


Intrauterine Infusion of Leukocyte-Poor Platelet-Rich Plasma Is an Effective Therapeutic Protocol for Patients with Recurrent Implantation Failure: A Retrospective Cohort Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. PRP Preparation
2.3. FET Protocol
2.4. PRP Administration Technique
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Margalioth, E.J.; Ben-Chetrit, A.; Gal, M.; Eldar-Geva, T. Investigation and treatment of repeated implantation failure following IVF-ET. Hum. Reprod. (Oxf. Engl.) 2006, 21, 3036–3043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busnelli, A.; Reschini, M.; Cardellicchio, L.; Vegetti, W.; Somigliana, E.; Vercellini, P. How common is real repeated implantation failure? An indirect estimate of the prevalence. Reprod. Biomed. Online 2020, 40, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coughlan, C.; Ledger, W.; Wang, Q.; Liu, F.; Demirol, A.; Gurgan, T.; Cutting, R.; Ong, K.; Sallam, H.; Li, T.C. Recurrent implantation failure: Definition and management. Reprod. Biomed. Online 2014, 28, 14–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polanski, L.T.; Baumgarten, M.N.; Quenby, S.; Brosens, J.; Campbell, B.K.; Raine-Fenning, N.J. What exactly do we mean by ‘recurrent implantation failure’? A systematic review and opinion. Reprod. Biomed. Online 2014, 28, 409–423. [Google Scholar] [CrossRef] [Green Version]
- Das, M.; Holzer, H.E. Recurrent implantation failure: Gamete and embryo factors. Fertil. Steril. 2012, 97, 1021–1027. [Google Scholar] [CrossRef]
- Hviid, M.M.; Macklon, N. Immune modulation treatments-where is the evidence? Fertil. Steril. 2017, 107, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Coksuer, H.; Akdemir, Y.; Ulas Barut, M. Improved in vitro fertilization success and pregnancy outcome with autologous platelet-rich plasma treatment in unexplained infertility patients that had repeated implantation failure history. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2019, 35, 815–818. [Google Scholar] [CrossRef]
- Nobijari, F.F.; Arefi, S.S.; Moini, A.; Taheripanah, R.; Fazeli, E.; Kharazi, H.; Hosseini, S.Z.; Hosseini, A.; Valojerdi, M.R.; Copin, H.; et al. Endometrium immunomodulation by intrauterine insemination administration of treated peripheral blood mononuclear cell prior frozen/thawed embryos in patients with repeated implantation failure. Zygote (Camb. Engl.) 2019, 27, 214–218. [Google Scholar] [CrossRef]
- Katzorke, N.; Vilella, F.; Ruiz, M.; Krüssel, J.S.; Simón, C. Diagnosis of Endometrial-Factor Infertility: Current Approaches and New Avenues for Research. Geburtshilfe Und Frauenheilkd. 2016, 76, 699–703. [Google Scholar] [CrossRef] [Green Version]
