRef]
- Veiga, E.; Olmedo, C.; Sanchez, L.; Fernandez, M.; Mauri, A.; Ferrer, E.; Ortiz, N. Recalculating the staff required to run a modern assisted reproductive technology laboratory. Hum. Reprod. 2022, 37, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Ezoe, K.; Shimazaki, K.; Miki, T.; Takahashi, T.; Tanimura, Y.; Amagai, A.; Sawado, A.; Akaike, H.; Mogi, M.; Kaneko, S.; et al. Association between a deep learning-based scoring system with morphokinetics and morphological alterations in human embryos. Reprod. Biomed. Online 2022, 45, 1124–1132. [Google Scholar] [CrossRef]
- Ahlstrom, A.; Westin, C.; Wikland, M.; Hardarson, T. Prediction of live birth in frozen-thawed single blastocyst transfer cycles by pre-freeze and post-thaw morphology. Hum. Reprod. 2013, 28, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.J.; Richter, K.S.; Heitmann, R.J.; Graham, J.R.; Tucker, M.J.; DeCherney, A.H.; Browne, P.E.; Levens, E.D. Trophectoderm grade predicts outcomes of single-blastocyst transfers. Fertil. Steril. 2013, 99, 1283–1289.e1281. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, J.; Wu, X.; Cao, S.; Zhou, L.; Wang, Y.; Chen, X.; Lu, J.; Zhao, C.; Chen, M.; et al. Trophectoderm morphology predicts outcomes of pregnancy in vitrified-warmed single-blastocyst transfer cycle in a Chinese population. J. Assist. Reprod. Genet. 2014, 31, 1475–1481. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.M.; Onwubalili, N.; Brown, K.; Jindal, S.K.; McGovern, P.G. Blastocyst expansion score and trophectoderm morphology strongly predict successful clinical pregnancy and live birth following elective single embryo blastocyst transfer (eSET): A national study. J. Assist. Reprod. Genet. 2013, 30, 1577–1581. [Google Scholar] [CrossRef] [Green Version]
- Honnma, H.; Baba, T.; Sasaki, M.; Hashiba, Y.; Ohno, H.; Fukunaga, T.; Endo, T.; Saito, T.; Asada, Y. Trophectoderm morphology significantly affects the rates of ongoing pregnancy and miscarriage in frozen-thawed single-blastocyst transfer cycle in vitro fertilization. Fertil. Steril. 2012, 98, 361–367. [Google Scholar] [CrossRef]
- Ahlstrom, A.; Westin, C.; Reismer, E.; Wikland, M.; Hardarson, T. Trophectoderm morphology: An important parameter for predicting live birth after single blastocyst transfer. Hum. Reprod. 2011, 26, 3289–3296. [Google Scholar] [CrossRef] [Green Version]
- Hammond, E.R.; Foong, A.K.M.; Rosli, N.; Morbeck, D.E. Should we freeze it? Agreement on fate of borderline blastocysts is poor and does not improve with a modified blastocyst grading system. Hum. Reprod. 2020, 35, 1045–1053. [Google Scholar] [CrossRef]
- Lassen, J.T.; Kragh, M.F.; Rimestad, J.; Johansen, M.N.; Berntsen, J. Development and validation of deep learning based embryo selection across multiple days of transfer. arXiv 2022. [Google Scholar] [CrossRef]
- Capalbo, A.; Poli, M.; Jalas, C.; Forman, E.J.; Treff, N.R. On the reproductive capabilities of aneuploid human preimplantation embryos. Am. J. Hum. Genet. 2022, 109, 1572–1581. [Google Scholar] [CrossRef] [PubMed]
- Gazzo, E.; Pena, F.; Valdez, F.; Chung, A.; Bonomini, C.; Ascenzo, M.; Velit, M.; Escudero, E. The Kidscore(TM) D5 algorithm as an additional tool to morphological assessment and PGT-A in embryo selection: A time-lapse study. JBRA Assist. Reprod. 2020, 24, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Diakiw, S.M.; Hall, J.M.M.; VerMilyea, M.; Lim, A.Y.X.; Quangkananurug, W.; Chanchamroen, S.; Bankowski, B.; Stones, R.; Storr, A.; Miller, A.; et al. An artificial intelligence model correlated with morphological and genetic features of blastocyst quality improves ranking of viable embryos. Reprod. Biomed. Online 2022, 45, 1105–1117. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Tan, W.; Li, Z.; Jin, L. An artificial intelligence model (euploid prediction algorithm) can predict embryo ploidy status based on time-lapse data. Reprod. Biol. Endocrinol. 2021, 19, 185. [Google Scholar] [CrossRef]
- Kato, K.; Ueno, S.; Berntsen, J.; Kragh, M.F.; Okimura, T.; Kuroda, T. Does embryo categorization by existing artificial intelligence, morphokinetic or morphological embryo selection models correlate with blastocyst euploidy rates? Reprod. Biomed. Online 2022, 46, 274–281. [Google Scholar] [CrossRef]
