
Twelve-Lead ECG, Holter Monitoring Parameters, and Genetic Testing in Brugada Syndrome: Insights from Analysis of Multigenerational Family with a History of Sudden Cardiac Arrest during Physical Activity
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
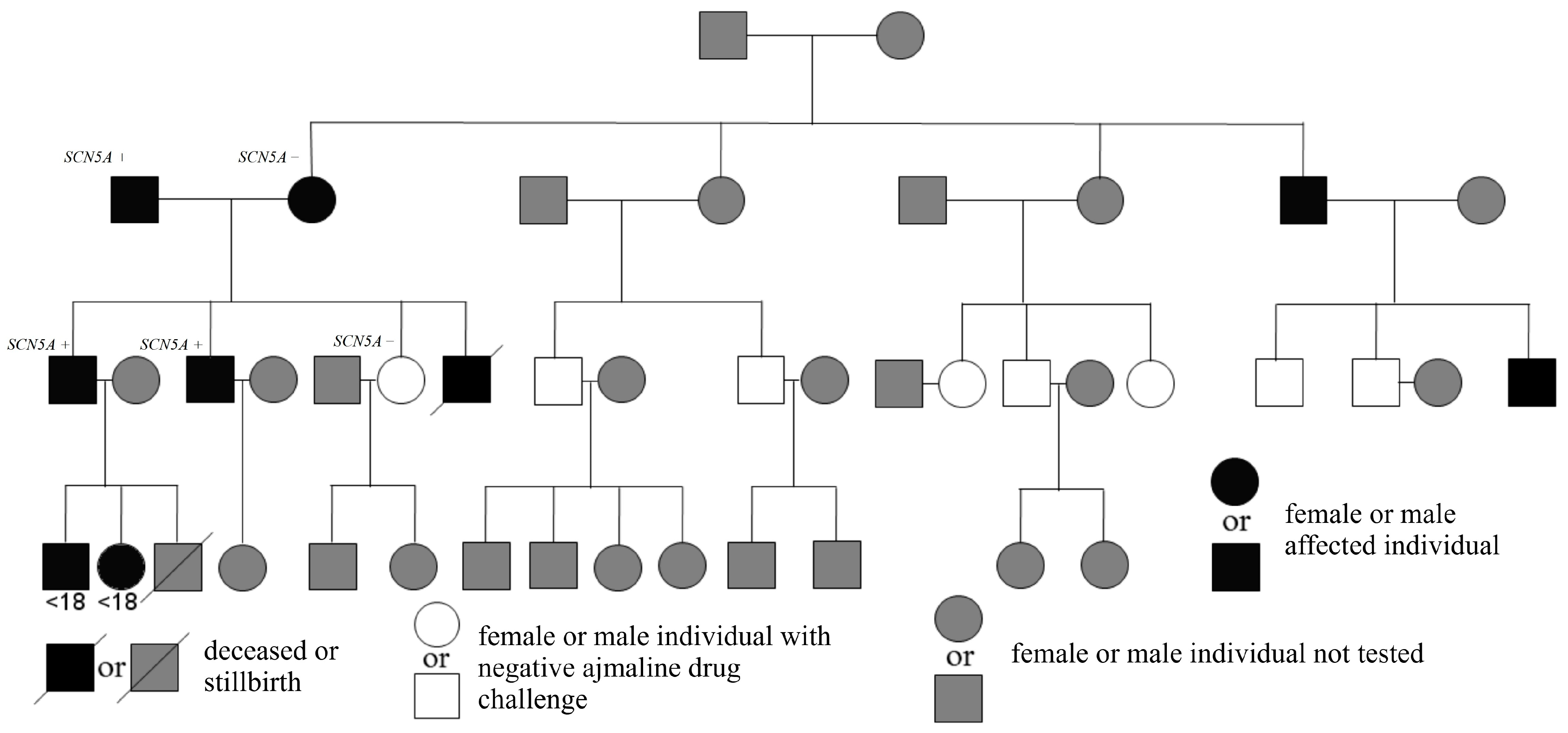
2.1. Patients
2.2. Brugada Syndrome Diagnosis and Risk Assessment
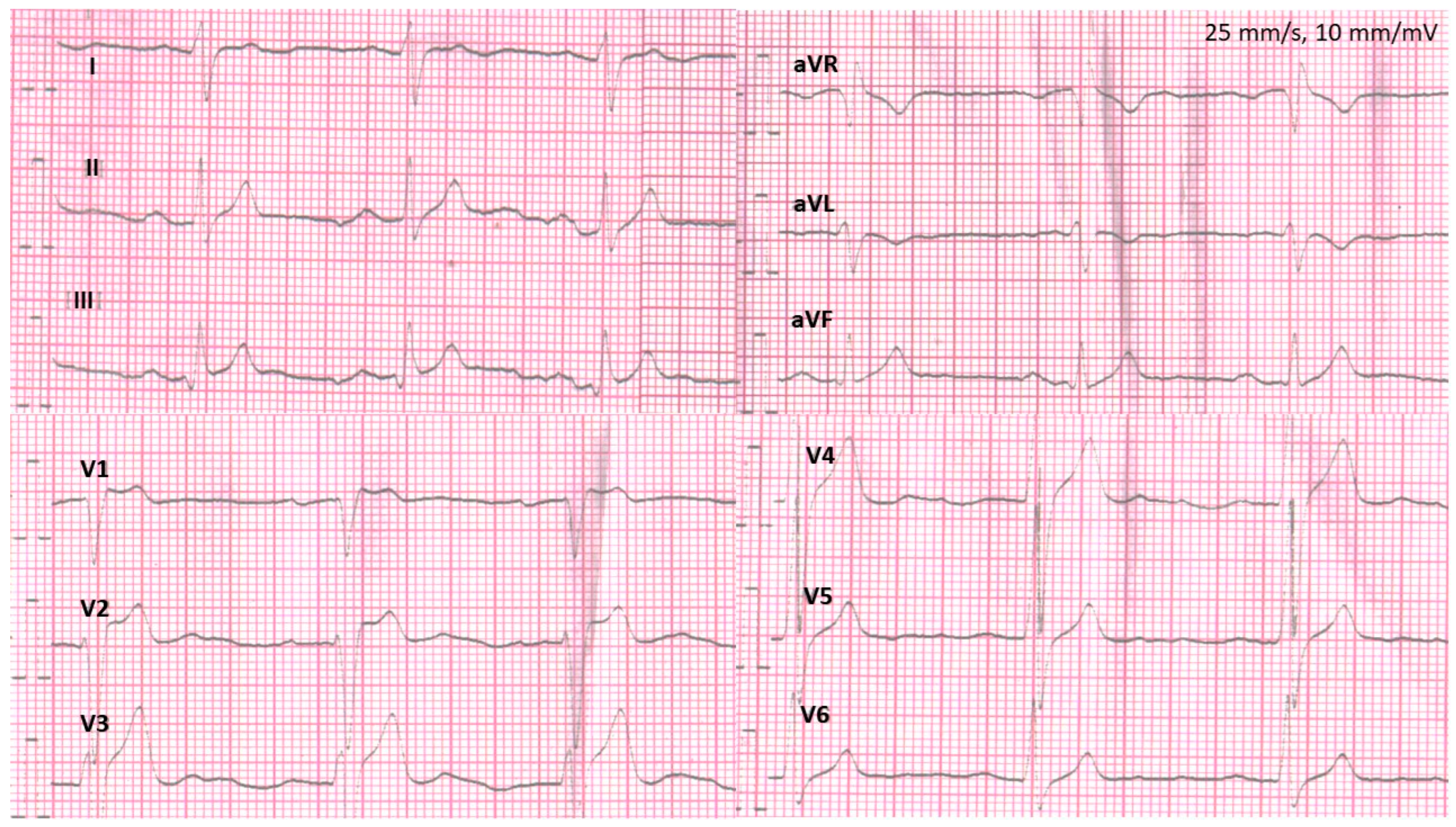
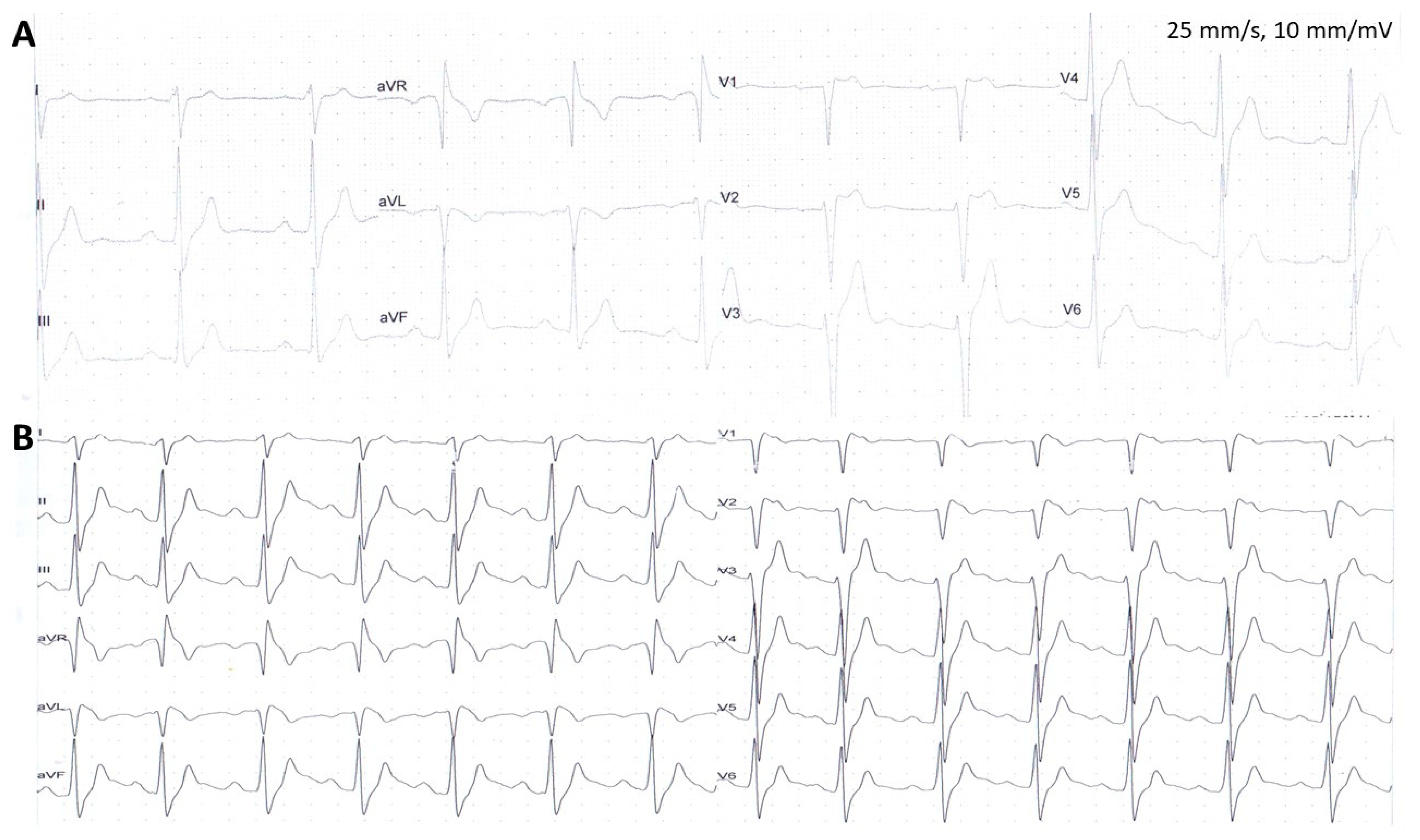
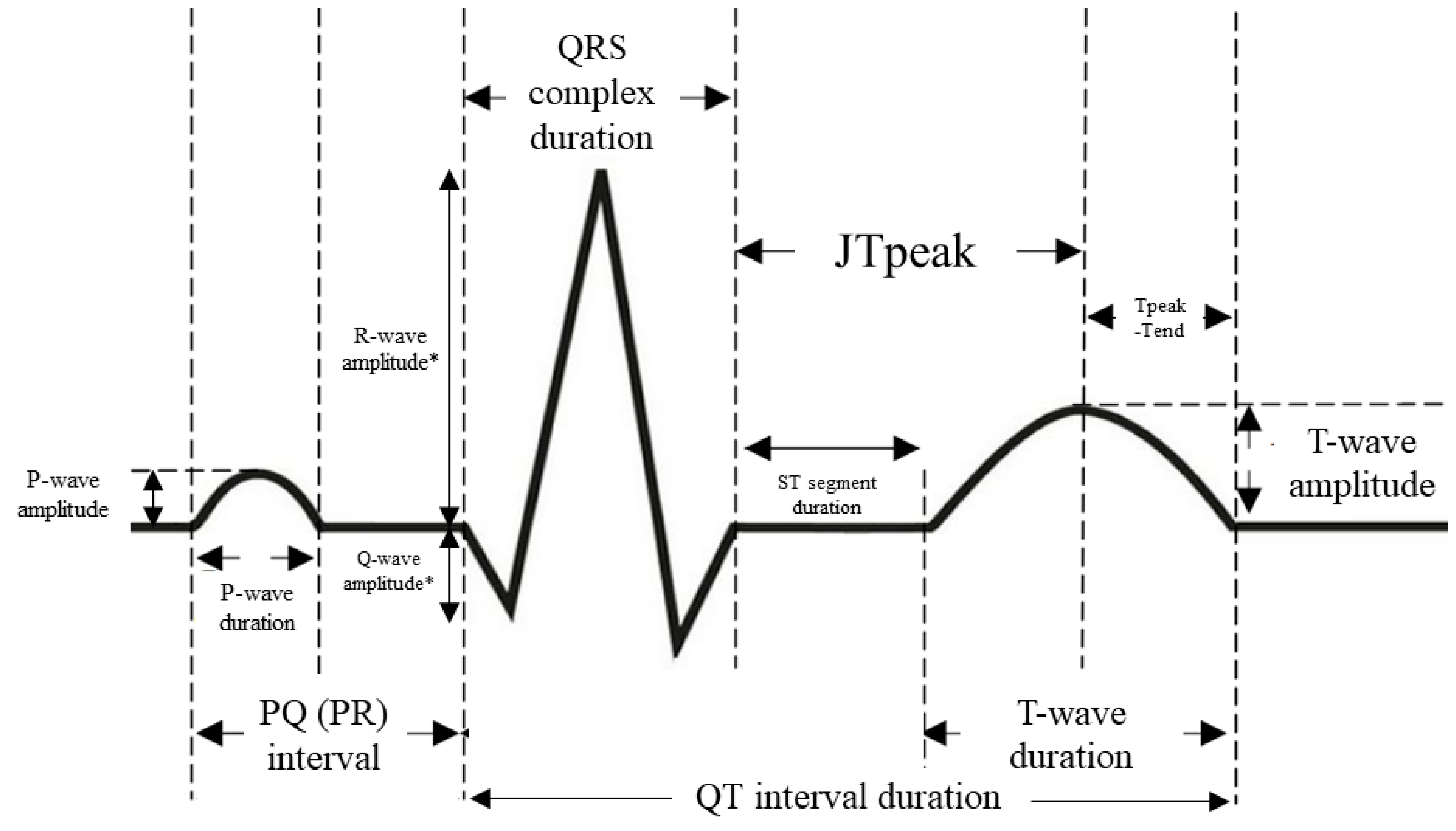
2.3. Electrocardiogram Assessment
2.4. Holter Electrocardiogram Recordings, Exercise Testing, and Echocardiography
2.5. Implantable Cardioverter-Defibrillator Placement and Parameters during Implantation Procedure
2.6. Genetic Testing
2.7. Follow-Up, including Assessment of Arrhythmic Outcomes and Device-Related Complications
2.8. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Electrocardiogram Assessment
3.3. Twenty-Four-Hour Holter Electrocardiogram Recordings, Exercise Testing, and Echocardiography
3.4. Genetic Testing Results
3.5. Follow-Up
4. Discussion
4.1. Characteristics of the Patients
4.2. Twelve-Lead ECG
4.3. Holter ECG Monitoring and Echocardiography
4.4. Genetic Findings
4.5. Limitations of the Study
4.6. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matusik, P.T. Insights into channelopathies: Progress in clinical practice and research. J. Electrocardiol. 2017, 50, 534–535. [Google Scholar] [CrossRef] [PubMed]
- Saffitz, J.E.; Corradi, D. The electrical heart: 25 years of discovery in cardiac electrophysiology, arrhythmias and sudden death. Cardiovasc. Pathol. 2015, 25, 149–157. [Google Scholar] [CrossRef]
- Campuzano, O.; Sarquella-Brugada, G.; Brugada, R.; Brugada, J. Genetics of channelopathies associated with sudden cardiac death. Glob. Cardiol. Sci. Pr. 2015, 2015, 39. [Google Scholar] [CrossRef]
- Brugada, P.; Brugada, J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: A distinct clinical and electrocardiographic syndrome. A multicenter report. J. Am. Coll. Cardiol. 1992, 20, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Aziz, H.M.; Zarzecki, M.P.; Garcia-Zamora, S.; Kim, M.S.; Bijak, P.; Tse, G.; Won, H.H.; Matusik, P.T. Pathogenesis and Management of Brugada Syndrome: Recent Advances and Protocol for Umbrella Reviews of Meta-Analyses in Major Arrhythmic Events Risk Stratification. J. Clin. Med. 2022, 11, 1912. [Google Scholar] [CrossRef] [PubMed]
- Balta, A.; Ceasovschih, A.; Sorodoc, V.; Dimitriadis, K.; Guzel, S.; Lionte, C.; Statescu, C.; Sascau, R.A.; Mantzouranis, E.; Sakalidis, A.; et al. Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders. J. Pers. Med. 2022, 12, 1754. [Google Scholar] [CrossRef]
- Martinez-Barrios, E.; Sarquella-Brugada, G.; Perez-Serra, A.; Fernandez-Falgueras, A.; Cesar, S.; Coll, M.; Puigmule, M.; Iglesias, A.; Alcalde, M.; Vallverdu-Prats, M.; et al. Discerning the Ambiguous Role of Missense TTN Variants in Inherited Arrhythmogenic Syndromes. J. Pers. Med. 2022, 12, 241. [Google Scholar] [CrossRef]
