
Effect of Total Hip Arthroplasty with Ceramic Acetabular Component on Clinical, Radiographic and Functional Parameters in Older Patients with Hip Osteoarthritis: Two-Year Follow-Up


Abstract
:1. Introduction
2. Materials and Methods
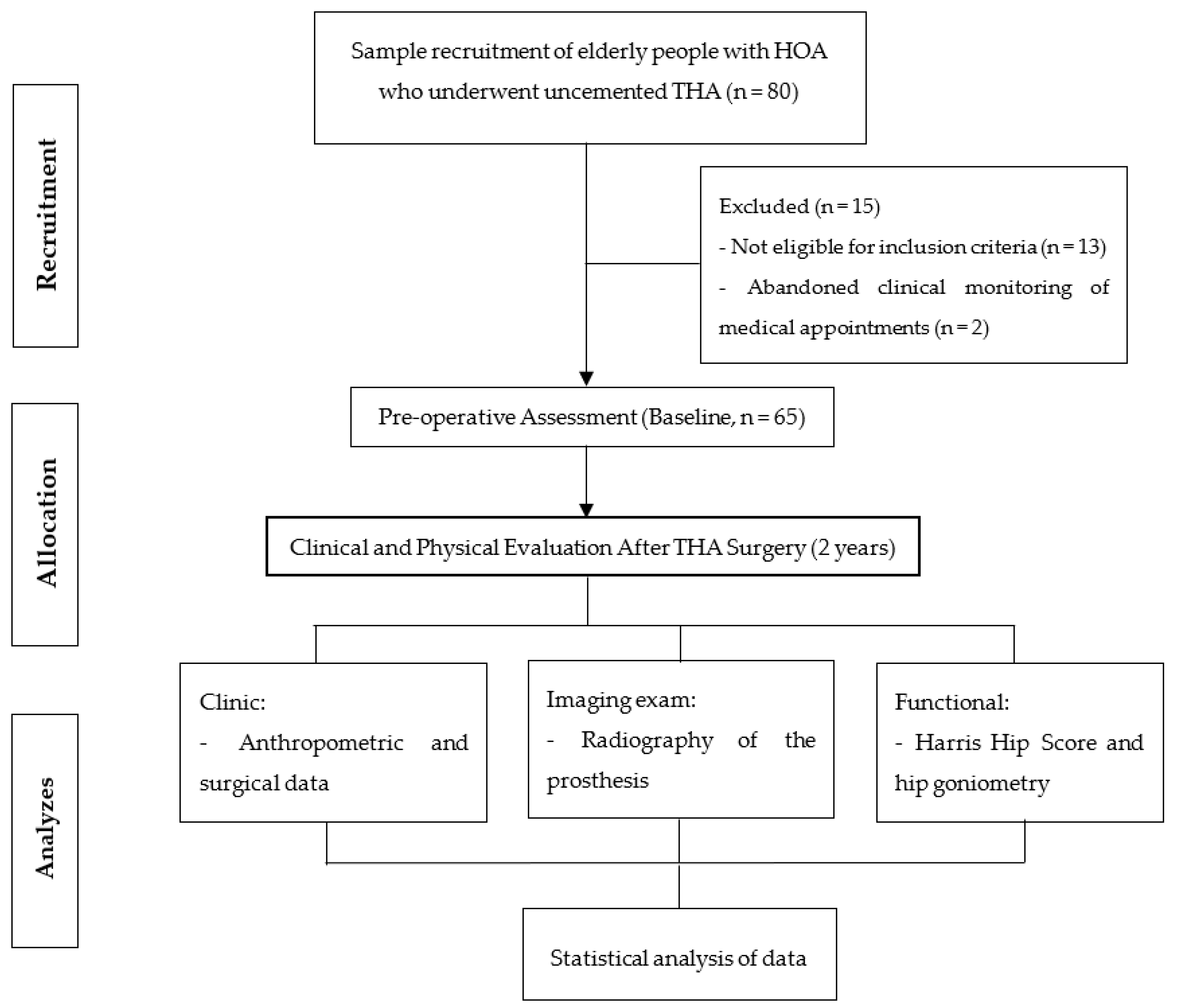
2.1. Study Design and Participants
2.2. Analysis of Medical Records
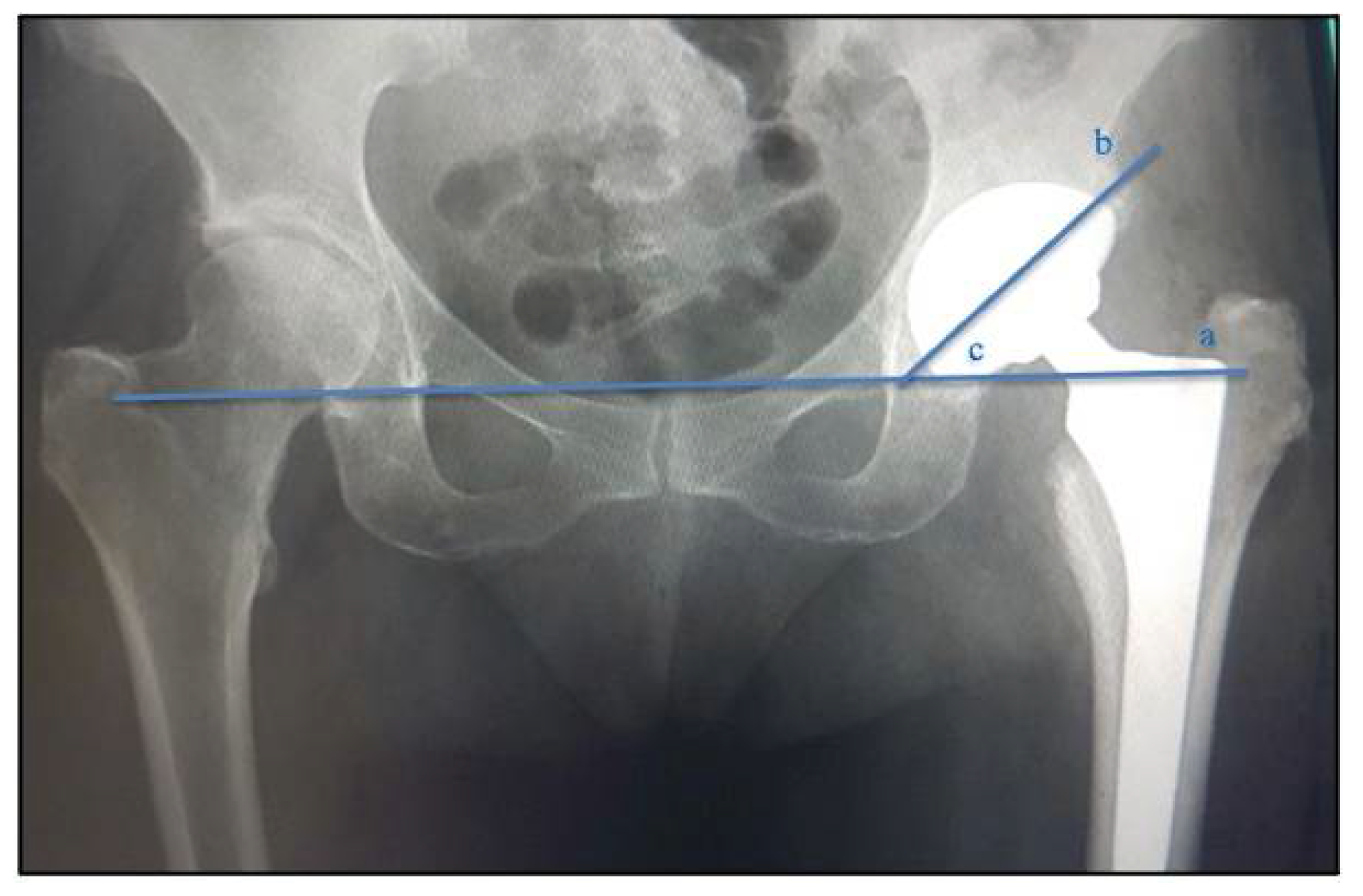
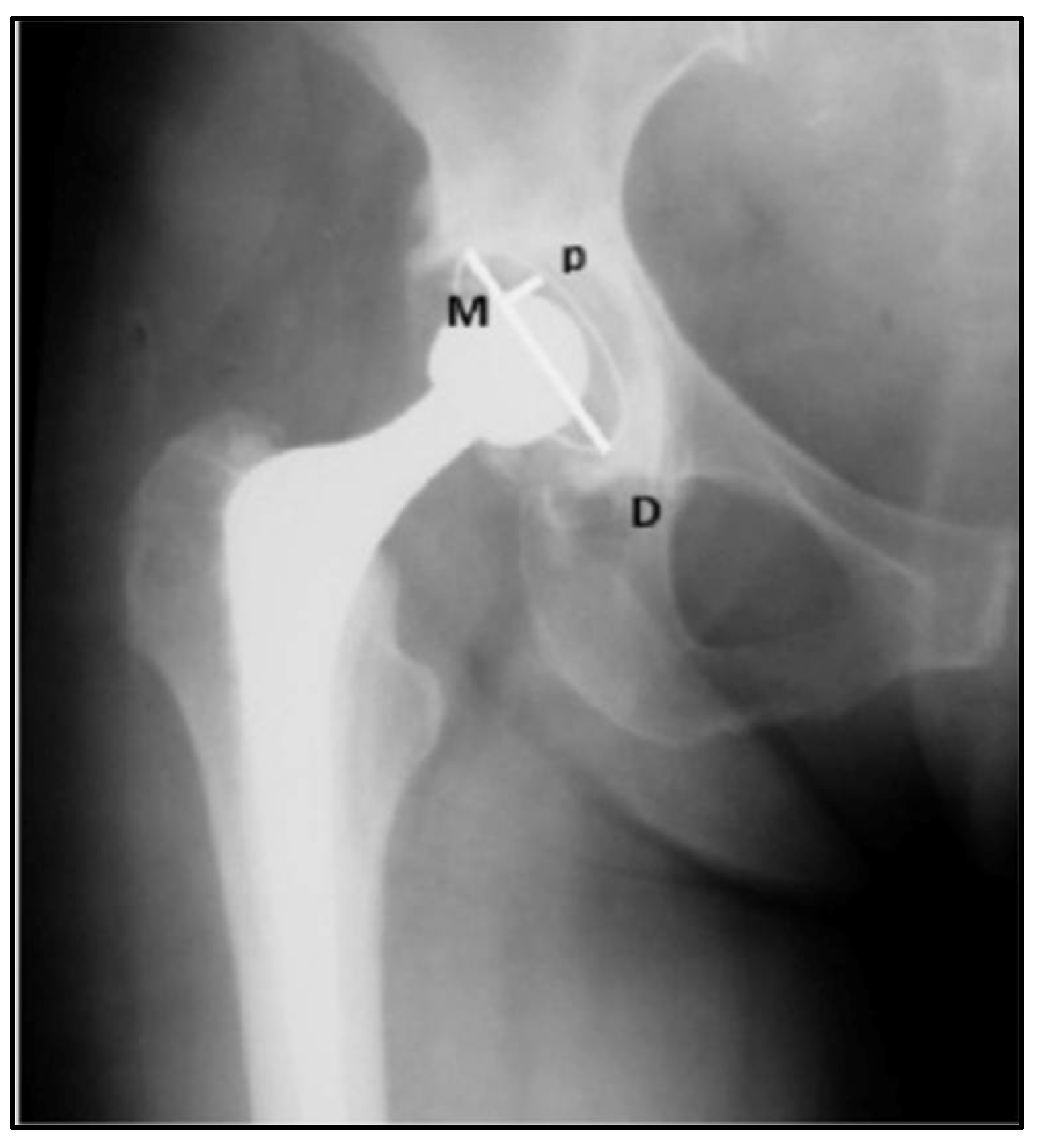
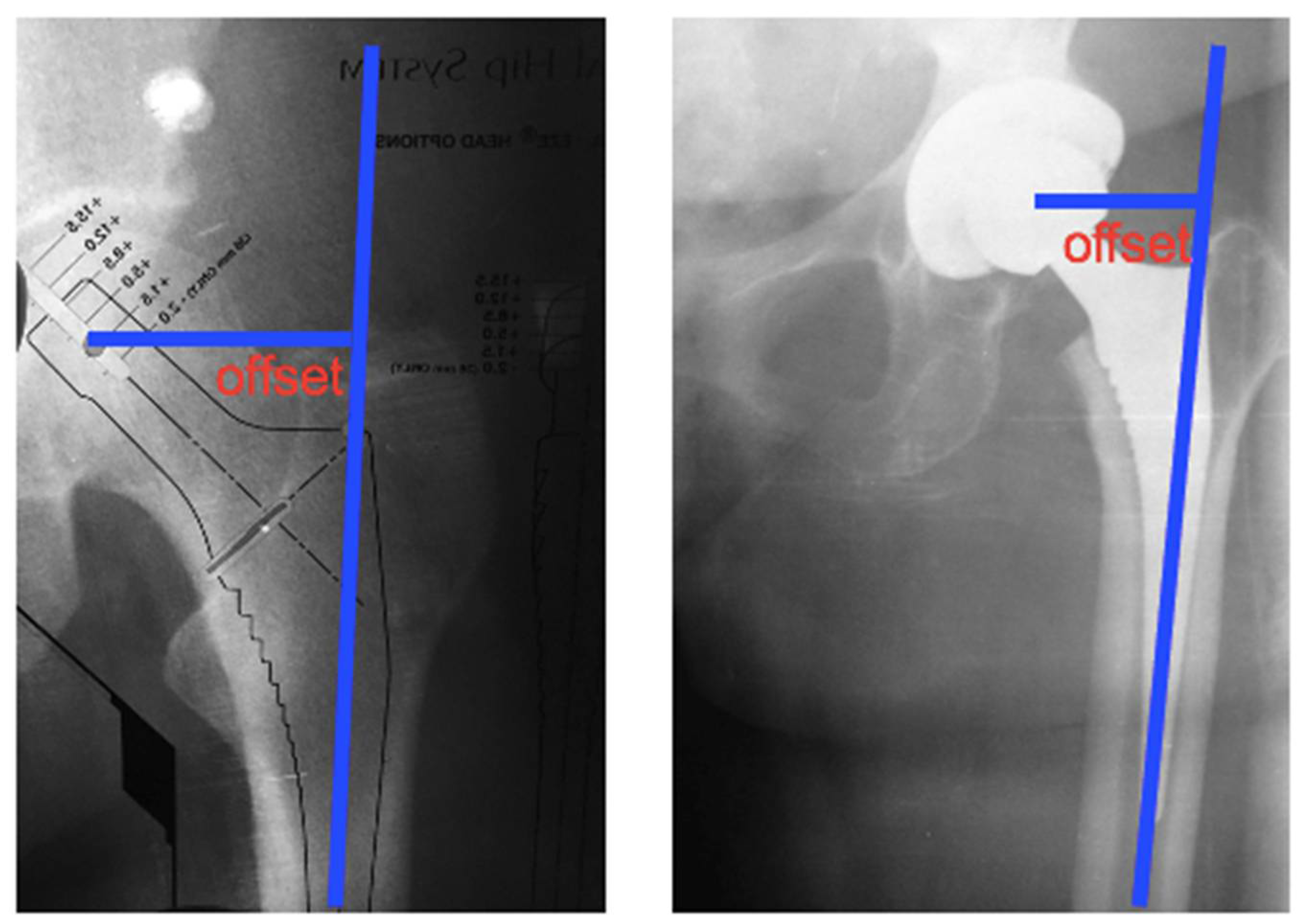
2.3. Analysis of Radiographic Parameters: Positioning and Inclinations of the Acetabular Component
2.4. Functional Parameters of the Hip
2.5. Hip Range of Motion Parameters
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.; Blanco, F.; Englund, M.; Karsdal, M.; Lohmander, L. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthr. Cartil. 2015, 23, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prieto-Alhambra, D.; Judge, A.; Javaid, M.K.; Cooper, C.; Diez-Perez, A.; Arden, N.K. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann. Rheum. Dis. 2013, 73, 1659–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.A. Epidemiology of Knee and Hip Arthroplasty: A Systematic Review§. Open Orthop. J. 2011, 5, 80–85. [Google Scholar] [CrossRef] [Green Version]
- Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Shan, L.; Shan, B.; Graham, D.; Saxena, A. Total hip replacement: A systematic review and meta-analysis on mid-term quality of life. Osteoarthr. Cartil. 2014, 22, 389–406. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Peat, G.; Bedson, J.; Jordan, K. Annual consultation incidence of osteoarthritis estimated from population-based health care data in England. Rheumatology 2015, 54, 2051–2060. [Google Scholar] [CrossRef] [Green Version]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar]
- Hunter, D.J.; Schofield, D.; Callander, E. The individual and socioeconomic impact of osteoarthritis. Nat. Rev. Rheumatol. 2014, 10, 437–441. [Google Scholar] [CrossRef]
