
Corneal Optical Densitometry in the Evaluation of 2-Year Graft Function Following Endothelial Keratoplasty

Abstract
:1. Introduction
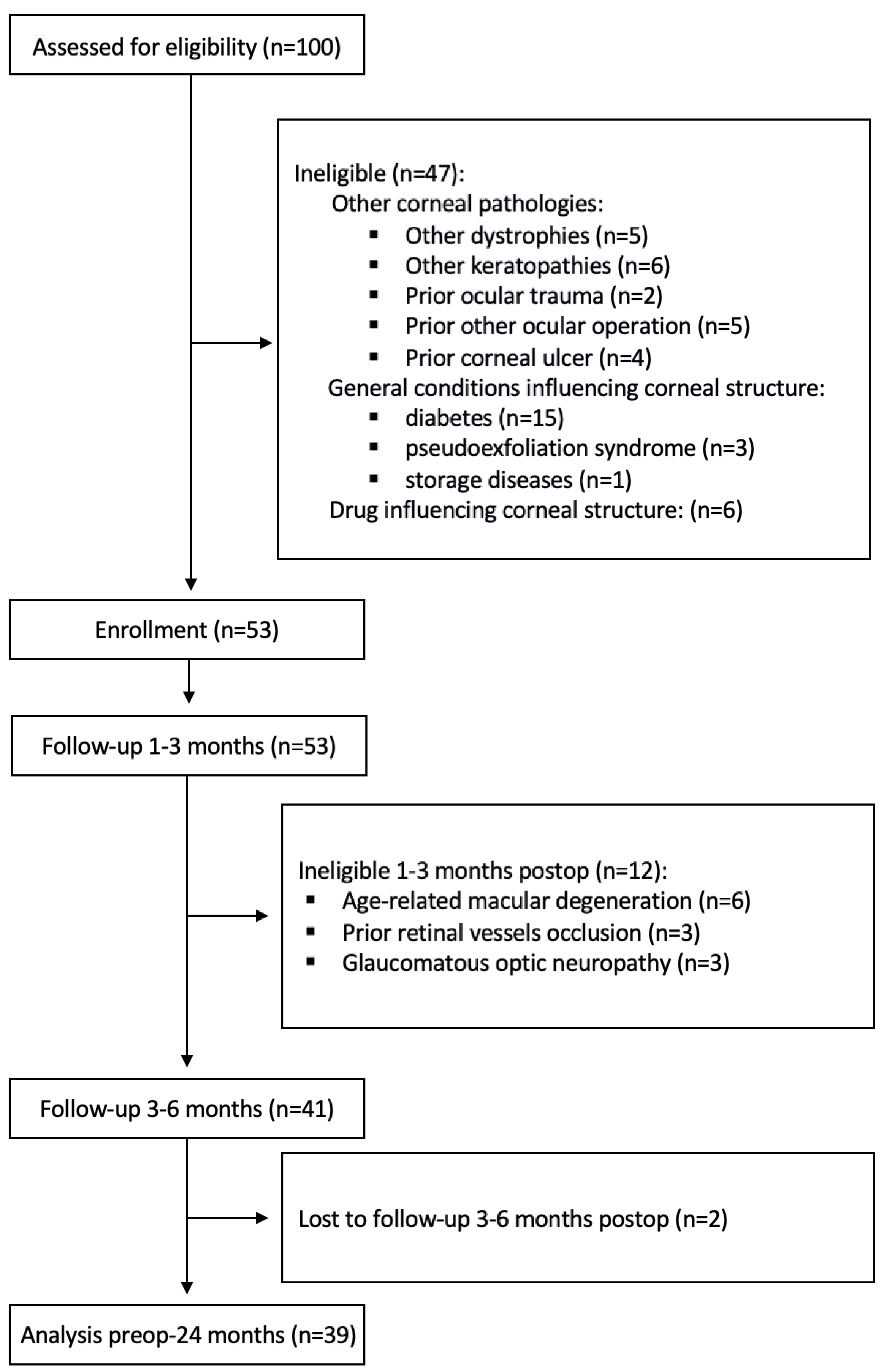
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Variability over Time
3.1.1. BCVA
3.1.2. Pachymetry
3.1.3. Densitometry
3.1.4. Endothelial Cell Density
3.2. Functional Stabilization of Vision
3.3. Correlation between Parameters at the Stabilization Time Point (6 Months Postoperatively)
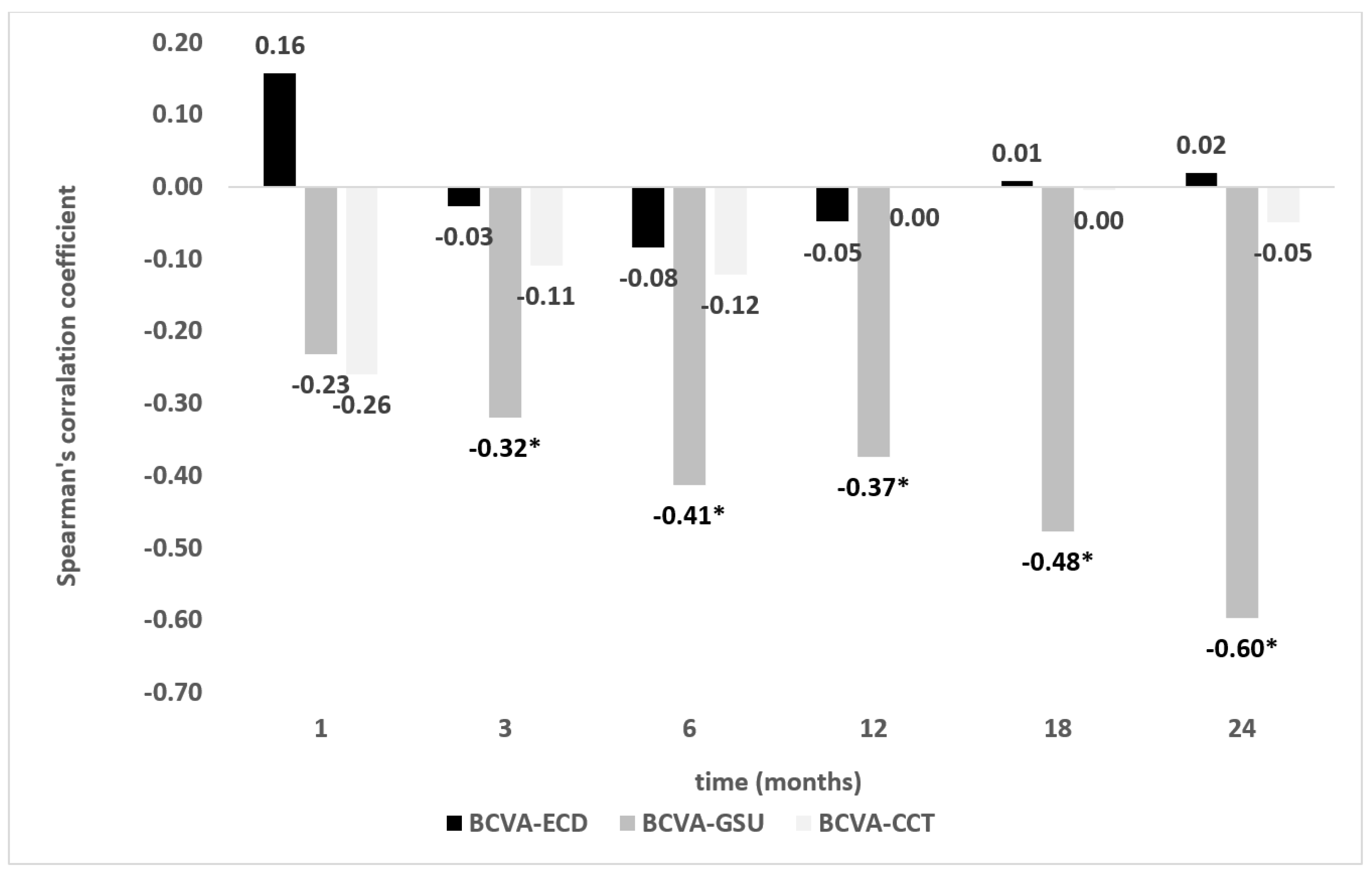
3.4. Correlation between Parameters throughout the 2-Year-Follow-Up Period
4. Discussion
Limitations of the Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maurice, D.M. The structure and transparency of the cornea. J. Physiol. 1957, 136, 263–286. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Farrell, R.A.; Hart, R.W.; Langham, M.E. The transparency of the mammalian cornea. J. Physiol. 1970, 210, 601–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, R.A.; McCally, R.L.; Tatham, P.E.R. Wave-length dependencies of light scattering in normal and cold swollen rabbit corneas and their structural implications. J. Physiol. 1973, 233, 589–612. [Google Scholar] [CrossRef] [PubMed]
- Edelhauser, H.F.; Ubels, J.L.; Hejny, C. The cornea and the sclera. In Adler’s Physiology of the Eye, 10th ed.; Kaufman, P.L., Alm, A., Eds.; Mosby: St. Louis, MO, USA, 2003; pp. 47–114. [Google Scholar]
- Zander, D.B.; Böhringer, D.; Fritz, M.; Grewing, V.; Maier, P.C.; Lapp, T.; Reinhard, T.; Wacker, K. Hyperosmolar eye Drops for Diurnal Corneal Edema in Fuchs’ Endothelial Dystrophy. Ophthalmology 2021, 128, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Price, F.W., Jr. Randomized, Double-Masked, Pilot Study of Netarsudil 0.02% Ophthalmic Solution for Treatment of Corneal Edema in Fuchs Dystrophy. Am. J. Ophthalmol. 2021, 227, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Terry, M.A. Endothelial keratoplasty: History, current state, and future directions. Cornea 2006, 25, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Seitz, B.; Daas, L.; Flockerzi, E.; Suffo, S. Descemet membrane endothelial keratoplasty DMEK—Spender und Empfänger Schritt für Schritt. Ophthalmologe 2020, 117, 811–828. [Google Scholar] [CrossRef]
