
Metal-on-Metal Hips: Ten-Year Clinical and Radiographic Outcomes of the ADEPT Metal-on-Metal Hip Resurfacing and Modular Total Hip Arthroplasty
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Steffen, R.T.; Pandit, H.P.; Palan, J.; Beard, D.J.; Gundle, R.; McLardy-Smith, P.; Murray, D.W.; Gill, H.S. The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J. Bone Jt. Surg. Br. 2008, 90, 436–441. [Google Scholar] [CrossRef]
- McMinn, D.; Daniel, J. History and modern concepts in surface replacement. Proc. Inst. Mech. Eng. H 2006, 220, 239–251. [Google Scholar] [CrossRef]
- McMinn, D. (Ed.) Modern Hip Resurfacing; Springer: London, UK, 2009; pp. 189–301. [Google Scholar]
- Kohan, L.; Field, C.J.; Kerr, D.R. Early complications of hip resurfacing. J. Arthroplast. 2012, 27, 997–1002. [Google Scholar] [CrossRef]
- Girard, J. Hip Resurfacing: International Perspectives: Review Article. HSS J. 2017, 13, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Gani, M.H.; Zahoor, U.; Hanna, S.A.; Scott, G. Metal-on-metal hip resurfacing arthroplasty provides excellent long-term survivorship and function in patients with a good-sized femoral head: Results of a single, non-designer surgeon’s cohort. Bone Jt. Open 2022, 3, 68–76. [Google Scholar] [CrossRef]
- National Joint Registry (NJR). 18th Annual Report 2021: National Joint Registry for England, Wales, Northern Ireland and Isle of Man. NJR Editorial Board. NJR 18th Annual Report 2021.pdf. 2021. Available online: https://reports.njrcentre.org.uk/2020 (accessed on 30 August 2022).
- AOANJRR. 2021 Annual Report: Hip & Knee Arthroplasty Adelaide, AOA. 2021. Available online: https://aoanjrr.sahmri.com/annual-reports-2021 (accessed on 30 August 2022).
- Van Der Straeten, C.; The International Hip Resurfacing Group. Hip resurfacing arthroplasty in young patients: International high-volume centres’ report on the outcome of 11,382 metal-on-metal hip resurfacing arthroplasties in patients ≤50 years at surgery. Hip Int. 2022, 32, 353–362. [Google Scholar] [CrossRef]
- Back, D.L.; E Dalziel, R.; Young, D.; Shimmin, A.J. Early results of primary Birmingham hip resurfacings. An independent prospective study of the first 230 hips. J. Bone Jt. Surg. Br. 2005, 87, 324–329. [Google Scholar] [CrossRef] [Green Version]
- Cossey, A.J.; Back, D.L.; Shimmin, A.; Young, D.; Spriggins, A.J. The nonoperative management of periprosthetic fractures associated with the Birmingham hip resurfacing procedure. J. Arthroplast. 2005, 20, 358–361. [Google Scholar] [CrossRef]
- Steffen, R.T.; Smith, S.R.; Urban, J.P.G.; McLardy-Smith, P.; Beard, D.J.; Gill, H.S.; Murray, D.W. The effect of hip resurfacing on oxygen concentration in the femoral head. J. Bone Jt. Surg. Br. 2005, 87, 1468–1474. [Google Scholar] [CrossRef] [Green Version]
- Salmons, H.I.; Fruth, K.M.; Lewallen, D.G.; Trousdale, R.T.; Berry, D.J.; Abdel, M.P. Revision Total Hip Arthroplasty for Aseptically Failed Metal-On-Metal Hip Resurfacing Arthroplasty. J. Arthroplast. 2022. published online ahead of print. [Google Scholar] [CrossRef]
- AOANJRR. 2010 Annual Report: Hip & Knee Arthroplasty Adelaide, AOA. 2010. Available online: https://aoanjrr.sahmri.com/annual-reports-2010 (accessed on 30 August 2022).