- Ramaswamy Reddy, S.H.; Reddy, R.; Babu, N.C.; Ashok, G.N. Stem-cell therapy and platelet-rich plasma in regenerative medicines: A review on pros and cons of the technologies. J. Oral Maxillofac. Pathol. JOMFP 2018, 22, 367–374. [Google Scholar] [CrossRef]
- Whitney, K.E.; Liebowitz, A.; Bolia, I.K.; Chahla, J.; Ravuri, S.; Evans, T.A.; Philippon, M.J.; Huard, J. Current perspectives on biological approaches for osteoarthritis. Ann. N. Y. Acad. Sci. 2017, 1410, 26–43. [Google Scholar] [CrossRef]
- Zhang, M.; Park, G.; Zhou, B.; Luo, D. Applications and efficacy of platelet-rich plasma in dermatology: A clinical review. J. Cosmet. Dermatol. 2018, 17, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Samadi, P.; Sheykhhasan, M.; Khoshinani, H.M. The Use of Platelet-Rich Plasma in Aesthetic and Regenerative Medicine: A Comprehensive Review. Aesthetic Plast. Surg. 2019, 43, 803–814. [Google Scholar] [CrossRef] [PubMed]
- Krüger, J.P.; Freymannx, U.; Vetterlein, S.; Neumann, K.; Endres, M.; Kaps, C. Bioactive factors in platelet-rich plasma obtained by apheresis. Transfus. Med. Hemotherapy Off. Organ Der Dtsch. Ges. Fur Transfus. Und Immunhamatol. 2013, 40, 432–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Li, J.; Chen, Y.; Wei, L.; Yang, X.; Shi, Y.; Liang, X. Autologous platelet-rich plasma promotes endometrial growth and improves pregnancy outcome during in vitro fertilization. Int. J. Clin. Exp. Med. 2015, 8, 1286–1290. [Google Scholar] [PubMed]
- Amable, P.R.; Carias, R.B.; Teixeira, M.V.; da Cruz Pacheco, I.; Corrêa do Amaral, R.J.; Granjeiro, J.M.; Borojevic, R. Platelet-rich plasma preparation for regenerative medicine: Optimization and quantification of cytokines and growth factors. Stem Cell Res. Ther. 2013, 4, 67. [Google Scholar] [CrossRef] [Green Version]
- Nazari, L.; Salehpour, S.; Hoseini, S.; Zadehmodarres, S.; Ajori, L. Effects of autologous platelet-rich plasma on implantation and pregnancy in repeated implantation failure: A pilot study. Int. J. Reprod. Biomed. 2016, 14, 625–628. [Google Scholar] [CrossRef] [Green Version]
- Tehraninejad, E.S.; Kashani, N.G.; Hosseini, A.; Tarafdari, A. Autologous platelet-rich plasma infusion does not improve pregnancy outcomes in frozen embryo transfer cycles in women with history of repeated implantation failure without thin endometrium. J. Obstet. Gynaecol. Res. 2021, 47, 147–151. [Google Scholar] [CrossRef]
