
Predictability of Radiologically Measured Psoas Muscle Area for Intraoperative Hypotension in Older Adult Patients Undergoing Femur Fracture Surgery
 and
and
Abstract
:1. Introduction
2. Materials and Methods
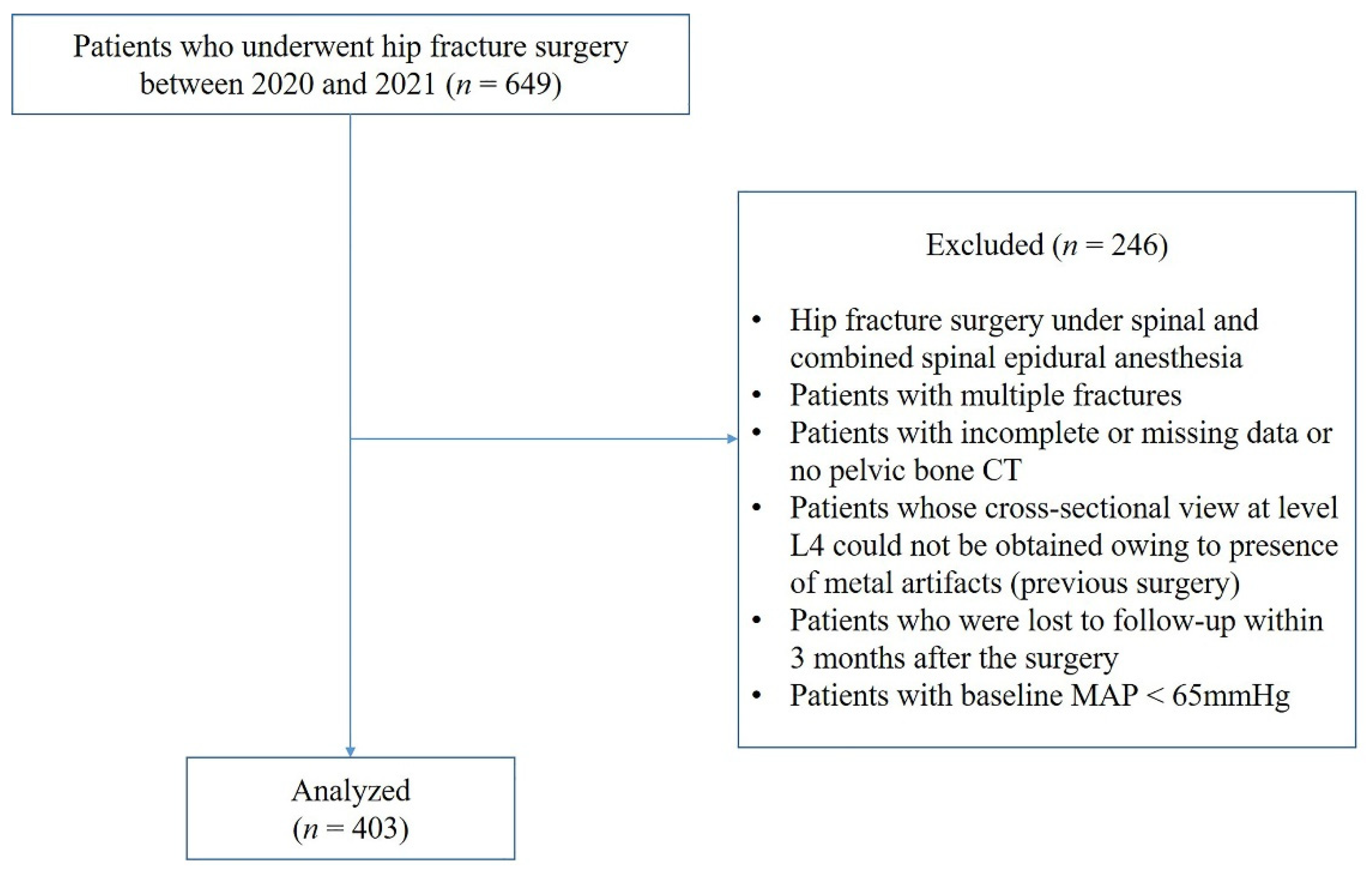
2.1. Study Design and Patients
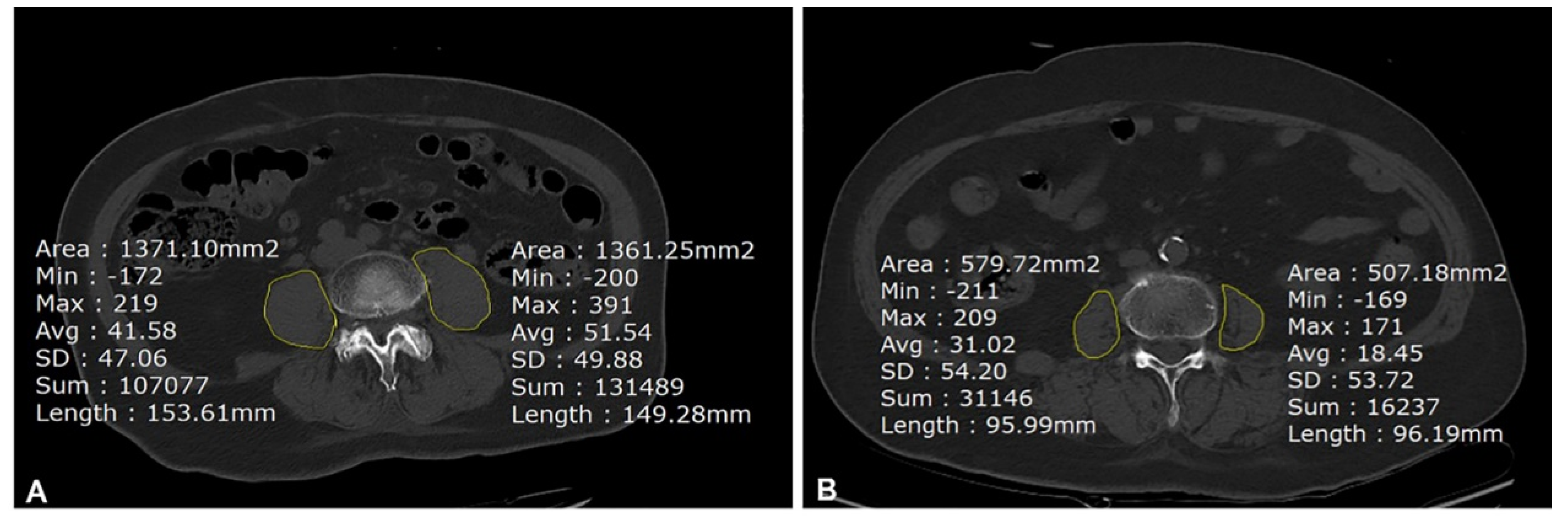
2.2. Measurement of Psoas Muscle Area
2.3. Assessment of Frailty and Intraoperative Hypotension
2.4. Data Collection
2.5. Study Outcomes
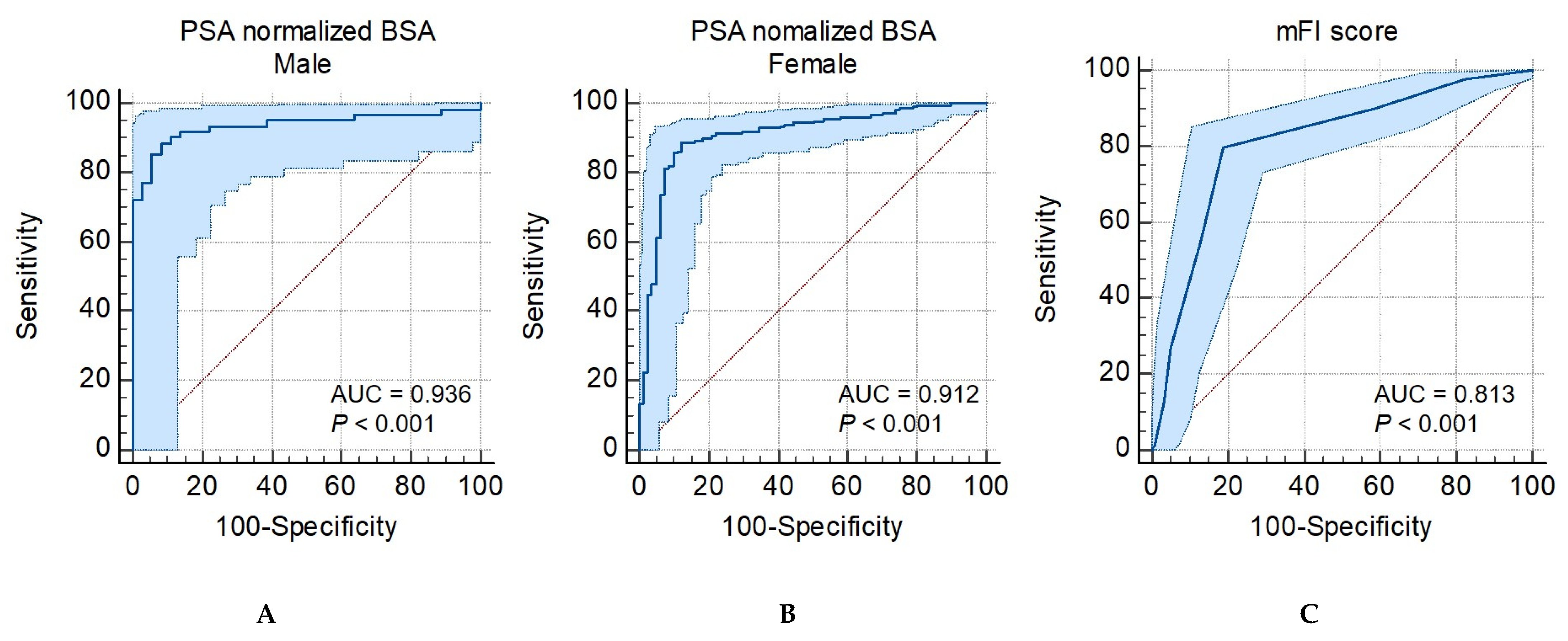
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, K.B.; Yang, N.P.; Lee, Y.H.; Chan, C.L.; Wu, C.H.; Chen, H.C.; Chang, N.T. The incidence and factors of hip fractures and subsequent morbidity in Taiwan: An 11-year population-based cohort study. PLoS ONE 2018, 13, e0192388. [Google Scholar] [CrossRef] [PubMed]
- Ove, T.; Fredrik, H.; Ola, E.D.; Are, H.P.; Olav, R. Clinical and biochemical prediction of early fatal outcome following hip fracture in the elderly. Int. Orthop. 2011, 35, 903–907. [Google Scholar]
- Istianah, U.; Nurjannah, I.; Magetsari, R. Post-discharge complications in postoperative patients with hip fracture. J. Clin. Orthop. Trauma 2021, 14, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.; Cha, Y.; Yoo, J.; Lee, J.; Lee, Y.; Koo, K. Effect of dementia on postoperative mortality in elderly patients with hip fracture. J. Korean Med. Sci. 2021, 36, e238. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.H.; Lee, S.H.; Kim, J.W.; Koh, W.U.; Kim, H.T.; Ro, Y.J.; Kim, H.J. Low psoas lumbar vertebral index is associated with mortality after hip fracture surgery in elderly patients: A retrospective analysis. J. Pers. Med. 2021, 11, 673. [Google Scholar] [CrossRef] [PubMed]
- Koizia, L.; Naik, M.; Peck, G.; Mikhail, G.W.; Sen, S.; Malik, I.S.; Ariff, B.; Fertleman, M.B. The utility of psoas muscle assessment in predicting frailty in patients undergoing transcatheter aortic valve replacement. Curr. Gerontol. Geriatr. Res. 2020, 2020, 5783107. [Google Scholar] [CrossRef] [PubMed]