- Gupta, S.; Hawker, G.A.; Laporte, A.; Croxford, R.; Coyte, P.C. The economic burden of disabling hip and knee osteoarthritis (OA) from the perspective of individuals living with this condition. Rheumatology 2005, 44, 1531–1537. [Google Scholar] [CrossRef] [Green Version]
- Najarian, B.C.; Kilgore, J.E.; Markel, D.C. Evaluation of Component Positioning in Primary Total Hip Arthroplasty Using an Imageless Navigation Device Compared With Traditional Methods. J. Arthroplast. 2009, 24, 15–21. [Google Scholar] [CrossRef]
- Reininga, I.H.; Zijlstra, W.; Wagenmakers, R.; Boerboom, A.L.; Huijbers, B.P.; Groothoff, J.W.; Bulstra, S.K.; Stevens, M. Minimally invasive and computer-navigated total hip arthroplasty: A qualitative and systematic review of the literature. BMC Musculoskelet. Disord. 2010, 11, 92–104. [Google Scholar] [CrossRef] [Green Version]
- Lenza, M.; Ferraz, S.D.B.; Viola, D.C.M.; Filho, R.J.G.; Neto, M.C.; Ferretti, M. Epidemiology of total hip and knee replacement: A cross-sectional study. Einstein 2013, 11, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schofield, D.; Cunich, M.; Shrestha, R.N.; Tanton, R.; Veerman, L.; Kelly, S.; Passey, M.E. The long-term economic impacts of arthritis through lost productive life years: Results from an Australian microsimulation model. BMC Public Health 2018, 18, 654. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.B.; Ecker, T.M.; Tannast, M. THA Performed using Conventional and Navigated Tissue-preserving Techniques. Clin. Orthop. Relat. Res. 2006, 453, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, K.-H.; Grützner, P.A. Joint replacement—Total hip replacement with CT-based navigation. Injury 2004, 35, 84–89. [Google Scholar] [CrossRef]
- Culliford, D.J.; Maskell, J.; Kiran, A.; Judge, A.; Javaid, M.K.; Cooper, C.; Arden, N.K. The lifetime risk of total hip and knee arthroplasty: Results from the UK general practice research database. Osteoarthr. Cartil. 2012, 20, 519–524. [Google Scholar] [CrossRef] [Green Version]