- Oudelaar, B.W.; Peerbooms, J.C.; Huis In ’t Veld, R.; Vochteloo, A.J.H. Concentrations of Blood Components in Commercial Platelet-Rich Plasma Separation Systems: A Review of the Literature. Am. J. Sport. Med. 2019, 47, 479–487. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, Y.B.; Ha, C.W.; Roh, Y.J.; Park, J.G. Adverse Reactions and Clinical Outcomes for Leukocyte-Poor Versus Leukocyte-Rich Platelet-Rich Plasma in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sport. Med. 2021, 9, 23259671211011948. [Google Scholar] [CrossRef]
- Zhao, D.; Han, Y.H.; Pan, J.K.; Yang, W.Y.; Zeng, L.F.; Liang, G.H.; Liu, J. The clinical efficacy of leukocyte-poor platelet-rich plasma in arthroscopic rotator cuff repair: A meta-analysis of randomized controlled trials. J. Shoulder Elb. Surg. 2021, 30, 918–928. [Google Scholar] [CrossRef]
- Noushin, M.A.; Ashraf, M.; Thunga, C.; Singh, S.; Basheer, R.; Ashraf, R.; Jayaprakasan, K. A comparative evaluation of subendometrial and intrauterine platelet-rich plasma treatment for women with recurrent implantation failure. F&S Sci. 2021, 2, 295–302. [Google Scholar] [CrossRef]
- Professional Committee of Clinical Transfusion Management. Chinese Blood Transfusion Association. Expert consensus on the technical preparation of autologous platelet-rich plasma. Chin. J. Blood Transfus. 2021, 31, 677–683. [Google Scholar]
- Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Reprod. Biomed. Online 2011, 22, 632–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, D.K.; Schoolcraft, W.B. Culture and transfer of human blastocysts. Curr. Opin. Obstet. Gynecol. 1999, 11, 307–311. [Google Scholar] [CrossRef]
- Wen, J.; Li, H.T.; Li, S.H.; Li, X.; Duan, J.M. Investigation of modified platelet-rich plasma (mPRP) in promoting the proliferation and differentiation of dental pulp stem cells from deciduous teeth. Braz. J. Med. Biol. Res. = Rev. Bras. De Pesqui. Med. E Biol. 2016, 49, e5373. [Google Scholar] [CrossRef] [Green Version]
- Fatemi, H.M.; Popovic-Todorovic, B. Implantation in assisted reproduction: A look at endometrial receptivity. Reprod. Biomed. Online 2013, 27, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Kang, Y.; Wang, Q.; Yan, L. Efficacy of Autologous Intrauterine Infusion of Platelet-Rich Plasma in Patients with Unexplained Repeated Implantation Failures in Embryo Transfer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6753. [Google Scholar] [CrossRef]
- Enatsu, Y.; Enatsu, N.; Kishi, K.; Otsuki, J.; Iwasaki, T.; Okamoto, E.; Kokeguchi, S.; Shiotani, M. Clinical outcome of intrauterine infusion of platelet-rich plasma in patients with recurrent implantation failure. Reprod. Med. Biol. 2022, 21, e12417. [Google Scholar] [CrossRef]