- NJR. 11th Annual Report 2014: National Joint Registry for England, Wales, Northern Ireland and Isle of Man [Internet]. NJR Editorial Board; 2014. NJR 11th Annual Report 2014.pdf. Available online: https://reports.njrcentre.org.uk/2013 (accessed on 30 August 2022).
- Morlock, M.M.; Dickinson, E.C.; Günther, K.-P.; Bünte, D.; Polster, V. Head Taper Corrosion Causing Head Bottoming Out and Consecutive Gross Stem Taper Failure in Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 3581–3590. [Google Scholar] [CrossRef] [Green Version]
- Borgwardt, A.; Borgwardt, L.; Borgwardt, L.; Zerahn, B.; Fabricius, S.D.; Ribel-Madsen, S. Clinical Performance of the ASR and ReCap Resurfacing Implants—7 Years Follow-Up. J. Arthroplast. 2015, 30, 993–997. [Google Scholar] [CrossRef]
- Konan, S.; Waugh, C.; Ohly, N.; Duncan, C.P.; A Masri, B.; Garbuz, D.S. Mid-term results of a prospective randomised controlled trial comparing large-head metal-on-metal hip replacement to hip resurfacing using patient-reported outcome measures and objective functional task-based outcomes. Hip Int. 2021, 31, 637–643. [Google Scholar] [CrossRef]
- Plant, J.G.A.; Prosser, G.H.; Burston, B.J.; Edmondston, S.J.; Yates, P.J. Mid-Term Review of ADEPT Metal-On-Metal Hip Prosthesis. Functional, Radiological and Metal Ion Analysis. Open J. Orthop. 2014, 4, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Murray, D.W.; Fitzpatrick, R.; Rogers, K.; Pandit, H.; Beard, D.J.; Carr, A.J.; Dawson, J. The use of the Oxford hip and knee scores. J. Bone Jt. Surg. Br. 2007, 89, 1010–1014. [Google Scholar] [CrossRef] [Green Version]
- Amstutz, H.C.; Thomas, B.J.; Jinnah, R.; Kim, W.; Grogan, T.; Yale, C. Treatment of primary osteoarthritis of the hip. A comparison of total joint and surface replacement arthroplasty. J. Bone Jt. Surg. Am. 1984, 66, 228–241. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Engh, C.A.; Bobyn, J.D.; Glassman, A.H. Porous-coated hip replacement. The factors governing bone ingrowth, stress shielding, and clinical results. J. Bone Jt. Surg. Br. 1987, 69, 45–55. [Google Scholar] [CrossRef]
- Gruen, T.A.; McNeice, G.M.; Amstutz, H.C. Modes of failure” of cemented stem-type femoral components: A radiographic analysis of loosening. Clin. Orthop. Relat. Res. 1979, 141, 17–27. [Google Scholar] [CrossRef]
- Johnston, R.C.; Fitzgerald, R.H.; Harris, W.H.; Poss, R.; E Müller, M.; Sledge, C.B. Clinical and radiographic evaluation of total hip replacement. A standard system of terminology for reporting results. J. Bone Jt. Surg. Am. 1990, 72, 161–168, Erratum in J. Bone Jt. Surg. Am. 1991, 73, 952. [Google Scholar] [CrossRef]
- DeLee, J.G.; Charnley, J. Radiological demarcation of cemented sockets in total hip replacement. Clin. Orthop. Relat. Res. 1976, 121, 20–32. [Google Scholar] [CrossRef]
- Brooker, A.F.; Bowerman, J.W.; Robinson, R.A.; Riley, L.H., Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J. Bone Jt. Surg. Am. 1973, 55, 1629–1632. [Google Scholar] [CrossRef]
- MacDonald, S.J.; Brodner, W.; Jacobs, J.J. A consensus paper on metal ions in metal-on-metal hip arthroplasties. J. Arthroplast. 2004, 19 (Suppl. 3), 12–16. [Google Scholar] [CrossRef]
- MHRA. All Metal-on-Metal (MoM) Hip Replacements: Updated Advice for Follow-Up of Patients. [Internet]. All Types of Metal-on-Metal Hip Implants Need Regular Review-GOV.UK. Available online: www.gov.uk (accessed on 30 August 2022).
