

Cardiovascular Safety Evaluation of Febuxostat and Allopurinol: Findings from the FDA Adverse Event Reporting System
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source, Extraction and Processing
2.2. Visualization of Data
2.3. Statistical Analysis
3. Results
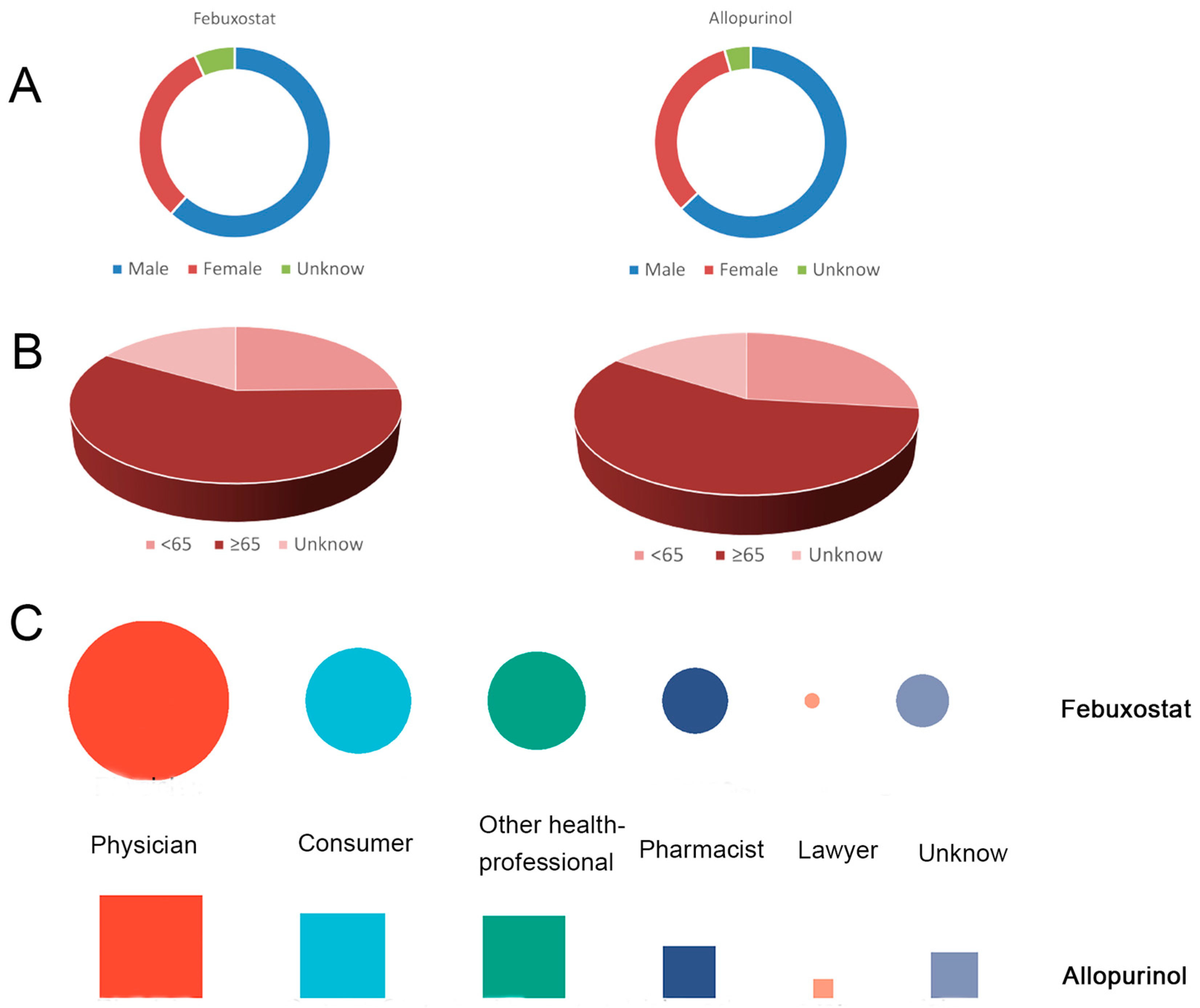
3.1. Study Population
3.2. Signaling of Cardiovascular Adverse Events with Febuxostat
3.3. Signaling of Cardiovascular Adverse Events with Allopurinol
3.4. Febuxostat Is Associated with an Increased Risk of Heart Failure, Ischemic Heart Disease, Hypertension, and Cardiomyopathy in Patients with Gout
3.5. Febuxostat Is Associated with a Higher Risk of Cardiovascular Adverse Events in Elderly Patients with Gout
3.6. Concomitant Use of Acetic Acid Derivatives NSAIDS Increased the Incidence of Cardiovascular Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dalbeth, N.; Gosling, A.L.; Gaffo, A.; Abhishek, A. Gout. Lancet 2021, 397, 1843–1855. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Rheumatol. 2020, 72, 879–895. [Google Scholar] [CrossRef]
- Okafor, O.N.; Farrington, K.; Gorog, D.A. Allopurinol as a therapeutic option in cardiovascular disease. Pharmacol. Ther. 2017, 172, 139–150. [Google Scholar] [CrossRef]
- Day, R.O.; Kannangara, D.R.; Stocker, S.L.; Carland, J.E.; Williams, K.M.; Graham, G.G. Allopurinol: Insights from studies of dose-response relationships. Expert. Opin. Drug Metab. Toxicol. 2017, 13, 449–462. [Google Scholar] [CrossRef]
- Annink, K.V.; Franz, A.R.; Derks, J.B.; Rudiger, M.; Bel, F.V.; Benders, M. Allopurinol: Old Drug, New Indication in Neonates? Curr. Pharm. Des. 2017, 23, 5935–5942. [Google Scholar] [CrossRef]
