
Effects of COVID-19 Lockdown on Heart Failure Patients: A Quasi-Experimental Study
 , , , , , , ,
, , , , , , ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Sample
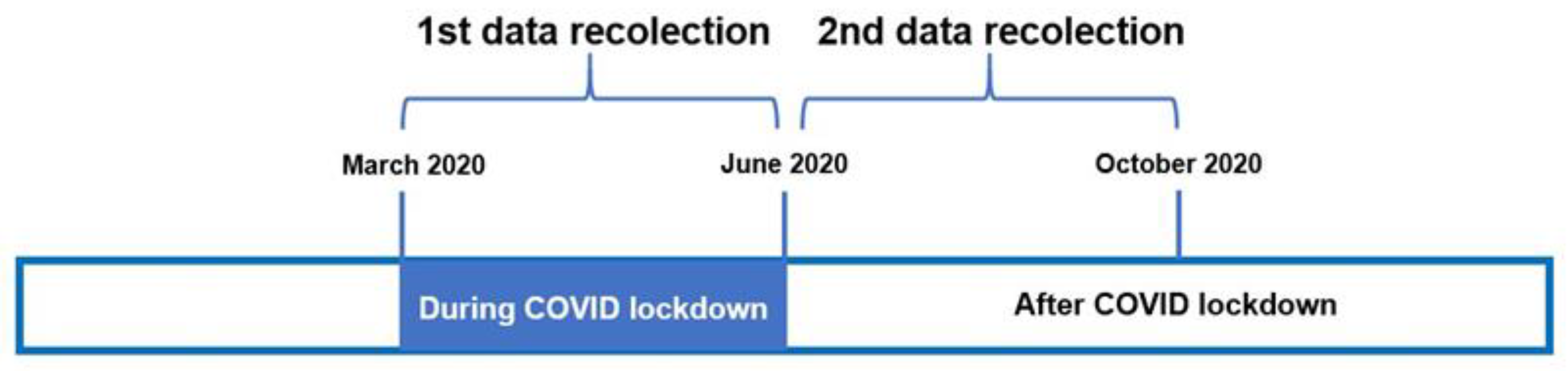
2.3. Procedure
2.4. Outcomes and Measures
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
4.1. Physical Activity (PA) during Lockdown
4.2. Quality of Life during Lockdown
4.3. Sleep Quality during Lockdown
4.4. Implications and Future Lines of Action
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ploumpidis, D. Living with COVID-19. Psychiatriki 2020, 31, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Vetrovsky, T.; Frybova, T.; Gant, I.; Semerad, M.; Cimler, R.; Bunc, V.; Siranec, M.; Miklikova, M.; Vesely, J.; Griva, M.; et al. The detrimental effect of COVID-19 nationwide quarantine on accelerometer-assessed physical activity of heart failure patients. ESC Heart Fail. 2020, 7, 2093–2097. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: A Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, A.K.; Sharma, N.; Samuel, A.J. Impact of Coronavirus disease-19 (COVID-19) lockdown on physical activity and energy expenditure among physiotherapy professionals and students using web-based open E-survey sent through WhatsApp, Facebook and Instagram messengers. Clin. Epidemiol. Glob. Health 2020, 9, 78–84. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Sell, N.M.; Silver, J.K.; Rando, S.; Draviam, A.C.; Mina, D.S.; Qadan, M. Prehabilitation Telemedicine in Neoadjuvant Surgical Oncology Patients During the Novel COVID-19 Coronavirus Pandemic. Ann. Surg. 2020, 272, e81–e83. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Chu, D.-T.; Ngoc, S.-M.V.; Thi, H.V.; Thi, Y.-V.N.; Ho, T.-T.; Hoang, V.-T.; Singh, V.; Al-Tawfiq, J.A. COVID-19 in Southeast Asia: Current status and perspectives. Bioengineered 2022, 13, 3797–3809. [Google Scholar] [CrossRef]
- Schwalb, A.; Armyra, E.; Méndez-Aranda, M.; Ugarte-Gil, C. COVID-19 in Latin America and the Caribbean: Two years of the pandemic. J. Intern. Med. 2022, 292, 409–427. [Google Scholar] [CrossRef]
- American Heart Association. What Is Heart Failure. 2023. Available online: https://www.heart.org/en/health-topics/heart-failure/what-is-heart-failure (accessed on 4 November 2023).
