1. Introduction
With the progress in cardiac surgery toward minimally invasive procedures, new challenges have arisen. The limited exploration of the surgical field, limited visibility in terms of optical angulations and longer distances contribute to a steep learning curve [
1,
2].
Atrial fibrillation (AF) is common in patients with heart disease and, if left untreated, is associated with a high risk of thromboembolic events. Oral anticoagulation plays an important role in preventing AF-related thromboembolic complications [
3]. Today, complex interventional or surgical options for the treatment of AF and the prophylaxis of thromboembolism are also available.
The prevalence of AF in patients with mitral valve regurgitation and atrial dilatation is high. The left atrial appendage (LAA), with its rough trabeculae, plays a central role in the development of stroke during atrial fibrillation. The AtriClip
® (AtriCure, Mason, OH, USA) device for LAA exclusion offers a safe and effective approach to managing AF complications. This technique is typically performed in combination with other cardiac surgical procedures under direct or thoracoscopic visualization and under TEE guidance. However, during minimally invasive surgical procedures, spatial constraints within the surgical field may be a challenge when applying the AtriClip
® (AtriCure, Mason, OH, USA) [
3,
4,
5]. Therefore, LAA occlusion is often performed through the transverse pericardial sinus during cardiac arrest. To improve TEE guidance for clip application, a beating heart technique has recently been described [
5].
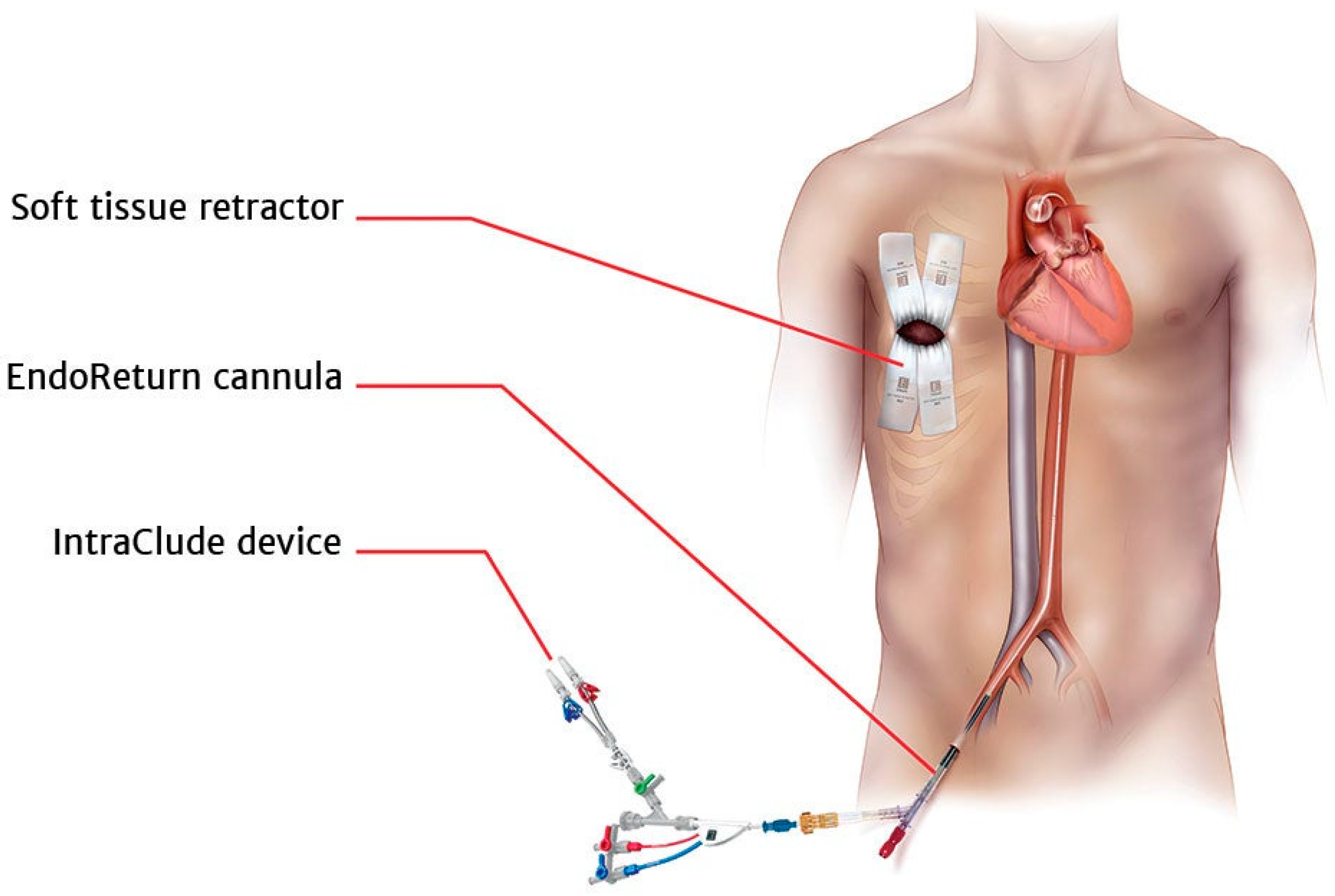
The IntraClude
® device can be used for the intraluminal occlusion of the aorta in patients undergoing a cardiopulmonary bypass with cardiac arrest. This device allows intraluminal pressure monitoring and the administration of cardioplegia during both conventional and minimally invasive cardiac surgery [
6]. The inflated IntraClude
® balloon occludes the ascending aorta and must be applied carefully to avoid distal or proximal migration.