- Stamp, L.K.; Barclay, M.L. How to prevent allopurinol hypersensitivity reactions? Rheumatology 2018, 57, i35–i41. [Google Scholar] [CrossRef]
- Hung, S.I.; Chung, W.H.; Liou, L.B.; Chu, C.C.; Lin, M.; Huang, H.P.; Lin, Y.L.; Lan, J.L.; Yang, L.C.; Hong, H.S.; et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc. Natl. Acad. Sci. USA 2005, 102, 4134–4139. [Google Scholar] [CrossRef]
- Hershfield, M.S.; Callaghan, J.T.; Tassaneeyakul, W.; Mushiroda, T.; Thorn, C.F.; Klein, T.E.; Lee, M.T. Clinical Pharmacogenetics Implementation Consortium guidelines for human leukocyte antigen-B genotype and allopurinol dosing. Clin. Pharmacol. Ther. 2013, 93, 153–158. [Google Scholar] [CrossRef]
- Waller, A.; Jordan, K.M. Use of febuxostat in the management of gout in the United Kingdom. Ther. Adv. Musculoskelet. Dis. 2017, 9, 55–64. [Google Scholar] [CrossRef]
- Pascual, E.; Sivera, F.; Yasothan, U.; Kirkpatrick, P. Febuxostat. Nat. Rev. Drug Discov. 2009, 8, 191–192. [Google Scholar] [CrossRef]
- Juge, P.A.; Truchetet, M.E.; Pillebout, E.; Ottaviani, S.; Vigneau, C.; Loustau, C.; Cornec, D.; Pascart, T.; Snanoudj, R.; Bailly, F.; et al. Efficacy and safety of febuxostat in 73 gouty patients with stage 4/5 chronic kidney disease: A retrospective study of 10 centers. Jt. Bone Spine 2017, 84, 595–598. [Google Scholar] [CrossRef]
- Yefei, H. Practice guideline for patients with hyperuricemia/gout. Zhonghua Xue Ye Xue Za Zhi 2020, 59, 519–527. [Google Scholar]
- FDA to Evaluate Increased Risk of Heart-Related Death and Death from All Causes with the Gout Medicine Febuxostat (Uloric). Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-adds-boxed-warning-increased-risk-death-gout-medicine-uloric-febuxostat (accessed on 22 July 2023).