- Schmitt, J.; Wenzel, B.; Brüsehaber, B.; Anguera, I.; de Sousa, J.; Nölker, G.; Bulava, A.; Marques, P.; Hatala, R.; Golovchiner, G.; et al. Impact of lockdown during COVID-19 pandemic on physical activity and arrhythmia burden in heart failure patients. Pacing Clin. Electrophysiol. 2022, 45, 471–480. [Google Scholar] [CrossRef]
- Harrison, S.L.; Buckley, B.J.R.; Rivera-Caravaca, J.M.; Zhang, J.; Lip, G.Y.H. Cardiovascular risk factors, cardiovascular disease, and COVID-19: An umbrella review of systematic reviews. Eur. Heart J.—Qual. Care Clin. Outcomes 2021, 7, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Bhaskarabhatla, K.V.; Birrer, R. Physical Activity and Diabetes Mellitus. Compr. Ther. 2005, 31, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Lucia, A.; Yvert, T.; Ruiz-Casado, A.; Pareja-Galeano, H.; Santos-Lozano, A.; Fiuza-Luces, C.; Garatachea, N.; Lippi, G.; Bouchard, C.; et al. Physical Inactivity and Low Fitness Deserve More Attention to Alter Cancer Risk and Prognosis. Cancer Prev. Res. 2015, 8, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Castrogiovanni, P.; Trovato, F.M.; Szychlinska, M.A.; Nsir, H.; Imbesi, R.; Musumeci, G. The importance of physical activity in osteoporosis. From the molecular pathways to the clinical evidence. Histol. Histopathol. 2016, 31, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Vasankari, V.; Husu, P.; Vähä-Ypyä, H.; Suni, J.H.; Tokola, K.; Borodulin, K.; Wennman, H.; Halonen, J.; Hartikainen, J.; Sievänen, H.; et al. Subjects with cardiovascular disease or high disease risk are more sedentary and less active than their healthy peers. BMJ Open Sport Exerc. Med. 2018, 4, e000363. [Google Scholar] [CrossRef] [PubMed]
- Van Bakel, B.M.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.; Eijsvogels, T.M. Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11929. [Google Scholar] [CrossRef]
- Van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Impact of COVID-19 lockdown on physical activity and sedentary behaviour in Dutch cardiovascular disease patients. Neth. Heart J. 2021, 29, 273–279. [Google Scholar] [CrossRef]
- Brasca, F.M.A.; Casale, M.C.; Canevese, F.L.; Tortora, G.; Pagano, G.; Botto, G.L. Physical Activity in Patients with Heart Failure During and After COVID-19 Lockdown: Single-Center Observational Retrospective Study. JMIR Cardio 2022, 6, e30661. [Google Scholar] [CrossRef]
- Cunha, P.M.; Ribeiro, A.S.; Tomeleri, C.M.; Schoenfeld, B.J.; Silva, A.M.; Souza, M.F.; Nascimento, M.A.; Sardinha, L.B.; Cyrino, E.S. The effects of resistance training volume on osteosarcopenic obesity in older women. J. Sports Sci. 2018, 36, 1564–1571. [Google Scholar] [CrossRef]
- Hwang, S.; Liao, W.; Huang, T. Predictors of quality of life in patients with heart failure. Jpn. J. Nurs. Sci. 2014, 11, 290–298. [Google Scholar] [CrossRef]