- Bosker, B.H.; Ettema, H.B.; Boomsma, M.F.; Kollen, B.J.; Maas, M.C.; Verheyen, C.C.P.M. High incidence of pseudotumour formation after large-diameter metal-on-metal total hip replacement: A prospective cohort study. J. Bone Jt. Surg. Br. 2012, 94, 755–761. [Google Scholar] [CrossRef]
- Illgen, R.L.; Heiner, J.P.; Squire, M.W.; Conrad, D.N. Large-head metal-on-metal total hip arthroplasty using the Durom acetabular component at minimum 1-year interval. J. Arthroplast. 2010, 25 (Suppl. 6), 26–30. [Google Scholar] [CrossRef]
- Long, W.T.; Dastane, M.; Harris, M.J.; Wan, Z.; Dorr, L.D. Failure of the Durom Metasul acetabular component. Clin. Orthop. Relat. Res. 2010, 468, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Berton, C.; Girard, J.; Krantz, N.; Migaud, H. The Durom large diameter head acetabular component: Early results with a large-diameter metal-on-metal bearing. J. Bone Jt. Surg. Br. 2010, 92, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Bernthal, N.M.; Celestre, P.C.; Stavrakis, A.I.; Ludington, J.C.; Oakes, D.A. Disappointing short-term results with the DePuy ASR XL metal-on-metal total hip arthroplasty. J. Arthroplast. 2012, 27, 539–544. [Google Scholar] [CrossRef]
- Steele, G.D.; Fehring, T.K.; Odum, S.M.; Dennos, A.C.; Nadaud, M.C. Early failure of articular surface replacement XL total hip arthroplasty. J. Arthroplast. 2011, 26 (Suppl. 6), 14–18. [Google Scholar] [CrossRef] [PubMed]
- Stoney, J.M.; Graves, S.E.M.; de Steiger, R.N.M.; Rainbird, S.B.; Kelly, T.-L.; Hatton, A.B.M. Is the Survivorship of Birmingham Hip Resurfacing Better Than Selected Conventional Hip Arthroplasties in Men Younger Than 65 Years of Age? A Study from the Australian Orthopaedic Association National Joint Replacement Registry. Clin. Orthop. Relat. Res. 2020, 478, 2625–2636. [Google Scholar] [CrossRef]
- Malahias, M.-A.; Mancino, F.; Gu, A.; Adriani, M.; De Martino, I.; Boettner, F.; Sculco, P.K. Acetabular impaction grafting with mesh for acetabular bone defects: A systematic review. Hip Int. 2022, 32, 185–196. [Google Scholar] [CrossRef]
- Lombardi, A.V., Jr.; Skeels, M.D.; Berend, K.R.; Adams, J.B.; Franchi, O.J. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin. Orthop. Relat. Res. 2011, 469, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Stroh, D.A.; Issa, K.; Johnson, A.J.; Delanois, R.E.; Mont, M.A. Reduced dislocation rates and excellent functional outcomes with large-diameter femoral heads. J. Arthroplast. 2013, 28, 1415–1420. [Google Scholar] [CrossRef]
