
Blood Type A1 Mismatch Does Not Affect Heart Transplant Outcomes at One Year

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Pre-Transplant Clinical Characteristics
3.2. Post-Transplant Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bergenfeldt, H.; Andersson, B.; Bućin, D.; Stehlik, J.; Edwards, L.; Rådegran, G.; Nilsson, J. Outcomes after ABO-incompatible heart transplantation in adults: A registry study. J. Heart Lung Transplant. 2015, 34, 892–898. [Google Scholar] [PubMed]
- Breimer, M.E.; Samuelsson, B.E. The specific distribution of glycolipid-based blood group A antigens in human kidney related to A1/A2, Lewis, and secretor status of single individuals. A possible molecular explanation for the successful transplantation of A2 kidneys into O recipients. Transplantation 1986, 42, 88–91. [Google Scholar] [PubMed]
- Public Comment Archive. Available online: https://optn.transplant.hrsa.gov/governance/public-comment/public-comment-archive/ (accessed on 22 August 2022).
- Ueda, N.; Nishimura, K.; Yoshida, Y.; Hirai, T.; Kishikawa, H.; Ichikawa, Y. Living-donor kidney transplant from a type a donor to a type a subgroup recipient. Exp. Clin. Transplant. 2015, 13, 193–195. [Google Scholar] [PubMed]
- Fadeyi, E.A.; Stratta, R.J.; Farney, A.C.; Pomper, G.J. Successful ABO-Incompatible Renal Transplantation: Blood Group A1B Donor into A2B Recipient with Anti-A1 Isoagglutinins. Am. J. Clin. Pathol. 2016, 146, 268–271. [Google Scholar] [PubMed]
- Fadeyi, E.A.; Stratta, R.J.; Farney, A.C.; Pomper, G.J. Successful unintentional ABO-incompatible renal transplantation: Blood group A1B donor into an A2B recipient. Am. J. Clin. Pathol. 2014, 141, 724–726. [Google Scholar] [CrossRef] [PubMed]
- Basha, H.I.; Hussain, S.; Raichlin, E.; Gudipati, S.; Liebo, M.; McGee, E.; De Christopher, P.; Heroux, A. Impact of Blood Group A Subtyping on Heart Transplantation: A Single Center Experience. J. Heart Lung Transplant. 2019, 38, S394. [Google Scholar] [CrossRef]
- Stewart, S.; Winters, G.L.; Fishbein, M.C.; Tazelaar, H.D.; Kobashigawa, J.; Abrams, J.; Andersen, C.B.; Angelini, A.; Berry, G.J.; Burke, M.M.; et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J. Heart Lung Transplant. 2005, 24, 1710–1720. [Google Scholar] [CrossRef] [PubMed]
- Berry, G.J.; Burke, M.M.; Andersen, C.; Bruneval, P.; Fedrigo, M.; Fishbein, M.C.; Goddard, M.; Hammond, E.H.; Leone, O.; Marboe, C.; et al. The 2013 International Society for Heart and Lung Transplantation Working Formulation for the standardization of nomenclature in the pathologic diagnosis of antibody-mediated rejection in heart transplantation. J. Heart Lung Transplant. 2013, 32, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Predicted Heart Mass (PHM) Match Calculator. Available online: https://insights.unos.org/phm-calculator (accessed on 16 August 2022).