- Sang, X.; Menhas, R.; Saqib, Z.A.; Mahmood, S.; Weng, Y.; Khurshid, S.; Iqbal, W.; Shahzad, B. The Psychological Impacts of COVID-19 Home Confinement and Physical Activity: A Structural Equation Model Analysis. Front. Psychol. 2021, 11, 614770. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Sang, X.; Menhas, R.; Xu, X.; Khurshid, S.; Mahmood, S.; Weng, Y.; Huang, J.; Cai, Y.; Shahzad, B.; et al. The Influence of COVID-19 Pandemic on Physical Health–Psychological Health, Physical Activity, and Overall Well-Being: The Mediating Role of Emotional Regulation. Front. Psychol. 2021, 12, 667461. [Google Scholar] [CrossRef] [PubMed]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef] [PubMed]
- Falkingham, J.; Evandrou, M.; Vlachantoni, A.; Qin, M. Sleep Problems and New Occurrence of Chronic Conditions during the COVID-19 Pandemic in the UK. Int. J. Environ. Res. Public Health 2022, 19, 15664. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of COVID-19 Lockdown on Mental Health and Sleep Disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Silva, P.C.; Neto, O.P.d.A.; Resende, E.S. Epidemiological profile, cardiopulmonary fitness and health-related quality of life of patients with heart failure: A longitudinal study. Health Qual. Life Outcomes 2021, 19, 129. [Google Scholar] [CrossRef]
- Peng, M.; Mo, B.; Liu, Y.; Xu, M.; Song, X.; Liu, L.; Fang, Y.; Guo, T.; Ye, J.; Yu, Z.; et al. Prevalence, risk factors and clinical correlates of depression in quarantined population during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 119–124. [Google Scholar] [CrossRef]
- Martínez-Quintana, E.; Vega-Acedo, L.d.C.; Santana-Herrera, D.; Pérez-Acosta, C.; Medina-Gil, J.M.; Muñoz-Díaz, E.; Rodríguez-González, F. Mental well-being among patients with congenital heart disease and heart failure during the COVID-19 pandemic. Am. J. Cardiovasc. Dis. 2021, 11, 618–623. [Google Scholar]
- Faulkner, J.; O’brien, W.J.; McGrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical activity, mental health and well-being of adults during initial COVID-19 containment strategies: A multi-country cross-sectional analysis. J. Sci. Med. Sport 2020, 24, 320–326. [Google Scholar] [CrossRef]
- Beck, F.; Léger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P. The Coconel Group COVID-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2021, 30, e13119. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Hurtig-Wennlöf, A.; Hagströmer, M.; Olsson, L.A. The International Physical Activity Questionnaire modified for the elderly: Aspects of validity and feasibility. Public Health Nutr. 2010, 13, 1847–1854. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, F.J.R. Medición de la Actividad Física en Personas Mayores de 65 Años Mediante El Ipaq-E: Validez de Contenido, Fiabilidad y Factores Asociados. Rev. Esp. Salud. Pública. 2017, 91, e1–e12. [Google Scholar]
- Cantril, H. The Pattern of Human Concerns; Rutgers University: New Brunswick, NJ, USA, 1965. [Google Scholar]
- Jaarsma, T.; Kastermans, M.C. Recovery and Quality of Life One Year after Coronary Artery Bypass Grafting. Scand. J. Caring Sci. 1997, 11, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, L.S.; Brodsky, M.; Schron, E.; Chung, M.; Rocco, T.; Lader, E.; Constantine, M.; Sheppard, R.; Holmes, D.; Mateski, D.; et al. Quality of life in atrial fibrillation: The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am. Heart J. 2005, 149, 112–120. [Google Scholar] [CrossRef]
