
The Challenging Differentiation of Psoriatic Arthritis from Other Arthropathies and Nonspecific Arthralgias in Patients with Psoriasis: Results of a Cross-Sectional Rheumatologic Assessment of a Large Dermatologic Cohort
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Outcome Definitions and Data Collection
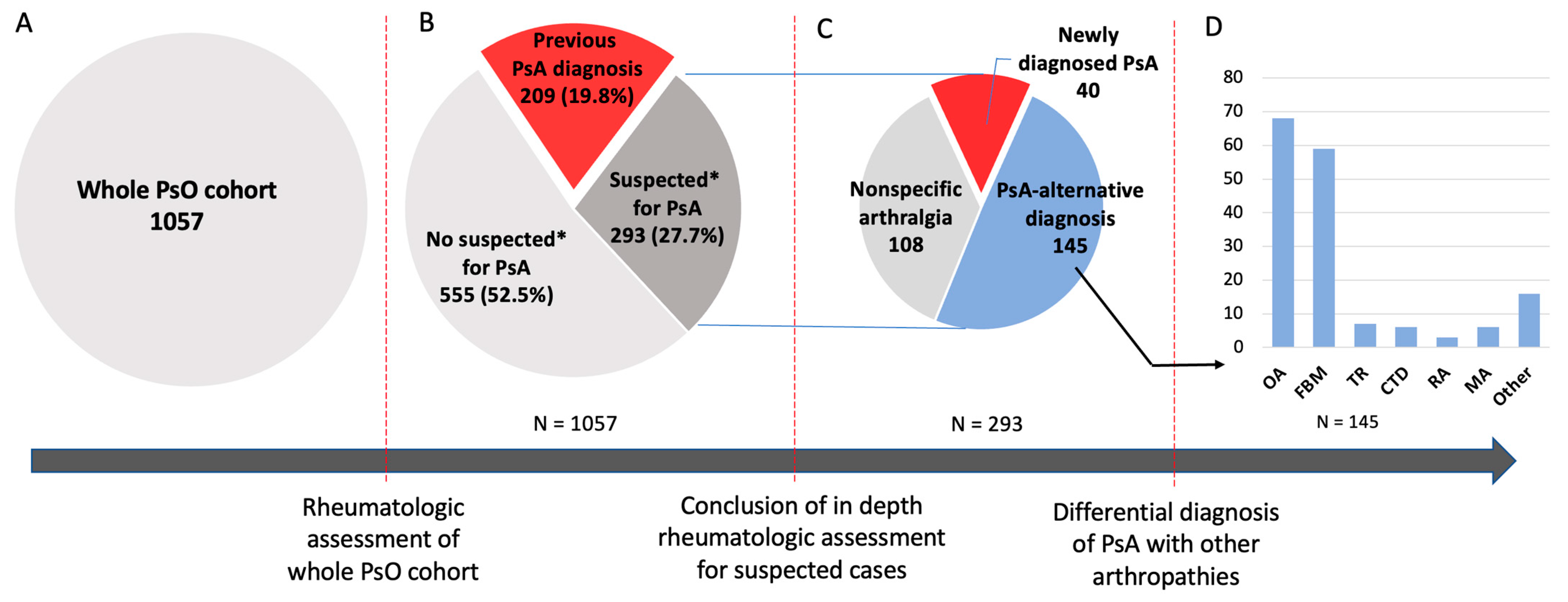
- Previous diagnosis of PsA: Patients with a pre-existing diagnosis of PsA. The previous diagnoses were retrospectively re-evaluated and then confirmed if they were formally made by a rheumatologist and fulfilled the classification criteria for psoriatic arthritis (CASPAR), which were developed and validated for clinical research but are frequently used in clinical practice to guide the clinician in the diagnosis process [19]. In particular, the following clinical criteria were retrospectively evaluated: occurrence of inflammatory articular manifestations, current PsO, personal or family history of PsO, dactylitis, juxta-articular new bone formation in hands or feet X-ray, negative rheumatoid factor, and psoriatic nail dystrophy [19].