- Vutthikraivit, W.; Rattanawong, P.; Putthapiban, P.; Sukhumthammarat, W.; Vathesatogkit, P.; Ngarmukos, T.; Thakkinstian, A. Worldwide Prevalence of Brugada Syndrome: A Systematic Review and Meta-Analysis. Acta Cardiol. Sin. 2018, 34, 267–277. [Google Scholar] [CrossRef]
- Podolec, P.; Baranchuk, A.; Brugada, J.; Kukla, P.; Lelakowski, J.; Kopec, G.; Rubis, P.; Stepniewski, J.; Podolec, J.; Komar, M.; et al. Clinical classification of rare cardiac arrhythmogenic and conduction disorders, and rare arrhythmias. Pol. Arch. Intern. Med. 2019, 129, 154–159. [Google Scholar] [CrossRef]
- Probst, V.; Goronflot, T.; Anys, S.; Tixier, R.; Briand, J.; Berthome, P.; Geoffroy, O.; Clementy, N.; Mansourati, J.; Jesel, L.; et al. Robustness and relevance of predictive score in sudden cardiac death for patients with Brugada syndrome. Eur. Heart J. 2021, 42, 1687–1695. [Google Scholar] [CrossRef]
- Brugada, R.; Campuzano, O.; Sarquella-Brugada, G.; Brugada, P.; Brugada, J.; Hong, K. Brugada Syndrome. In GeneReviews((R)); Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Osher, H.L.; Wolff, L. Electrocardiographic pattern simulating acute myocardial injury. Am. J. Med. Sci. 1953, 226, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Martini, B.; Nava, A.; Thiene, G.; Buja, G.F.; Canciani, B.; Scognamiglio, R.; Daliento, L.; Dalla Volta, S. Ventricular fibrillation without apparent heart disease: Description of six cases. Am. Heart J. 1989, 118, 1203–1209. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [CrossRef] [PubMed]
- Molitor, N.; Duru, F. Arrhythmogenic Right Ventricular Cardiomyopathy and Differential Diagnosis with Diseases Mimicking Its Phenotypes. J. Clin. Med. 2022, 11, 1230. [Google Scholar] [CrossRef] [PubMed]
- Bayes de Luna, A.; Brugada, J.; Baranchuk, A.; Borggrefe, M.; Breithardt, G.; Goldwasser, D.; Lambiase, P.; Riera, A.P.; Garcia-Niebla, J.; Pastore, C.; et al. Current electrocardiographic criteria for diagnosis of Brugada pattern: A consensus report. J. Electrocardiol. 2012, 45, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Martini, N.; Testolina, M.; Toffanin, G.L.; Arancio, R.; De Mattia, L.; Cannas, S.; Morani, G.; Martini, B. Role of Provocable Brugada ECG Pattern in The Correct Risk Stratification for Major Arrhythmic Events. J. Clin. Med. 2021, 10, 1025. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Juhani Junttila, M. Clinical aspects of inherited J-wave syndromes. Trends Cardiovasc. Med. 2015, 25, 24–30. [Google Scholar] [CrossRef]
- Oliva, A.; Grassi, S.; Pinchi, V.; Cazzato, F.; Coll, M.; Alcalde, M.; Vallverdu-Prats, M.; Perez-Serra, A.; Martinez-Barrios, E.; Cesar, S.; et al. Structural Heart Alterations in Brugada Syndrome: Is it Really a Channelopathy? A Systematic Review. J. Clin. Med. 2022, 11, 4406. [Google Scholar] [CrossRef]
- Wilde, A.A.M.; Semsarian, C.; Marquez, M.F.; Shamloo, A.S.; Ackerman, M.J.; Ashley, E.A.; Sternick, E.B.; Barajas-Martinez, H.; Behr, E.R.; Bezzina, C.R.; et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus Statement on the state of genetic testing for cardiac diseases. Europace 2022, 24, 1307–1367. [Google Scholar] [CrossRef]