- Padgett, D.E.; Hendrix, S.L.; Mologne, T.S.; Peterson, D.A.; Holley, K.A. Effectiveness of an Acetabular Positioning Device in Primary Total Hip Arthroplasty. HSS J. 2005, 1, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Kiefer, H. Orthopilot cup navigation—How to optimize cup positioning? Int. Orthop. 2003, 27 (Suppl. 1), S37–S42. [Google Scholar]
- Jolles, B.M.; Genoud, P.; Hoffmeyer, P. Computer-assisted cup placement techniques in total hip arthroplasty improve ac-curacy of placement. Clin. Orthop. Relat. Res. 2004, 426, 174–179. [Google Scholar] [CrossRef]
- Ishikura, H.; Nakamura, M.; Nakamura, S.; Tanaka, T.; Kawano, H.; Tanaka, S. Relationship between the Accuracy of the Acetabular Cup Angle and BMI in Posterolateral Total Hip Arthroplasty with CT-Based Navigation. Medicina 2022, 58, 856. [Google Scholar] [CrossRef] [PubMed]
- Kanesaki, K.; Hieda, H.; Nagata, K. Current status of navigated cup replacement in dysplastic cases. Orthopedics 2006, 29, S113–S116. [Google Scholar]
- Dorr, L.D.; Malik, A.; Wan, Z.; Long, W.T.; Harris, M. Precision and Bias of Imageless Computer Navigation and Surgeon Estimates for Acetabular Component Position. Clin. Orthop. Relat. Res. 2007, 465, 92–99. [Google Scholar] [CrossRef]
- Ybinger, T.; Kumpan, W.; Hoffart, H.; Muschalik, B.; Bullmann, W.; Zweymüller, K. Accuracy of Navigation-Assisted Acetabular Component Positioning Studied by Computed Tomography Measurements: Methods and Results. J. Arthroplast. 2007, 22, 812–817. [Google Scholar] [CrossRef]
- Mainard, D. Navigated and nonnavigated total hip arthroplasty: Results of two consecutive series using a cementless straight hip stem. Orthopedics 2008, 31, 321–322. [Google Scholar]
