
Allopregnanolone Is Associated with a Stress-Induced Reduction of Heart Rate Variability in Premenstrual Dysphoric Disorder
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Procedures
2.4. Diagnosis
2.5. Measures
2.6. Data Analyses
2.7. Statistical Analyses
3. Results
3.1. Study Participants
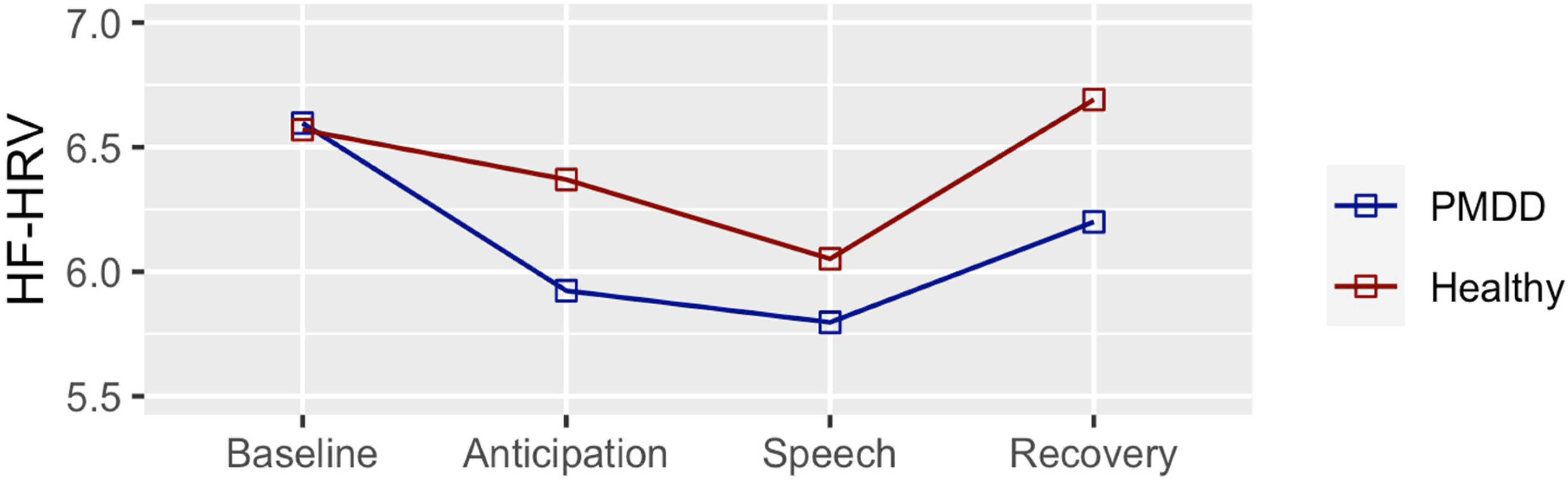
3.2. High Frequency Heart Rate Variability
3.3. Allopregnanolone
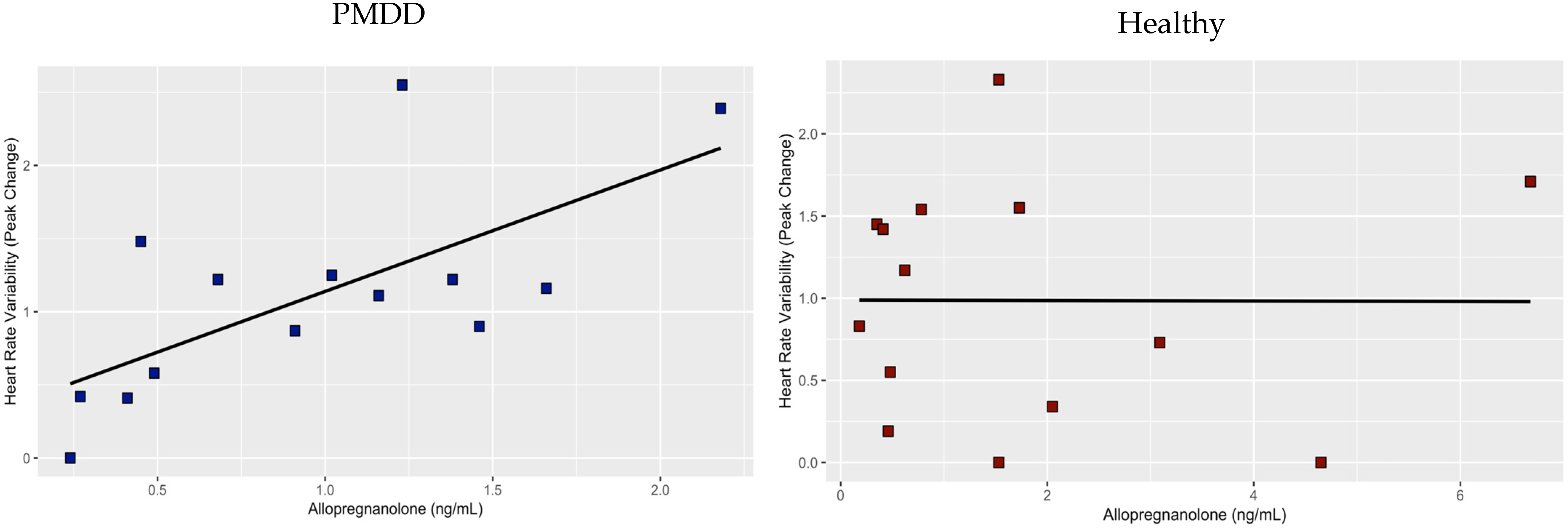
3.4. Association between Allopregnanolone and HRV
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Halbreich, U.; Borenstein, J.; Pearlstein, T.; Kahn, L.S. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD). Psychoneuroendocrinology 2003, 28 (Suppl. 3), 1–23. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Walters, E.E. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the National Comorbidity Survey. Depress. Anxiety 1998, 7, 3–14. [Google Scholar] [CrossRef]
- Brownley, K.A.; Girdler, S.S.; Stout, A.L.; McLeod, M.N. Chromium Supplementation for Menstrual Cycle-Related Mood Symptoms. J. Diet. Suppl. 2013, 10, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Gehlert, S.; Song, I.H.; Chang, C.-H.; Hartlage, S.A. The prevalence of premenstrual dysphoric disorder in a randomly selected group of urban and rural women. Psychol. Med. 2008, 39, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonkers, K.A.; Simoni, M.K. Premenstrual disorders. Am. J. Obstet. Gynecol. 2018, 218, 68–74. [Google Scholar] [CrossRef]
- Epperson, C.N.; Steiner, M.; Hartlage, S.A.; Eriksson, E.; Schmidt, P.J.; Jones, I.; Yonkers, K.A.; Eisenlohr-Moul, T.A.; Girdler, S.S.; Schmalenberger, K.M.; et al. Premenstrual Dysphoric Disorder: Evidence for a New Category for DSM-5. Am. J. Psychiatry 2012, 169, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Beddig, T.; Kuehner, C. Current Aspects of Premenstrual Dysphoric Disorder—A Review. Psychother. Psychosom. Med. Psychol. 2017, 67, 504–513. [Google Scholar]
- Kleinstäuber, M.; Schmelzer, K.; Ditzen, B.; Andersson, G.; Hiller, W.; Weise, C. Psychosocial Profile of Women with Premenstrual Syndrome and Healthy Controls: A Comparative Study. Int. J. Behav. Med. 2016, 23, 752–763. [Google Scholar] [CrossRef]
- Perkonigg, A.; Yonkers, K.A.; Pfister, H.; Lieb, R.; Wittchen, H.U. Risk factors for premenstrual dysphoric disorder in a community sample of young women: The role of traumatic events and posttraumatic stress disorder. J. Clin. Psychiatry 2004, 65, 1314–1322. [Google Scholar] [CrossRef]
