

Cardiac Contractility Modulation Therapy in Patients with Amyloid Cardiomyopathy and Heart Failure, Case Report, Review of the Biophysics of CCM Function, and AMY-CCM Registry Presentation
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
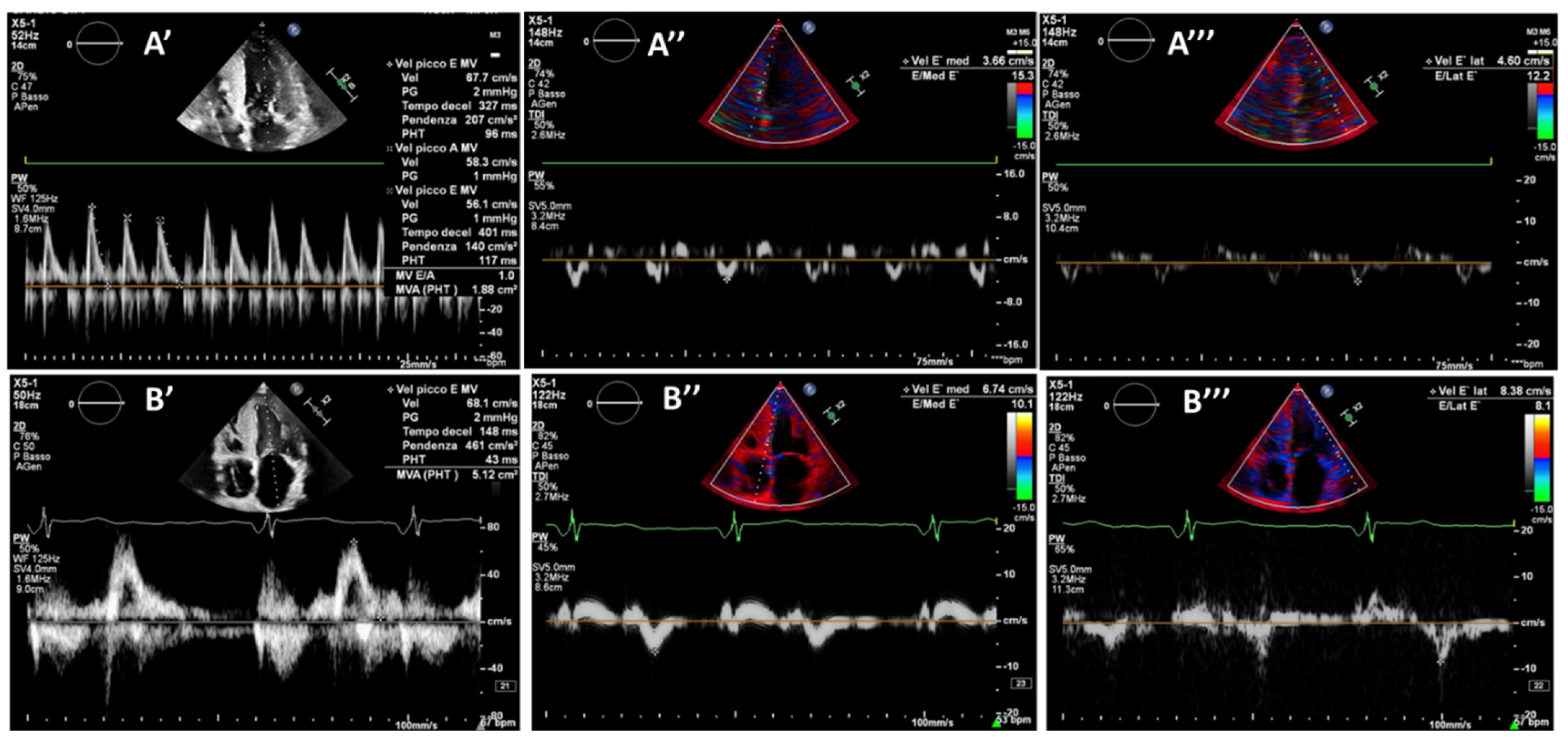
2. Case Report: Wild Type TTR
3. Discussion and Review of CCM Function
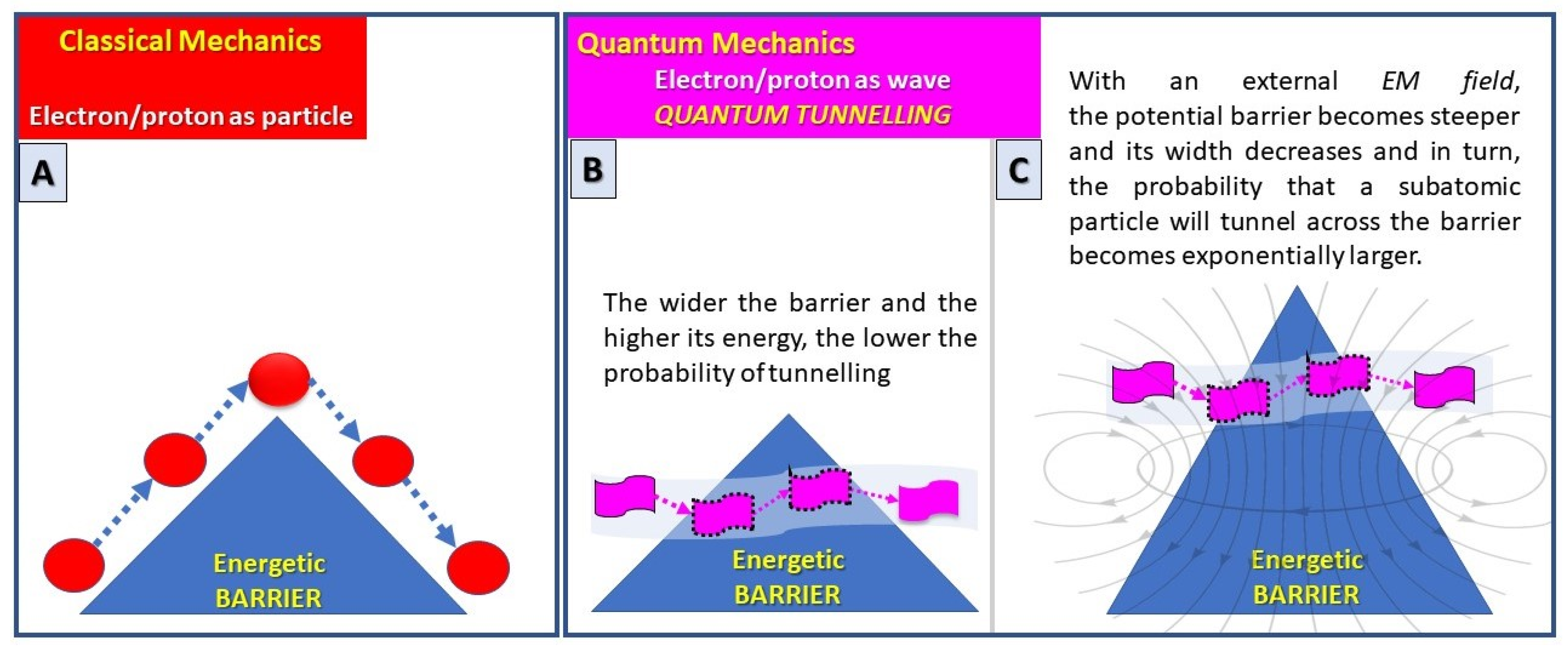
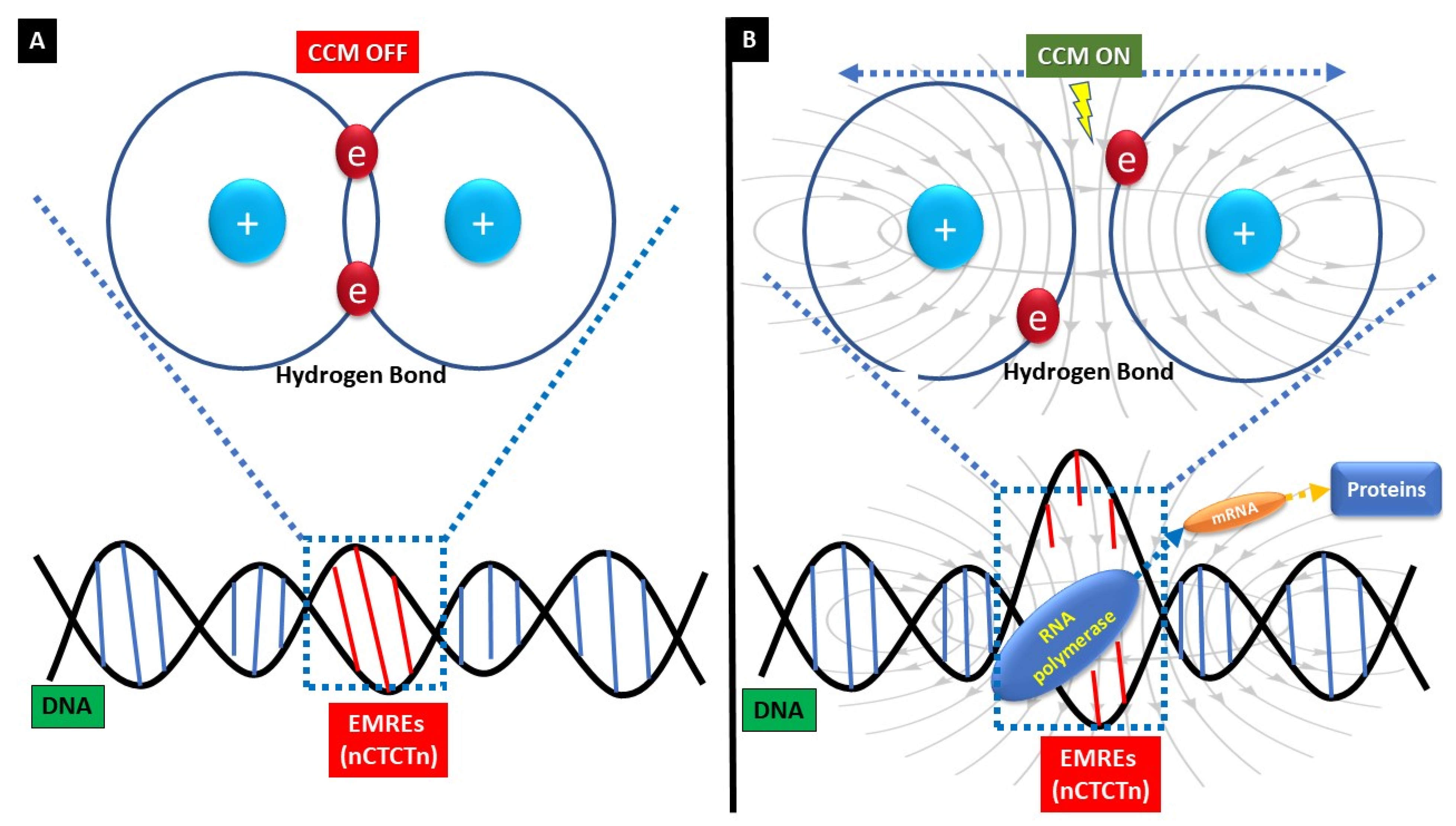
4. CCM “Pharmacodynamic”: Are We Dealing with Quantum Medicine?
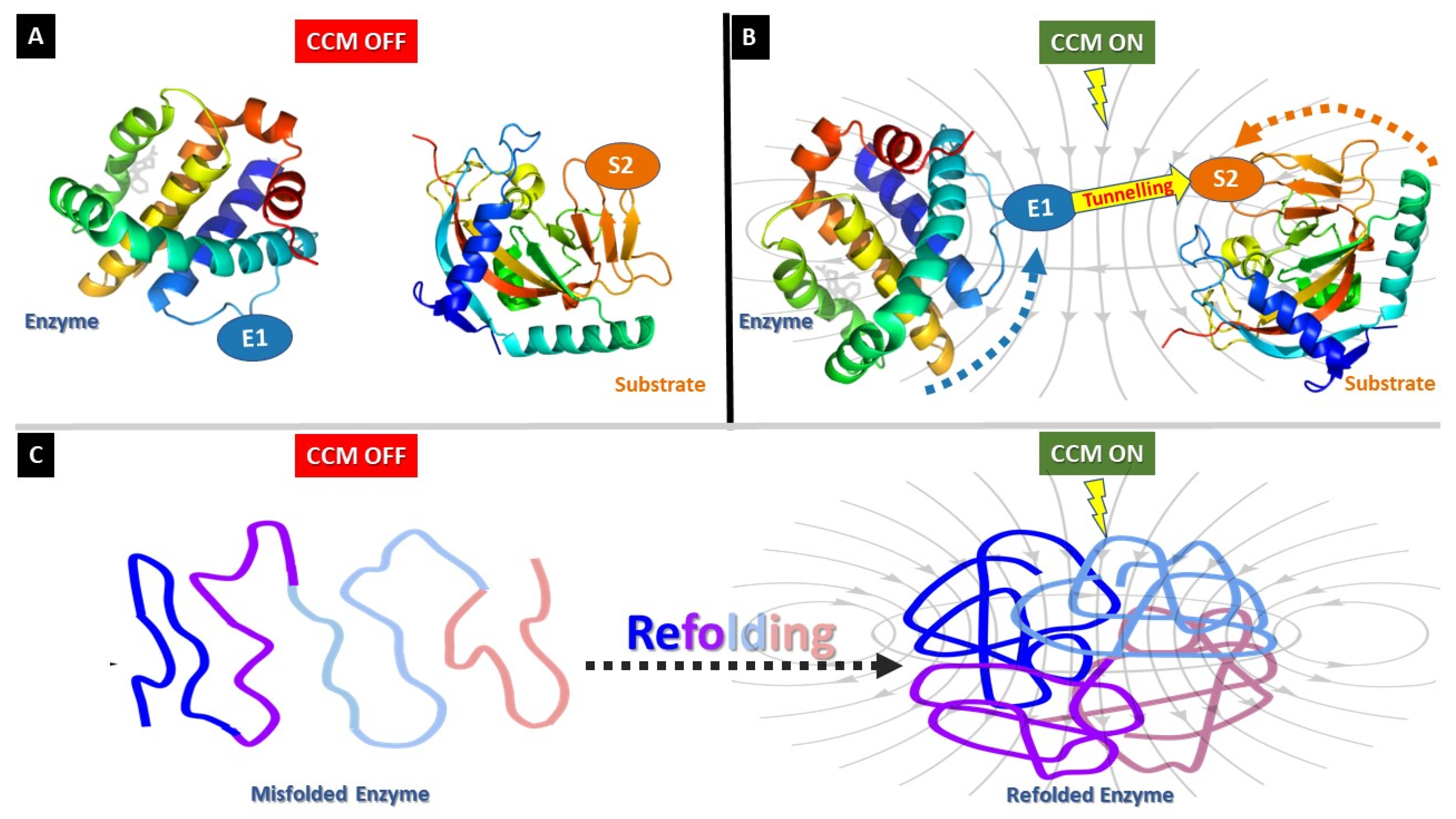
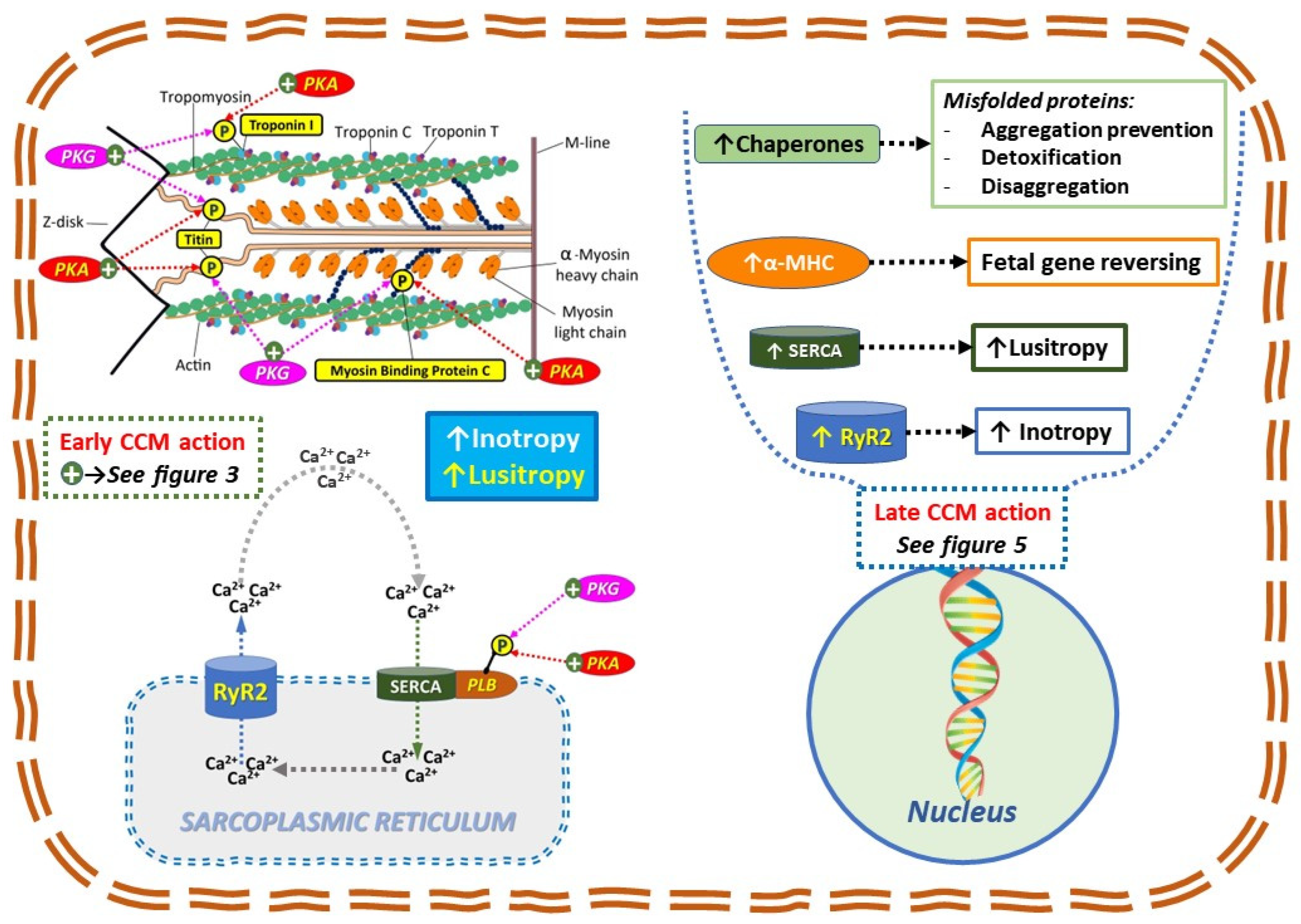
5. CCM Early-Onset Effects: Enzymes Modulation
6. CCM Late-Onset Effects: Maladaptive Fetal Gene Remodeling
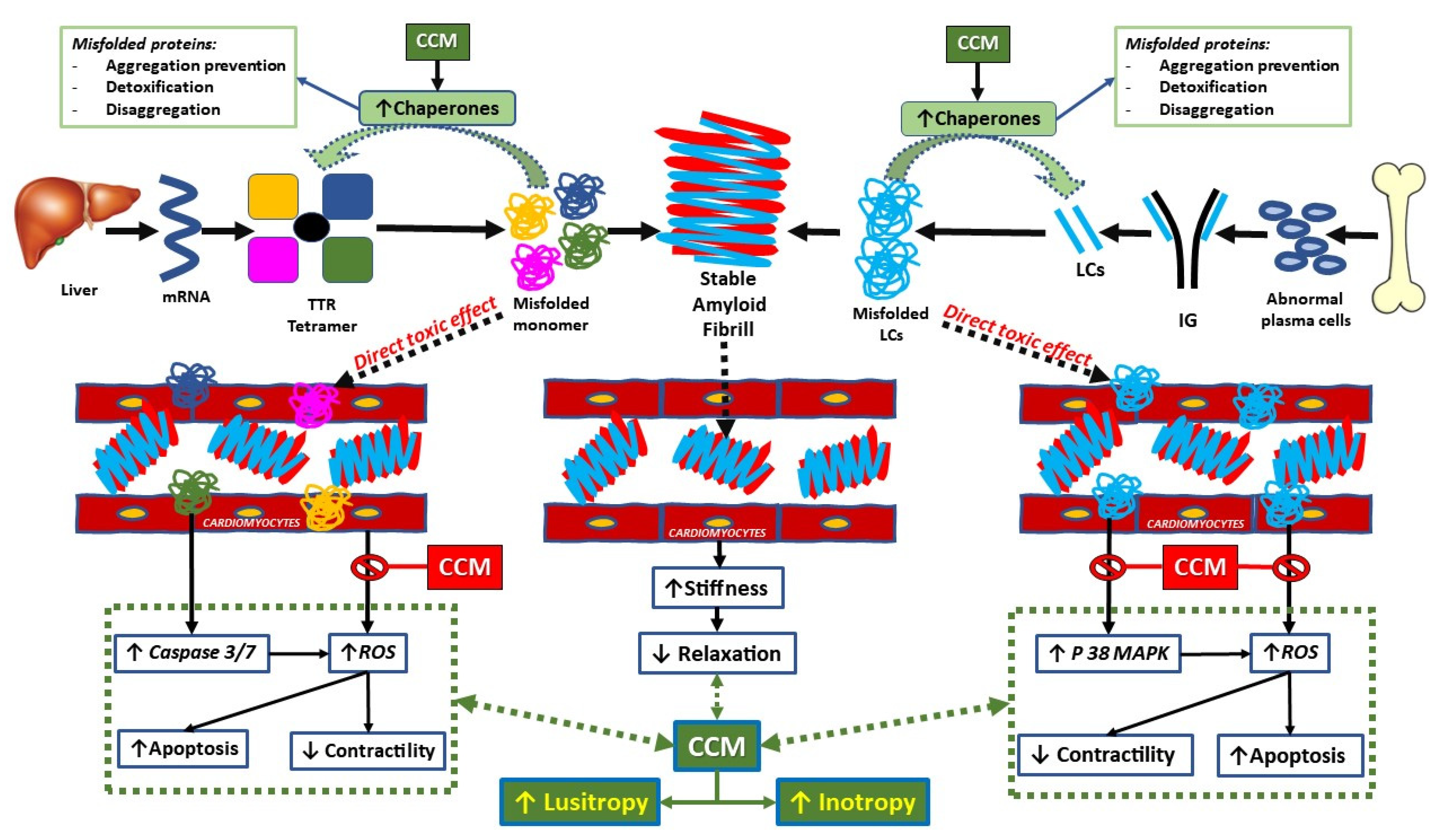
7. Cardiac Contractility Modulation Therapy in Amyloid Cardiomyopathy Patients with Heart Failure (AMY-CCM: ClinicalTrials.gov Identifier: NCT05167799)
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liao, R.; Ward, J. Amyloid Cardiomyopathy: Disease on the Rise. Circ. Res. 2017, 120, 1865–1867. [Google Scholar] [CrossRef]