2. Case Presentation
A 62-year-old male patient (172 cm, 70.4 kg, BMI: 23.8 kg/m
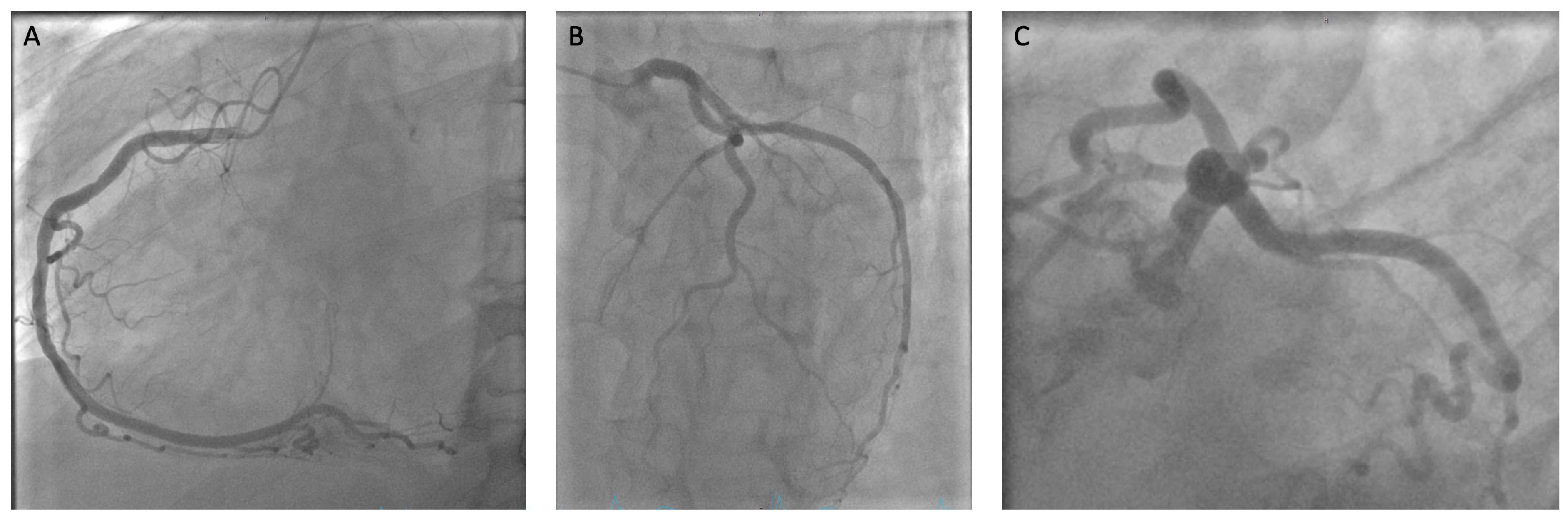
2) was referred to our university department of cardiac surgery with the diagnosis of symptomatic mitral valve regurgitation, tricuspid valve regurgitation and atrial fibrillation. The diagnosis included mild irrelevant aortic regurgitation, a patent foramen ovale, arterial hypertension and a combined pre- and post-capillary pulmonary hypertension. A therapy-relevant stenosing coronary artery disease was excluded by coronary angiography (
Figure 1). The preoperative computed tomography of the aortic was performed to ensure the feasibility of performing a minimally invasive procedure and to exclude occlusive peripheral arterial disease.
Preoperative transesophageal echocardiography (TEE) showed severe mitral valve regurgitation with an eccentric regurgitant jet, a flail of the medial portion of the A3 segment, and a prolapse of the A3 segment. The vena contracta (VC) at 9–10 mm had an estimated effective regurgitant orifice (ERO) of 0.5 cm2 and an estimated regurgitation volume (RV) of 95 mL. Additionally, there was a prolapse in the septal tricuspid valve leaflet with severe tricuspid regurgitation, a VC of 9 mm × 10 mm, an estimated ERO of 0.4 cm2 and an estimated RV of 53 mL. The right ventricular ejection fraction was within the normal range.
3. Surgical Technique
Preoperatively, angio-CT confirmed the feasibility of a peripheral cardio-pulmonary bypass placement via the inguinal vessels with the cross-sectional diameter of the right common femoral artery measuring 14 mm. The ascending aorta had a diameter of 35 mm. Adhesions or anatomic contraindications for a minimally invasive procedure were excluded. A decision for surgical mitral and tricuspid valve repair was made in accordance with the 2021-ESC/EACTS guidelines for the management of valvular heart disease.