- Suspected PsA: Patients without a pre-existing diagnosis of PsA but with suspected PsA based on the rheumatologist’s judgment (according to the presence of manifestations considered as potentially attributable to PsA) and/or an Early Psoriatic Arthritis Screening Questionnaire (EARP) score ≥ 3 [20]. The EARP is a simple self-administered questionnaire consisting of 10 questions that investigate signs or symptoms that are potentially attributable to PsA (presence = 1, absent = 0). A total score ≥ 3 was validated to identify suspected PsA cases [20]. Following the in-depth rheumatologic assessment, the suspected PsA cases were then classified as follows:
- o
- New PsA diagnosis: a new diagnosis of PsA made according to the CASPAR criteria after the rheumatologic assessment.
- o
- PsA-alternative disease: Any other diagnosis explaining the recorded MSK symptoms. When available, the other rheumatologic diseases (e.g., fibromyalgia, connective tissue diseases, rheumatoid arthritis, knee osteoarthritis, and gout) were diagnosed according to the currently used and validated diagnostic/classification criteria [21,22,23,24,25,26,27,28,29].
- o
- Nonspecific arthralgia: arthralgia not explained by PsA [21] or other concomitant diseases.
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Suspected PsA
3.2.1. New PsA Diagnosis
3.2.2. PsA-Alternative Diagnosis
3.2.3. Nonspecific Arthralgia
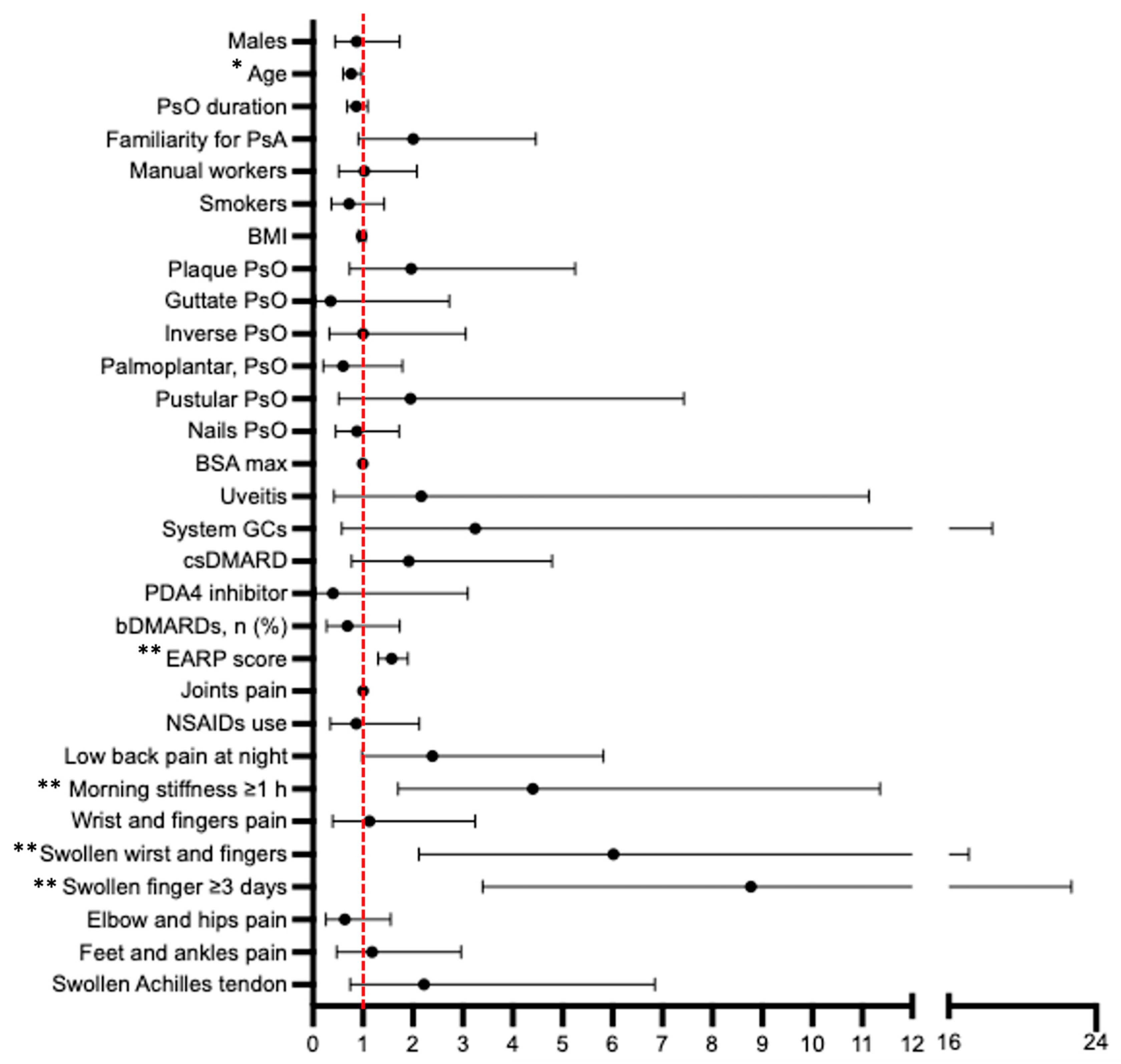
3.3. Factors Differentiating PsA from Nonconfirmed PsA Suspected Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FitzGerald, O.; Ogdie, A.; Chandran, V.; Coates, L.C.; Kavanaugh, A.; Tillett, W.; Leung, Y.Y.; de Wit, M.; Scher, J.U.; Mease, P.J. Psoriatic arthritis. Nat. Rev. Dis. Primer 2021, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Siannis, F. Clinical and radiological damage in psoriatic arthritis. Ann. Rheum. Dis. 2006, 65, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Helliwell, P.; Ritchlin, C.T. Psoriatic Arthritis and Burden of Disease: Patient Perspectives from the Population-Based Multinational Assessment of Psoriasis and Psoriatic Arthritis (MAPP) Survey. Rheumatol. Ther. 2016, 3, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Wervers, K.; Luime, J.J.; Tchetverikov, I.; Gerards, A.H.; Kok, M.R.; Appels, C.W.Y.; van der Graaff, W.L.; van Groenendael, J.H.L.M.; Korswagen, L.-A.; Dieren, J.J.V.; et al. Influence of Disease Manifestations on Health-related Quality of Life in Early Psoriatic Arthritis. J. Rheumatol. 2018, 45, 1526–1531. [Google Scholar] [CrossRef] [PubMed]