- Singh, J.A.; Cleveland, J.D. Comparative effectiveness of allopurinol and febuxostat for the risk of atrial fibrillation in the elderly: A propensity-matched analysis of Medicare claims data. Eur. Heart J. 2019, 40, 3046–3054. [Google Scholar] [CrossRef]
- Desideri, G.; Rajzer, M.; Gerritsen, M.; Nurmohamed, M.T.; Giannattasio, C.; Tausche, A.K.; Borghi, C. Effects of intensive urate lowering therapy with febuxostat in comparison with allopurinol on pulse wave velocity in patients with gout and increased cardiovascular risk: The FORWARD study. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 236–242. [Google Scholar] [CrossRef]
- Ju, C.; Lai, R.W.C.; Li, K.H.C.; Hung, J.K.F.; Lai, J.C.L.; Ho, J.; Liu, Y.; Tsoi, M.F.; Liu, T.; Cheung, B.M.Y.; et al. Comparative cardiovascular risk in users versus non-users of xanthine oxidase inhibitors and febuxostat versus allopurinol users. Rheumatology 2020, 59, 2340–2349. [Google Scholar] [CrossRef]
- Chen, C.H.; Chen, C.B.; Chang, C.J.; Lin, Y.J.; Wang, C.W.; Chi, C.C.; Lu, C.W.; Chen, W.T.; Pan, R.Y.; Su, S.C.; et al. Hypersensitivity and Cardiovascular Risks Related to Allopurinol and Febuxostat Therapy in Asians: A Population-Based Cohort Study and Meta-Analysis. Clin. Pharmacol. Ther. 2019, 106, 391–401. [Google Scholar] [CrossRef]
- White, W.B.; Saag, K.G.; Becker, M.A.; Borer, J.S.; Gorelick, P.B.; Whelton, A.; Hunt, B.; Castillo, M.; Gunawardhana, L.; Investigators, C. Cardiovascular Safety of Febuxostat or Allopurinol in Patients with Gout. N. Engl. J. Med. 2018, 378, 1200–1210. [Google Scholar] [CrossRef]
- Mackenzie, I.S.; Ford, I.; Nuki, G.; Hallas, J.; Hawkey, C.J.; Webster, J.; Ralston, S.H.; Walters, M.; Robertson, M.; De Caterina, R.; et al. Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): A multicentre, prospective, randomised, open-label, non-inferiority trial. Lancet 2020, 396, 1745–1757. [Google Scholar] [CrossRef]
- Ahdi, H.S.; Wichelmann, T.A.; Pandravada, S.; Ehrenpreis, E.D. Medication-induced osteonecrosis of the jaw: A review of cases from the Food and Drug Administration Adverse Event Reporting System (FAERS). BMC Pharmacol. Toxicol. 2023, 24, 15. [Google Scholar] [CrossRef]
- Yu, R.J.; Krantz, M.S.; Phillips, E.J.; Stone, C.A., Jr. Emerging Causes of Drug-Induced Anaphylaxis: A Review of Anaphylaxis-Associated Reports in the FDA Adverse Event Reporting System (FAERS). J. Allergy Clin. Immunol. Pract. 2021, 9, 819–829.e812. [Google Scholar] [CrossRef]
- Faruque, L.I.; Ehteshami-Afshar, A.; Wiebe, N.; Tjosvold, L.; Homik, J.; Tonelli, M. A systematic review and meta-analysis on the safety and efficacy of febuxostat versus allopurinol in chronic gout. Semin. Arthritis Rheum. 2013, 43, 367–375. [Google Scholar] [CrossRef]
- Zhang, S.; Xu, T.; Shi, Q.; Li, S.; Wang, L.; An, Z.; Su, N. Cardiovascular Safety of Febuxostat and Allopurinol in Hyperuricemic Patients With or Without Gout: A Network Meta-Analysis. Front. Med. 2021, 8, 698437. [Google Scholar] [CrossRef]