- Bakhsh, A.S.; Maleki, N.; Sadeghi, M.R.; SadeghiTabar, A.; Tavakoli, M.; Zafardoust, S.; Karimi, A.; Askari, S.; Jouhari, S.; Mohammadzadeh, A. Effects of Autologous Platelet-Rich Plasma in women with repeated implantation failure undergoing assisted reproduction. JBRA Assist. Reprod. 2022, 26, 84–87. [Google Scholar] [CrossRef]
- Obidniak, D.; Gzgzyan, A.; Feoktistov, A.; Niauri, D. Randomized controlled trial evaluating efficacy of autologous platelet -rich plasma therapy for patients with recurrent implantation failure. Fertil. Steril. 2017, 108, e370. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Boffa, A.; Andriolo, L.; Romandini, I.; Altamura, S.A.; Cenacchi, A.; Roverini, V.; Zaffagnini, S.; Filardo, G. Leukocyte-Rich versus Leukocyte-Poor Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis: A Double-Blind Randomized Trial. Am. J. Sport. Med. 2022, 50, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Dhurat, R.; Sukesh, M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J. Cutan. Aesthetic Surg. 2014, 7, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Boswell, S.G.; Schnabel, L.V.; Mohammed, H.O.; Sundman, E.A.; Minas, T.; Fortier, L.A. Increasing platelet concentrations in leukocyte-reduced platelet-rich plasma decrease collagen gene synthesis in tendons. Am. J. Sport. Med. 2014, 42, 42–49. [Google Scholar] [CrossRef]
- Maleki-Hajiagha, A.; Razavi, M.; Rouholamin, S.; Rezaeinejad, M.; Maroufizadeh, S.; Sepidarkish, M. Intrauterine infusion of autologous platelet-rich plasma in women undergoing assisted reproduction: A systematic review and meta-analysis. J. Reprod. Immunol. 2020, 137, 103078. [Google Scholar] [CrossRef]
- Liu, K.; Cheng, H.; Guo, Y.; Liu, Y.; Li, L.; Zhang, X. Autologous platelet-rich plasma intrauterine perfusion to improve pregnancy outcomes after implantation failure: A systematic review and meta-analysis. J. Obstet. Gynaecol. Res. 2022, 48, 3137–3151. [Google Scholar] [CrossRef]
- Hajipour, H.; Nejabati, H.R.; Latifi, Z.; Hamdi, K.; Bahrami-Asl, Z.; Fattahi, A.; Nouri, M. Lymphocytes immunotherapy for preserving pregnancy: Mechanisms and Challenges. Am. J. Reprod. Immunol. 2018, 80, e12853. [Google Scholar] [CrossRef]
- Liang, P.Y.; Diao, L.H.; Huang, C.Y.; Lian, R.C.; Chen, X.; Li, G.G.; Zhao, J.; Li, Y.Y.; He, X.B.; Zeng, Y. The pro-inflammatory and anti-inflammatory cytokine profile in peripheral blood of women with recurrent implantation failure. Reprod. Biomed. Online 2015, 31, 823–826. [Google Scholar] [CrossRef] [Green Version]