- Kane, D.; Stafford, L.; Bresnihan, B.; FitzGerald, O. A prospective, clinical and radiological study of early psoriatic arthritis: An early synovitis clinic experience. Rheumatol. Oxf. Engl. 2003, 42, 1460–1468. [Google Scholar] [CrossRef]
- Haroon, M.; Gallagher, P.; FitzGerald, O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann. Rheum. Dis. 2015, 74, 1045–1050. [Google Scholar] [CrossRef]
- Mease, P.; Goffe, B.S. Diagnosis and treatment of psoriatic arthritis. J. Am. Acad. Dermatol. 2005, 52, 1–19. [Google Scholar] [CrossRef]
- Gratacós, J.; Behrens, F.; Coates, L.C.; Lubrano, E.; Thaçi, D.; Bundy, C.; de la Torre-Aboki, J.; Luelmo, J.; Voorneveld, H.; Richette, P. A 12-point recommendation framework to support advancement of the multidisciplinary care of psoriatic arthritis: A call to action. Jt. Bone Spine 2021, 88, 105175. [Google Scholar] [CrossRef]
- Rida, M.A.; Chandran, V. Challenges in the clinical diagnosis of psoriatic arthritis. Clin. Immunol. 2020, 214, 108390. [Google Scholar] [CrossRef]
- Eder, L.; Polachek, A.; Rosen, C.F.; Chandran, V.; Cook, R.; Gladman, D.D. The Development of Psoriatic Arthritis in Patients With Psoriasis Is Preceded by a Period of Nonspecific Musculoskeletal Symptoms: A Prospective Cohort Study. Arthritis Rheumatol. 2017, 69, 622–629. [Google Scholar] [CrossRef]
- Ritchlin, C.T.; Colbert, R.A.; Gladman, D.D. Psoriatic Arthritis. N. Engl. J. Med. 2017, 376, 957–970. [Google Scholar] [CrossRef]
- Scher, J.U.; Ogdie, A.; Merola, J.F.; Ritchlin, C. Preventing psoriatic arthritis: Focusing on patients with psoriasis at increased risk of transition. Nat. Rev. Rheumatol. 2019, 15, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Landewé, R.B.M. Overdiagnosis and overtreatment in rheumatology: A little caution is in order. Ann. Rheum. Dis. 2018, 77, 1394–1396. [Google Scholar] [CrossRef] [PubMed]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Luchetti, M.M.; Benfaremo, D.; Campanati, A.; Molinelli, E.; Ciferri, M.; Cataldi, S.; Capeci, W.; Di Carlo, M.; Offidani, A.M.; Salaffi, F.; et al. Clinical outcomes and feasibility of the multidisciplinary management of patients with psoriatic arthritis: Two-year clinical experience of a dermo-rheumatologic clinic. Clin. Rheumatol. 2018, 37, 2741–2749. [Google Scholar] [CrossRef]