- Terry, M.A.; Ousley, P.J. Deep lamellar endothelial keratoplasty in the first United States patients: Early clinical results. Cornea 2001, 20, 239–243. [Google Scholar] [CrossRef]
- Melles, G.R.; Lander, F.; Nieuwendaal, C. Sutureless, posterior lamellar keratoplasty: A case report of a modified technique. Cornea 2002, 21, 325–327. [Google Scholar] [CrossRef]
- Price, F.W., Jr.; Price, M.O. Descemet’s stripping with endothelial keratoplasty in 50 eyes: A refractive neutral corneal transplant. J. Refract. Surg. 2005, 21, 339–345. [Google Scholar] [CrossRef]
- Melles, G.R.J.; Ong, T.S.; Ververs, B.; van der Wees, J. Descemet membrane endothelial keratoplasty (DMEK). Cornea 2006, 25, 987–990. [Google Scholar] [PubMed]
- Busin, M.; Madi, S.; Santorum, P.; Scorcia, V.; Beltz, J. Ultrathin descemet’s stripping automated endothelial keratoplasty with the microkeratome double-pass technique: Two-year outcomes. Ophthalmology 2013, 120, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Ní Dhubhghaill, S.; Rozema, J.J.; Jongenelen, S.; Ruiz Hidalgo, I.; Zakaria, N.; Tassignon, M.J. Normative values for corneal densitometry analysis by Scheimpflug optical assessment. Investig. Ophthalmol. Vis. Sci. 2014, 55, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faik Orucoglu, F.; Talaz, S.; Aksu, A.; Muftuoglu, O. Corneal densitometry evaluation in archipelago keratitis. Int. Ophthalmol. 2014, 34, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, R.; Lopez, I.; Villa-Collar, C.; González-Méijome, J.M. Corneal transparency after cross-linking for keratoconus: 1-year follow-up. J. Refract. Surg. 2012, 28, 781–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fares, U.; Otri, A.M.; Al-Aqaba, M.A.; Faraj, L.; Dua, H.S. Wavefront-optimized excimer laser in situ keratomileusis for myopia and