- Beddig, T.; Reinhard, I.; Kuehner, C. Stress, mood, and cortisol during daily life in women with Premenstrual Dysphoric Disorder (PMDD). Psychoneuroendocrinology 2019, 109, 104372. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Balzarotti, S.; Biassoni, F.; Colombo, B.; Ciceri, M.R. Cardiac vagal control as a marker of emotion regulation in healthy adults: A review. Biol. Psychol. 2017, 130, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Sternberg, E. Beyond Heart Rate Variability: Vagal Regulation of Allostatic Systems. Ann. N. Y. Acad. Sci. 2006, 1088, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Hamidovic, A.; Van Hedger, K.; Choi, S.H.; Flowers, S.; Wardle, M.; Childs, E. Quantitative meta-analysis of heart rate variability finds reduced parasympathetic cardiac tone in women compared to men during laboratory-based social stress. Neurosci. Biobehav. Rev. 2020, 114, 194–200. [Google Scholar] [CrossRef]
- Martinez, P.E.; Rubinow, D.R.; Nieman, L.K.; Koziol, D.E.; Morrow, A.L.; Schiller, C.E.; Cintron, D.; Thompson, K.D.; Khine, K.K.; Schmidt, P.J. 5α-Reductase Inhibition Prevents the Luteal Phase Increase in Plasma Allopregnanolone Levels and Mitigates Symptoms in Women with Premenstrual Dysphoric Disorder. Neuropsychopharmacology 2015, 41, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Hantsoo, L.; Epperson, C.N. Allopregnanolone in premenstrual dysphoric disorder (PMDD): Evidence for dysregulated sensitivity to GABA-A receptor modulating neuroactive steroids across the menstrual cycle. Neurobiol. Stress 2020, 12, 100213. [Google Scholar] [CrossRef]
- Neckel, H.; Quagliotto, E.; Casali, K.R.; Montano, N.; Lago, P.D.; Rasia-Filho, A.A. Glutamate and GABA in the medial amygdala induce selective central sympathetic/parasympathetic cardiovascular responses. Can. J. Physiol. Pharmacol. 2012, 90, 525–536. [Google Scholar] [CrossRef]
- Johnston, G.A.R. Muscimol as an Ionotropic GABA Receptor Agonist. Neurochem. Res. 2014, 39, 1942–1947. [Google Scholar] [CrossRef]
- Salomé, N.; Ngampramuan, S.; Nalivaiko, E. Intra-amygdala injection of GABAA agonist, muscimol, reduces tachycardia and modifies cardiac sympatho-vagal balance during restraint stress in rats. Neuroscience 2007, 148, 335–341. [Google Scholar] [CrossRef]