- Abraham, W.T.; Kuck, K.-H.; Goldsmith, R.L.; Lindenfeld, J.; Reddy, V.Y.; Carson, P.E.; Mann, D.L.; Saville, B.; Parise, H.; Chan, R.; et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. JACC Heart Fail. 2018, 6, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Cappannoli, L.; Scacciavillani, R.; Rocco, E.; Perna, F.; Narducci, M.L.; Vaccarella, M.; D’Amario, D.; Pelargonio, G.; Massetti, M.; Crea, F.; et al. Cardiac contractility modulation for patient with refractory heart failure: An updated evidence-based review. Heart Fail. Rev. 2021, 26, 227–235. [Google Scholar] [CrossRef]
- Kuschyk, J.; Nägele, H.; Heinz-Kuck, K.; Butter, C.; Lawo, T.; Wietholt, D.; Roeger, S.; Gutterman, D.; Burkhoff, D.; Rousso, B.; et al. Cardiac contractility modulation treatment in patients with symptomatic heart failure despite optimal medical therapy and cardiac resynchronization therapy (CRT). Int. J. Cardiol. 2019, 277, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Tint, D.; Florea, R.; Micu, S. New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment. J. Clin. Med. 2019, 8, 588. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Borggrefe, M.; Neuser, H.; Ohlow, M.