- Deng, J.H.; Zhang, J.X. Comment on: Cardiovascular safety of febuxostat compared to allopurinol for the treatment of gout: A systematic and meta-analysis. Clin. Cardiol. 2022, 45, 685–686. [Google Scholar] [CrossRef]
- Shin, A.; Choi, S.R.; Han, M.; Ha, Y.J.; Lee, Y.J.; Lee, E.B.; Kang, E.H. Cardiovascular safety associated with febuxostat versus allopurinol among patients with gout: Update with accumulated use of febuxostat. Semin. Arthritis Rheum. 2022, 56, 152080. [Google Scholar] [CrossRef]
- Wu, B.; Wu, F.B.; Luo, M.; Qin, Z.; Xu, T. Application of MedEx in FAERS drug names standardization. Chin. J. Hosp. Pharm. 2019, 39, 1989–1992. [Google Scholar]
- Seabroke, S.; Candore, G.; Juhlin, K.; Quarcoo, N.; Wisniewski, A.; Arani, R.; Painter, J.; Tregunno, P.; Noren, G.N.; Slattery, J. Performance of Stratified and Subgrouped Disproportionality Analyses in Spontaneous Databases. Drug Saf. 2016, 39, 355–364. [Google Scholar] [CrossRef]
- Caldito, N.G.; Shirani, A.; Salter, A.; Stuve, O. Adverse event profile differences between rituximab and ocrelizumab: Findings from the FDA Adverse Event Reporting Database. Mult. Scler. 2021, 27, 1066–1076. [Google Scholar] [CrossRef]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data mining of the public version of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2013, 10, 796–803. [Google Scholar] [CrossRef]
- van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef]
- Costantino, S.; Paneni, F.; Cosentino, F. Ageing, metabolism and cardiovascular disease. J. Physiol. 2016, 594, 2061–2073. [Google Scholar] [CrossRef]
- Li, Y.; Jimeno Yepes, A.; Xiao, C. Combining Social Media and FDA Adverse Event Reporting System to Detect Adverse Drug Reactions. Drug Saf. 2020, 43, 893–903. [Google Scholar] [CrossRef]
- Hair, P.I.; McCormack, P.L.; Keating, G.M. Febuxostat. Drugs 2008, 68, 1865–1874. [Google Scholar] [CrossRef]
- Chen, R.; Xu, P.; Song, P.; Wang, M.; He, J. China has faster pace than Japan in population aging in next 25 years. Biosci. Trends 2019, 13, 287–291. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully Automated Echocardiogram Interpretation in Clinical Practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [CrossRef]
- Borghi, C.; Agabiti-Rosei, E.; Johnson, R.J.; Kielstein, J.T.; Lurbe, E.; Mancia, G.; Redon, J.; Stack, A.G.; Tsioufis, K.P. Hyperuricaemia and gout in cardiovascular, metabolic and kidney disease. Eur. J. Intern. Med. 2020, 80, 1–11. [Google Scholar] [CrossRef]
- Woodward, M. Cardiovascular Disease and the Female Disadvantage. Int. J. Environ. Res. Public. Health 2019, 16, 1165. [Google Scholar] [CrossRef]
- Schjerning, A.M.; McGettigan, P.; Gislason, G. Cardiovascular effects and safety of (non-aspirin) NSAIDs. Nat. Rev. Cardiol. 2020, 17, 574–584. [Google Scholar] [CrossRef]
- Antman, E.M.; Bennett, J.S.; Daugherty, A.; Furberg, C.; Roberts, H.; Taubert, K.A.; American Heart, A. Use of nonsteroidal antiinflammatory drugs: An update for clinicians: A scientific statement from the American Heart Association. Circulation 2007, 115, 1634–1642. [Google Scholar] [CrossRef]