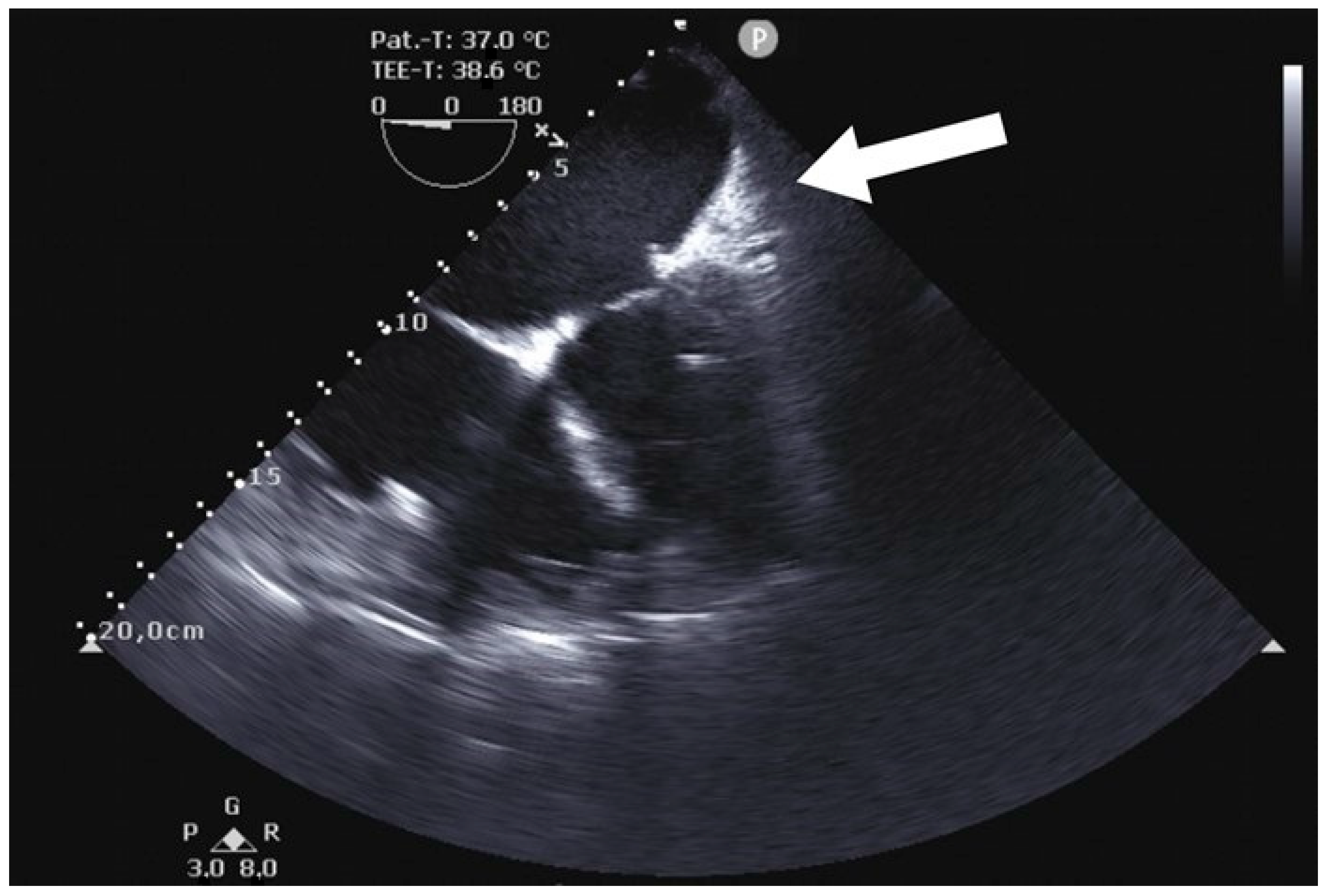
After a skin incision and preparing the right femoral artery and vein, the endoreturn arterial (ThruPort Edwards 23 mm) and bicaval venous peripheral cannulas (Estech RAP 23/25 Fr) were inserted and extracorporeal circulation was initiated. With the use of TEE guidance, the IntraClude
® balloon was positioned in the ascending aorta, with its tip located 20 to 30 mm distal to the aortic annulus at the sinotubular junction level, but was not inflated (
Figure 2).
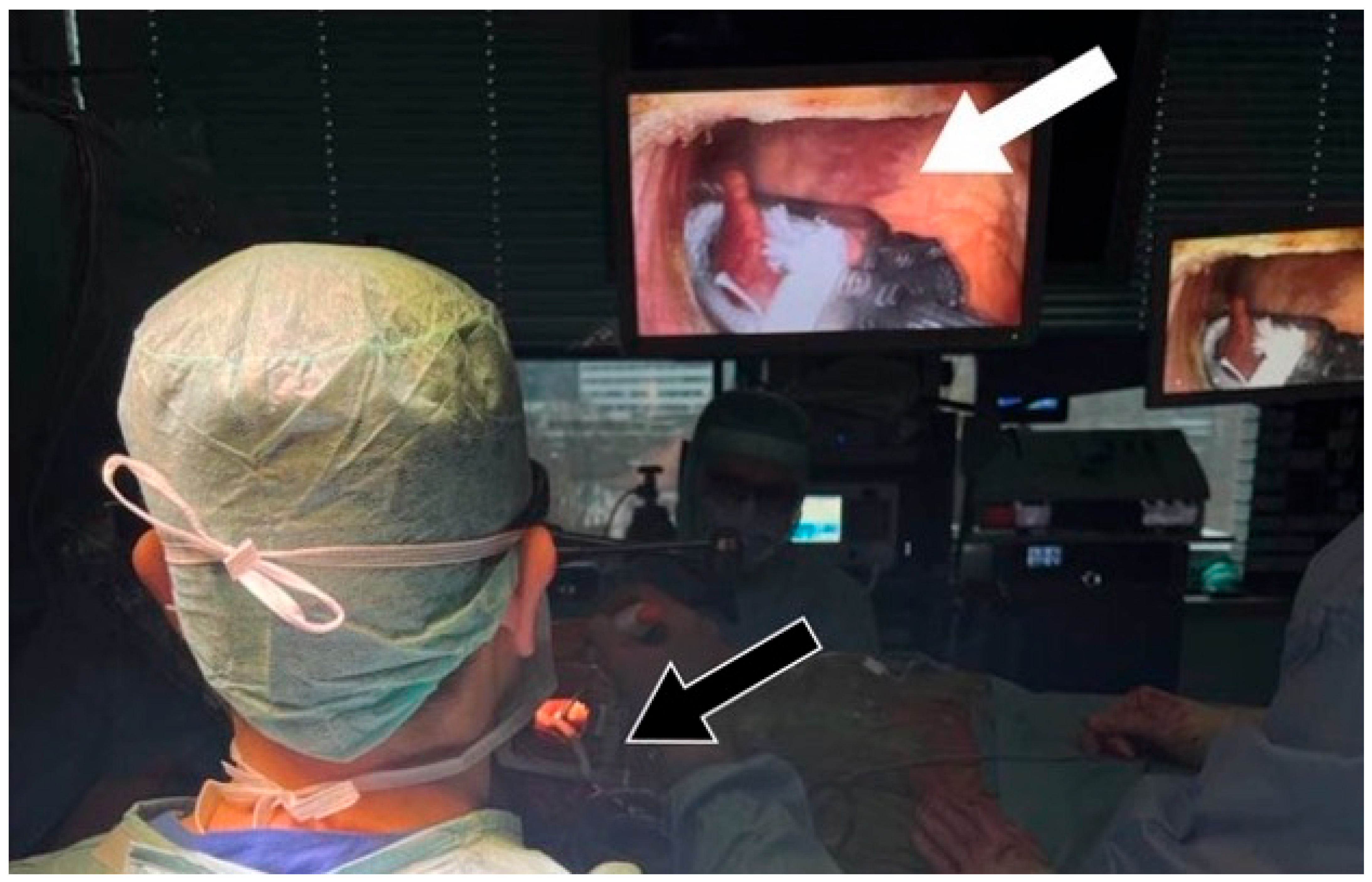
A right mini thoracotomy was performed in the 5th intercostal space (ICS), and a 3D endoscopic camera (Aesculap “Eddy” 3D EinsteinVision Endoscope 30°) was inserted in the 3rd ICS. To enhance visualization, the diaphragm was fixed and pulled down using a U-suture. Subsequently, the right side of the pericardium was opened above the phrenic nerve, exposing the heart. A Jackson–Pratt drain was placed through the transverse pericardial sinus around the aorta, and with lateral traction, the LAA was exposed [