-A.; Röger, S.; Goette, A.; Remppis, B.A.; Kuck, K.; Najarian, K.B.; Gutterman, D.D.; et al. Cardiac contractility modulation improves long-term survival and hospitalizations in heart failure with reduced ejection fraction. Eur. J. Heart Fail. 2019, 21, 1103–1113. [Google Scholar] [CrossRef]
- Tschöpe, C.; Van Linthout, S.; Spillmann, F.; Klein, O.; Biewener, S.; Remppis, A.; Gutterman, D.; Linke, W.A.; Pieske, B.; Hamdani, N.; et al. Cardiac contractility modulation signals improve exercise intolerance and maladaptive regulation of cardiac key proteins for systolic and diastolic function in HFpEF. Int. J. Cardiol. 2016, 203, 1061–1066. [Google Scholar] [CrossRef]
- Lyon, A.R.; Samara, M.A.; Feldman, D.S. Cardiac contractility modulation therapy in advanced systolic heart failure. Nat. Rev. Cardiol. 2013, 10, 584–598. [Google Scholar] [CrossRef]
- Butter, C.; Rastogi, S.; Minden, H.-H.; Meyhöfer, J.; Burkhoff, D.; Sabbah, H.N. Cardiac Contractility Modulation Electrical Signals Improve Myocardial Gene Expression in Patients with Heart Failure. J. Am. Coll. Cardiol. 2008, 51, 1784–1789. [Google Scholar] [CrossRef]