- Barten, M.J.; Schulz, U.; Beiras-Fernandez, A.; Berchtold-Herz, M.; Boeken, U.; Garbade, J.; Hirt, S.; Richter, M.; Ruhpawar, A.; Sandhaus, T.; et al. The clinical impact of donor-specific antibodies in heart transplantation. Transplant. Rev. 2018, 32, 207–217. [Google Scholar]
- Chan, J.; Kobashigawa, J.; Aintablian, T.L.; Dimbil, S.J.; Perry, P.A.; Patel, J.K.; Kittleson, M.M.; Czer, L.S.; Zarrini, P.; Velleca, A.; et al. Characterizing Predictors and Severity of Vasoplegia Syndrome After Heart Transplantation. Ann. Thorac. Surg. 2018, 105, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.F.; Omran, S.S.; Genuardi, M.V.; Horn, E.T.; Kilic, A.; Sciortino, C.M.; Keebler, M.E.; Kormos, R.L.; Hickey, G.W. Primary Graft Dysfunction in Heart Transplant Recipients-Risk Factors and Longitudinal Outcomes. ASAIO J. 2021, 68, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Patients with Certain Blood Groups Wait Much Longer for Heart Transplants. 2018. Available online: https://www.organdonation.nhs.uk/get-involved/news/patients-with-certain-blood-groups-wait-longer-for-heart-transplants/ (accessed on 12 September 2022).
- Montgomery, J.R.; Berger, J.C.; Warren, D.S.; James, N.T.; Montgomery, R.A.; Segev, D.L. Outcomes of ABO-incompatible kidney transplantation in the United States. Transplantation 2012, 93, 603–609. [Google Scholar]
- Rydberg, L. ABO-incompatibility in solid organ transplantation. Transfus. Med. 2001, 11, 325–342. [Google Scholar]