5] (
Figure 3).
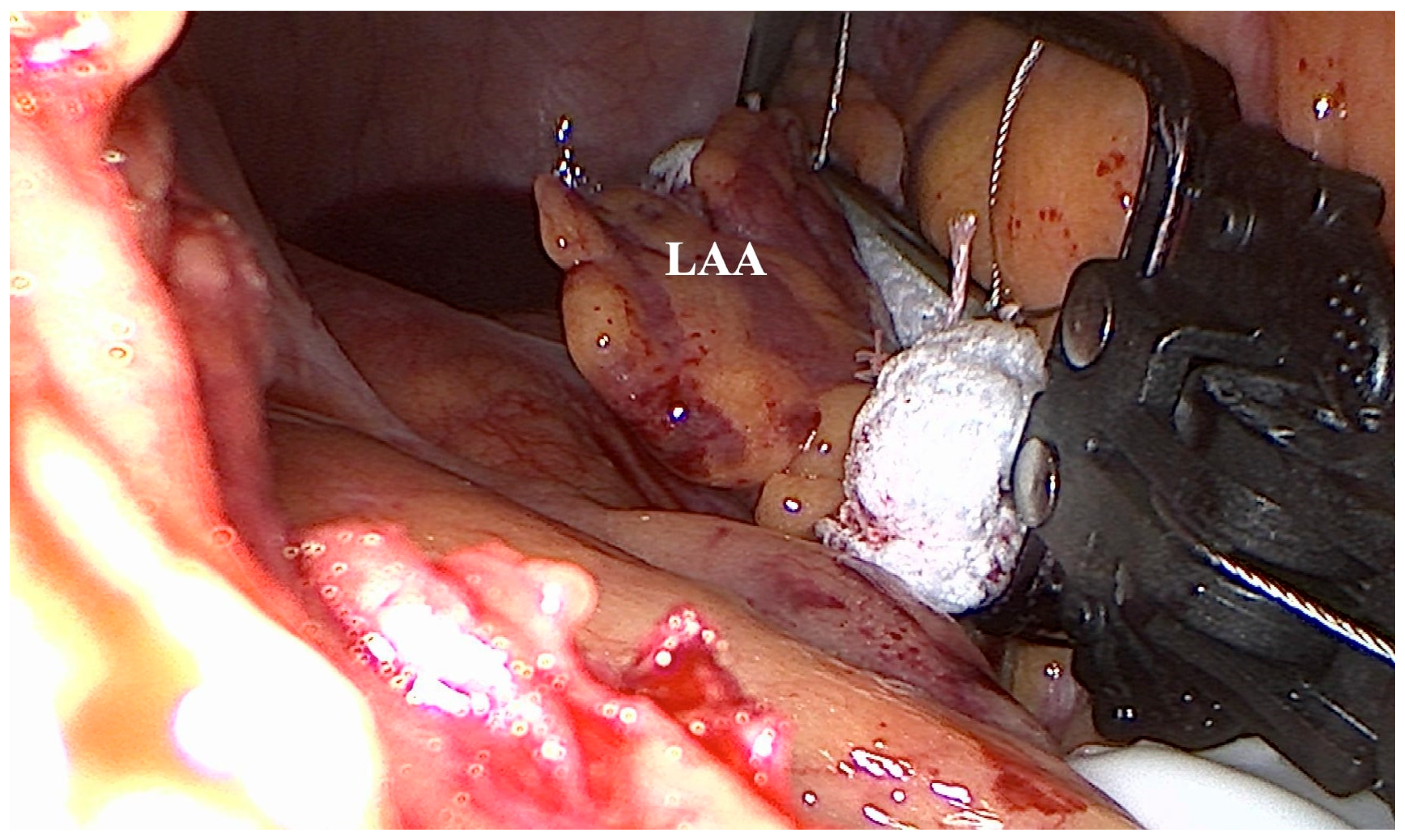
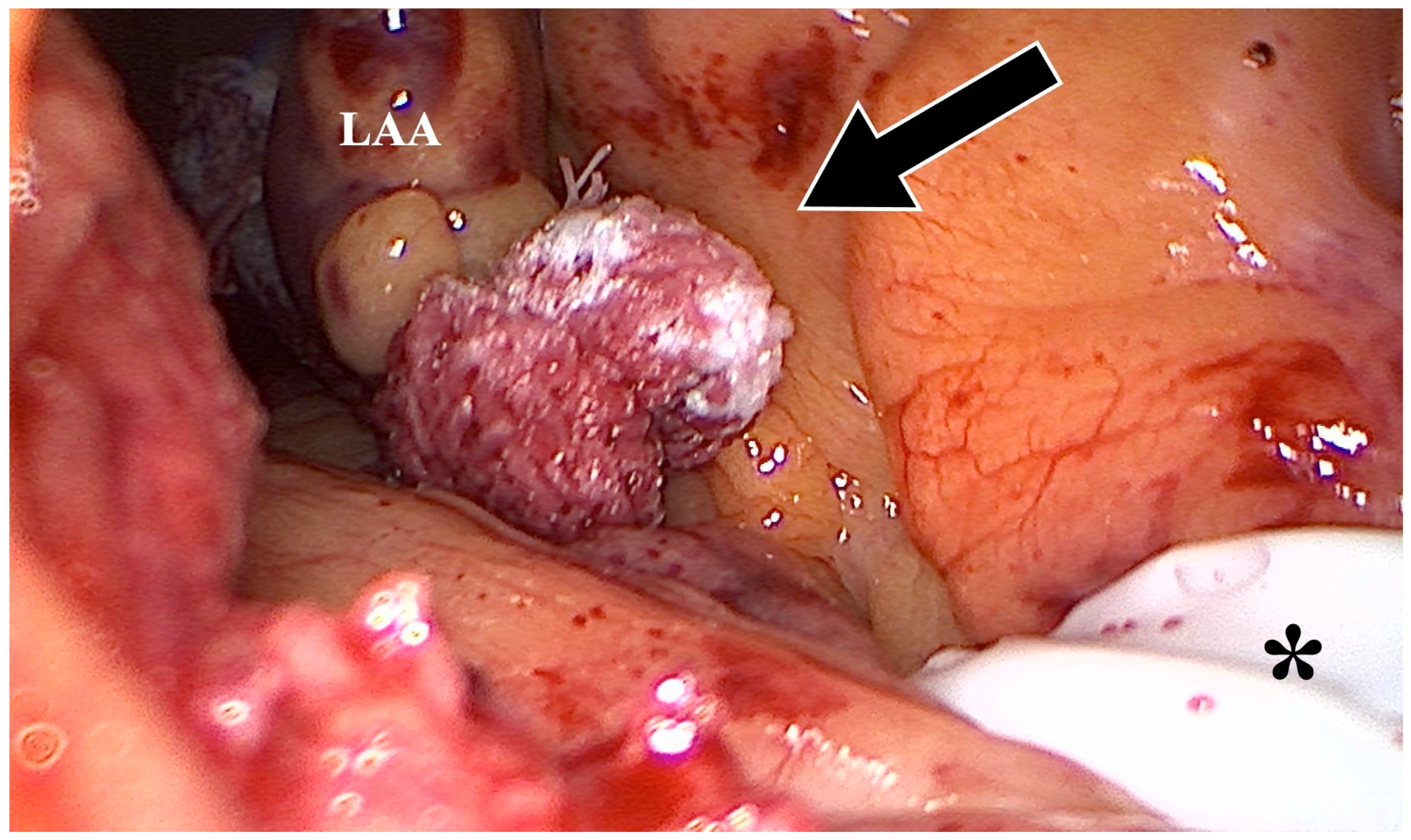
Using the AtriCure
® (AtriCure, Mason, OH, USA) measuring device, the LAA base size was measured. After bending the AtriClip-Pro
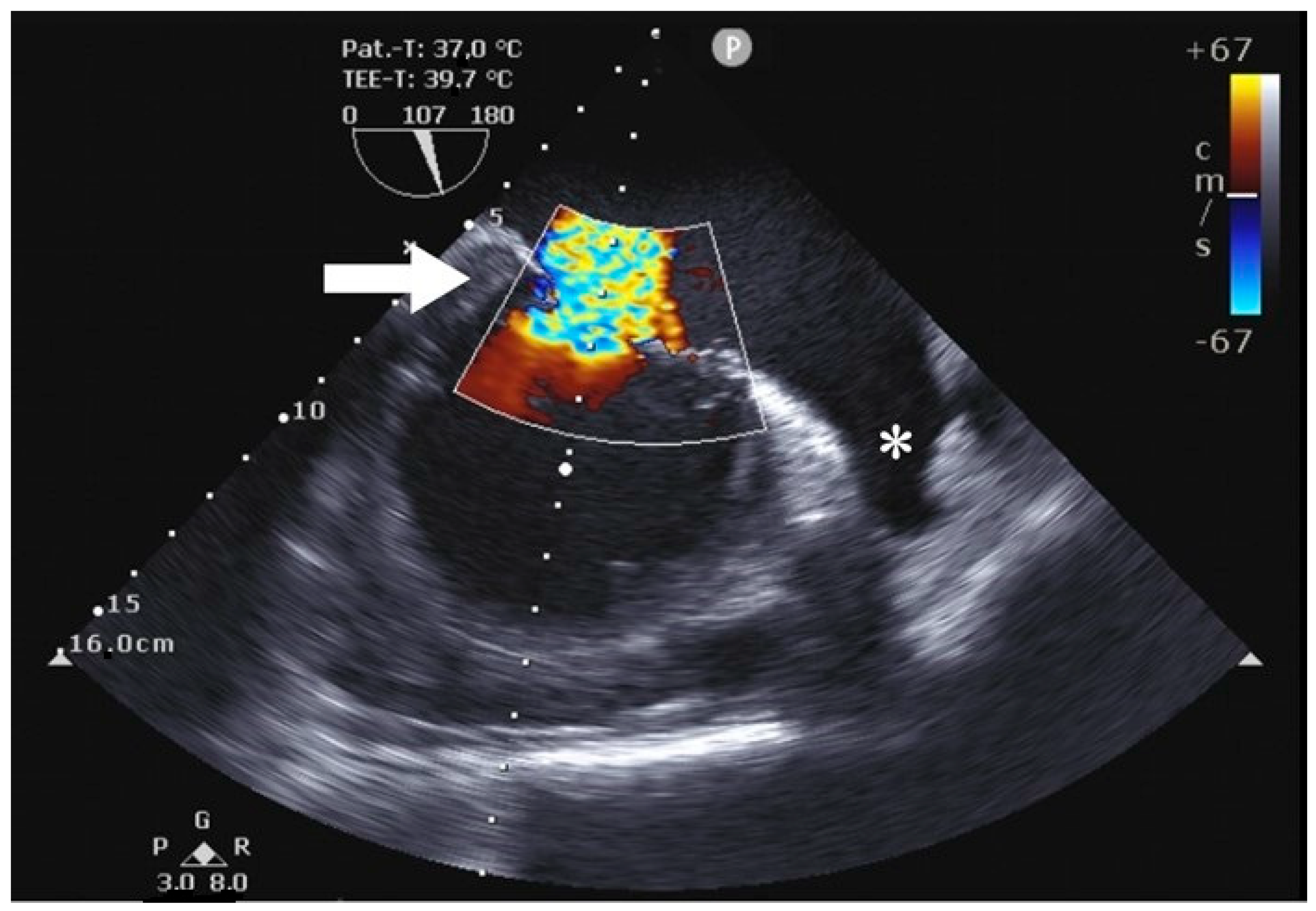
® (AtriCure, Mason, OH, USA) device, the clip was anteriorly passed over the LAA apex, gently compressing the great arteries and exposing the LAA. With a beating heart, the Atriclip-Pro
® (AtriCure, Mason, OH, USA) was adequately placed under TEE guidance (
Figure 4 and
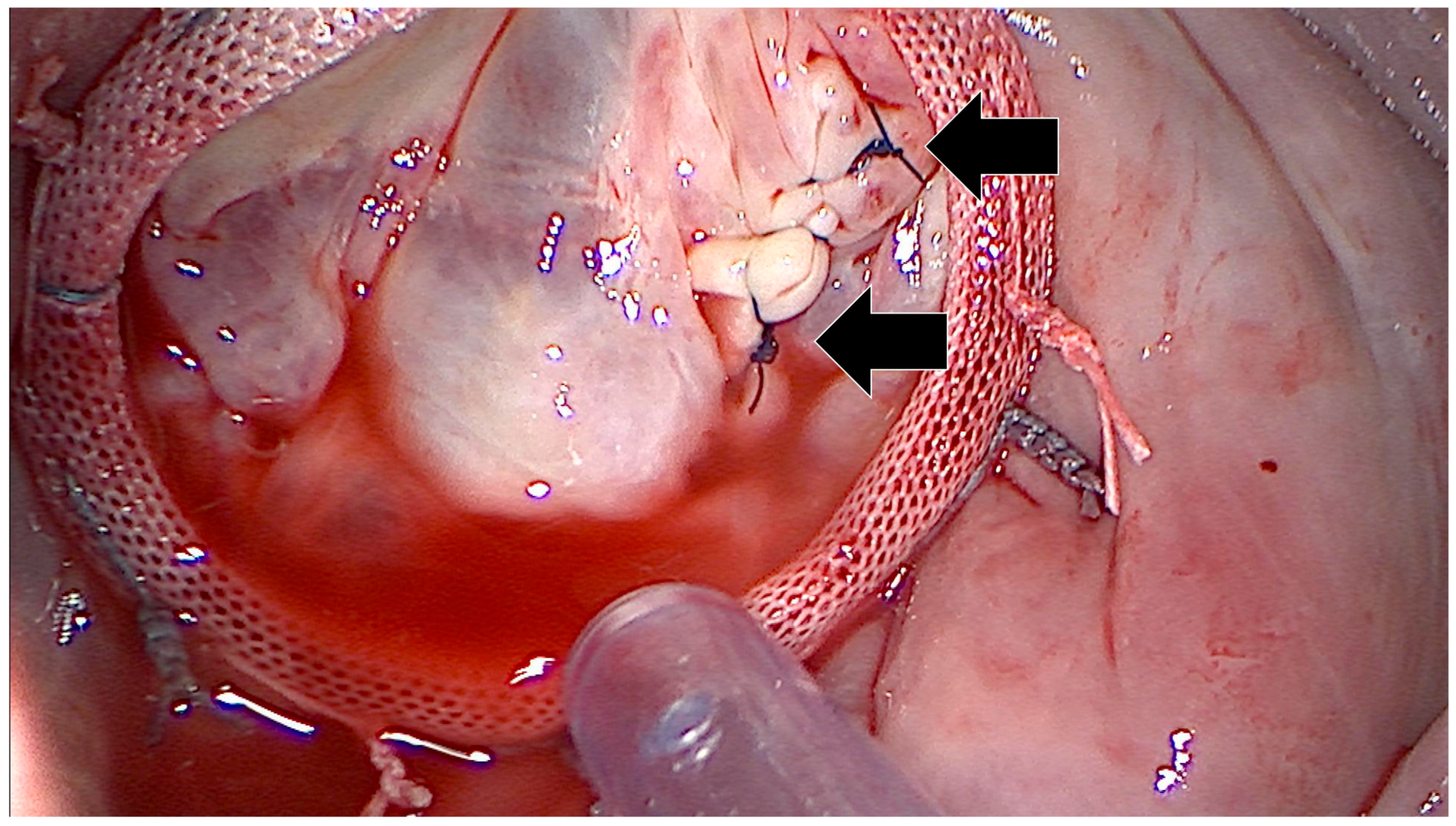
Figure 5), and the device was released after the confirmation of LAA closure (
Figure 6 and
Figure 7;
Supplementary Video S1).
The interatrial sulcus was exposed by placing holding sutures. After the fibrillation of the heart, the ascending aorta was occluded with the IntraClude