- Denham, N.C.; Pearman, C.M.; Ding, W.Y.; Waktare, J.; Gupta, D.; Snowdon, R.; Hall, M.; Cooper, R.; Modi, S.; Todd, D.; et al. Systematic re-evaluation of SCN5A variants associated with Brugada syndrome. J. Cardiovasc. Electrophysiol. 2019, 30, 118–127. [Google Scholar] [CrossRef]
- Mizusawa, Y.; Wilde, A.A. Brugada syndrome. Circ. Arrhythm. Electrophysiol. 2012, 5, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Zienciuk-Krajka, A.; Chmara, M.; Lica-Gorzynska, M.; Dorniak, K.; Kwiatkowska, J.; Kowalski, J.; Kaufmann, D.; Danilowicz-Szymanowicz, L.; Raczak, G. The novel pathogenic variant in the LMNA gene in a four-generation family with sudden deaths and cardiomyopathy: Utility of molecular autopsy. Kardiol. Pol. 2021, 79, 1368–1371. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Avishay, D.M.; Jones, C.R.; Shaikh, J.D.; Kaur, R.; Aljadah, M.; Kichloo, A.; Shiwalkar, N.; Keshavamurthy, S. Sudden cardiac death: Epidemiology, pathogenesis and management. Rev. Cardiovasc. Med. 2021, 22, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Ferradini, V.; Cosma, J.; Romeo, F.; De Masi, C.; Murdocca, M.; Spitalieri, P.; Mannucci, S.; Parlapiano, G.; Di Lorenzo, F.; Martino, A.; et al. Clinical Features of LMNA-Related Cardiomyopathy in 18 Patients and Characterization of Two Novel Variants. J. Clin. Med. 2021, 10, 5075. [Google Scholar] [CrossRef] [PubMed]
- Franke, M.; Ksiazczyk, T.M.; Pietrzak, R.; Werner, B. Incidental diagnosis of Brugada syndrome in two girls hospitalized for pediatric inflammatory multisystem syndrome related to COVID-19 (PIMS-TS). Kardiol. Pol. 2022, 80, 1045–1046. [Google Scholar] [CrossRef]
- Matusik, P.T.; Komar, M.; Podolec, J.; Karkowski, G.; Lelakowski, J.; Podolec, P. Exercise ECG unmasked Brugada sign: Manifestation of the risk of sports-associated sudden cardiac arrest (RCD code: V-1A.1). J. Rare Cardiovasc. Dis. 2017, 3, 92–97. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Antzelevitch, C.; Yan, G.X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace 2017, 19, 665–694. [Google Scholar] [CrossRef]
- Sieira, J.; Conte, G.; Ciconte, G.; Chierchia, G.B.; Casado-Arroyo, R.; Baltogiannis, G.; Di Giovanni, G.; Saitoh, Y.; Julia, J.; Mugnai, G.; et al. A score model to predict risk of events in patients with Brugada Syndrome. Eur. Heart J. 2017, 38, 1756–1763. [Google Scholar] [CrossRef]
- Chung, C.T.; Bazoukis, G.; Radford, D.; Coakley-Youngs, E.; Rajan, R.; Matusik, P.T.; Liu, T.; Letsas, K.P.; Lee, S.; Tse, G. Predictive risk models for forecasting arrhythmic outcomes in Brugada syndrome: A focused review. J. Electrocardiol. 2022, 72, 28–34. [Google Scholar] [CrossRef]
- Tse, G.; Li, K.H.C.; Li, G.; Liu, T.; Bazoukis, G.; Wong, W.T.; Chan, M.T.V.; Wong, M.C.S.; Xia, Y.; Letsas, K.P.; et al. Higher Dispersion Measures of Conduction and Repolarization in Type 1 Compared to Non-type 1 Brugada Syndrome Patients: An Electrocardiographic Study From a Single Center. Front. Cardiovasc. Med. 2018, 5, 132. [Google Scholar] [CrossRef] [PubMed]