- Rangel, E.L.; Rios-Diaz, A.J.; Uyeda, J.W.; Castillo-Angeles, M.; Cooper, Z.; Olufajo, O.A.; Salim, A.; Sodickson, A.D. Sarcopenia increases risk of long-term mortality in elderly patients undergoing emergency abdominal surgery. J. Trauma Acute Care Surg. 2017, 83, 1179–1186. [Google Scholar] [CrossRef]
- Ebbeling, L.; Grabo, D.J.; Shashaty, M.; Dua, R.; Sonnad, S.S.; Sims, C.A.; Pascual, J.L.; Schwab, C.W.; Holena, D.N. Psoas: Lumbar vertebra index: Central sarcopenia independently predicts morbidity in elderly trauma patients. Eur. J. Trauma Emerg. Surg. 2014, 40, 57–65. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rolfson, D.B.; Majumdar, S.R.; Tsuyuki, R.T.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsiouris, A.; Hammoud, Z.T.; Velanovich, V.; Hodari, A.; Borgi, J.; Rubinfeld, I. A modified frailty index to assess morbidity and mortality after lobectomy. J. Surg. Res. 2013, 183, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Canales, C.; Mazor, E.; Coy, H.; Grogan, T.R.; Duval, V.; Raman, S.; Cannesson, M.; Singh, S.P. Preoperative point-of-care ultrasound to identify frailty and predict postoperative outcomes: A diagnostic accuracy study. Anesthesiology 2022, 136, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Balsam, L.B. Psoas muscle area: A new standard for frailty assessment in cardiac surgery? J. Thorac. Dis. 2018, 10 (Suppl. 33), S3846–S3849. [Google Scholar] [CrossRef] [PubMed]
- Bentov, I.; Kaplan, S.J.; Pham, T.N.; Reed, M.J. Frailty assessment: From clinical to radiological tools. Br. J. Anaesth. 2019, 123, 37–50. [Google Scholar] [CrossRef]
- Sun, L.Y.; Wijeysundera, D.N.; Tait, G.A.; Beattie, W.S. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology 2015, 123, 515–523. [Google Scholar] [CrossRef]
- Salmasi, V.; Maheshwari, K.; Yang, D.; Mascha, E.J.; Singh, A.; Sessler, D.I.; Kurz, A. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Anesthesiology 2017, 126, 47–65. [Google Scholar] [CrossRef]
- Bijker, J.B.; Persoon, S.; Peelen, L.M.; Moons, K.G.; Kalkman, C.J.; Kappelle, L.J.; van Klei, W.A. Intraoperative hypotension and perioperative ischemic stroke after general surgery: A nested case-control study. Anesthesiology 2012, 116, 658–664. [Google Scholar] [CrossRef] [Green Version]