- Theodorakopoulou, E.; Dalamaga, M.; Katsimbri, P.; Boumpas, D.T.; Papadavid, E. How does the joint dermatology–rheumatology clinic benefit both patients and dermatologists? Dermatol. Ther. 2020, 33, e13283. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; Soriano, E.R.; Corp, N.; Bertheussen, H.; Callis Duffin, K.; Campanholo, C.B.; Chau, J.; Eder, L.; Fernández-Ávila, D.G.; FitzGerald, O.; et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA): Updated treatment recommendations for psoriatic arthritis 2021. Nat. Rev. Rheumatol. 2022, 18, 465–479. [Google Scholar] [CrossRef]
- Mandl, P.; Navarro-Compán, V.; Terslev, L.; Aegerter, P.; van der Heijde, D.; D’Agostino, M.A.; Baraliakos, X.; Pedersen, S.J.; Jurik, A.G.; Naredo, E.; et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann. Rheum. Dis. 2015, 74, 1327–1339. [Google Scholar] [CrossRef]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H. CASPAR Study Group Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef]
- Tinazzi, I.; Adami, S.; Zanolin, E.M.; Caimmi, C.; Confente, S.; Girolomoni, G.; Gisondi, P.; Biasi, D.; McGonagle, D. The early psoriatic arthritis screening questionnaire: A simple and fast method for the identification of arthritis in patients with psoriasis. Rheumatology 2012, 51, 2058–2063. [Google Scholar] [CrossRef]
- Neogi, T.; Jansen, T.L.T.A.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, B.; Cimmino, M.A.; Maradit-Kremers, H.; Schmidt, W.A.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 provisional classification criteria for polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann. Rheum. Dis. 2012, 71, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- Altman, R.; Alarcón, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Feldman, D.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991, 34, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Altman, R.; Alarcon, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Gray, R.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum. 1990, 33, 1601–1610. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Peat, G.; Bierma-Zeinstra, M.A.; Arden, N.K.; Bresnihan, B.; Herrero-Beaumont, G.; Kirschner, S.; Leeb, B.F.; Lohmander, L.S.; et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 483–489. [Google Scholar] [CrossRef]
- Gudu, T.; Jadon, D.R. Multidisciplinary working in the management of axial and peripheral spondyloarthritis. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20975888. [Google Scholar] [CrossRef]