- Blank, M.; Goodman, R. A mechanism for stimulation of biosynthesis by electromagnetic fields: Charge transfer in DNA and base pair separation. J. Cell. Physiol. 2008, 214, 20–26. [Google Scholar] [CrossRef]
- Albery, W.J.; Knowles, J.R. Evolution of enzyme function and the development of catalytic efficiency. Biochemistry 1976, 15, 5631–5640. [Google Scholar] [CrossRef]
- Kraut, J. How Do Enzymes Work? Science 1988, 242, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, M.J.; Scrutton, N.S. Enzymology takes a quantum leap forward. Philos. Trans. Ser. A Math. Phys. Eng. Sci. 2000, 358, 367–386. [Google Scholar] [CrossRef] [PubMed]
- Johannissen, L.O.; Hay, S.; Scrutton, N.S. Nuclear quantum tunnelling in enzymatic reactions—An enzymologist’s perspective. Phys. Chem. Chem. Phys. 2015, 17, 30775–30782. [Google Scholar] [CrossRef] [PubMed]
- Klinman, J.P.; Kohen, A. Hydrogen Tunneling Links Protein Dynamics to Enzyme Catalysis. Annu. Rev. Biochem. 2013, 82, 471–496. [Google Scholar] [CrossRef]
- Marcus, R.; Sutin, N. Electron transfers in chemistry and biology. Biochim. Et Biophys. Acta BBA Rev. Bioenerg. 1985, 811, 265–322. [Google Scholar] [CrossRef]