- Babai Bigi, M.A.; Aslani, A.; Shahrzad, S. aVR sign as a risk factor for life-threatening arrhythmic events in patients with Brugada syndrome. Heart Rhythm. 2007, 4, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.; Brugada, J.; Oliva, A.; Berruezo-Sanchez, A.; Potenza, D.; Pollevick, G.D.; Guerchicoff, A.; Matsuo, K.; Burashnikov, E.; Dumaine, R.; et al. Value of electrocardiographic parameters and ajmaline test in the diagnosis of Brugada syndrome caused by SCN5A mutations. Circulation 2004, 110, 3023–3027. [Google Scholar] [CrossRef]
- Maury, P.; Sacher, F.; Gourraud, J.B.; Pasquie, J.L.; Raczka, F.; Bongard, V.; Duparc, A.; Mondoly, P.; Sadron, M.; Chatel, S.; et al. Increased Tpeak-Tend interval is highly and independently related to arrhythmic events in Brugada syndrome. Heart Rhythm. 2015, 12, 2469–2476. [Google Scholar] [CrossRef]
- Gray, B.; Kirby, A.; Kabunga, P.; Freedman, S.B.; Yeates, L.; Kanthan, A.; Medi, C.; Keech, A.; Semsarian, C.; Sy, R.W. Twelve-lead ambulatory electrocardiographic monitoring in Brugada syndrome: Potential diagnostic and prognostic implications. Heart Rhythm. 2017, 14, 866–874. [Google Scholar] [CrossRef]
- JCS Joint Working Group. Guidelines for Non-Pharmacotherapy of Cardiac Arrhythmias (JCS 2011). Circ. J. 2013, 77, 249–274. [Google Scholar] [CrossRef]
- Brown, R.B. Sudden Infant Death Syndrome, Pulmonary Edema, and Sodium Toxicity: A Grounded Theory. Diseases 2022, 10, 59. [Google Scholar] [CrossRef]
- Tsai, C.F.; Chuang, Y.T.; Huang, J.Y.; Ueng, K.C. Long-Term Prognosis of Febrile Individuals with Right Precordial Coved-Type ST-Segment Elevation Brugada Pattern: A 10-Year Prospective Follow-Up Study. J. Clin. Med. 2021, 10, 4997. [Google Scholar] [CrossRef]
- Yalta, K.; Taylan, G.; Ozturk, C.; Yalta, T. Fever-induced type-1 Brugada pattern: A sign of revealed Brugada syndrome or just a Brugada phenocopy? Kardiol. Pol. 2022, 80, 1161–1162. [Google Scholar] [CrossRef]
- Werner, B.; Franke, M.; Pietrzak, R.; Książczyk, T.M. Fever-induced type-1 Brugada pattern: A sign of revealed Brugada syndrome or just a Brugada phenocopy? Author’s reply. Kardiol. Pol. (Pol. Heart. J.) 2022, 80, 1163–1164. [Google Scholar] [CrossRef]
- Vasireddi, S.K.; Sattayaprasert, P.; Yang, D.; Dennis, A.T.; Bektik, E.; Fu, J.D.; Mackall, J.A.; Laurita, K.R. Adipogenic Signaling Promotes Arrhythmia Substrates before Structural Abnormalities in TMEM43 ARVC. J. Pers. Med. 2022, 12, 1680. [Google Scholar] [CrossRef] [PubMed]
- Pardo, G.J.; Sepulveda, T.J.; Lira Lp, G.; Perez, S.A.; Dighero, E.B.; Herrera, F.M.; Gonzalez, A.F.; Egger, Z.J.; Ramirez, L.G.; Wiener, D.A.; et al. Sudden cardiac death during exercise due to Brugada syndrome. Report of one case. Rev. Med. Chil. 2021, 149, 939–944. [Google Scholar] [CrossRef]
- Zhu, Y.B.; Zhang, J.H.; Ji, Y.Y.; Hu, Y.N.; Wang, H.L.; Ruan, D.D.; Meng, X.R.; Lin, X.F.; Luo, J.W.; Chen, W. Analysis of a Family with Brugada Syndrome and Sudden Cardiac Death Caused by a Novel Mutation of SCN5A. Cardiol. Res. Pr. 2022, 2022, 9716045. [Google Scholar] [CrossRef]