- Droguett, V.S.; Santos Ada, C.; de Medeiros, C.E.; Marques, D.P.; do Nascimento, L.S.; Brasileiro-Santos Mdo, S. Cardiac autonomic modulation in healthy elderly after different intensities of dynamic exercise. Clin. Interv. Aging 2015, 10, 203–208. [Google Scholar]
- Ackland, G.L.; Abbott, T.E.F. Hypotension as a marker or mediator of perioperative organ injury: A narrative review. Br. J. Anaesth. 2022, 128, 915–930. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.J.; Lee, S.H. Computed tomographic measurements of the psoas muscle as a predictor of mortality in hip fracture patients: Muscle attenuation helps predict mortality in hip fracture patients. Injury 2021, 52, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; Mitnitski, A. Changes in relative fitness and frailty across the adult lifespan: Evidence from the Canadian National Population Health Survey. CMAJ 2011, 183, E487–E494. [Google Scholar] [CrossRef] [Green Version]
- Choi, M.H.; Chae, J.S.; Lee, H.J.; Woo, J.H. Pre-anaesthesia ultrasonography of the subclavian/infraclavicular axillary vein for predicting hypotension after inducing general anaesthesia: A prospective observational study. Eur. J. Anaesthesiol. 2020, 37, 474–481. [Google Scholar] [CrossRef]
- Griffiths, R.; White, S.M.; Moppett, I.K.; Parker, M.J.; Chesser, T.J.; Costa, M.L.; Johansen, A.; Wilson, H.; Timperley, A.J. Safety guideline: Reducing the risk from cemented hemiarthroplasty for hip fracture 2015: Association of Anaesthetists of Great Britain and Ireland British Orthopaedic Association British Geriatric Society. Anaesthesia 2015, 70, 623–626. [Google Scholar]
- Griffiths, R.; Babu, S.; Dixon, P.; Freeman, N.; Hurford, D.; Kelleher, E.; Moppett, I.; Ray, D.; Sahota, O.; Shields, M.; et al. Guideline for the management of hip fractures 2020: Guideline by the Association of Anaesthetists. Anaesthesia 2021, 76, 225–237. [Google Scholar] [CrossRef]