- Vendittoli, P.-A.; Ganapathi, M.; Roy, A.G.; Lusignan, D.; Lavigne, M. A comparison of clinical results of hip resurfacing arthroplasty and 28 mm metal on metal total hip arthroplasty: A randomised trial with 3–6 years follow-up. Hip Int. 2010, 20, 1–13. [Google Scholar] [CrossRef]
- Pollard, T.C.B.; Baker, R.P.; Eastaugh-Waring, S.J.; Bannister, G.C. Treatment of the young active patient with osteoarthritis of the hip. A five- to seven-year comparison of hybrid total hip arthroplasty and metal-on-metal resurfacing. J. Bone Jt. Surg. Br. 2006, 88, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Mancino, F.; Jones, C.W.; Sculco, T.P.; Sculco, P.K.; Maccauro, G.; De Martino, I. Survivorship and Clinical Outcomes of Constrained Acetabular Liners in Primary and Revision Total Hip Arthroplasty: A Systematic Review. J. Arthroplast. 2021, 36, 3028–3041. [Google Scholar] [CrossRef]
- Ridon, P.-E.; Putman, S.; Migaud, H.; Berton, C.; Pasquier, G.; Girard, J. Long-term comparative study of large-diameter metal-on-metal bearings: Resurfacing versus total arthroplasty with large-diameter Durom™ bearing. Orthop. Traumatol. Surg. Res. 2019, 105, 943–948. [Google Scholar] [CrossRef]
- Hothi, H.S.; Berber, R.; Whittaker, R.K.; Blunn, G.W.; Skinner, J.A.; Hart, A.J. The Relationship Between Cobalt/Chromium Ratios and the High Prevalence of Head-Stem Junction Corrosion in Metal-on-Metal Total Hip Arthroplasty. J. Arthroplast. 2016, 31, 1123–1127. [Google Scholar] [CrossRef] [Green Version]
- Kearns, S.J.W.; Bourget-Murray, J.; Johnston, K.; Werle, J. Comparing 1-year and 10-year whole blood metal ion results following Birmingham hip resurfacing for osteoarthritis. Can. J. Surg. 2022, 65, E504–E511. [Google Scholar] [CrossRef]
- Pietiläinen, S.; Lindström, M.; Laaksonen, I.; Venäläinen, M.S.; Lankinen, P.; Mäkelä, K.T. Long-term blood metal ion levels and clinical outcome after Birmingham hip arthroplasty. Scand. J. Surg. 2022, 111, 14574969211066197. [Google Scholar] [CrossRef] [PubMed]
- Su, E.P.; Ho, H.; Bhal, V.; Housman, L.R.; Masonis, J.L.; Noble, J.W.; Hopper, R.H.; Engh, C.A. Results of the First U.S. FDA-Approved Hip Resurfacing Device at 10-Year Follow-up. J. Bone Jt. Surg. Am. 2021, 103, 1303–1311. [Google Scholar] [CrossRef]