- Gandhi, R.; Marchie, A.; Farrokhyar, F.; Mahomed, N. Computer navigation in total hip replacement: A meta-analysis. Int. Orthop. 2009, 33, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Jerosch, J.; Weipert, A.; Hanusek, S.; Schneppenheim, M. Movement Mapping as dynamic preoperative surgical planning in total hip replacement. Arch. Orthop. Trauma Surg. 2002, 122, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Nogler, M.; Kessler, O.; Prassl, A.; Donnelly, B.; Streicher, R.; Sledge, J.B.; Krismer, M. Reduced variability of acetabular cup po-sitioning with use of an imageless navigation system. Clin. Orthop. Relat. Res. 2004, 426, 159–163. [Google Scholar] [CrossRef]
- Lazovic, D.; Kaib, N.; T, F.; S, F.; S, N.; N, S.; S, Y.; F, I. Results with Navigated Bicontact Total Hip Arthroplasty. Orthopedics 2005, 28, S1227–S1233. [Google Scholar] [CrossRef] [PubMed]
- Sotereanos, N.G.; Miller, M.C.; Smith, B.; Hube, R.; Sewecke, J.J.; Wohlrab, D. Using Intraoperative Pelvic Landmarks for Acetabular Component Placement in Total Hip Arthroplasty. J. Arthroplast. 2006, 21, 832–840. [Google Scholar] [CrossRef]
- Babisch, J.W.; Layher, F.; Amiot, L.-P. The Rationale for Tilt-Adjusted Acetabular Cup Navigation. J. Bone Joint Surg. Am. 2008, 90, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Murtha, P.E.; Hafez, M.A.; Jaramaz, B.; DiGioia, A.M., III. Variations in acetabular anatomy with reference to total hip replace-ment. J. Bone Joint Surg. Br. 2008, 90, 308–315. [Google Scholar] [CrossRef]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The Epidemiology of Revision Total Hip Arthroplasty in the United States. J. Bone Joint Surg. Am. 2009, 91, 128–133. [Google Scholar] [CrossRef]
- Leenders, T.; Vandevelde, D.; Mahieu, G.; Nuyts, R. Reduction in variability of acetabular cup abduction using computer as-sisted surgery: A prospective and randomized study. Comput. Aided. Surg. 2002, 7, 99–106. [Google Scholar] [CrossRef]
- Kalteis, T.; Handel, M.; Bäthis, H.; Perlick, L.; Tingart, M.; Grifka, J. Imageless navigation for insertion of the acetabular com-ponent in total hip arthroplasty: Is it as accurate as CT- based navigation? J. Bone J. Surg. Br. 2006, 88, 163–167. [Google Scholar] [CrossRef]