- Zysko, D.; Sutton, R.; Timler, D.; Furtan, S.; Melander, O.; Fedorowski, A. History of syncope predicts loss of consciousness after head trauma: Retrospective study. Cardiol. J. 2014, 21, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Rivasi, G.; Ungar, A.; Moya, A.; Brignole, M.; Sutton, R.; Fedorowski, A. Syncope: New solutions for an old problem. Kardiol. Pol. 2021, 79, 1068–1078. [Google Scholar] [CrossRef] [PubMed]
- Wilde, A.A.M.; Amin, A.S.; Morita, H.; Tadros, R. Use, misuse, and pitfalls of the drug challenge test in the diagnosis of the Brugada syndrome. Eur. Heart J. 2023, 44, 2427–2439. [Google Scholar] [CrossRef]
- Wolpert, C.; Echternach, C.; Veltmann, C.; Antzelevitch, C.; Thomas, G.P.; Spehl, S.; Streitner, F.; Kuschyk, J.; Schimpf, R.; Haase, K.K.; et al. Intravenous drug challenge using flecainide and ajmaline in patients with Brugada syndrome. Heart Rhythm. 2005, 2, 254–260. [Google Scholar] [CrossRef]
- Conte, G.; Dewals, W.; Sieira, J.; de Asmundis, C.; Ciconte, G.; Chierchia, G.B.; Di Giovanni, G.; Baltogiannis, G.; Saitoh, Y.; Levinstein, M.; et al. Drug-induced brugada syndrome in children: Clinical features, device-based management, and long-term follow-up. J. Am. Coll. Cardiol. 2014, 63, 2272–2279. [Google Scholar] [CrossRef]
- Conte, G.; de Asmundis, C.; Ciconte, G.; Julia, J.; Sieira, J.; Chierchia, G.B.; Brugada, P. Follow-up from childhood to adulthood of individuals with family history of Brugada syndrome and normal electrocardiograms. JAMA 2014, 312, 2039–2041. [Google Scholar] [CrossRef]
- Pranata, R.; Yonas, E.; Chintya, V.; Deka, H.; Raharjo, S.B. Association between PR Interval, First-degree atrioventricular block and major arrhythmic events in patients with Brugada syndrome—Systematic review and meta-analysis. J. Arrhythm. 2019, 35, 584–590. [Google Scholar] [CrossRef]
- Drezner, J.A.; Fischbach, P.; Froelicher, V.; Marek, J.; Pelliccia, A.; Prutkin, J.M.; Schmied, C.M.; Sharma, S.; Wilson, M.G.; Ackerman, M.J.; et al. Normal electrocardiographic findings: Recognising physiological adaptations in athletes. Br. J. Sports Med. 2013, 47, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, T.; Nagase, S.; Kamakura, T.; Wada, M.; Ishibashi, K.; Inoue, Y.Y.; Miyamoto, K.; Noda, T.; Aiba, T.; Takaki, H.; et al. Clinical and Electrocardiographic Differences in Brugada Syndrome With Spontaneous or Drug-Induced Type 1 Electrocardiogram. Circ. J. 2019, 83, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.; Putra, I.C.S.; Pranata, R.; Budiarso, M.N.; Pramudyo, M.; Goenawan, H.; Akbar, M.R.; Kartasasmita, A.S. Electrocardiographic Markers Indicating Right Ventricular Outflow Tract Conduction Delay as a Predictor of Major Arrhythmic Events in Patients With Brugada Syndrome: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 931622. [Google Scholar] [CrossRef] [PubMed]
- Krittayaphong, R.; Veerakul, G.; Nademanee, K.; Kangkagate, C. Heart rate variability in patients with Brugada syndrome in Thailand. Eur. Heart J. 2003, 24, 1771–1778. [Google Scholar] [CrossRef]
- Shimeno, K.; Takagi, M.; Maeda, K.; Tatsumi, H.; Doi, A.; Yoshiyama, M. Usefulness of multichannel Holter ECG recording in the third intercostal space for detecting type 1 Brugada ECG: Comparison with repeated 12-lead ECGs. J. Cardiovasc. Electrophysiol. 2009, 20, 1026–1031. [Google Scholar] [CrossRef]