- Ueno, S.; Berntsen, J.; Ito, M.; Okimura, T.; Kato, K. Correlation between an annotation-free embryo scoring system based on deep learning and live birth/neonatal outcomes after single vitrified-warmed blastocyst transfer: A single-centre, large-cohort retrospective study. J. Assist. Reprod. Genet. 2022, 39, 2089–2099. [Google Scholar] [CrossRef]
- Liao, Q.; Zhang, Q.; Feng, X.; Huang, H.; Xu, H.; Tian, B.; Liu, J.; Yu, Q.; Guo, N.; Liu, Q.; et al. Development of deep learning algorithms for predicting blastocyst formation and quality by time-lapse monitoring. Commun. Biol. 2021, 4, 415. [Google Scholar] [CrossRef]
- Barnes, J.; Brendel, M.; Gao, V.R.; Rajendran, S.; Kim, J.; Li, Q.; Malmsten, J.E.; Sierra, J.T.; Zisimopoulos, P.; Sigaras, A.; et al. A non-invasive artificial intelligence approach for the prediction of human blastocyst ploidy: A retrospective model development and validation study. Lancet Digit. Health 2023, 5, e28–e40. [Google Scholar] [CrossRef]
- Rocafort, E.; Enciso, M.; Leza, A.; Sarasa, J.; Aizpurua, J. Euploid embryos selected by an automated time-lapse system have superior SET outcomes than selected solely by conventional morphology assessment. J. Assist. Reprod. Genet. 2018, 35, 1573–1583. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome: euploidy | UnivariateOR, 95% CI, p-value | Multivariate-OR, 95% CI, p-value |
| Maternal age | 0.82, 95% CI 0.8–0.84, p < 0.01 | 0.82, 95% CI 0.8–0.84, p < 0.01 |
| iDAScore v1.0 | 1.18, 95% CI 1.14–1.22, p < 0.01 | 1.18, 95% CI 1.14–1.22, p < 0.01 |
| Outcome: LB per euploid SET | Univariate OR, 95% CI, p-value | - |
| iDAScore v1.0 | 1.30, 95% CI 1.2–1.4, p < 0.01 | - |
| Outcome: euploidy | Univariate OR, 95% CI, p-value | Multivariate OR, 95% CI, p-value |
| Maternal age | 0.82, 95% CI 0.8–0.84, p < 0.01 | 0.82, 95% CI 0.8–0.84, p < 0.01 |
| Blastocyst quality: | ||
| AA | - | - |
| AB, BA | 0.57, 95% CI 0.47–0.69, p < 0.01 | 0.57, 95% CI 0.47–0.71, p < 0.01 |
| BB, AC, CA | 0.30, 95% CI 0.24–0.38, p < 0.01 | 0.32, 95% CI 0.25–0.40, p < 0.01 |
| CC, BC, CA | 0.23, 95% CI 0.19–0.27, p < 0.01 | 0.25, 95% CI 0.2–0.31, p < 0.01 |
| Day of biopsy: | ||
| 5 | - | - |
| 6 | 0.62, 95% CI 0.54–0.72, p < 0.01 | 1.02, 95% CI 0.87–1.2, p = 0.81 |
| 7 | 0.34, 95% CI 0.25–0.45, p < 0.01 | 0.78, 95% CI 0.55–1.1, p = 0.16 |
| Outcome: LB per euploid SET | Univariate OR, 95% CI, p-value | Multivariate OR, 95% CI, p-value |
| Blastocyst quality: | ||
| AA | - | - |
| AB, BA | 0.61, 95% CI 0.40–0.94, p = 0.02 | 0.72, 95% CI 0.46–1.11, p = 0.14 |
| BB, AC, CA | 0.39, 95% CI 0.22–0.70, p < 0.01 | 0.50, 95% CI 0.28–0.90, p = 0.02 |
| CC, BC, CA | 0.18, 95% CI 0.09–0.35, p < 0.01 | 0.24, 95% CI 0.12–0.47, p < 0.01 |
| Day of biopsy: | ||
| 5 | - | - |
| 6 | 0.48, 95% CI 0.36–0.64, p < 0.01 | 0.59, 95% CI 0.44–0.81, p < 0.01 |
| 7 | 0.26, 95% CI 0.11–0.63, p < 0.01 | 0.47, 95% CI 0.19–1.18, p = 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimadomo, D.; Chiappetta, V.; Innocenti, F.; Saturno, G.; Taggi, M.; Marconetto, A.; Casciani, V.; Albricci, L.; Maggiulli, R.; Coticchio, G.; et al. Towards Automation in IVF: Pre-Clinical Validation of a Deep Learning-Based Embryo Grading System during PGT-A Cycles. J. Clin. Med. 2023, 12, 1806. https://doi.org/10.3390/jcm12051806
Cimadomo D, Chiappetta V, Innocenti F, Saturno G, Taggi M, Marconetto A, Casciani V, Albricci L, Maggiulli R, Coticchio G, et al. Towards Automation in IVF: Pre-Clinical Validation of a Deep Learning-Based Embryo Grading System during PGT-A Cycles. Journal of Clinical Medicine. 2023; 12(5):1806. https://doi.org/10.3390/jcm12051806
Chicago/Turabian StyleCimadomo, Danilo, Viviana Chiappetta, Federica Innocenti, Gaia Saturno, Marilena Taggi, Anabella Marconetto, Valentina Casciani, Laura Albricci, Roberta Maggiulli, Giovanni Coticchio, and et al. 2023. "Towards Automation in IVF: Pre-Clinical Validation of a Deep Learning-Based Embryo Grading System during PGT-A Cycles" Journal of Clinical Medicine 12, no. 5: 1806. https://doi.org/10.3390/jcm12051806