- Wentzensen, A.; Zheng, G.; Vock, B.; Langlotz, U.; Korber, J.; Nolte, L.P.; Grützner, P.A. Image-based hip navigation. Int. Orthop. 2003, 27, S43–S46. [Google Scholar] [PubMed]
- Grützner, P.A.; Zheng, G.; Langlotz, U.; Von Recum, J.; Nolte, L.P.; Wentzensen, A.; Widmer, K.-H.; Wendl, K. C-arm based navigation in total hip arthroplasty—Background and clinical experience. Injury 2004, 35, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Ecker, T.M.; Tannast, M.; Murphy, S.B. Computed Tomography-based Surgical Navigation for Hip Arthroplasty. Clin. Orthop. Relat. Res. 2007, 465, 100–105. [Google Scholar] [CrossRef]
- Haaker, R.G.; Tiedjen, K.; Ottersbach, A.; Rubenthaler, F.; Stockheim, M.; Stiehl, J.B. Comparison of Conventional Versus Computer-Navigated Acetabular Component Insertion. J. Arthroplast. 2007, 22, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Munigangaiah, S.; O’Dwyer, S.; Masterson, E. Uncemented total hip arthroplasty in osteoarthritis of hip secondary to low and high dislocated hips: A mid-term follow-up study. J. Nat. Sci. Biol. Med. 2016, 7, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Ejnisman, L.; Leonhardt, N.Z.; Fernandes, L.F.L.; Leonhardt, M.; Vicente, J.R.N.; Croci, A.T. Comparison of total hip arthroplasty in osteoarthritis of mechanical and rheumatologic causes. Acta Ortop. Bras. 2014, 22, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Loehr, J.F.; Munzinger, U.; Tibesku, C. Uncemented Total Hip Arthroplasty in Patients With Rheumatoid Arthritis. Clin. Orthop. Relat. Res. 1999, 366, 31–38. [Google Scholar] [CrossRef]
- Delee, J.G.; Charnley, J. Radiological Demarcation of Cemented Sockets in Total Hip Replacement. Clin. Orthop. Relat. Res. 1976, 121, 20–32. [Google Scholar] [CrossRef]