- Bryan, C.F.; Cherikh, W.S.; Sesok-Pizzini, D.A. A2/A2 B to B Renal Transplantation: Past, Present, and Future Directions. Am. J. Transplant. 2016, 16, 11–20. [Google Scholar] [PubMed]
- Kluger, M.D.; Guarrera, J.V.; Olsen, S.K.; Brown, R.S., Jr.; Emond, J.C.; Cherqui, D. Safety of blood group A2-to-O liver transplantation: An analysis of the United Network of Organ Sharing database. Transplantation 2012, 94, 526–531. [Google Scholar] [PubMed]
- Ge, J.; Roberts, J.P.; Lai, J.C. A2 liver transplantation across the ABO barrier: Increasing options in the donor pool? Clin. Liver Dis. 2017, 10, 135–138. [Google Scholar]
- Ott, G.Y.; Norman, D.; Ratkovec, R.R.; Hershberger, R.; Hosenpud, J.D.; Cobanoglu, A. ABO-incompatible heart transplantation: A special case for the A2 donor. J. Heart Lung Transplant. 1993, 12, 504–507. [Google Scholar] [PubMed]
- Pober, J.S.; Chih, S.; Kobashigawa, J.; Madsen, J.C.; Tellides, G. Cardiac allograft vasculopathy: Current review and future research directions. Cardiovasc. Res. 2021, 117, 2624–2638. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
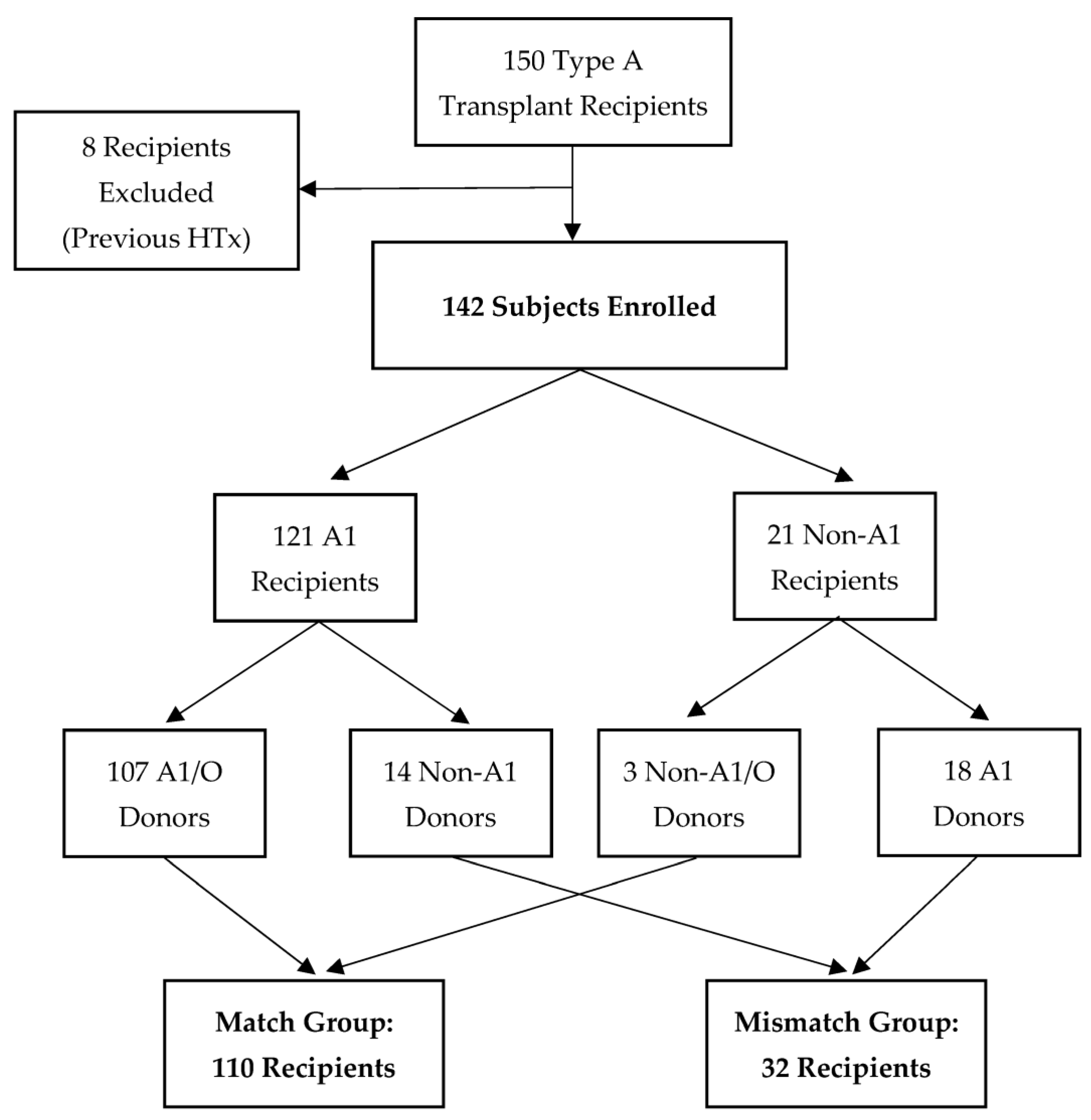
| A1 Donor-Recipient Match (n = 110) | A1 Donor-Recipient Mismatch (n = 32) | p-Value | |
|---|---|---|---|
| Recipient Age (Years) | 57.4 ± 12.9 | 55.2 ± 12.1 | 0.40 |
| Donor Age (Years) | 37.3 ± 12.8 | 34.9 ± 13.2 | 0.35 |
| Race | 0.02 | ||
| White | 80.9% (n = 89) | 62.5% (n = 20) | - |
| African-American | 12.7% (n = 14) | 12.5% (n = 4) | - |
| Asian | 3.6% (n = 4) | 6.3% (n = 2) | - |