- Høl, P.J.; Hallan, G.; Indrekvam, K. Metal ion levels in the blood of patients with metal-on-metal hip prostheses. Metallionenivåer i blod fra pasienter med metall-mot-metall-hofteprotese. Tidsskr. Nor. Laegeforen 2021, 141, 1–10. [Google Scholar] [CrossRef]
- Kiran, M.; Santhapuri, S.; Moeen, S.; Merchant, I.; Arvinte, D.; Sood, M. 10-year results of ReCap hip resurfacing arthroplasty: A non-designer case series. Hip Int. 2019, 29, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Cooper, H.; Urban, R.M.; Wixson, R.L.; Meneghini, R.; Jacobs, J.J. Adverse local tissue reaction arising from corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J. Bone Jt. Surg. Am. 2013, 95, 865–872. [Google Scholar] [CrossRef]
- Hart, A.J.; Quinn, P.D.; Lali, F.; Sampson, B.; Skinner, J.A.; Powell, J.J.; Nolan, J.; Tucker, K.; Donell, S.; Flanagan, A.; et al. Cobalt from metal-on-metal hip replacements may be the clinically relevant active agent responsible for periprosthetic tissue reactions. Acta Biomater. 2012, 8, 3865–3873. [Google Scholar] [CrossRef]
- Kop, A.M.; Swarts, E. Corrosion of a hip stem with a modular neck taper junction: A retrieval study of 16 cases. J. Arthroplast. 2009, 24, 1019–1023. [Google Scholar] [CrossRef]
- Dyrkacz, R.M.; Brandt, J.-M.; Ojo, O.A.; Turgeon, T.R.; Wyss, U.P. The influence of head size on corrosion and fretting behaviour at the head-neck interface of artificial hip joints. J. Arthroplast. 2013, 28, 1036–1040. [Google Scholar] [CrossRef]
- Panagiotidou, A.; Meswania, J.; Hua, J.; Muirhead-Allwood, S.; Hart, A.; Blunn, G. Enhanced wear and corrosion in modular tapers in total hip replacement is associated with the contact area and surface topography. J. Orthop. Res. 2013, 31, 2032–2039. [Google Scholar] [CrossRef] [Green Version]
- Lavigne, M.; Therrien, M.; Nantel, J.; Roy, A.; Prince, F.; Vendittoli, P.-A. The John Charnley Award: The functional outcome of hip resurfacing and large-head THA is the same: A randomized, double-blind study. Clin. Orthop. Relat. Res. 2010, 468, 326–336. [Google Scholar] [CrossRef] [Green Version]
- Jameson, S.; Baker, P.N.; Mason, J.; Porter, M.L.; Deehan, D.; Reed, M.R. Independent predictors of revision following metal-on-metal hip resurfacing: A retrospective cohort study using National Joint Registry data. J. Bone Jt. Surg. Br. 2012, 94, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Kostretzis, L.; Lavigne, M.; Kiss, M.-O.; Shahin, M.; Barry, J.; Vendittoli, P.-A. Despite higher revision rate, MoM large-head THA offers better clinical scores than HR: 14-year results from a randomized controlled trial involving 48 patients. BMC Musculoskelet Disord. 2021, 22, 400. [Google Scholar] [CrossRef] [PubMed]