- Villani, A.P.; Rouzaud, M.; Sevrain, M.; Barnetche, T.; Paul, C.; Richard, M.-A.; Beylot-Barry, M.; Misery, L.; Joly, P.; Le Maitre, M.; et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: Systematic review and meta-analysis. J. Am. Acad. Dermatol. 2015, 73, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Nguyen, T.U.; Poon, K.-Y.T.; Herrinton, L.J. The association of psoriasis with autoimmune diseases. J. Am. Acad. Dermatol. 2012, 67, 924–930. [Google Scholar] [CrossRef]
- Cooper, G.S.; Stroehla, B.C. The epidemiology of autoimmune diseases. Autoimmun. Rev. 2003, 2, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.-P. Osteoarthritis. Nat. Rev. Dis. Primer 2016, 2, 16072. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Weiss, P. The Epidemiology Psoriatic Arthritis. Rheum. Dis. Clin. North Am. 2015, 41, 545–568. [Google Scholar] [CrossRef]
- Marchesoni, A.; Macchioni, P.; Gasparini, S.; Perricone, C.; Perrotta, F.M.; Grembiale, R.D.; Silvagni, E.; Ramonda, R.; Costa, L.; Zabotti, A.; et al. Use of Ultrasonography to Discriminate Psoriatic Arthritis from Fibromyalgia: A Post-Hoc Analysis of the ULISSE Study. J. Clin. Med. 2021, 11, 180. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Perez-Chada, L.M.; Haberman, R.H.; Chandran, V.; Rosen, C.F.; Ritchlin, C.; Eder, L.; Mease, P.; Reddy, S.; Ogdie, A.; Merola, J.F.; et al. Consensus terminology for preclinical phases of psoriatic arthritis for use in research studies: Results from a Delphi consensus study. Nat. Rev. Rheumatol. 2021, 17, 238–243. [Google Scholar] [CrossRef]
- Savage, L.; Tinazzi, I.; Zabotti, A.; Laws, P.M.; Wittmann, M.; McGonagle, D. Defining Pre-Clinical Psoriatic Arthritis in an Integrated Dermato-Rheumatology Environment. J. Clin. Med. 2020, 9, 3262. [Google Scholar] [CrossRef]
- Zabotti, A.; McGonagle, D.G.; Giovannini, I.; Errichetti, E.; Zuliani, F.; Zanetti, A.; Tinazzi, I.; Lucia, O.D.; Batticciotto, A.; Idolazzi, L.; et al. Transition phase towards psoriatic arthritis: Clinical and ultrasonographic characterisation of psoriatic arthralgia. RMD Open 2019, 5, e001067. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Males, n (%) | 585 (55.3) |
| Age, mean (SD), yrs | 55.3 (14.7) |
| Age at the PsO onset, mean (SD), yrs | 35.4 (18.2) |
| PsO disease duration, mean (SD), yrs | 20.1 (14.8) |
| Familiarity for PsA, n (%) | 138 (13.1) |
| Manual workers, n (%) | 466 (48.0) |
| Smokers, n (%) | 670 (63.9) |
| BMI, mean (SD) kg/m2 | 26.5 (5.0) |
| PsO skin pattern | |
| Plaque, n (%) | 897 (84.9%) |
| Guttate, n (%) | 53 (5.0%) |
| Inverse, n (%) | 89 (8.4%) |
| Palmoplantar, n (%) | 132 (12.5%) |
| Pustular, n (%) | 32 (3.0%) |