| Other | 2.7% (n = 3) | 18.8% (n = 6) | - |
| BMI (kg/m2) | 25.1 ± 4.8 | 25.9 ± 4.2 | 0.41 |
| PHM | 1.08 ± 0.230 | 1.01 ± 0.163 | 0.10 |
| Female | 29.0% (n = 32) | 25.0% (n = 8) | 0.65 |
| Type of Cardiomyopathy | 0.63 | ||
| Nonischemic | 61.8% (n = 68) | 65.6% (n = 21) | - |
| Ischemic | 26.4% (n = 29) | 21.9% (n = 7) | - |
| Congenital | 0.9% (n = 1) | 3.1% (n = 1) | - |
| Restrictive/Infiltrative | 10.9% (n = 12) | 9.4% (n = 3) | - |
| Previous Diabetes | 33.6% (n = 37) | 31.3% (n = 10) | 0.80 |
| Previous Hypertension | 59.0% (n = 65) | 53.1% (n = 17) | 0.55 |
| Prior Cardiac Surgery | 41.8% (n = 46) | 34.4% (n = 11) | 0.45 |
| Cytomegalovirus Mismatch | 46.4% (n = 51) | 59.4% (n = 19) | 0.20 |
| Previous Pregnancy in Females | 65.6% (n = 21) | 50.0% (n = 4) | 0.44 |
| Prior Blood Transfusion | 30.9% (n = 34) | 31.3% (n = 10) | 0.97 |
| Pre-transplant PRA with MFI > 5000 | 15.5% (n = 17) | 6.3% (n = 2) | 0.24 |
| Pre-transplant Desensitization | 9.1% (n = 10) | 9.4% (n = 3) | 1.00 |
| Induction with ATG | 58.2% (n = 64) | 50.0% (n = 16) | 0.41 |
| Time on Waitlist (days) | 149.7 ± 269.8 | 153.8 ± 254.4 | 0.94 |
| Urgent Status at Transplant 2 | 66.4% (n = 73) | 65.6% (n = 21) | 0.94 |
| Mechanical Circulatory Support | 41.8% (n = 46) | 43.8% (n = 14) | 0.85 |
| Pre-transplant Creatinine (mg/dL) | 1.5 ± 0.9 | 1.6 ± 1.8 | 0.69 |
| Ischemic Time (min) | 181.7 ± 52.7 | 195.4 ± 44.0 | 0.18 |
| A1 Donor-Recipient Match (n = 110) | A1 Donor-Recipient Mismatch (n = 32) | p-Value | |