- Lee, T.C.; Ho, P.S.; Lin, H.T.; Ho, M.L.; Huang, H.T.; Chang, J.K. One-year readmission risk and mortality after hip fracture surgery: A National Population-Based Study in Taiwan. Aging Dis. 2017, 8, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Sudfeld, S.; Brechnitz, S.; Wagner, J.Y.; Reese, P.C.; Pinnschmidt, H.O.; Reuter, D.A.; Saugel, B. Post-induction hypotension and early intraoperative hypotension associated with general anaesthesia. Br. J. Anaesth. 2017, 119, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Nicholas, C.C.; Viandsa, S.S.; Giovanini, T.; Friedo, W.D.; Edouard, L.F.; Carmine, Z. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 2022, 15, 14–20. [Google Scholar]
- Soysal, P.; Kocyigit, S.E.; Dokuzlar, O.; Ates Bulut, E.; Smith, L.; Isik, A.T. Relationship between sarcopenia and orthostatic hypotension. Age Ageing 2020, 49, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.B.; Rosenthal, R.A.; Merkow, R.P.; Ko, C.Y.; Esnaola, N.F. Optimal preoperative assessment of the geriatric surgical patient: A best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J. Am. Coll. Surg. 2012, 215, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Beggs, T.; Sepehri, A.; Szwajcer, A.; Tangri, N.; Arora, R.C. Frailty and perioperative outcomes: A narrative review. Can. J. Anaesth. 2015, 62, 143–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin. Nutr. 2012, 31, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Antoro, L.; Antoliquido, A.; Isto, A.; Picca, A.; Marzetti, E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos. Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef]
- Robinson, B.J.; Ebert, T.J.; O’Brien, T.J.; Colinco, M.D.; Muzi, M. Mechanisms whereby propofol mediates peripheral vasodilation in humans. Sympathoinhibition or direct vascular relaxation? Anesthesiology 1997, 86, 64–72. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Cogan, L.; O’Shea, D.; Lawlor, B.A.; Kenny, R.A. Orthostatic haemodynamics may be impaired in frailty. Age Ageing 2011, 40, 576–583. [Google Scholar] [CrossRef] [Green Version]
- Belton, P.S.; Packer, K.J. Pulsed NMR studies of water in striated muscle. 3. The effects of water content. Biochim. Biophys. Acta 1974, 354, 305–314. [Google Scholar] [CrossRef]