- Hastie, G.R.; Collinson, S.C.; Aqil, A.; Basu, S.; Temperley, D.E.; Board, T.N.; Wynn-Jones, H. Study to Assess the Rate of Adverse Reaction to Metal Debris in Hip Resurfacing at a Minimum 13-year Follow-up. J. Arthroplast. 2021, 36, 1055–1059. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Hip Resurfacing | SD (±) | (Range) | Modular Total Hip Arthroplasty | SD (±) | (Range) | p | |
|---|---|---|---|---|---|---|---|
| Age [yrs] | 46.3 | 6.7 | 30–63 | 56.6 | 6.4 | 44–62 | <0.05 |
| Weight [Kg] | 89.5 | 17.2 | 58–134 | 98.7 | 14.1 | 73–119 | 0.065 |
| Height [m] | 1.76 | 0.1 | 1.58–1.95 | 1.78 | 0.1 | 1.68–1.92 | 0.261 |
| BMI [Kg/m2] | 28.4 | 4.5 | 18–39 | 30.1 | 2.5 | 26–33 | 0.100 |
| ASA | 1.6 | 0.6 | 1–3 | 1.4 | 0.5 | 1–2 | 0.657 |
| Follow-up [months] | 141 | 14.1 | 120–170 | 137 | 15.6 | 120–159 | 0.419 |
| Indication of Index Surgery | HR (24 Hips) | THA (15 Hips) |
|---|---|---|
| Primary Hip OA | 19 (79.2%) | 10 (66.7%) |
| DDH | 5 (20.8%) | - |
| Periprosthetic fracture | - | 2 (13.3%) |
| Secondary OA | - | 1 (6.7%) |
| AVN | - | 1 (6.7%) |
| OA in Haemochromatosis | - | 1 (6.7) |
| Implant (N) | Oxford Hips Score | WOMAC | UCLA | |||
|---|---|---|---|---|---|---|
| Mid-Term | Last | Mid-Term | Last | Mid-Term | Last | |
| HR (22) | 45 ± 3.9 (34–48) | 43 ± 9.3 (18–48) | 6 ± 9.4 (0–36) | 9 ± 16.8 (0–54) | 7 ± 1.9 (3–10) | 6 ± 1.8 (3–10) |
| Modular THA (13) | 41 ± 6.4 (27–48) | 43 ± 6.5 (27–48) | 13 ± 15.1 (0–46) | 8 ± 12.5 (0–40) | 6 ± 1.8 (3–9) | 6 ± 2.1 (3–8) |
| p | 0.877 | 0.806 | 0.866 | |||
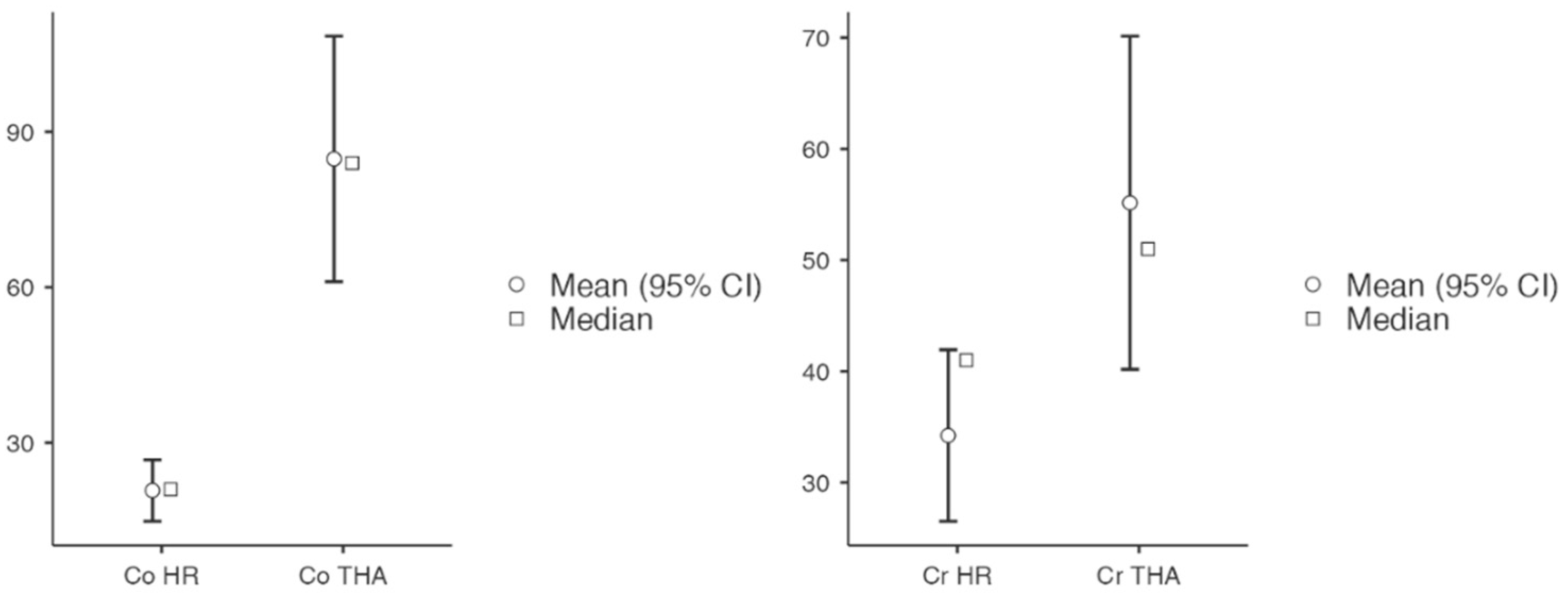
| Cobalt HR (nmol/L) | Chromium HR (nmol/L) | Cobalt Modular THA (nmol/L) | Chromium Modular THA (nmol/L) | |
|---|---|---|---|---|
| N | 20 | 20 | 13 | 13 |
| Mean | 22.3 | 33.5 | 84.8 | 55.2 |
| Median | 21.0 | 37.5 | 84 | 51 |
| SD | 13.8 | 14.9 | 43.6 | 27.6 |
| Minimum | 8 | 8 | 29 | 23 |
| Maximum | 55 | 56 | 140 | 111 |
| HR | Modular THA | Test | Statistic | df | p | Mean Difference | SE Difference |
|---|---|---|---|---|---|---|---|
| Co (nmol/L) | Co (nmol/L) | Student’s t | −5.78 | 12.0 | <0.001 | −64.0 | 11.07 |
| Wilcoxon W | 0.0 | <0.001 | −65.0 | 11.07 | |||
| Cr (nmol/L) | Cr (nmol/L) | Student’s t | −2.15 | 12.0 | 0.026 | −20.9 | 9.75 |
| Wilcoxon W | 17.0 | 0.024 | −17.5 | 9.75 | |||