- Senten, M.C. The Well-Being of Patients Having Coronary Artery Bypass Surgery: A Test of Orem’s Self-Care Nursing Theory. Ph.D. Thesis, Maastricht University, Maastricht, The Netherlands, 1991. [Google Scholar]
- Jaarsma, T.; Halfens, R.; Abu-Saad, H.H.; Dracup, K.; Stappers, J.; van Ree, J. Quality of life in older patients with systolic and diastolic heart failure. Eur. J. Heart Fail. 1999, 1, 151–160. [Google Scholar] [CrossRef]
- Levin, K.A.; Currie, C. Reliability and Validity of an Adapted Version of the Cantril Ladder for Use with Adolescent Samples. Soc. Indic. Res. 2014, 119, 1047–1063. [Google Scholar] [CrossRef]
- Czapinski, J. Illusions and Biases in Psychological Well Being: An “Onion” Theory of Happiness. In Working Meeting of ISR and ISS; Institute for Social Studies, University of Warsaw: Warsaw, Poland, 2001. [Google Scholar]
- Hellström, A.; Hagell, P.; Fagerström, C.; Willman, A. Measurement properties of the Minimal Insomnia Symptom Scale (MISS) in an elderly population in Sweden. BMC Geriatr. 2010, 10, 84. [Google Scholar] [CrossRef]
- Broman, J.-E.; Smedje, H.; Mallon, L.; Hetta, J. The Minimal Insomnia Symptom Scale (MISS). Upsala J. Med. Sci. 2008, 113, 131–142. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Kirsch, M.; Vitiello, D. The COVID-19 Pandemic Lowers Active Behavior of Patients with Cardiovascular Diseases, Healthy Peoples and Athletes. Int. J. Environ. Res. Public Health 2022, 19, 1108. [Google Scholar] [CrossRef]
- Kim, K.; Zhang, S.; Ding, P.; Wang, Y.; Yim, B.H.; Hu, Z.; Sui, S. Changes in Physical Activity and Health Indicators among Koreans during the COVID-19 Pandemic: Comparison between 2019 and 2020. Healthcare 2022, 10, 2549. [Google Scholar] [CrossRef] [PubMed]
- Rees-Punia, E.; Newton, C.C.; Rittase, M.H.; Hodge, R.A.; Nielsen, J.; Cunningham, S.; Teras, L.R.; Patel, A. Prospective changes in physical activity, sedentary time and sleep during the COVID-19 pandemic in a US-based cohort study. BMJ Open 2021, 11, e053817. [Google Scholar] [CrossRef] [PubMed]
- Van Erck, D.; Dolman, C.D.; Snaterse, M.; Tieland, M.; Driessen, A.H.G.; Weijs, P.J.M.; Reimer, W.J.M.S.O.; Henriques, J.P.; Schoufour, J.D. Physical activity, dietary intake and quality of life during COVID-19 lockdown in patients awaiting transcatheter aortic valve implantation. Neth. Heart J. 2021, 29, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Mukherjee, A.; Bhattacharyya, B.; Mohanakumar, K.; Biswas, A. Quality of life and concerns of parkinson’s disease patients and their caregivers during COVID-19 pandemic: An indian study. Ann. Indian Acad. Neurol. 2022, 25, 676. [Google Scholar] [CrossRef] [PubMed]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in Times of Lockdown: An Analysis of the Impact of COVID-19 on Levels and Patterns of Exercise among Adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2020, 18, 210. [Google Scholar] [CrossRef] [PubMed]
- Dobler, C.L.; Krüger, B.; Strahler, J.; Weyh, C.; Gebhardt, K.; Tello, K.; Ghofrani, H.A.; Sommer, N.; Gall, H.; Richter, M.J.; et al. Physical Activity and Mental Health of Patients with Pulmonary Hypertension during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 4023. [Google Scholar] [CrossRef] [PubMed]