- Son, H.E.; Ryu, J.Y.; Lee, K.; Choi, Y.I.; Kim, M.S.; Park, I.; Shin, G.T.; Kim, H.; Ahn, C.; Kim, S.; et al. The importance of muscle mass in predicting intradialytic hypotension in patients undergoing maintenance hemodialysis. Korean J. Nephrol. 2022, 41, 611–622. [Google Scholar] [CrossRef]
- Jor, O.; Maca, J.; Koutna, J.; Gemrotova, M.; Vymazal, T.; Litschmannova, M.; Sevcik, P.; Reimer, P.; Mikulova, V.; Trlicova, M.; et al. Hypotension after induction of general anesthesia: Occurrence, risk factors, and therapy. A prospective multicentre observational study. J. Anesth. 2018, 32, 673–680. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographics | All Patients (n = 403) | No-IOH (n = 117) | IOH (n = 286) | p-Value |
|---|---|---|---|---|
| Age, year | 81.34 ± 8.60 | 78.62 ± 8.43 | 82.46 ± 8.45 | 0.001 |
| Sex, female | 305 (75.7) | 81 (69.1) | 224 (78.3) | 0.053 |
| BMI, kg/m2 | 22.15 ± 3.76 | 21.62 ± 2.89 | 21.77 ± 3.35 | 0.997 |
| ASA status | 0.372 | |||
| <III | 145 (36) | 46 (39.3) | 99 (34.6) | |
| ≥III | 258 (64) | 71 (60.7) | 187 (65.4) | |
| Chronic arterial hypertension | 316 (78.4) | 85 (26.9) | 231 (73.1) | <0.001 |
| No medication | 5 (1.6) | 1 (1.2) | 4 (1.6) | |
| ARB | 41 (12.9) | 9 (10.6) | 32 (13.9) | |
| Ca+2 antagonist | 127 (39.8) | 35 (41.2) | 92 (39.8) | |
| β-Blocker | 16 (5.0) | 2 (2.3) | 14 (6.1) | |
| ACE inhibitor | 2 (0.6) | 0 (0) | 2 (0.9) | |
| Diuretics | 6 (1.9) | 1 (1.2) | 5 (2.2) | |
| Combined drugs | 117 (38.2) | 37 (43.5) | 82 (35.5) | |
| DM | 142 (35.2) | 40 (34.2) | 102 (35.6) | 0.196 |
| Surgical category | 0.726 | |||
| Open reduction internal fixation | 186 (46.2) | 54 (46.2) | 132 (46.2) | |
| Closed reduction internal fixation | 18 (4.5) | 4 (3.4) | 14 (4.9) | |
| Bipolar hemiarthroplasty | 123 (30.5) | 32 (27.4) | 91 (31.8) | |
| Total hip replacement | 76 (18.8) | 27 (23) | 49 (17.1) | |
| Emergency surgery | 72 (17.9) | 14 (12) | 58 (20.3) | 0.048 |
| Preoperative data | ||||
| Hemoglobin, g/dL | 11.53 ± 7.08 | 11.41 ± 1.90 | 10.92 ± 1.95 | 0.113 |
| Platelet, 109/L | 209.84 ± 80.76 | 212.35 ± 82.06 | 208.74 ± 80.34 | 0.719 |
| WBC, 103/uL | 8.90 ±3.21 | 8.91 ±2.97 | 8.90 ±3.32 | 0.992 |
| Albumin, g/dL | 3.67 ± 0.28 | 3.67 ± 0.28 | 3.67 ± 0.28 | 0.243 |