| Author (Year) | Type of Study | Hip Arthroplasty | Implant | Follow-Up (yrs) | Revision Rate (N) | Metal Ion Levels ± SD (Range) |
|---|---|---|---|---|---|---|
| Gani et al. (2022) [7] | Retrospective | 105 HR | 36 BHR 69 ADEPT | 14.9 | 13.3% (14/105) | Co 26.6 nmol/L ± 24.5 Cr 30.6 nmol/L ± 15.3 |
| Kearns et al. (2022) [46] | Retrospective | 71 HR | BHR | 12.7 ± 1.4 | N/A | Co 3.12 ± 6.31 μg/L = 52.9 nmol/L Cr 2.62 ± 2.69 μg/L = 50.5 nmol/L |
| Pietiläinen et al. (2022) [47] | Retrospective | 171 HR | BHR | 7.5 (3.9–14) | N/A | Co 1.6 ppb (0.1–100) = 27.2 nmol/L Cr 1.5 ppb (0.2–63) = 28.9 nmol/L |
| Kostretzis et al. (2021) [58] | RCT | 24 HR 24 LDH THA | Durom | 15 | HR: 8.3% (2/24) THA: 20.8% (5/24) | HR Co 1.7 μg/L ± 2 = 28.9 nmol/L HR Cr 1.4 μg/L ± 1.1 = 26.9 nmol/L LDH Co 3.8 μg/L ± 3.2 = 64.5 nmol/L LDH Cr 1.9 μg/L ± 1 = 36.6 nmol/L |
| Su et al. (2021) [48] | Retrospective | 280 HR | BHR | 10 | 7.1% | Co 1.3 ppb = 22.1 nmol/L Cr 1.4 ppb = 26.9 nmol/L |
| Høl et al. (2021) [49] | Retrospective | 44 HR | BHR | 5 | N/A | Co 1.1 µg/L (0.4–6.3) = 18.7 nmol/L Cr 1.4 µg/L (0.4–11.7) = 26.9 nmol/L |
| Ridon et al. (2019) [44] | Retrospective | 90 HR 83 LDH THA | Durom | 10 | THA 29.9% HR 2.3% | THA Co 5.75 μg/L (3.82–19.2) = 97.6 nmol/L THA Cr 1.75 μg/L (1.34–2.94) = 33.7 nmol/L HR Co 0.89 μg/L (0.67–2.89) = 15.1 nmol/L HR Cr 1.07 μg/L (0.67–1.65) = 20.6 nmol/L |
| Kiran et al. (2019) [50] | Retrospective | 72 HR | ReCap | 10 | 2.8% (2) | Co 28.83 ± 8.42 nmol/L Cr 39.93 ± 9.64 nmol/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mancino, F.; Finsterwald, M.A.; Jones, C.W.; Prosser, G.H.; Yates, P.J. Metal-on-Metal Hips: Ten-Year Clinical and Radiographic Outcomes of the ADEPT Metal-on-Metal Hip Resurfacing and Modular Total Hip Arthroplasty. J. Clin. Med. 2023, 12, 889. https://doi.org/10.3390/jcm12030889
Mancino F, Finsterwald MA, Jones CW, Prosser GH, Yates PJ. Metal-on-Metal Hips: Ten-Year Clinical and Radiographic Outcomes of the ADEPT Metal-on-Metal Hip Resurfacing and Modular Total Hip Arthroplasty. Journal of Clinical Medicine. 2023; 12(3):889. https://doi.org/10.3390/jcm12030889
Chicago/Turabian StyleMancino, Fabio, Michael A. Finsterwald, Christopher W. Jones, Gareth H. Prosser, and Piers J. Yates. 2023. "Metal-on-Metal Hips: Ten-Year Clinical and Radiographic Outcomes of the ADEPT Metal-on-Metal Hip Resurfacing and Modular Total Hip Arthroplasty" Journal of Clinical Medicine 12, no. 3: 889. https://doi.org/10.3390/jcm12030889