myopic astigmatism: Refractive outcomes and corneal densitometry. J. Cataract. Refract. Surg. 2012, 38, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, U.K.; Fares, U.; Rahman, I.; Said, D.G.; Maharajan, S.V.; Dua, H.S. Outcomes of deep anterior lamellar keratoplasty following successful and failed ‘big bubble’. Br. J. Ophthalmol. 2012, 96, 564–569. [Google Scholar] [CrossRef]
- Pantanelli, S.M.; Sabesan, R.; Ching, S.S.; Yoon, G.; Hindman, H.B. Visual performance with wave aberration correction after penetrating, deep anterior lamellar, or endothelial keratoplasty. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4797–4804. [Google Scholar] [CrossRef]
- Ham, L.; Dapena, I.; van der Wees, J.; Melles, G.R. Secondary DMEK for poor visual outcome after DSEK: Donor posterior stroma may limit visual acuity in endothelial keratoplasty. Cornea 2010, 29, 1278–1283. [Google Scholar] [CrossRef]
- Dirisamer, M.; Parker, J.; Naveiras, M.; Liarakos, V.S.; Ham, L.; van Dijk, K.; Melles, G.R. Identifying causes for poor visual outcome after DSEK/DSAEK following secondary DMEK in the same eye. Acta Ophthalmol. 2013, 91, 131–139. [Google Scholar] [CrossRef]
- Seery, L.S.; Nau, C.B.; McLaren, J.W.; Baratz, K.H.; Patel, S.V. Graft thickness, graft folds, and aberrations after Descemet stripping endothelial keratoplasty for Fuchs dystrophy. Am. J. Ophthalmol. 2011, 152, 910–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolph, M.; Laaser, K.; Bachmann, B.O.; Cursiefen, C.; Epstein, D.; Kruse, F.E. Corneal higher-order aberrations after descemet’s membrane endothelial keratoplasty. Ophthalmology 2012, 119, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Ohnuma, K.; Tomida, D.; Konomi, K.; Satake, Y.; Negishi, K.; Tsubota, K.; Shimazaki, J. The contribution of the posterior surface to the corneal aberrations in eyes after keratoplasty. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6222–6229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dijk, K.; Droutsas, K.; Hou, J.; Sangsari, S.; Liarakos, V.S.; Melles, G.R. Optical quality of the cornea after descemet membrane endothelial keratoplasty. Am. J. Ophthalmol. 2014, 158, 71–79.e1. [Google Scholar] [CrossRef] [PubMed]