- Devault, D. Quantum mechanical tunnelling in biological systems. Q. Rev. Biophys. 1980, 13, 387–564. [Google Scholar] [CrossRef]
- Miklavčič, D. Handbook of Electroporation, 1st ed.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Li, Y.; Zhang, S.; Bao, Z.; Sun, N.; Lin, S. Exploring the activation mechanism of alcalase activity with pulsed electric field treatment: Effects on enzyme activity, spatial conformation, molecular dynamics simulation and molecular docking parameters. Innov. Food Sci. Emerg. Technol. 2022, 76, 102918. [Google Scholar] [CrossRef]
- Masgrau, L.; Roujeinikova, A.; Johannissen, L.O.; Hothi, P.; Basran, J.; Ranaghan, K.E.; Mulholland, A.J.; Sutcliffe, M.J.; Scrutton, N.S.; Leys, D. Atomic Description of an Enzyme Reaction Dominated by Proton Tunneling. Science 2006, 312, 237–241. [Google Scholar] [CrossRef]
- Moser, C.C.; Anderson, R.; Dutton, P.L. Guidelines for tunneling in enzymes. Biochim. Et Biophys. Acta BBA Bioenerg. 2010, 1797, 1573–1586. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.J.; Chiang, H.; Fu, Y.T.; Yu, Y.N.; Xie, H.Y.; Lu, D.Q. Exposure to 50 Hz Electromagnetic Fields Induces the Phosphorylation and Activity of Stress-Activated Protein Kinase in Cultured Cells. Electromagn. Biol. Med. 2001, 20, 415–423. [Google Scholar] [CrossRef]