- Endicott, J.; Nee, J.; Harrison, W. Daily Record of Severity of Problems (DRSP): Reliability and validity. Arch. Women’s Ment. Health 2006, 9, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Gingnell, M.; Bannbers, E.; Wikström, J.; Fredrikson, M.; Sundström-Poromaa, I. Premenstrual dysphoric disorder and prefrontal reactivity during anticipation of emotional stimuli. Eur. Neuropsychopharmacol. 2013, 23, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Solís-Ortiz, S.; Corsi-Cabrera, M. Sustained attention is favored by progesterone during early luteal phase and visuo-spatial memory by estrogens during ovulatory phase in young women. Psychoneuroendocrinology 2008, 33, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Sohda, S.; Suzuki, K.; Igari, I. Relationship Between the Menstrual Cycle and Timing of Ovulation Revealed by New Protocols: Analysis of Data from a Self-Tracking Health App. J. Med. Internet Res. 2017, 19, e391. [Google Scholar] [CrossRef] [Green Version]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef]
- Li, H.J.; Goff, A.; Rudzinskas, S.A.; Jung, Y.; Dubey, N.; Hoffman, J.; Hipolito, D.; Mazzu, M.; Rubinow, D.R.; Schmidt, P.J.; et al. Altered estradiol-dependent cellular Ca2+ homeostasis and endoplasmic reticulum stress response in Premenstrual Dysphoric Disorder. Mol. Psychiatry 2021, 26, 6963–6974. [Google Scholar] [CrossRef]
- Dubey, N.; Hoffman, J.F.; Schuebel, K.; Yuan, Q.; Martinez, P.E.; Nieman, L.K.; Rubinow, D.R.; Schmidt, P.J.; Goldman, D. The ESC/E(Z) complex, an effector of response to ovarian steroids, manifests an intrinsic difference in cells from women with premenstrual dysphoric disorder. Mol. Psychiatry 2017, 22, 1172–1184. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, P.J.; Martinez, P.E.; Nieman, L.K.; Koziol, D.E.; Thompson, K.D.; Schenkel, L.; Wakim, P.G.; Rubinow, D.R. Premenstrual Dysphoric Disorder Symptoms Following Ovarian Suppression: Triggered by Change in Ovarian Steroid Levels But Not Continuous Stable Levels. Am. J. Psychiatry 2017, 174, 980–989. [Google Scholar] [CrossRef]
- Marrocco, J.; Einhorn, N.R.; Petty, G.H.; Li, H.; Dubey, N.; Hoffman, J.; Berman, K.F.; Goldman, D.; Lee, F.S.; Schmidt, P.J.; et al. Epigenetic intersection of BDNF Val66Met genotype with premenstrual dysphoric disorder transcriptome in a cross-species model of estradiol add-back. Mol. Psychiatry 2018, 25, 572–583. [Google Scholar] [CrossRef] [Green Version]
- Porges, S.W.; Bohrer, R.E. The analysis of periodic processes in psychophysiological research. In Principles of Psychophysiology: Physical, Social, and Inferential Elements; Cambridge University Press: New York, NY, USA, 1990; pp. 708–753. [Google Scholar]