- Pantos, K.; Grigoriadis, S.; Maziotis, E.; Pistola, K.; Xystra, P.; Pantou, A.; Kokkali, G.; Pappas, A.; Lambropoulou, M.; Sfakianoudis, K.; et al. The Role of Interleukins in Recurrent Implantation Failure: A Comprehensive Review of the Literature. Int. J. Mol. Sci. 2022, 23, 2198. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | PRP Group (n = 64) | Non-PRP Treatment Group (n = 54) | p-Value |
|---|---|---|---|
| Age (years) | 32.04 ± 4.36 | 32.22 ± 4.31 | 0.916 |
| BMI (kg/m2) | 20.69 ± 4.36 | 22.52 ± 2.99 | 0.713 |
| AMH (ng/mL) | 4.61 (2.25, 7.31) | 4.49 (2.64, 7.32) | 0.884 |
| Basal FSH (U/L) | 6.64 ± 3.21 | 5.78 ± 2.27 | 0.236 |
| Basal LH (mIU/mL) | 5.19 (3.34, 10.43) | 5.12 (3.39, 6.93) | 0.223 |
| Basal E2 (pg/mL) | 75.26 (44.25, 124.5) | 67.06 (44.92, 103.8) | 0.461 |
| Basal progesterone (ng/mL) | 0.59 (0.36, 0.91) | 0.53 (0.36, 0.76) | 0.746 |
| Diagnosis of infertility | |||
| Tubal factors | 41 (64.1%) | 37 (68.5%) | 0.697 |
| Polycystic ovary syndrome | 18 (28.1%) | 14 (25.9%) | 0.838 |
| Unexplained infertility | 5 (7.8%) | 3 (5.6%) | 0.725 |
| Duration of infertility (years) | 3 (2,4) | 3.5 (2,5) | 0.310 |
| No. of the blastocyst-stage embryos transferred | 40 (62.5%) | 34 (63.0%) | 1.000 |
| No. of the cleavage-stage embryos transferred | 24 (37.5%) | 20 (37.0%) | 1.000 |
| No. of previous ET attempts | 3 (3, 4) | 3 (3, 4) | 0.826 |
| Endometrial thickness before first PRP infusion (mm) | 10.88 ± 1.83 | 10.95 ± 1.66 | 0.795 |
| Endometrial thickness on the ET day after two PRP infusions (mm) | 11.64 ± 2.06 | 11.29 ± 1.76 | 0.366 |
| Variables | PRP Group (n = 40) | Non-PRP Treatment Group (n = 34) | p-Value |
|---|---|---|---|
| Age (years) | 31.53 ± 4.03 | 32.0 ± 4.20 | 0.806 |
| BMI (kg/m2) | 23.23 ± 3.25 | 22.76 ± 3.12 | 0.398 |
| AMH (ng/mL) | 5.07 (2.58, 7.39) | 3.76 (2.87, 6.74) | 0.488 |
| Basal FSH (U/L) | 6.06 ± 2.24 | 5.44 ± 2.21 | 0.392 |
| Basal LH (mIU/mL) | 5 (3.34, 10.12) | 4.64 (3.49, 6.59) | 0.368 |
| Basal E2 (pg/mL) | 93.33 (47.95, 149.25) | 68 (43.84, 109.65) | 0.300 |
| Basal progesterone (ng/mL) | 0.57 ± 0.24 | 0.52 ± 0.22 | 0.428 |
| Duration of infertility (years) | 3 (2, 4) | 3 (2, 5) | 0.332 |
| No. of previous ET attempts | 3 (3, 4) | 3 (3, 4) | 0.825 |
| No. of oocytes retrieved | 15.18 ± 1.25 | 14.18 ± 0.93 | 0.276 |
| No. of available embryos | 8.32 ± 0.72 | 9.21 ± 0.67 | 0.135 |
| No. of good-quality embryos | 5.68 ± 0.38 | 5.59 ± 0.32 | 0.491 |
| No. of blastocysts transferred | 0.218 | ||
| 1 | 15 (37.5%) | 8 (23.5%) | |
| 2 | 25 (62.5%) | 26 (76.5%) | |
| Endometrial thickness before first PRP infusion (mm) | 10.84 ± 2.00 | 11.34 ± 1.59 | 0.159 |
| Endometrial thickness on the ET day after two PRP infusions (mm) | 11.72 ± 2.09 | 11.63 ± 1.62 | 0.905 |