- Imai, M.; Rastogi, S.; Gupta, R.C.; Mishra, S.; Sharov, V.G.; Stanley, W.C.; Mika, Y.; Rousso, B.; Burkhoff, D.; Ben-Haim, S.; et al. Therapy with Cardiac Contractility Modulation Electrical Signals Improves Left Ventricular Function and Remodeling in Dogs with Chronic Heart Failure. J. Am. Coll. Cardiol. 2007, 49, 2120–2128. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Kherad, B.; Klein, O.; Lipp, A.; Blaschke, F.; Gutterman, D.; Burkhoff, D.; Hamdani, N.; Spillmann, F.; Van Linthout, S. Cardiac contractility modulation: Mechanisms of action in heart failure with reduced ejection fraction and beyond. Eur. J. Heart Fail. 2019, 21, 14–22. [Google Scholar] [CrossRef]
- Rajabi, M.; Kassiotis, C.; Razeghi, P.; Taegtmeyer, H. Return to the fetal gene program protects the stressed heart: A strong hypothesis. Heart Fail. Rev. 2007, 12, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Dang, Y.; Li, Y.; Hao, Q.; Li, R.; Qi, X. Cardiac Contractility Modulation Attenuate Myocardial Fibrosis by Inhibiting TGF-β1/Smad3 Signaling Pathway in a Rabbit Model of Chronic Heart Failure. Cell. Physiol. Biochem. 