- Antman, E.M.; DeMets, D.; Loscalzo, J. Cyclooxygenase inhibition and cardiovascular risk. Circulation 2005, 112, 759–770. [Google Scholar] [CrossRef]
- Kearney, P.M.; Baigent, C.; Godwin, J.; Halls, H.; Emberson, J.R.; Patrono, C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ 2006, 332, 1302–1308. [Google Scholar] [CrossRef]
- Bally, M.; Dendukuri, N.; Rich, B.; Nadeau, L.; Helin-Salmivaara, A.; Garbe, E.; Brophy, J.M. Risk of acute myocardial infarction with NSAIDs in real world use: Bayesian meta-analysis of individual patient data. BMJ 2017, 357, j1909. [Google Scholar] [CrossRef]
- Schmidt, M.; Christiansen, C.F.; Mehnert, F.; Rothman, K.J.; Sorensen, H.T. Non-steroidal anti-inflammatory drug use and risk of atrial fibrillation or flutter: Population based case-control study. BMJ 2011, 343, d3450. [Google Scholar] [CrossRef]
- Edwards, B.J.; Bunta, A.D.; Lane, J.; Odvina, C.; Rao, D.S.; Raisch, D.W.; McKoy, J.M.; Omar, I.; Belknap, S.M.; Garg, V.; et al. Bisphosphonates and nonhealing femoral fractures: Analysis of the FDA Adverse Event Reporting System (FAERS) and international safety efforts: A systematic review from the Research on Adverse Drug Events And Reports (RADAR) project. J. Bone Jt. Surg. Am. 2013, 95, 297–307. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Febuxostat | Allopurinol | |
|---|---|---|
| Total number of reports | 2939 | 25,219 |
| Number of reports available | 2601 | 24,214 |
| Sex | ||
| Male | 1601 (61.55) | 15,223 (62.87) |
| Female | 821 (31.56) | 7915 (32.69) |
| Unknow | 179 (6.88) | 1076 (4.44) |
| Age | ||
| <65 | 641 (24.64) | 6500 (26.84) |
| ≥65 | 1528 (58.75) | 13,836 (57.14) |
| Unknow | 432 (16.61) | 3878 (16.02) |
| Reporter | ||
| Physician | 1265 (48.64) | 8691 (35.89) |
| Consumer | 537 (20.65) | 5857 (24.19) |
| Other health-professional | 461 (17.72) | 5536 (22.86) |
| Pharmacist | 202 (7.77) | 2163 (8.93) |
| Lawyer | 8 (0.31) | 266 (1.10) |
| Unknow | 128 (4.92) | 1701 (7.02) |
| Country | ||
| Japan | 1010 (38.83) | 1879 (7.76) |
| United Sates | 879 (33.79) | 10,366 (42.81) |
| France | 206 (7.92) | 1354 (5.59) |
| Germany | 152 (5.84) | 1991 (8.22) |
| United Kingdom | 46 (1.77) | 1566 (6.47) |
| Canada | 27 (1.04) | 643 (2.66) |
| China | 19 (0.73) | 78 (0.32) |
| Other countries | 208 (8.00) | 4559 (18.83) |
| Unknow | 54 (2.08) | 1778 (7.34) |
| PT | N (%) | PRR | χ2 | ROR | ROR 95% CI |
|---|---|---|---|---|---|
| Total number of reports = 2706 | |||||
| Edema peripheral | 451 (14.38) | 2.21 | 303.33 | 2.25 | 2.05 |
| Cardiac failure | 389 (9.57) | 6.42 | 1774.31 | 6.57 | 5.94 |
| Atrial fibrillation | 221 (8.17) | 3.04 | 302.45 | 3.07 | 2.69 |
| Cardiac failure congestive | 220 (8.13) | 2.60 | 216.62 | 2.62 | 2.29 |
| Edema | 119 (7.10) | 2.80 | 138.05 | 2.82 | 2.35 |
| Blood creatine phosphokinase increased | 99 (4.40) | 3.65 | 189.55 | 3.66 | 3.01 |
| Arrhythmia | 95 (3.66) | 2.39 | 76.79 | 2.40 | 1.96 |
| Angina pectoris | 67 (3.51) | 2.60 | 65.99 | 2.61 | 2.05 |
| Ascites | 67 (2.47) | 2.86 | 80.85 | 2.87 | 2.26 |
| Cardiac failure acute | 67 (2.47) | 15.62 | 899.30 | 15.69 | 12.31 |