- Beck, A.T.; Ward, C.; Mendelson, M. Beck depression inventory (BDI). Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Epstein, N. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 12 December 2020).
- Hamidovic, A.; Soumare, F.; Naveed, A.; Davis, J.; Sun, J.; Dang, N. Reduced Dehydroepiandrosterone-Sulfate Levels in the Mid-Luteal Subphase of the Menstrual Cycle: Implications to Women’s Health Research. Metabolites 2022, 12, 941. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; Colrain, I.M.; Trinder, J. Reduced parasympathetic activity during sleep in the symptomatic phase of severe premenstrual syndrome. J. Psychosom. Res. 2008, 65, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Zambotti, M.; Nicholas, C.L.; Colrain, I.M.; Trinder, J.A.; Baker, F.C. Autonomic regulation across phases of the menstrual cycle and sleep stages in women with premenstrual syndrome and healthy controls. Psychoneuroendocrinology 2013, 38, 2618–2627. [Google Scholar] [CrossRef] [Green Version]
- Landén, M.; Wennerblom, B.; Tygesen, H.; Modigh, K.; Sörvik, K.; Ysander, C.; Ekman, A.; Nissbrandt, H.; Olsson, M.; Eriksson, E. Heart rate variability in premenstrual dysphoric disorder. Psychoneuroendocrinology 2004, 29, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Ushiroyama, T.; Kimura, T.; Hayashi, T.; Moritani, T. Altered autonomic nervous system activity as a potential etiological factor of premenstrual syndrome and premenstrual dysphoric disorder. Biopsychosoc. Med. 2007, 1, 24. [Google Scholar] [CrossRef] [Green Version]
- Mumford, S.L.; Schisterman, E.F.; Gaskins, A.J.; Pollack, A.Z.; Perkins, N.J.; Whitcomb, B.W.; Ye, A.; Wactawski-Wende, J. Realignment and multiple imputation of longitudinal data: An application to menstrual cycle data. Paediatr. Périnat. Epidemiol. 2011, 25, 448–459. [Google Scholar] [CrossRef] [Green Version]
- Meng, Y.; Chang, L.; Hou, L.; Zhou, R. Menstrual attitude and social cognitive stress influence autonomic nervous system in women with premenstrual syndrome. Stress 2022, 25, 87–96. [Google Scholar] [CrossRef]
- Oda, Y. Influences of premenstrual syndrome on daily psychological states and salivary cortisol level. Jpn. J. Psychol. 2005, 76, 426–435. [Google Scholar] [CrossRef] [Green Version]
- Andreen, L.; Sundström-Poromaa, I.; Bixo, M.; Nyberg, S.; Bäckström, T. Allopregnanolone concentration and mood—A bimodal association in postmenopausal women treated with oral progesterone. Psychopharmacology 2006, 187, 209–221. [Google Scholar] [CrossRef]