- Priori, S.G.; Gasparini, M.; Napolitano, C.; Della Bella, P.; Ottonelli, A.G.; Sassone, B.; Giordano, U.; Pappone, C.; Mascioli, G.; Rossetti, G.; et al. Risk stratification in Brugada syndrome: Results of the PRELUDE (PRogrammed ELectrical stimUlation preDictive valuE) registry. J. Am. Coll. Cardiol. 2012, 59, 37–45. [Google Scholar] [CrossRef]
- Morita, H.; Kusano, K.F.; Miura, D.; Nagase, S.; Nakamura, K.; Morita, S.T.; Ohe, T.; Zipes, D.P.; Wu, J. Fragmented QRS as a marker of conduction abnormality and a predictor of prognosis of Brugada syndrome. Circulation 2008, 118, 1697–1704. [Google Scholar] [CrossRef]
- Gray, B.; Gnanappa, G.K.; Bagnall, R.D.; Femia, G.; Yeates, L.; Ingles, J.; Burns, C.; Puranik, R.; Grieve, S.M.; Semsarian, C.; et al. Relations between right ventricular morphology and clinical, electrical and genetic parameters in Brugada Syndrome. PLoS ONE 2018, 13, e0195594. [Google Scholar] [CrossRef]
- van Hoorn, F.; Campian, M.E.; Spijkerboer, A.; Blom, M.T.; Planken, R.N.; van Rossum, A.C.; de Bakker, J.M.; Wilde, A.A.; Groenink, M.; Tan, H.L. SCN5A mutations in Brugada syndrome are associated with increased cardiac dimensions and reduced contractility. PLoS ONE 2012, 7, e42037. [Google Scholar] [CrossRef]
- Catalano, O.; Antonaci, S.; Moro, G.; Mussida, M.; Frascaroli, M.; Baldi, M.; Cobelli, F.; Baiardi, P.; Nastoli, J.; Bloise, R.; et al. Magnetic resonance investigations in Brugada syndrome reveal unexpectedly high rate of structural abnormalities. Eur. Heart J. 2009, 30, 2241–2248. [Google Scholar] [CrossRef]
- Molitor, N.; Medeiros-Domingo, A.; Fokstuen, S.; Ruschitzka, F.; Duru, F.; Saguner, A. Brugada Syndrome Associated with Different Heterozygous SCN5A Variants in Two Unrelated Families. J. Clin. Med. 2022, 11, 5625. [Google Scholar] [CrossRef]
- Ishikawa, T.; Kimoto, H.; Mishima, H.; Yamagata, K.; Ogata, S.; Aizawa, Y.; Hayashi, K.; Morita, H.; Nakajima, T.; Nakano, Y.; et al. Functionally validated SCN5A variants allow interpretation of pathogenicity and prediction of lethal events in Brugada syndrome. Eur. Heart J. 2021, 42, 2854–2863. [Google Scholar] [CrossRef]
- Matusik, P.; Mazur, P.; Stepien, E.; Pfitzner, R.; Sadowski, J.; Undas, A. Architecture of intraluminal thrombus removed from abdominal aortic aneurysm. J. Thromb. Thrombolysis 2010, 30, 7–9. [Google Scholar] [CrossRef]
- Glowicki, B.; Matusik, P.T.; Plens, K.; Undas, A. Prothrombotic State in Atrial Fibrillation Patients With One Additional Risk Factor of the CHA(2)DS(2)-VASc Score (Beyond Sex). Can J. Cardiol. 2019, 35, 634–643. [Google Scholar] [CrossRef]
- Matusik, P.T.; Prior, S.M.; Butenas, S.; Malecka, B.; Lelakowski, J.; Undas, A. Association of cardiac troponin I with prothrombotic alterations in atrial fibrillation. Kardiol. Pol. 2018, 76, 1106–1109. [Google Scholar] [CrossRef]
- Okolska, M.; Skubera, M.; Matusik, P.; Plazak, W.; Pajak, J.; Rog, B.; Podolec, P.; Tomkiewicz-Pajak, L. Chronotropic incompetence causes multiple organ complications in adults after the Fontan procedure. Kardiol. Pol. 2021, 79, 410–417. [Google Scholar] [CrossRef]