- Kite, C.; Atkinson, L.; McGregor, G.; Clark, C.C.T.; Brown, J.E.; Kyrou, I.; Randeva, H.S. Sleep Disruption and Depression, Stress and Anxiety Levels in Women with Polycystic Ovary Syndrome (PCOS) During the Lockdown Measures for COVID-19 in the UK. Front. Glob. Women’s Health 2021, 2, 649104. [Google Scholar] [CrossRef]
- ElHafeez, S.A.; Cruz, M.M.E.; Gouda, S.; Nofal, M.; Fayed, A.; Ghazy, R.M.; Mekky, J. Sleep quality and anxiety among Egyptian population during COVID-19 pandemic. Sleep Sci. 2022, 15, 8–16. [Google Scholar] [CrossRef]
- Doukky, R.; Mangla, A.; Ibrahim, Z.; Poulin, M.-F.; Avery, E.; Collado, F.M.; Kaplan, J.; Richardson, D.; Powell, L.H. Impact of Physical Inactivity on Mortality in Patients with Heart Failure. Am. J. Cardiol. 2016, 117, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Akar, J.G.; Bao, H.; Jones, P.W.; Wang, Y.; Varosy, P.D.; Masoudi, F.A.; Stein, K.M.; Saxon, L.A.; Normand, S.-L.T.; Curtis, J.P.; et al. Use of Remote Monitoring Is Associated with Lower Risk of Adverse Outcomes Among Patients With Implanted Cardiac Defibrillators. Circ. Arrhythmia Electrophysiol. 2015, 8, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.T.; Treskes, R.W.; Caiani, E.G.; Casado-Arroyo, R.; Cowie, M.R.; Dilaveris, P.; Duncker, D.; Di Rienzo, M.; Frederix, I.; De Groot, N.; et al. ESC working group on e-cardiology position paper: Use of commercially available wearable technology for heart rate and activity tracking in primary and secondary cardiovascular prevention—In collaboration with the European Heart Rhythm Association, European Association of Preventive Cardiology, Association of Cardiovascular Nursing and Allied Professionals, Patient Forum, and the Digital Health Committee. Eur. Heart J.—Digit. Health 2021, 2, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Shakhovska, N.; Fedushko, S.; Greguš ml., M.; Melnykova, N.; Shvorob, I.; Syerov, Y. Big Data analysis in development of personalized medical system. Procedia Comput. Sci. 2019, 160, 229–234. [Google Scholar] [CrossRef]
- Scherrenberg, M.; Wilhelm, M.; Hansen, D.; Völler, H.; Cornelissen, V.; Frederix, I.; Kemps, H.; Dendale, P. The future is now: A call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 524–540. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- European Commission. The Digital Economy and Society Index (DESI); European Commission: Brussels, Belgium, 2022. [Google Scholar]


{kind=link}
| Intra-Observer Reliability | Internal Consistency | |
|---|---|---|
| Physical activity (IPAQ) | 0.900–0.914 | 0.51 |
| Quality of life (Cantril Ladder of Life) | 0.914 | - |
| Quality of sleep (MISS) | 0.79 | 0.73 |
| By Sex | By Age | ||||
|---|---|---|---|---|---|
| Variables | Total (n = 107) | Male | Female | <65 | ≥65 |
| Age, (years), mean (SD) | 73.18 (12.68) | 73.54 (12.91) | 72.70 (12.51) | 53.48 (8.78) * | 77.99 (7.95) * |
| Sex, n (%) | |||||
| Male | 61.00 (57.00) | 61.00 (100.00) | 0.00 (0.00) | 12.00 (57.10) | 49.00 (57.00) |
| Female | 46.00 (43.00) | 0.00 (0.00) | 46.00 (100.00) | 9.00 (42.90) | 37.00 (43.00) |