| CRP, mg/dL | 2.50 ± 3.00 | 2.50 ± 3.00 | 2.50 ± 3.00 | 0.361 |
| BUN, mg/dL | 22.29 ± 7.09 | 22.29 ± 7.09 | 22.29 ± 7.09 | 0.596 |
| Creatinine, mg/dL | 0.85 ±0.51 | 0.86 ±0.48 | 0.84 ±0.52 | 0.705 |
| Intraoperative data | ||||
| Baseline SBP | 149.86 ± 21.16 | 141.46 ± 20.13 | 153.45 ± 20.61 | <0.001 |
| Baseline DBP | 82.16 ± 14.78 | 79.85 ± 12.71 | 83.15 ± 15.51 | 0.068 |
| Baseline MBP | 104.40 ± 15.15 | 102.39 ± 12.79 | 106.11 ± 15.77 | 0.052 |
| Lowest SBP | 92.20 ± 13.90 | 99.18 ± 14.38 | 89.21 ± 12.59 | <0.001 |
| Lowest DBP | 50.96 ± 10.15 | 57.12 ± 10.51 | 48.33 ± 8.79 | <0.001 |
| Lowest MBP | 64.50 ± 10.32 | 71.14 ± 10.10 | 61.68 ± 9.05 | <0.001 |
| Input, mL, (IQR) | 801.01 (762.40, 839.62) | 792.66 (748.56, 836.76) | 820.22 (741.90, 898.55) | 0.035 |
| Estimated blood loss, mL, (IQR) | 227.83 (209.69, 245.96) | 243.17 (204.07, 282.26) | 221.16 (201.28, 241.04) | 0.903 |
| Anesthesia time, min | 114.03 ± 29.61 | 107.24 ± 26.41 | 114.03 ± 27.30 | 0.612 |
| Operation time, min | 60.21 ± 24.81 | 57.44 ± 22.17 | 58.94 ± 22.81 | 0.649 |
| All Patients (n = 403) | No-IOH (n = 117) | IOH (n = 286) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| PMA | |||||||
| Male | 9.35 ± 2.75 | 11.55 ±3.01 | 8.20 ±2.48 | <0.001 | |||
| Female | 6.20 ± 1.64 | 7.81 ±1.65 | 5.68 ±1.63 | <0.001 | |||
| PMA normalized by BSA | |||||||
| Male | 5.63 ± 1.48 | 6.90 ± 0.73 | 4.95 ± 1.20 | <0.001 | |||
| Female | 4.13 ±1.03 | 5.18 ± 0.81 | 3.78 ± 0.75 | <0.001 | |||
| mFI score | 0.29 ± 0.17 | 0.17 ± 0.14 | 0.34 ±0.15 | <0.001 | |||
| Not-frail (mFI < 0.27) | 125 (31) | 103 (88) | 23 (7.7) | <0.001 | |||
| Frail (mFI ≥ 0.27) | 278 (69) | 14 (12) | 263 (92.3) | <0.001 | |||
| Before IPTW adjustment | p-value | After IPTW adjustment | p-Value | ||||
| All patients (n = 403) | No-IOH (n = 117) | IOH (n = 286) | No-IOH (n = 394) | IOH (n = 377) | |||
| ICU admission | 117 (29) | 17 (14.5) | 100 (35) | <0.001 | 57 (14.5) | 125 (33.2) | <0.001 |
| Hospital length of stay, days | 14.13 ± 10.13 | 11.96 ± 6.08 | 15.02 ±10.00 | 0.006 | 12.46 ± 6.36 | 14.60 ± 11.63 | 0.002 |
| Delirium | 138 (34.3) | 34 (29.3) | 104 (36.4) | 0.177 | |||