- Matusik, P.T.; Lesniak, W.J.; Heleniak, Z.; Undas, A. Thromboembolism and bleeding in patients with atrial fibrillation and stage 4 chronic kidney disease: Impact of biomarkers. Kardiol. Pol. 2021, 79, 1086–1092. [Google Scholar] [CrossRef]
- Crijns, H.; Sanders, P.; Albert, C.M.; Lambiase, P.D. The year in cardiovascular medicine 2021: Arrhythmias. Eur. Heart J. 2022, 43, 1191–1197. [Google Scholar] [CrossRef]
- Matusik, P.; Dubiel, M.; Wizner, B.; Fedyk-Lukasik, M.; Zdrojewski, T.; Opolski, G.; Dubiel, J.; Grodzicki, T. Age-related gap in the management of heart failure patients. The National Project of Prevention and Treatment of Cardiovascular Diseases—POLKARD. Cardiol. J. 2012, 19, 146–152. [Google Scholar] [CrossRef]
- Kempa, M.; Przybylski, A.; Budrejko, S.; Krupa, W.; Kaczmarek, K.; Ostrega, M.; Syska, P.; Sokal, A.; Grabowski, M.; Jagielski, D.; et al. Evolution of implantation technique and indications for a subcutaneous cardioverter-defibrillator: Over 7 years of experience in Poland. Kardiol. Pol. 2021, 79, 1016–1018. [Google Scholar] [CrossRef]
- Pitak, M.J.; Jastrzebski, M.; Rudek-Budzynska, A.; Werynski, P.; Winter, J.; Goreczny, S. Subcutaneous implantable cardioverter-defibrillator and the two-incision intermuscular technique in pediatric patients—A single center experience. Kardiol. Pol. 2021, 79, 1025–1027. [Google Scholar] [CrossRef] [PubMed]
- Kempa, M.; Przybylski, A.; Budrejko, S.; Krupa, W.; Kaczmarek, K.; Kurek, A.; Syska, P.; Sokal, A.; Grabowski, M.; Jagielski, D.; et al. Multicenter Registry of Subcutaneous Cardioverter- -Defibrillator Implantations: A preliminary report. Kardiol. Pol. 2021, 79, 697–699. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Type 1 BrS ECG Pattern (n = 7) | Without Type 1 BrS ECG Pattern (n = 8) | p-Value |
|---|---|---|---|
| Age (years) | 43.0 ± 16.7 | 29.9 ± 6.0 | 0.16 |
| Male sex (%) | 6 (85.7%) | 5 (62.5%) | 0.57 |
| Type 2 BrS ECG changes | 4 (57.1%) | 0 (0%) | 0.026 |
| Syncope $ | 2 (28.6%) | 0 (0%) | 0.20 |
| Syncope or presyncope associated with physical activity $ | 2 (28.6%) | 0 (0%) | 0.20 |
| Early (<45 years) SCD or aborted SCD in FDR | 4 (57.1%) | 1 (12.5%) | 0.10 |
| Relation to index-case | |||
| FDR | 4 (66.7%) | 1 (12.5%) | 0.028 |
| 2nd-degree relative | 1 (16.7%) | 0 (0%) | |
| 3rd-degree relative | 1 (16.7%) | 7 (87.5%) | |
| Scores for diagnosis and/or arrhythmic outcomes risk assessment | |||
| Shanghai Score # | 4.0 (2.5–6.0) | 2.0 (2.0–2.0) | 0.002 |
| Modified Shanghai Score # | 4.5 (4.0–6.0) | 2.0 (2.0–2.0) | <0.001 |
| Sieira model * | 1.0 (0–4.0) | 0 (0–0) | 0.021 |
| Positive aVR sign | 5 (71.4%) | 1 (12.5%) | 0.03 |
| Fragmented QRS complexes ** | 2 (28.6%) | 0 (0%) | 0.20 |
| Variable | Type 1 BrS ECG Pattern (n = 7) | Without Type 1 BrS ECG Pattern (n = 8) | p-Value |
|---|---|---|---|
| Twelve-lead ECG analysis | |||
| RR interval duration [ms] | 900 (811–1066) | 830.5 (754–929.5) | 0.27 |
| P-wave duration [ms] | 120 (102–155) | 92.5 (88–110) | 0.013 |
| P-wave voltage [mV] | 0.13 (0.05–0.14) | 0.09 (0.08–0.10) | 0.45 |