- Nilsdotter, A.; Bremander, A. Measures of hip function and symptoms: Harris Hip Score (HHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), Oxford Hip Score (OHS), Lequesne Index of Severity for Osteoarthritis of the Hip (LISOH), and American Academy of Orthopedic Surgeons (AAOS) Hip and Knee Questionnaire. Arthritis Care Res. (Hoboken) 2011, 63 (Suppl. 11), S200–S207. [Google Scholar]
- Guimarães, R.P.; Alves, D.P.L.; Silva, G.B.; Bittar, S.T.; Ono, N.K.; Honda, E.; Polesello, G.C.; Junior, W.R.; de Carvalho, N.A.A. Translation and cultural adaptation of the Harris Hip Score into Portuguese. Acta Ortop. Bras. 2010, 18, 142–147. [Google Scholar] [CrossRef]
- Huang, J.; Tian, F.; Zhang, Z.; Shi, W.; Lin, J.; Chen, L.; Yang, H. Reliability and concurrent validity of angle measurements in lower limb: EOS 3D goniometer versus 2D manual goniometer. J. Orthop. Transl. 2020, 24, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.S.; McLaughlin, R.J.; Berry, D.J.; Lewallen, D.G.; Trousdale, R.T.; Sierra, R.J. What Is the Survivorship of Revision Surgery Performed for the Chronically Dislocated THA? Clin. Orthop. Relat. Res. 2019, 477, 374–379. [Google Scholar] [CrossRef]
- Jordan, J.; Helmick, C.; Renner, J.; Luta, G. Prevalence of hip symptoms and radiographic symptomatic hip osteoarthritis in African-Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagenais, S.; Garbedian, S.; Wai, E.K. Systematic Review of the Prevalence of Radiographic Primary Hip Osteoarthritis. Clin. Orthop. Relat. Res. 2009, 467, 623–637. [Google Scholar] [CrossRef] [Green Version]
- Felson, D. Preventing knee and hip osteoarthritis. Bull. Rheum. Dis. 1998, 47, 1–4. [Google Scholar]
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Daigle, M.E.; Weinstein, A.M.; Katz, J.N.; Losina, E. The cost-effectiveness of total joint arthroplasty: A systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 2012, 26, 649–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrizzi, L.J.; Vilaça, K.H.C.; Takata, E.T.; Trigueiro, G. Pre- and Post-Surgery analysis of functional capacity and quality of life of patienst with Osteoarthritis submitted to Total Hip Artroplasty. Rev. Bras. Reumatol. 