|---|---|---|---|
| Primary Graft Dysfunction | 12.7% (n = 14) | 18.8% (n = 6) | 0.40 |
| Vasoplegia | 11.8% (n = 13) | 15.6% (n = 5) | 0.56 |
| Intensive Care Unit Length of Stay (Days) | 6.5 ± 3.6 | 8.0 ± 5.8 | 0.08 |
| Hospital Length of Stay (Days) | 13.5 ± 8.4 | 17.1 ± 10.2 | 0.04 |
| Ejection Fraction (%) 2 | 62.6 ± 5.2 | 60.9 ± 4.7 | 0.11 |
| Donor-Specific Antibodies 2 | 17.3% (n = 19) | 9.4% (n = 3) | 0.41 |
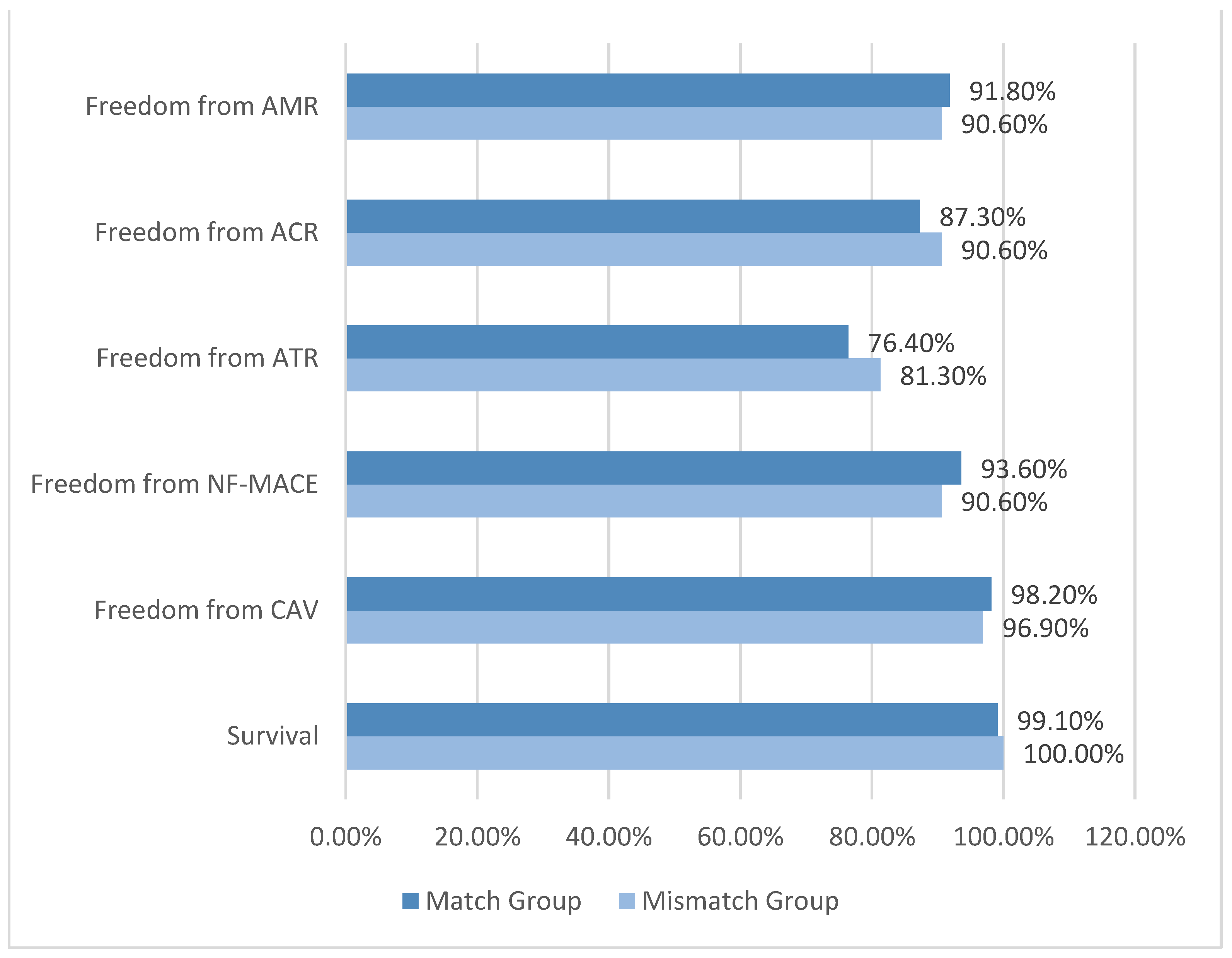
| Survival 2 | 99.1% | 100.0% | 0.58 |
| Freedom from CAV2 | 98.2% | 96.9% | 0.67 |
| Freedom from NF-MACE 2 | 93.6% | 90.6% | 0.52 |
| Freedom from ATR 2 | 76.4% | 81.3% | 0.61 |
| Freedom from ACR 2 | 87.3% | 90.6% | 0.62 |
| Freedom from AMR 2 | 91.8% | 90.6% | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, L.; Kim, S.; Klapper, E.; Kobashigawa, J.A.; Kittleson, M.M. Blood Type A1 Mismatch Does Not Affect Heart Transplant Outcomes at One Year. J. Clin. Med. 2023, 12, 1337. https://doi.org/10.3390/jcm12041337
Cao L, Kim S, Klapper E, Kobashigawa JA, Kittleson MM. Blood Type A1 Mismatch Does Not Affect Heart Transplant Outcomes at One Year. Journal of Clinical Medicine. 2023; 12(4):1337. https://doi.org/10.3390/jcm12041337
Chicago/Turabian StyleCao, Louie, Seongkyu Kim, Ellen Klapper, Jon A. Kobashigawa, and Michelle M. Kittleson. 2023. "Blood Type A1 Mismatch Does Not Affect Heart Transplant Outcomes at One Year" Journal of Clinical Medicine 12, no. 4: 1337. https://doi.org/10.3390/jcm12041337