- Chaurasia, S.; Price, M.O.; McKee, Y.; Price, F.W. Descemet membrane endothelial keratoplasty combined with epithelial debridement and mitomycin-C application for Fuchs dystrophy with preoperative subepithelial fibrosis or anterior basement membrane dystrophy. Cornea 2014, 33, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Droutsas, K.; Lazaridis, A.; Giallouros, E.; Kymionis, G.; Chatzistefanou, K.; Sekundo, W. Scheimpflug densitometry after DMEK versus DSAEK-two-year outcomes. Cornea 2018, 37, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Arnalich-Montiel, F.; Hernández-Verdejo, J.L.; Oblanca, N.; Muñoz-Negrete, F.J.; De Miguel, M.P. Comparison of corneal haze and visual outcome in primary DSAEK versus DSAEK following failed DMEK. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 2575–2584. [Google Scholar] [CrossRef]
- Ivarsen, A.; Hjortdal, J. Recipient corneal thickness and visual outcome after descemet’s stripping automated endothelial keratoplasty. Br. J. Ophthalmol. 2014, 98, 30–34. [Google Scholar] [CrossRef]
- Lee, W.B.; Jacobs, D.S.; Musch, D.C.; Kaufman, S.C.; Reinhart, W.J.; Shtein, R.M. Descemet’s stripping endothelial keratoplasty: Safety and outcomes: A report by the American Academy of Ophthalmology. Ophthalmology 2009, 116, 1818–1830. [Google Scholar] [CrossRef]
- Hassell, J.R.; Birk, D.E. The molecular basis of corneal transparency. Exp. Eye Res. 2010, 91, 326–335. [Google Scholar] [CrossRef] [Green Version]
- Anseth, A. Studies on corneal polysaccharides. V. Changes in corneal glycosaminoglycans in transient stromal edema. Exp. Eye Res. 1969, 8, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Kangas, T.A.; Edelhauser, H.F.; Twining, S.S.; O’Brien, W.J. Loss of stromal glycosaminoglycans during corneal edema. Investig. Ophthalmol. Vis. Sci. 1990, 31, 1994–2002. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BCVA | CCT | Densitometry | ECD | ||