® device and antegrade Brettschneider’s cardioplegia (overall volume: 1800 mL) was administered over 7 min. A transverse atriotomy was performed to expose the left atrium. Following a left-sided MAZE procedure, the mitral valve was successfully reconstructed using commissural sutures and the implantation of an Edwards Physio II annuloplasty ring (
Figure 8). The visualized PFO could be closed by direct suture. The left atriotomy was closed after venting the left heart. After slinging both venae cavae, the right atrium was opened. The tricuspid valve was reconstructed with a 34 mm Edwards Physio 6200 Tricuspid Valve annuloplasty ring, and the right atriotomy was closed after venting the right heart. Upon deflating the aortic balloon, a sinus rhythm recurred. Intraoperative transesophageal echocardiography showed a good reconstructive result with a competent mitral and tricuspid valve and an effectively closed LAA. The complete postoperative course was uneventful, and the patient was discharged on postoperative day 9.
4. Discussion
To our knowledge, this is the first case in which LAA closure was performed on the beating heart under minimally invasive conditions using endoclamping.
Minimally invasive mitral valve procedures are becoming increasingly common. Small working ports make anatomy more difficult to visualize, and subsequently, the surgeon has less space to manipulate. In addition, the need to cross-clamp the aorta for cardiopulmonary bypasses increases these difficulties, as the surgeon has limited space to perform the aortic cross-clamping. As conventional aortic cross-clamping (exoclamping) is not always feasible, endoclamping techniques have been developed to improve a minimally invasive procedure approach [
7].
The IntraClude
® device (Edwards Lifesciences) has been shown to be safe and to achieve results comparable with conventional exoclamping [
8]. This makes endoclamping a viable alternative to conventional exoclamping without extending the clamping time or pump time, as well as in-hospital stay and postoperative outcome. However, endoclamping does have disadvantages, including a higher incidence of iatrogenic aortic dissections, challenges in aortic exposure, the instability of the endoclamp, as well as higher costs [
8].
Different pharmacological, interventional and surgical options are available for the treatment of AF. The surgical closure of the LAA has become increasingly important in the mitigation of a stroke. In fact, stapler occlusion, including the resection of the LAA or the use of an epicardial device for LAA occlusion, such as the AtriClip
® (AtriCure, Mason, OH, USA) device, are common procedures. As other authors have shown [
9], the mechanical occlusion of the LAA is not only safe and effective but also results in electrical isolation that reduces the risk of persistent or reoccurrence of AF by 28% [
9].