2004, 44, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Teloken, M.A.; Bissett, G.; Hozack, W.J.; Sharkey, P.F.; Rothman, R.H. Ten to fifteen-year follow-up after total hip arthroplasty with a tapered cobalt-chromium femoral component (tri-lock) inserted without cement. J. Bone Joint Surg. Am. 2002, 84, 2140–2144. [Google Scholar] [CrossRef]
- Scheidt, R.B.; Rosito, R.; Macedo, C.A.D.S.; Galia, C.R. Artroplastia total de quadril com prótese Biomec: 20 anos de seguimento. Rev. Bras. Ortop. 2010, 45, 155–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xará-Leite, F.; Pereira, A.D.; Andrade, R.; Sarmento, A.; Sousa, R.; Ayeni, O.R.; Espregueira-Mendes, J.; Soares, D. The ce-ment-in-cement technique is a reliable option in hip arthroplasty revision surgery: A systematic review. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 7–22. [Google Scholar] [CrossRef]
- Corten, K.; Bourne, R.B.; Charron, K.D.; Au, K.; Rorabeck, C.H. Comparison of Total Hip Arthroplasty Performed with and without Cement: A Randomized Trial. J. Bone Joint Surg. Am. 2011, 93, 1335–1338. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | GPO (n = 65) | THA (n = 65) | p |
|---|---|---|---|
| Age (years) | 60.3 ± 14.8 | 62.8 ± 15.0 | 0.010 * |
| Mass (Kg/cm2) | 75.5 ± 10.6 | 74.5 ± 9.6 | 0.063 |
| Stature (cm) | 1.64 ± 0.5 | 1.65 ± 0.6 | 0.164 |
| BMI (Kg/cm2) | 27.8 ± 4.2 | 28.1 ± 3.9 | 0.383 |
| Sex (%) | F (46.2); M (53.8) | F (46.2); M (53.8) | - |
| Radiographic Examination | GPO (n = 65) | THA (n = 65) | p |
|---|---|---|---|
| Acetabular placement (degrees) | 44.3 ± 5.9 | 44.4 ± 6.3 | 0.083 |
| Implant Femoral Offset (cm) | 4.5 ± 0.7 | 4.5 ± 0.6 | 0.102 |
| HHS Domains | GPO (n = 65) | THA (n = 65) | p |
|---|---|---|---|
| Pain | 41.3 ± 3.5 | 20.7 ± 8.5 | 0.001 * |