|---|---|---|---|---|---|
| Loss of Statistical Significance (p > 0.05) of Changes Comparing Subsequent Time Points | 6 mo | 6 mo | 3 mo | 12 mo | |
| Mean 24-month value or better | 1 mo | 7.7% | 89.7% | 12.8% | 100% |
| 3 mo | 20.5% | 94.9% | 23.1% | 100% | |
| 6 mo | 38.5% | 87.2% | 25.6% | 84.6% | |
| 12 mo | 56.4% | 71.8% | 46.2% | 74.4% | |
| 18 mo | 66.7% | 48.7% | 56.4% | 64.1% | |
| 24 mo | 66.7% | 48.7% | 64.1% | 46.2% | |
| 1 mo | 3 mo | 6 mo | 12 mo | 18 mo | 24 mo | |
|---|---|---|---|---|---|---|
| 1 mo | >0.051 | 0.0062 | <0.011 | <0.013 | <0.011 | |
| 3 mo | >0.051 | 0.0055 | 0.0026 | <0.014 | <0.012 | |
| 6 mo | 0.0062 | 0.0055 | >0.053 | 0.037 | 0.0036 | |
| 12 mo | <0.011 | 0.0026 | >0.053 | >0.054 | >0.054 | |
| 18 mo | <0.013 | <0.014 | 0.037 | >0.054 | >0.053 | |
| 24 mo | <0.011 | <0.012 | 0.0036 | >0.054 | >0.053 |
| mean ± SD | Parameter | ECD 6 mo | BCVA 6 mo | GSU 6 mo | CCT 6 mo |
|---|---|---|---|---|---|
| 1889.00 ± 230.62 | ECD 6 mo | −0.08 | −0.02 | −0.07 | |
| 0.57 ± 0.26 | BCVA 6 mo | −0.08 | −0.41 * | −0.12 | |
| 20.07 ± 8.07 | GSU 6 mo | −0.02 | −0.41 * | 0.03 | |
| 602.69 ± 75.85 | CCT 6 mo | −0.07 | −0.12 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piotrowiak-Słupska, I.; Kałużny, B.J.; Malukiewicz, G. Corneal Optical Densitometry in the Evaluation of 2-Year Graft Function Following Endothelial Keratoplasty. J. Clin. Med. 2023, 12, 1552. https://doi.org/10.3390/jcm12041552
Piotrowiak-Słupska I, Kałużny BJ, Malukiewicz G. Corneal Optical Densitometry in the Evaluation of 2-Year Graft Function Following Endothelial Keratoplasty. Journal of Clinical Medicine. 2023; 12(4):1552. https://doi.org/10.3390/jcm12041552
Chicago/Turabian StylePiotrowiak-Słupska, Ilona, Bartłomiej J. Kałużny, and Grażyna Malukiewicz. 2023. "Corneal Optical Densitometry in the Evaluation of 2-Year Graft Function Following Endothelial Keratoplasty" Journal of Clinical Medicine 12, no. 4: 1552. https://doi.org/10.3390/jcm12041552