The conventional approach for LAA occlusion typically involves performing it during cardiac arrest, which can unnecessarily prolong ischemia time. Additionally, this method limits the echocardiographer’s ability to assess occlusion efficacy using TEE due to cardiac emptying during ischemia. Consequently, our technique enables the real-time visualization of the occlusion performed by the surgeon. Furthermore, research has indicated that surgical LAA occlusion might not be as efficacious as the utilization of an external clip, such as the Atriclip
® (AtriCure, Mason, OH, USA). Given the thin and delicate nature of the atrial tissue, the early and delayed tearing of the surgical closure could occur, potentially leading to the reopening of the LAA orifice over time and the recanalization of the LAA [
10] (
Table 1).
The advantage of the “anterior pathway” for the application of an AtriClip® (AtriCure, Mason, OH, USA) is the beating heart technique with TEE guidance, which is achieved by applying lateral traction to the aorta. Moreover, the use of a 30° endoscope provides a superior visibility of the structures posterior to the aorta, such as the LAA. This technique can also be applied when an IntraClude® catheter has been inserted into the ascending aorta but should be performed before balloon inflation.
5. Conclusions
LAA occlusion is an effective surgical technique to prevent stroke from AF. As shown in the presented case, the use of AtriClip® (AtriCure, Mason, OH, USA) during minimally invasive mitral valve replacement is possible, even if endoclamping is planned. However, if possible, the AtriClip® (AtriCure, Mason, OH, USA) should be placed before the aortic occlusion with the IntraClude® device.
Author Contributions
Conception and design: M.N.S., A.-S.K. and C.H.; Administrative support: C.H. and M.W.; Provision of study materials or patients: C.H., J.F. and M.W.; Collection and assembly of data: M.N.S., A.-S.K. and J.F.; Data analysis and interpretation: M.N.S., A.-S.K. and C.H.; Manuscript writing: all authors; Final approval of manuscript: all authors. All authors have read and agreed to the published version of the manuscript.
Funding
The authors acknowledge financial support by Deutsche Forschungsgemeinschaft and Friedrich-Alexander-Universität Erlangen-Nürnberg within the funding programme “Open Access Publication Funding”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Holzhey, D.M.; Seeburger, J.; Misfeld, M.; Borger, M.A.; Mohr, F.W. Learning minimally invasive mitral valve surgery: A cumulative sum sequential probability analysis of 3895 operations from a single high-volume center. Circulation 2013, 128, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Heim, C.; Muller, P.P.; Massoudy, P.; Harig, F.; Nooh, E.; Weyand, M.; Czesla, M. Pass On What You Have Learned: A Structured Mentor-Mentee Concept for the Implementation of a Minimally Invasive Mitral Valve Surgery Program. Eur. Surg. Res. 2022, 63, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Willems, S.; Gunawardene, M.A.; Eickholt, C.; Hartmann, J.; Schmoeckel, M.; Schäffer, B. Medical, interventional, and surgical treatment strategies for atrial fibrillation. Dtsch. Ärzteblatt Int. 2022, 119, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Toale, C.; Fitzmaurice, G.J.; Eaton, D.; Lyne, J.; Redmond, K.C. Outcomes of left atrial appendage occlusion using the AtriClip device: A systematic review. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Vondran, M.; Rose, F.; Treede, H.; Liebold, A.; Doll, N.; Choi, Y.H.; Kaminski, A. Anterior Pathway for Epicardial Left Atrial Appendage Clip Occlusion During Minimally Invasive Atrioventricular Valve Surgery. Innovations 2022, 17, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Marullo, A.G.; Irace, F.G.; Vitulli, P.; Peruzzi, M.; Rose, D.; D’Ascoli, R.; Iaccarino, A.; Pisani, A.; De Carlo, C.; Mazzesi, G.; et al. Recent Developments in Minimally Invasive Cardiac Surgery: Evolution or Revolution? BioMed Res. Int. 2015, 2015, 483025. [Google Scholar] [CrossRef] [PubMed]
- Misfeld, M. Mitralklappenchirurgie der letzten 50 Jahre. Z. Für Herz-Thorax-Und Gefäßchirurgie 2022, 36, 8–18. [Google Scholar] [CrossRef]
- Cetinkaya, A.; Ebraheem, E.; Bramlage, K.; Hein, S.; Bramlage, P.; Choi, Y.H.; Richter, M. Long-term results of endoclamping in patients undergoing minimally invasive mitral valve surgery where external aortic clamping cannot be used—A propensity matched analysis. J. Cardiothorac. Surg. 2020, 15, 313. [Google Scholar] [CrossRef] [PubMed]
- Kiankhooy, A.; Liem, B.; Dunnington, G.H.; Pierce, C.; Eisenberg, S.J.; Burk, S.; Huber, D. Left Atrial Appendage Ligation Using the AtriClip Device: Single-Center Study of Device Safety and Efficacy. Innovations 2022, 17, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Hanke, T.; Sievers, H.H.; Doll, N.; Weimar, T. Surgical closure of the left atrial appendage in patients with atrial fibrillation. Indications, techniques and results. Herzschrittmacherther+ Elektrophysiol 2013, 24, 53–57. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}