| Marital status, n (%) | |||||
| Married | 90.00 (84.10) | 52.00 (85.20) | 38.00 (82.60) | 70.00 (81.40) | 70.00 (81.40) |
| Single | 2.00 (1.90) | 2.00 (3.30) | 0.00 (0.00) | 1.00 (1.20) | 1.00 (1.20) |
| Widowed | 15.00 (14.00) | 7.00 (11.5) | 8.00 (17.40) | 15.00 (17.40) | 15.00 (17.40) |
| Working status, n (%) | |||||
| Employed | 1.00 (10.20) | 7.00 (11.40) | 4.00 (8.70) | 10.00 (47.70) | 1.00 (1.20) |
| Unemployed | 4.00 (3.70) | 2.00 (3.30) | 2.00 (4.30) | 4.00 (19.00) | 0.00 (0.00) |
| Housekeeper | 14.00 (13.10) | 5.00 (8.20) | 9.00 (19.60) | 0.00 (0.00) | 14.00 (16.30) |
| Retired | 78.00 (72.90) | 47.00 (77.00) | 31.00 (67.40) | 7.00 (33.30) | 71.00 (82.50) |
| Education, n (%) | |||||
| None | 17.00 (15.80) | 7.00 (11.40) | 10.00 (21.70) | 0.00 (0.00) | 17.00 (19.80) |
| Primary education | 39.00 (36.40) | 24.00 (39.30) | 15.00 (32.60) | 2.00 (9.50) | 37.00 (43.00) |
| Secondary education | 38.00 (35.50) | 20.00 (32.80) | 13.00 (28.30) | 14.00 (66.60) | 24.00 (27.90) |
| University | 13.00 (12.10) | 8.00 (13.10) | 5.00 (10.90) | 5.00 (23.80) | 8.00 (9.30) |
| Time since diagnosis, months, mean (SD) | 96.54 (134.81) | 82.75 (121.87) | 114.83 (149.69) | 64.38 (76.85) | 104.40 (144.76) |
| LVEF, %, mean (SD) | 43.36 (15.44) | 40.51 (15.00) * | 47.12 (15.38) * | 41.74 (13.60) | 43.75 (15.91) |
| NYHA Classification, n (%) | |||||
| I | 7.00 (6.50) | 5.00 (8.20) | 2.00 (4.30) | 1.00 (4.80) | 6.00 (7.00) |
| II | 73.00 (68.2) | 43.00 (70.50) | 30.00 (65.20) | 15.00 (71.40) | 58.00 (67.40) |
| III | 22.00 (20.6) | 10.00 (16.40) | 12.00 (26.10) | 5.00 (23.80) | 17.00 (19.80) |
| IV | 5.00 (4.70) | 3.00 (4.90) | 2.00 (4.30) | 0.00 (0.00) | 5.00 (5.80) |
| Weight, kilograms, mean (SD) | 71.78 (14.11) | 75.59 (13.80) * | 66.72 (13.02) * | 74.38 (14.64) | 71.14 (13.99) |
| BMI, mean (SD) | 26.42 (4.73) | 26.51 (4.58) | 26.30 (4.97) | 27.45 (4.42) | 26.17 (4.79) |
| During Lockdown Mean (SD) | After Lockdown Mean (SD) | T Student p Value | |
|---|---|---|---|
| Physical activity (IPAQ) | |||
| Vigorous PA, METS minute/week | 0.00 (0.00) | 26.92 (206.74) | 0.181 |
| Moderate PA, METS minute/week | 87.48 (329.90) | 129.35 (424.27) | 0.068 |
| Walking, METS minute/week | 302.61 (371.98) | 871.23 (931.94) | <0.001 * |
| Sedentary time, hours/day | 5.88 (5.41) | 5.80 (4.66) | 0.872 |
| Total score, METS minute/week | 386.85 (581.69) | 999.16 (10) | <0.001 * |
| Quality of life (Cantril Ladder of Life) | 5.61 (2.32) | 5.84 (2.31) | 0.091 |
| Quality of sleep (MISS) | |||
| Difficulties falling asleep | 1.40 (1.46) | 1.41 (1.45) | 0.897 |
| Night awakenings | 1.51 (1.29) | 1.51 (1.33) | 1.000 |
| Not being rested by sleep | 0.63 (1.04) | 0.59 (1.00) | 0.495 |
| <65 Years Old Mean (SD) | p Value | ≥65 Years Old Mean (SD) | p Value | |||
|---|---|---|---|---|---|---|
| During Lockdown | After Lockdown | During Lockdown | After Lockdown | |||
| Physical activity (IPAQ) | ||||||
| Vigorous PA, METS/min/week | 0.00 (0.00) | 91.43 (418.98) | 0.329 | 0.00 (0.00) | 11.16 (103.52) | 0.320 |
| Moderate PA, METS/min/week | 80.00 (366.61) | 80.00 (366.61) | 1.000 | 89.30 (322.62) | 141.40 (438.29) | 0.068 |