- Miczek, K.A.; Barry, H. Effects of alcohol on attack and defensive-submissive reactions in rats. Psychopharmacology 1977, 52, 231–237. [Google Scholar] [CrossRef] [PubMed]
- DeBold, J.F.; Miczek, K.A. Testosterone modulates the effects of ethanol on male mouse aggression. Psychopharmacology 1985, 86, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Miczek, K.A.; Weerts, E.M.; Tornatzky, W.; DeBold, J.F.; Vatne, T.M. Alcohol and “bursts” of aggressive behavior: Ethological analysis of individual differences in rats. Psychopharmacology 1992, 107, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Winslow, J.T.; Miczek, K.A. Androgen dependency of alcohol effects on aggressive behavior: A seasonal rhythm in high-ranking squirrel monkeys. Psychopharmacology 1988, 95, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Hantsoo, L.; Epperson, C.N. Premenstrual Dysphoric Disorder: Epidemiology and Treatment. Curr. Psychiatry Rep. 2015, 17, 87. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Davis, M. Role of the Hippocampus, the Bed Nucleus of the Stria Terminalis, and the Amygdala in the Excitatory Effect of Corticotropin-Releasing Hormone on the Acoustic Startle Reflex. J. Neurosci. 1997, 17, 6434–6446. [Google Scholar] [CrossRef] [Green Version]
- Toufexis, D.J.; Davis, C.; Hammond, A.; Davis, M. Progesterone attenuates corticotropin-releasing factor-enhanced but not fear-potentiated startle via the activity of its neuroactive metabolite, allopregnanolone. J. Neurosci. 2004, 24, 10280–10287. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.E.; Keevil, B.; Huhtaniemi, I.T. Mass spectrometry and immunoassay: How to measure steroid hormones today and tomorrow. Eur. J. Endocrinol. 2015, 173, D1–D12. [Google Scholar] [CrossRef] [Green Version]
- Ney, L.J.; Felmingham, K.L.; Nichols, D. Reproducibility of saliva progesterone measured by immunoassay compared to liquid chromatography mass spectrometry. Anal. Biochem. 2020, 610, 113984. [Google Scholar] [CrossRef]
- Stanczyk, F.Z.; Clarke, N.J. Advantages and challenges of mass spectrometry assays for steroid hormones. J. Steroid Biochem. Mol. Biol. 2010, 121, 491–495. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Variable | Category | Diagnosis | p Value | |
|---|---|---|---|---|
| PMDD (n = 17) | Healthy (n = 18) | |||
| Age | 26.05 (5.21) | 26.44 (5.30) | 0.83 | |
| Race | White | 6 | 8 | 0.95 |
| Black or African American | 2 | 3 | ||
| American Indian or Alaska Native | 1 | 0 | ||
| Asian | 6 | 6 | ||
| Native Hawaiian or Other Pacific Islander | 0 | 0 | ||
| More than one race | 1 | 1 | ||