2016, 39, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Guan, J.; Jiang, B.; Brenner, D.A.; del Monte, F.; Ward, J.E.; Connors, L.H.; Sawyer, D.B.; Semigran, M.J.; Macgillivray, T.E.; et al. Amyloidogenic light chains induce cardiomyocyte contractile dysfunction and apoptosis via a non-canonical p38α MAPK pathway. Proc. Natl. Acad. Sci. USA 2010, 107, 4188–4193. [Google Scholar] [CrossRef]
- Wentink, A.; Nussbaum-Krammer, C.; Bukau, B. Modulation of Amyloid States by Molecular Chaperones. Cold Spring Harb. Perspect. Biol. 2019, 11, a033969. [Google Scholar] [CrossRef]
- Wentink, A.S.; Nillegoda, N.B.; Feufel, J.; Ubartaitė, G.; Schneider, C.P.; Rios, P.D.L.; Hennig, J.; Barducci, A.; Bukau, B. Molecular dissection of amyloid disaggregation by human HSP70. Nature 2020, 587, 483–488. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchese, P.; Gennaro, F.; Mazzotta, G.; Acciarri, C.; Amabili, S.; Bonanni, C.; D’Antonio, A.; Delfino, D.; Di Vito, L.; Partemi, M.; et al. Cardiac Contractility Modulation Therapy in Patients with Amyloid Cardiomyopathy and Heart Failure, Case Report, Review of the Biophysics of CCM Function, and AMY-CCM Registry Presentation. J. Clin. Med. 2023, 12, 1184. https://doi.org/10.3390/jcm12031184
Marchese P, Gennaro F, Mazzotta G, Acciarri C, Amabili S, Bonanni C, D’Antonio A, Delfino D, Di Vito L, Partemi M, et al. Cardiac Contractility Modulation Therapy in Patients with Amyloid Cardiomyopathy and Heart Failure, Case Report, Review of the Biophysics of CCM Function, and AMY-CCM Registry Presentation. Journal of Clinical Medicine. 2023; 12(3):1184. https://doi.org/10.3390/jcm12031184
Chicago/Turabian StyleMarchese, Procolo, Francesca Gennaro, Giovanni Mazzotta, Claudia Acciarri, Stenio Amabili, Carlo Bonanni, Antonella D’Antonio, Domenico Delfino, Luca Di Vito, Manrico Partemi, and et al. 2023. "Cardiac Contractility Modulation Therapy in Patients with Amyloid Cardiomyopathy and Heart Failure, Case Report, Review of the Biophysics of CCM Function, and AMY-CCM Registry Presentation" Journal of Clinical Medicine 12, no. 3: 1184. https://doi.org/10.3390/jcm12031184