| No. of good-quality BSE (grade A or B) transferred per ET cycle | 1 (1, 1) | 2 (1, 2) | 0.030 * |
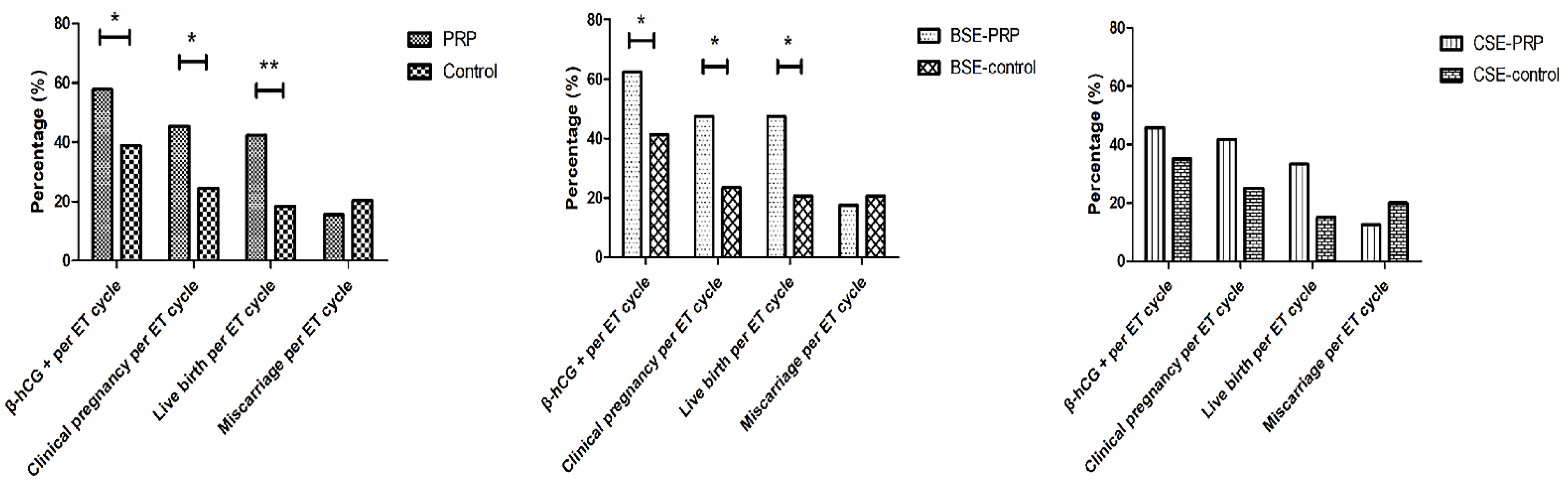
| β-hCG+ per ET cycle | 26 (65.0%) | 14 (41.2%) | 0.040 * |
| Clinical pregnancy per ET cycle | 19 (47.5%) | 8 (23.5%) | 0.033 * |
| Live birth per ET cycle | 19 (47.5%) | 7 (20.6%) | 0.027 * |
| Miscarriage per ET cycle | 7 (17.5%) | 7 (20.6%) | 0.773 |
| Variables | PRP Group (n = 24) | Non-PRP Treatment Group (n = 20) | p-Value |
|---|---|---|---|
| Age (years) | 32.90 ± 4.86 | 32.60 ± 4.57 | 0.822 |
| BMI (kg/m2) | 21.42 ± 2.85 | 22.11 ± 2.78 | 0.706 |
| AMH (ng/mL) | 4.90 ± 3.72 | 5.68 ± 3.32 | 0.234 |
| Basal FSH (U/L) | 7.81 ± 4.15 | 6.36 ± 2.31 | 0.340 |
| Basal LH (mIU/mL) | 7.51 ± 4.31 | 5.43 ± 2.41 | 0.248 |
| Basal E2 (pg/mL) | 67.63 ± 52.17 | 72.28 ± 38.45 | 0.777 |
| Basal progesterone (ng/mL) | 0.58 ± 0.32 | 0.56 ± 0.24 | 0.925 |
| Duration of infertility (years) | 4.53 ± 2.23 | 4.15 ± 2.21 | 0.693 |
| No. of previous ET attempts | 3.5 (3, 4) | 3.5 (3, 4.75) | 0.969 |
| Endometrial thickness before first PRP infusion (mm) | 11.02 ± 1.56 | 10.29 ± 1.61 | 0.147 |
| Endometrial thickness on the ET day after two PRP infusions (mm) | 11.51 ± 2.04 | 10.71 ± 1.88 | 0.167 |
| No. of oocytes retrieved | 14.40 ± 2.21 | 11.95 ± 1.16 | 0.759 |
| No. of available embryos | 6.75 ± 0.82 | 7.70 ± 0.69 | 0.234 |
| No. of good-quality embryos | 3.60 ± 0.15 | 3.45 ± 0.13 | 0.433 |
| No. of grade I embryos transferred per ET cycle | 0 (0, 1) | 0 (0, 1.75) | 0.947 |
| No. of grade II embryos transferred per ET cycle | 1 (0.25, 2) | 1 (0, 2) | 0.940 |
| β-hCG + per ET cycle | 11 (45.8%) | 7 (35.0%) | 0.226 |
| Clinical pregnancy per ET cycle | 10 (41.7%) | 5 (25.0%) | 0.246 |
| Live birth per ET cycle | 8 (33.3%) | 3 (15.0%) | 0.294 |
| Miscarriage per ET cycle | 3 (12.5%) | 4 (20.0%) | 0.498 |
| Variables | PRP Group (n = 64) | Non-PRP Treatment Group (n = 54) | p-Value |
|---|---|---|---|
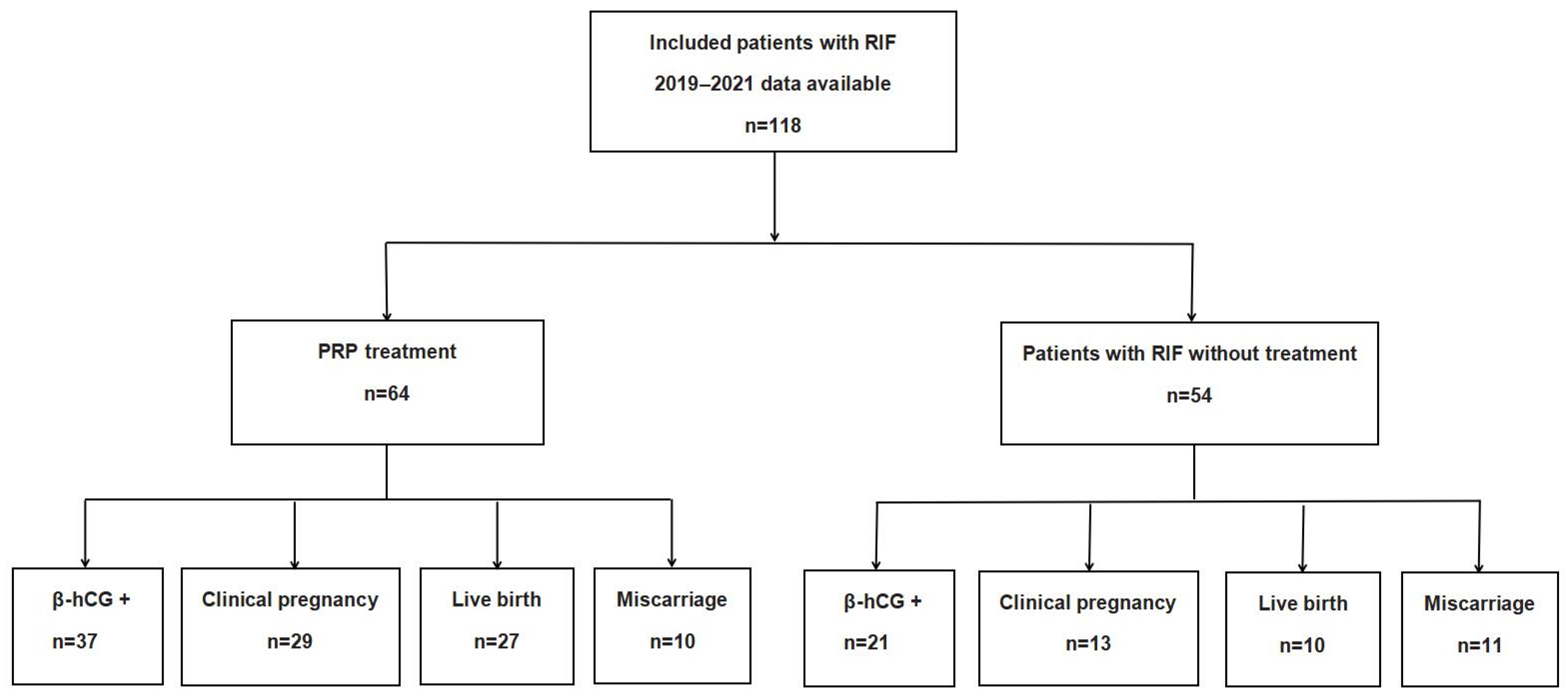
| β-hCG+ per ET cycle | 37 (57.8%) | 21(38.9%) | 0.041 * |
| Clinical pregnancy per ET cycle | 29 (45.3%) | 13 (24.1%) | 0.022 * |
| Live birth per ET cycle | 27 (42.2%) | 10 (18.5%) | 0.009 ** |
| Miscarriage per ET cycle | 10 (15.6%) | 11 (20.4%) | 0.630 |
| Variables | PRP Group (n = 64) | p-Value | |||
|---|---|---|---|---|---|
| β-hCG+ (n = 37) | CP (n = 29) | Non-Pregnancy (n = 27) | β-hCG+ vs. CP | β-hCG+ vs. Non-Pregnancy | |
| Baseline platelet count (109/L) | 240.48 ± 51.50 | 231.07 ± 47.51 | 217.07 ± 37.72 | 0.978 | 0.170 |
| Platelet count in PRP (109/L) | 745.56 ± 189.59 | 758.44 ± 428.81 | 652.67 ± 140.31 | 0.894 | 0.355 |