| Unknown/Do not want to specify | 1 | 0 | ||
| Ethnicity | Hispanic | 4 | 4 | 0.60 |
| Non-Hispanic | 13 | 12 | ||
| Unknown/Do not want to specify | 0 | 2 | ||
| Student Status | Yes | 11 | 6 | 0.09 |
| No | 6 | 12 | ||
| Marital Status | Single | 14 | 17 | 0.40 |
| Married | 2 | 1 | ||
| Divorced | 1 | 0 | ||
| Widowed | 0 | 0 | ||
| Income | Less than $20,000 | 8 | 10 | 0.53 |
| $20,000—$34,999 | 1 | 3 | ||
| $35,000—$49,999 | 4 | 1 | ||
| $50,000—$74,999 | 2 | 3 | ||
| 75,000 or more | 2 | 1 | ||
| Age of Menarche | 12.06 (1.56) | 11.66 (1.72) | 0.53 | |
| BMI * | 25.33 (5.26) | 23.86 (4.08) | 0.36 | |
| BDI ** | 3.00 (2.29) | 2.94 (3.33) | 0.95 | |
| PMDD | |||||
|---|---|---|---|---|---|
| Contrast | Estimate | SE | df | t. Ratio | p Value |
| Baseline vs. Instruction | 0.673 | 0.224 | 99 | 3.001 | 0.0176 * |
| Baseline vs. TSST | 0.8 | 0.224 | 99 | 3.568 | 0.0031 ** |
| Baseline vs. Recovery | 0.396 | 0.224 | 99 | 1.768 | 0.2949 |
| Instruction vs. TSST | 0.127 | 0.224 | 99 | 0.567 | 0.9417 |
| Instruction vs. Recovery | −0.276 | 0.224 | 99 | −1.233 | 0.6076 |
| TSST vs. Recovery | −0.404 | 0.224 | 99 | −1.799 | 0.2797 |
| Healthy | |||||
| Baseline vs. Instruction | 0.2 | 0.218 | 99 | 0.918 | 0.7954 |
| Baseline vs. TSST | 0.518 | 0.218 | 99 | 2.378 | 0.0879 |
| Baseline vs. Recovery | −0.121 | 0.218 | 99 | −0.556 | 0.9448 |
| Instruction vs. TSST | 0.318 | 0.218 | 99 | 1.461 | 0.465 |
| Instruction vs. Recovery | −0.321 | 0.218 | 99 | −1.473 | 0.4573 |
| TSST vs. Recovery | −0.639 | 0.218 | 99 | −2.934 | 0.0213 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamidovic, A.; Davis, J.; Soumare, F.; Naveed, A.; Ghani, Y.; Semiz, S.; Khalil, D.; Wardle, M. Allopregnanolone Is Associated with a Stress-Induced Reduction of Heart Rate Variability in Premenstrual Dysphoric Disorder. J. Clin. Med. 2023, 12, 1553. https://doi.org/10.3390/jcm12041553
Hamidovic A, Davis J, Soumare F, Naveed A, Ghani Y, Semiz S, Khalil D, Wardle M. Allopregnanolone Is Associated with a Stress-Induced Reduction of Heart Rate Variability in Premenstrual Dysphoric Disorder. Journal of Clinical Medicine. 2023; 12(4):1553. https://doi.org/10.3390/jcm12041553
Chicago/Turabian StyleHamidovic, Ajna, John Davis, Fatimata Soumare, Aamina Naveed, Yaseen Ghani, Selma Semiz, Dina Khalil, and Margaret Wardle. 2023. "Allopregnanolone Is Associated with a Stress-Induced Reduction of Heart Rate Variability in Premenstrual Dysphoric Disorder" Journal of Clinical Medicine 12, no. 4: 1553. https://doi.org/10.3390/jcm12041553