| Acute myocardial infarction | 61 (2.25) | 2.21 | 40.53 | 2.22 | 1.72 |
| Cardiac failure chronic | 55 (2.03) | 23.21 | 1135.24 | 23.29 | 17.80 |
| Multiple organ dysfunction syndrome | 50 (1.84) | 3.85 | 105.01 | 3.86 | 2.92 |
| Orthostatic hypotension | 45 (1.66) | 3.40 | 76.04 | 3.41 | 2.54 |
| Acute coronary syndrome | 42 (1.55) | 5.48 | 152.90 | 5.49 | 4.05 |
| Pulmonary congestion | 41 (1.51) | 3.97 | 90.71 | 3.98 | 2.93 |
| Sudden death | 38 (1.40) | 3.74 | 76.07 | 3.75 | 2.73 |
| Ventricular tachycardia | 37 (1.37) | 2.74 | 40.84 | 2.75 | 1.99 |
| Right ventricular failure | 35 (1.29) | 5.39 | 124.30 | 5.40 | 3.87 |
| Troponin increased | 32 (1.18) | 6.84 | 158.36 | 6.86 | 4.84 |
| Stress cardiomyopathy | 29 (1.07) | 8.35 | 185.64 | 8.36 | 5.80 |
| Ventricular extrasystoles | 28 (1.03) | 3.06 | 38.67 | 3.06 | 2.11 |
| PT | N (%) | PRR | χ2 | ROR | ROR 95% CI |
|---|---|---|---|---|---|
| Total number of reports = 25,967 | |||||
| Peripheral swelling | 2275 (8.76) | 2.71 | 2407.17 | 2.74 | 2.63 |
| Atrial fibrillation | 2066 (7.96) | 3.86 | 4241.72 | 3.92 | 3.75 |
| Cardiac failure | 1942 (7.48) | 4.36 | 4846.20 | 4.42 | 4.22 |
| Congestive cardiomyopathy | 1542 (5.94) | 2.44 | 1291.34 | 2.46 | 2.34 |
| Syncope | 1416 (5.45) | 2.33 | 1058.34 | 2.35 | 2.23 |
| Bradycardia | 1069 (4.12) | 3.44 | 1794.50 | 3.46 | 3.26 |
| Edema | 882 (3.40) | 2.80 | 995.04 | 2.81 | 2.63 |
| Pulmonary oedema | 787 (3.03) | 2.97 | 1003.90 | 2.99 | 2.78 |
| Arrhythmia | 621 (2.39) | 2.09 | 347.13 | 2.10 | 1.94 |
| Acute myocardial infarction | 596 (2.30) | 2.92 | 731.27 | 2.93 | 2.70 |
| Coronary artery disease | 530 (2.04) | 2.16 | 324.39 | 2.17 | 1.99 |
| Blood creatine phosphokinase increased | 514 (1.98) | 2.54 | 468.89 | 2.55 | 2.33 |
| Ascites | 467 (1.80) | 2.68 | 480.08 | 2.69 | 2.45 |
| Angina pectoris | 466 (1.80) | 2.43 | 383.29 | 2.43 | 2.22 |
| Mental status changes | 434 (1.67) | 2.43 | 358.16 | 2.44 | 2.22 |
| Orthostatic hypotension | 389 (1.50) | 4.00 | 843.50 | 4.01 | 3.62 |
| Electrocardiogram QT prolonged | 387 (1.50) | 2.05 | 203.68 | 2.05 | 1.85 |
| Cardiomegaly | 380 (1.46) | 4.27 | 914.22 | 4.28 | 3.86 |
| Ventricular tachycardia | 353 (1.35) | 3.55 | 624.60 | 3.56 | 3.20 |
| Multiple organ dysfunction syndrome | 320 (1.23) | 3.33 | 505.32 | 3.34 | 2.98 |
| Ejection fraction decreased | 260 (1.00) | 3.28 | 400.08 | 3.29 | 2.91 |
| CVAEs | Febuxostat | Allopurinol | p-Value | OR [95% CI] |
|---|---|---|---|---|
| Total number of adverse events | 4943 | 27,310 | ||
| Total number of reports | 1927 | 6494 | ||
| Cardiac failure | 125 (2.53%) | 461 (1.69%) | <0.001 | 1.511 (1.24–1.85) |
| Ischemic heart disease | 111 (2.25%) | 284 (1.04%) | <0.001 | 2.186 (1.75–2.73) |
| Cardiomyopathy | 100 (2.02%) | 410 (1.50%) | 0.007 | 1.355 (1.09–1.69) |
| Cardiac arrhythmias | 58 (1.17%) | 334 (1.22%) | 0.77 | 0.959 (0.72–1.27) |
| Hypertension | 48 (0.97%) | 189 (0.69%) | 0.035 | 1.407 (1.02–1.93) |
| Torsade de pointes/QT prolongation | 43 (0.87%) | 277 (1.01%) | 0.346 | 0.856 (0.62–1.18) |