| DVT | 119 (29.9) | 31 (27.2) | 88 (31) | 0.455 | |||
| pneumonia | 50 (12.4) | 10 (20) | 40 (14) | 0.140 | |||
| CVA | 14 (3.5) | 1 (0.9) | 13 (4.5) | 0.068 | |||
| 3-month outcomes | 113 (28.0) | 12 (10.2) | 101 (35.3) | <0.001 | 62 (15.6) | 140 (37.1) | <0.001 |
| Rehospitalization | 86 (21.3) | 10 (25.6) | 76 (27.2) | 0.001 | 51 (13) | 109 (28.9) | <0.001 |
| Death | 10 (2.5) | 0 | 10 (3.5) | 0.046 | 4 (1.0) | 12 (3.3) | 0.030 |
| Falls | 17 (4.2) | 2 (1.7) | 15 (5.4) | 0.099 | |||
| Variables | Unadjusted Analysis | Adjusted Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age (for 1 year increase) | 1.047 (1.02, 1.08) | 0.002 | 1.06 (1.02, 1.10) | 0.003 |
| Sex (female) | 1.45 (0.84, 2.49) | 0.182 | 1.23 (0.58, 2.60) | 0.580 |
| ASA <III vs. ≥III | 1.25 (0.79, 1.90) | 0.372 | 0.68 (0.33, 1.42) | 0.305 |
| Emergency | 1.02 (0.55, 1.88) | 0.945 | — | — |
| Albumin | 0.49 (0.30, 0.82) | 0.007 | 0.76 (0.40, 1.45) | 0.400 |
| Hemoglobin | 0.83 (0.72, 0.94) | 0.004 | 1.08 (0.87, 1.33) | 0.512 |
| Baseline SBP | 1.03 (1.02, 1.04) | <0.001 | 1.03 (1.01, 1.05) | 0.001 |
| PMA normalized by BSA (Reference: 5th quintile) | 3.85 (2.92, 5.07) | <0.001 | 3.86 (2.82, 5.29) | <0.001 |
| mFI variables (categorical) | 2.07 (1.71, 2.52) | <0.001 | 1.01 (0.85, 1.21) | 0.870 |
| DM | 2.39 (1.39, 4.13) | 0.502 | — | — |
| CHF | 2.97 (1.55, 5.68) | 0.001 | — | — |
| HTN | 3.00 (1.75, 5.13) | <0.001 | — | — |
| TIA or CVA | 4.25 (2.27, 7.95) | <0.001 | — | — |
| Dependent functional status | 8.67 (4.99, 15.04) | <0.001 | — | — |
| MI | 3.61 (0.81, 16.03) | 0.091 | — | — |
| Peripheral disease | 2.23 (0.89, 5.56) | 0.086 | — | — |
| CVA with sequelae | 2.79 (1.26, 6.18) | 0.011 | — | — |
| Pulmonary disease | 3.58 (1.63, 7.86) | 0.001 | — | — |
| Cardiac intervention or angina | 3.60 (1.37, 9.47) | 0.009 | — | — |
| Impaired sensory | 1.13 (0.52, 2.44) | 0.761 | — | — |
| Variables | Unadjusted Analysis | Adjusted Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age (for 1 year increase) | 1.24 (0.6, 2.57) | 0.560 | 1.08 (1.04, 1.12) | <0.001 |
| Sex (female) | 1.04 (1.00, 1.08) | 0.045 | 1.29 (0.58, 2.89) | 0.537 |