| PQ (PR) interval duration [ms] | 211.3 ± 26.3 | 161.6 ± 18.9 | 0.001 |
| Prolonged PQ interval duration, n [%] | 4 (57%) | 0 (0%) | 0.026 |
| QRS complex duration [ms] | 125 (87–128) | 89 (86–98.5) | 0.18 |
| Prolonged QRS complex duration, n [%] | 4 (57%) | 0 (0%) | 0.026 |
| QTc interval duration [ms] | 401 (387–403) | 389 (376–427) | 0.52 |
| JTpeak interval in V1 [ms] | 172.9 ± 29.7 | 183.1 ± 32.9 | 0.54 |
| JTpeak interval in V2 [ms] | 165 ± 24.2 | 170.6 ± 21.5 | 0.64 |
| T-wave duration [ms] | 165 (165–195) | 193 (178–204) | 0.093 |
| T-wave voltage [mV] | 0.20 (0.20–0.23) | 0.36 (0.21–0.53) | 0.083 |
| Tpeak-Tend interval in V1 [ms] | 85 ± 17.2 | 85 ± 16.6 | 1.0 |
| Tpeak-Tend interval in V2 [ms] | 105.8 ± 9.1 | 101.4 ± 22.7 | 0.63 |
| Prolonged Tpeak-Tend interval in V1, n [%] | 1 (17%) | 2 (33%) | 0.55 |
| Prolonged Tpeak-Tend interval in V2, n [%] | 4 (57%) | 6 (75%) | 0.43 |
| Holter ECG monitoring analysis # | |||
| Mean heart rate [bpm] | 65.0 ± 7.0 | 75.1 ± 6.9 | 0.019 |
| Minimal heart rate [bpm] | 48.2 ± 6.1 | 54.4 ± 4.6 | 0.049 |
| Maximal heart rate [bpm] | 97.3 ± 8.5 | 121.1 ± 9.4 | <0.001 |
| Supraventricular extrasystolic beats [n] | 5.5 (2.0–12.0) | 0.5 (0.0–5.5) | 0.26 |
| Ventricular extrasystolic beats [n] | 1.0 (0.0–7.0) | 3.0 (0.5–18.5) | 0.74 |
| Echocardiography study results ## | |||
| Left ventricular ejection fraction [%] | 65.0 (63–70) | 65.0 (62–66) | 0.61 |
| Left ventricular end-diastolic diameter [mm] | 48.9 ± 3.4 | 47.8 ± 2.4 | 0.55 |
| Left ventricular end-systolic diameter [mm] | 31.8 ± 6.3 | 31.4 ± 3.6 | 0.92 |
| Interventricular septum thickness [mm] | 9.9 ± 1.1 | 9.7 ± 1.8 | 0.24 |
| Posterior wall thickness [mm] | 10.0 (10.0–11.0) | 10.5 (9.0–11.0) | 0.77 |
| Left atrial diameter [mm] | 37.3 ± 4.3 | 34.5 ± 3.4 | 0.24 |
| Ascending aorta diameter [mm] | 29.8 ± 4.0 | 28.3 ± 3.5 | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matusik, P.T.; Bijak, P.; Kaźnica-Wiatr, M.; Karpiński, M.; Matusik, P.S.; Maziarz, A.; Podolec, P.; Lelakowski, J. Twelve-Lead ECG, Holter Monitoring Parameters, and Genetic Testing in Brugada Syndrome: Insights from Analysis of Multigenerational Family with a History of Sudden Cardiac Arrest during Physical Activity. J. Clin. Med. 2023, 12, 6581. https://doi.org/10.3390/jcm12206581
Matusik PT, Bijak P, Kaźnica-Wiatr M, Karpiński M, Matusik PS, Maziarz A, Podolec P, Lelakowski J. Twelve-Lead ECG, Holter Monitoring Parameters, and Genetic Testing in Brugada Syndrome: Insights from Analysis of Multigenerational Family with a History of Sudden Cardiac Arrest during Physical Activity. Journal of Clinical Medicine. 2023; 12(20):6581. https://doi.org/10.3390/jcm12206581
Chicago/Turabian StyleMatusik, Paweł T., Piotr Bijak, Magdalena Kaźnica-Wiatr, Marek Karpiński, Patrycja S. Matusik, Andrzej Maziarz, Piotr Podolec, and Jacek Lelakowski. 2023. "Twelve-Lead ECG, Holter Monitoring Parameters, and Genetic Testing in Brugada Syndrome: Insights from Analysis of Multigenerational Family with a History of Sudden Cardiac Arrest during Physical Activity" Journal of Clinical Medicine 12, no. 20: 6581. https://doi.org/10.3390/jcm12206581