| Platelet enrichment coefficient (PEC) | 3.05 ± 0.72 | 3.27 ± 1.37 | 3.03 ± 0.51 | 0.701 | 0.849 |
| WBC count in PRP (106/L) | 553.33 ± 228.98 | 550.74 ± 286.36 | 496.33 ± 179.42 | 0.917 | 0.770 |
| Univariate Analysis | |||
| Variables | Odds Ratio | 95% CI | p-Value |
| Age (years) | 1.038 | (0.949–1.135) | 0.419 |
| BMI (kg/m2) | 0.963 | (0.850–1.092) | 0.556 |
| AMH (ng/mL) | 0.921 | (0.821–1.033) | 0.159 |
| Basal FSH (U/L) | 1.230 | (1.049–1.442) | 0.011 * |
| Basal LH (mIU/mL) | 0.971 | (0.883–1.068) | 0.543 |
| Basal E2 (pg/mL) | 0.997 | (0.990–1.003) | 0.325 |
| Basal progesterone (ng/mL) | 0.788 | (0.396–1.571) | 0.499 |
| Duration of infertility (years) | 0.873 | (0.717–1.064) | 0.178 |
| Previous ET attempts | 1.025 | (0.730–1.440) | 0.887 |
| Endometrial thickness during FET cycle (mm) | 0.809 | (0.641–1.020) | 0.073 |
| PRP group | 2.613 | (1.181–5.785) | 0.018 * |
| Multivariate Analysis | |||
| Variables | Odds Ratio | 95% CI | p-Value |
| Age (years) | 0.997 | (0.895–1.111) | 0.960 |
| BMI (kg/m2) | 0.958 | (0.831–1.104) | 0.552 |
| AMH (ng/mL) | 0.936 | (0.830–1.057) | 0.287 |
| Basal FSH (U/L) | 1.182 | (0.984–1.420) | 0.075 |
| Basal LH (mIU/mL) | 0.947 | (0.843–1.064) | 0.361 |
| Basal E2 (pg/mL) | 0.999 | (0.991–1.007) | 0.743 |
| Basal progesterone (ng/mL) | 0.859 | (0.389–1.897) | 0.706 |
| Duration of infertility (years) | 0.864 | (0.696–1.071) | 0.183 |
| Previous ET attempts | 1.050 | (0.705–1.565) | 0.810 |
| Endometrial thickness during FET cycle (mm) | 0.825 | (0.640–1.063) | 0.137 |
| PRP group | 2.750 | (1.136–6.660) | 0.025 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ban, Y.; Yang, X.; Xing, Y.; Que, W.; Yu, Z.; Gui, W.; Chen, Y.; Liu, X. Intrauterine Infusion of Leukocyte-Poor Platelet-Rich Plasma Is an Effective Therapeutic Protocol for Patients with Recurrent Implantation Failure: A Retrospective Cohort Study. J. Clin. Med. 2023, 12, 2823. https://doi.org/10.3390/jcm12082823
Ban Y, Yang X, Xing Y, Que W, Yu Z, Gui W, Chen Y, Liu X. Intrauterine Infusion of Leukocyte-Poor Platelet-Rich Plasma Is an Effective Therapeutic Protocol for Patients with Recurrent Implantation Failure: A Retrospective Cohort Study. Journal of Clinical Medicine. 2023; 12(8):2823. https://doi.org/10.3390/jcm12082823
Chicago/Turabian StyleBan, Yanna, Xiaoliang Yang, Yan Xing, Wenjun Que, Zebo Yu, Wenwu Gui, Ying Chen, and Xiru Liu. 2023. "Intrauterine Infusion of Leukocyte-Poor Platelet-Rich Plasma Is an Effective Therapeutic Protocol for Patients with Recurrent Implantation Failure: A Retrospective Cohort Study" Journal of Clinical Medicine 12, no. 8: 2823. https://doi.org/10.3390/jcm12082823