| Total Number of Reports (n = 1927) | Any CVAE (n = 400) | Non-CVAE (n = 1527) | p-Value | OR [95% CI] | |
|---|---|---|---|---|---|
| Age | 1371 (71.15) | 306 (76.50) | 1065 (69.74) | ||
| Mean (SD), range | 66.33 (14.34), 6–98 | 68.20 (13.26), 26–98 | 65.79 (14.59), 6–97 | 0.007 a | / |
| ≥65 | 783 (40.63) | 195 (48.75) | 588 (38.51) | 0.008 b | 1.426 (1.10–1.85) |
| <65 | 588 (30.51) | 111 (27.75) | 477 (31.24) | ||
| Sex | 1778 (92.27) | 376 (94.00) | 1402 (91.81) | ||
| Male | 1249 (64.82) | 265 (66.25) | 984 (64.44) | 0.912 b | 1.014 (0.79–1.30) |
| Female | 529 (27.45) | 111 (27.75) | 418 (27.37) | ||
| Dose (mg) | 1197 (62.12) | 260 (65.00) | 937 (61.36) | ||
| ≤80 (Recommended) | 1170 (60.72) | 254 (63.50) | 916 (59.99) | 0.949 b | 0.971 (0.39–2.43) |
| >80 (Overdose) | 27 (1.40) | 6 (1.50) | 21 (1.38) |
| Total Number of Reports (n = 6494) | Any CVAE (n = 1453) | Non-CVAE (n = 5041) | p-Value | OR (95% CI) | |
|---|---|---|---|---|---|
| Age | 5631 (86.71) | 1285 (88.44) | 4346 (86.22) | ||
| Mean (SD), range | 68.47 (12.54), 13–105 | 68.16 (11.61), 22–96 | 68.57 (12.80), 13–105 | 0.065 a | / |
| ≥65 | 3705 (57.05) | 819 (56.37) | 2886 (57.25) | 0.076 b | 0.889 (0.78–1.01) |
| <65 | 1926 (29.66) | 466 (32.07) | 1460 (28.96) | ||
| Sex | 6101 (93.94) | 1393 (95.87) | 4708 (93.40) | ||
| Male | 4285 (65.98) | 999 (68.75) | 3286 (65.19) | 0.169 b | 1.097 (0.96–1.25) |
| Female | 1816 (27.96) | 394 (27.12) | 1422 (28.21) | ||
| Dose (mg) | 3503 (53.94) | 758 (52.17) | 2745 (54.45) | ||
| ≤300 (Recommended) | 3439 (52.96) | 750 (51.62) | 2689 (53.34) | 0.073 b | 0.512 (0.24–1.08) |
| >300 (overdose) | 64 (0.99) | 8 (0.55) | 56 (1.11) |
| Total Number of Reports | Any CVAE | Non-CVAE | p-Value | OR [95% CI] | |
|---|---|---|---|---|---|
| Concomitant drugs | 166 | 41 | 125 | ||
| Propionic acid derivatives | 91 (54.82) | 21 (51.22) | 70 (56.00) | 0.576 | 1.153 (0.70–1.90) |
| Naproxen | 48 (28.92) | 14 (34.14) | 34 (18.40) | 0.146 | 1.593 (0.85–3.00) |
| Ibuprofen | 36 (21.69) | 7 (17.07) | 29 (23.20) | 0.845 | 0.920 (0.40–2.12) |
| Acetic acid Derivatives | 46 (27.71) | 15 (36.59) | 31 (24.80) | 0.045 | 1.880 (1.01–3.52) |
| Selective COX-2 inhibitor | 29 (17.47) | 5 (12.20) | 24 (19.20) | 0.638 | 0.793 (0.30–2.09) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.; Wu, B.; Gou, L.; Fang, Z.; Xu, T.; Zhang, T.; Li, Y. Cardiovascular Safety Evaluation of Febuxostat and Allopurinol: Findings from the FDA Adverse Event Reporting System. J. Clin. Med. 2023, 12, 6089. https://doi.org/10.3390/jcm12186089
Bai Y, Wu B, Gou L, Fang Z, Xu T, Zhang T, Li Y. Cardiovascular Safety Evaluation of Febuxostat and Allopurinol: Findings from the FDA Adverse Event Reporting System. Journal of Clinical Medicine. 2023; 12(18):6089. https://doi.org/10.3390/jcm12186089
Chicago/Turabian StyleBai, Yang, Bin Wu, Liangwen Gou, Zhenwei Fang, Ting Xu, Tiejun Zhang, and Yuwen Li. 2023. "Cardiovascular Safety Evaluation of Febuxostat and Allopurinol: Findings from the FDA Adverse Event Reporting System" Journal of Clinical Medicine 12, no. 18: 6089. https://doi.org/10.3390/jcm12186089