| Function | 9.5 ± 2.1 | 12.7 ± 1.6 | 0.012 * |
| Gait | 22.5 ± 5.8 | 31.1 ± 4.9 | 0.001 * |
| Deformity | 3.4 ± 1.2 | 4.0 ± 1.0 | 0.013 * |
| Total score | 56.3 ± 14.6 | 85.8 ± 9.6 | <0.001 * |
| Post Implant Complications | Number (n = 65) | Percentage (0–100%) |
|---|---|---|
| Inappropriate positioning | 1 | 1.5% |
| Dislocation (recurrent dislocation) | 2 | 3.0% |
| Loosening | 1 | 1.5% |
| Joint infection in two hips (deep periprosthetic) | 0 | 0% |
| Total | 4 | 6.0% |
| Hip Goniometry | GPO (n = 65) | THA (n = 65) | p |
|---|---|---|---|
| Flexion | 36.6 ± 6.1 | 54.4 ± 11.2 | 0.001 * |
| Extension | 5.4 ± 1.8 | 7.7 ± 1.3 | 0.001 * |
| Abduction | 15.7 ± 3.1 | 25.9 ± 7.6 | <0.001 * |
| Adduction | 6.3 ± 2.4 | 11.1 ± 1.9 | <0.001 * |
| External rotation | 13.3 ± 3.7 | 25.6 ± 5.3 | 0.001 * |
| Internal rotation | 11.0 ± 1.6 | 22.1 ± 5.4 | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torini, A.P.; Barsotti, C.E.; Andrade, R.M.; Nali, L.H.d.S.; Ribeiro, A.P. Effect of Total Hip Arthroplasty with Ceramic Acetabular Component on Clinical, Radiographic and Functional Parameters in Older Patients with Hip Osteoarthritis: Two-Year Follow-Up. J. Clin. Med. 2023, 12, 670. https://doi.org/10.3390/jcm12020670
Torini AP, Barsotti CE, Andrade RM, Nali LHdS, Ribeiro AP. Effect of Total Hip Arthroplasty with Ceramic Acetabular Component on Clinical, Radiographic and Functional Parameters in Older Patients with Hip Osteoarthritis: Two-Year Follow-Up. Journal of Clinical Medicine. 2023; 12(2):670. https://doi.org/10.3390/jcm12020670
Chicago/Turabian StyleTorini, Alexandre Penna, Carlos Eduardo Barsotti, Rodrigo Mantelatto Andrade, Luiz Henrique da Silva Nali, and Ana Paula Ribeiro. 2023. "Effect of Total Hip Arthroplasty with Ceramic Acetabular Component on Clinical, Radiographic and Functional Parameters in Older Patients with Hip Osteoarthritis: Two-Year Follow-Up" Journal of Clinical Medicine 12, no. 2: 670. https://doi.org/10.3390/jcm12020670