| ASA <III vs. ≥III | 3.19 (1.57, 6.47) | 0.001 | 1.30 (0.62, 2.72) | 0.482 |
| Emergency | 0.61 (0.29, 1.27) | 0.185 | — | — |
| Albumin | 0.40 (0.22, 0.74) | 0.004 | 0.44 (0.23, 0.85) | 0.014 |
| Hemoglobin | 0.79 (0.66, 0.92) | 0.003 | 0.93 (0.82, 1.07) | 0.300 |
| Baseline SBP | 1.02 (1.00, 1.04) | 0.057 | — | — |
| IOH | 3.00 (1.38, 6.51) | 0.005 | 1.42 (0.54, 3.74) | 0.478 |
| PMA normalized by BSA (Reference: 5th quintile) | 1.44 (1.19, 1.76) | <0.001 | 1.62 (1.37, 1.91) | <0.001 |
| mFI score (categorical) | 2.38 (1.12, 5.07) | 0.025 | 0.95 (0.76, 1.19) | 0.658 |
| DM | 1.31 (0.78, 2.19) | 0.302 | — | — |
| CHF | 1.25 (0.72, 2.17) | 0.433 | — | — |
| HTN | 1.57 (0.87, 2.82) | 0.134 | — | — |
| TIA or CVA | 2.60 (1.51, 4.47) | 0.001 | — | — |
| Dependent functional status | 1.29 (0.75, 2.22) | 0.359 | — | — |
| MI | 1.85 (0.64, 5.49) | 0.267 | — | — |
| Peripheral disease | 0.93 (0.42, 2.04) | 0.853 | — | — |
| CVA with sequelae | 1.78 (0.92, 3.45) | 0.088 | — | — |
| Pulmonary disease | 1.18 (0.64, 2.18) | 0.591 | — | — |
| Cardiac intervention or angina | 1.36 (0.68, 2.73) | 0.390 | — | — |
| Impaired sensory | 1.20 (0.54, 2.70) | 0.655 | — | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.Y.; Woo, J.H.; Yoon, I.-Y.; Lee, H.J.; Ahn, S.-M.; Chae, J.S.; Kim, Y.J. Predictability of Radiologically Measured Psoas Muscle Area for Intraoperative Hypotension in Older Adult Patients Undergoing Femur Fracture Surgery. J. Clin. Med. 2023, 12, 1691. https://doi.org/10.3390/jcm12041691
Lee YY, Woo JH, Yoon I-Y, Lee HJ, Ahn S-M, Chae JS, Kim YJ. Predictability of Radiologically Measured Psoas Muscle Area for Intraoperative Hypotension in Older Adult Patients Undergoing Femur Fracture Surgery. Journal of Clinical Medicine. 2023; 12(4):1691. https://doi.org/10.3390/jcm12041691
Chicago/Turabian StyleLee, Youn Young, Jae Hee Woo, In-Young Yoon, Hyun Jung Lee, Sang-Mee Ahn, Ji Seon Chae, and Youn Jin Kim. 2023. "Predictability of Radiologically Measured Psoas Muscle Area for Intraoperative Hypotension in Older Adult Patients Undergoing Femur Fracture Surgery" Journal of Clinical Medicine 12, no. 4: 1691. https://doi.org/10.3390/jcm12041691