| Walking PA, METS/min/week | 196.43 (244.12) | 891.79 (899.75) | <0.001 * | 328.85 (394.03) | 866.15 (944.86) | <0.001 * |
| Sedentary time | 7.10 (5.30) | 7.38 (3.58) | 0.788 | 5.58 (5.42) | 5.42 (4.83) | 0.756 |
| Total score, METS/min/week | 276.43 (488.48) | 1063.21 (1180.22) | 0.003 * | 413.81 (601.73) | 983.52 (1069.83) | <0.001 * |
| Quality of life (Cantril Ladder of Life) | 6.33 (2.31) | 6.24 (1.90) | 0.776 | 5.43 (2.30) | 5.74 (2.40) | 0.039 * |
| Sleep quality (MISS) | ||||||
| Difficulties falling asleep | 1.33 (1.53) | 1.48 (1.66) | 0.526 | 1.42 (1.45) | 1.40 (1.40) | 0.748 |
| Night awakenings | 1.24 (1.22) | 1.38 (1.28) | 0.379 | 1.58 (1.31) | 1.55 (1.34) | 0.671 |
| Not being rested by sleep | 0.43 (0.81) | 0.43 (0.81) | 1.000 | 0.67 (1.09) | 0.63 (1.04) | 0.436 |
| Men Mean (SD) | p Value | Women Mean (SD) | p Value | |||
|---|---|---|---|---|---|---|
| During Lockdown | After Lockdown | During Lockdown | After Lockdown | |||
| Physical activity (IPAQ) | ||||||
| Vigorous PA, METS/min/week | 0.00 (0.00) | 47.21 (273.01) | 0.182 | 0.00 (0.00) | 0.00 (0.00) | 1.000 |
| Moderate PA, METS/min/week | 78.69 (324.14) | 106.23 (343.70) | 0.366 | 99.13 (340.64) | 160 (514.60) | 0.084 |
| Walking PA, METS/min/week | 347.33 (374.82) | 929.14 (880.67) | <0.001 * | 242 (393.44) | 792.73 (1002.01) | <0.001 * |
| Sedentary time | 6.72 (5.36) | 6.57 (4.34) | 0.815 | 4.76 (5.32) | 4.78 (4.92) | 0.975 |
| Total score, METS/min/week | 426.18 (527.38) | 1082.58 (1060.86) | <0.001 * | 334.70 (649.09) | 888.54 (1123.06) | <0.001 * |
| Quality of life (Cantril Ladder of Life) | 5.70 (2.25) | 5.87 (2.22) | 0.450 | 5.48 (2.43) | 5.80 (2.46) | 0.046 * |
| Sleep quality (MISS) | ||||||
| Difficulties falling asleep | 1.44 (1.50) | 1.49 (1.49) | 0.643 | 1.35 (1.41) | 1.30 (1.40) | 0.642 |
| Night awakenings | 1.57 (1.35) | 1.56 (1.37) | 0.874 | 1.43 (1.22) | 1.46 (1.28) | 0.830 |
| Not being rested by sleep | 0.61 (1.05) | 0.61 (1.05) | 0.471 | 0.59 (0.98) | 0.57 (0.94) | 0.811 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-González, J.L.; Almenar-Bonet, L.; Moreno-Segura, N.; Gurdiel-Álvarez, F.; Atef, H.; Sillero-Sillero, A.; López-Vilella, R.; Santolalla-Arnedo, I.; Juárez-Vela, R.; Tejada-Garrido, C.I.; et al. Effects of COVID-19 Lockdown on Heart Failure Patients: A Quasi-Experimental Study. J. Clin. Med. 2023, 12, 7090. https://doi.org/10.3390/jcm12227090
Sánchez-González JL, Almenar-Bonet L, Moreno-Segura N, Gurdiel-Álvarez F, Atef H, Sillero-Sillero A, López-Vilella R, Santolalla-Arnedo I, Juárez-Vela R, Tejada-Garrido CI, et al. Effects of COVID-19 Lockdown on Heart Failure Patients: A Quasi-Experimental Study. Journal of Clinical Medicine. 2023; 12(22):7090. https://doi.org/10.3390/jcm12227090
Chicago/Turabian StyleSánchez-González, Juan Luis, Luis Almenar-Bonet, Noemí Moreno-Segura, Francisco Gurdiel-Álvarez, Hady Atef, Amalia Sillero-Sillero, Raquel López-Vilella, Iván Santolalla-Arnedo, Raúl Juárez-Vela, Clara Isabel Tejada-Garrido, and et al. 2023. "Effects of COVID-19 Lockdown on Heart Failure Patients: A Quasi-Experimental Study" Journal of Clinical Medicine 12, no. 22: 7090. https://doi.org/10.3390/jcm12227090