| Erythroderma, n (%) | 22 (2.1%) |
| Nails PsO, n (%) | 504 (47.7%) |
| BSA max, mean (SD) | 35.4 (18.3) |
| SpA-related comorbidities | |
| Uveitis, n (%) | 16 (1.5%) |
| IBD, n (%) | 11 (1.0%) |
| Ongoing treatment | |
| Topic, n (%) | 753 (71.2%) |
| Phototherapy, n (%) | 10 (0.9%) |
| Systemic glucocorticoids, n (%) | 27 (2.6%) |
| cs-DMARDs, n (%) | 176 (16.7%) |
| Apremilast, n (%) | 58 (5.5%) |
| b-DMARDs, n (%) | 380 (36.0%) |
| Total EARP score, mean (SD) | 2.5 (2.7) |
| Individual EARP items * | |
| Joints pains, n (%) | 342 (58.8) |
| NSAIDs used twice last 3 months, n (%) | 104 (17.9) |
| Low back pain at night, n (%) | 83 (14.3) |
| Morning stiffness ≥ 1 h, n (%) | 100 (17.2) |
| Wrist and finger pain, n (%) | 219 (37.6) |
| Swollen joints, n (%) | 127 (21.9%) |
| Swollen wrist and fingers ≥ 3 days, n (%) | 69 (11.9) |
| Elbow and hip pain, n (%) | 123 (21.1) |
| Feet and ankle pain, n (%) | 163 (28.0) |
| Swollen Achilles tendon, n (%) | 40 (6.9) |
| Previous PsA diagnosis, n (%) | 209 (34.6%) |
| New PsA Diagnosis (n = 40) | Other Diagnosis (n = 145) | Unspecific Arthralgia (n = 108) | |
|---|---|---|---|
| Demographics | |||
| Males, n (%) | 15 (37.5) | 53 (36.6) | 50 (46.3) |
| Age, mean (SD), yrs | 51.9 (11.6) | 58.1 (14.1) | 55.4 (13.6) |
| Age at PsO onset, mean (SD), yrs | 34.8 (19.0) | 38.1 (18.7) | 35.2 (17.9) |
| PsO duration, mean (SD), yrs | 17.1 (13.6) | 20.2 (15.5) | 20.3 (15.5) |
| Familiarity for PsA, n (%) | 10 (25.0) | 21 (14.5) | 15 (13.9) |
| Manual workers, n (%) | 21 (56.7) | 78 (53.8) | 53 (49.1) |
| Smokers, n (%) | 23 (57.5) | 89 (61.4) | 36 (33.3) |
| BMI, mean (SD) kg/m2 | 26.1 (4.0) | 26.9 (4.9) | 26.3 (5.3) |
| PsO skin pattern | |||
| Plaque, n (%) | 35 (87.5) | 111 (76.6) | 85 (78.7) |
| Guttate, n (%) | 1 (2.5) | 14 (9.7) | 3 (2.8) |
| Inverse, n (%) | 4 (10.0) | 16 (11.0) | 9 (8.3) |
| Palmoplantar, n (%) | 4 (10.0) | 22 (15.2) | 17 (15.7) |
| Pustular, n (%) | 4 (10.0) | 4 (2.8) | 6 (5.6) |
| Erythroderma, n (%) | 0 | 3 (2.1) | 3 (2.8) |
| Nails PsO, n (%) | 19 (47.5) | 64 (44.1) | 63 (58.3) |
| BSA max, mean (SD) | 16.2 (14.2) | 18.6 (20.0) | 18.9 (21.7) |
| SpA-related comorbidities | |||
| Uveitis, n (%) | 2 (5.0%) | 5 (3.4) | 1 (0.9) |
| IBD, n (%) | 0 | 2 (1.4) | 1 (0.9) |
| Ongoing treatment | |||
| Topic, n (%) | 35 (87.5) | 117 (80.7) | 84 (77.8) |
| Phototherapy, n (%) | 0 | 2 (1.4) | 2 (1.9) |
| Systemic glucocorticoids, n (%) | 2 (5.0) | 1 (0.7) | 3 (2.8) |
| cs-DMARD, n (%) | 7 (17.5) | 12 (8.3) | 13 (12.0) |
| PDA4 inhibitor, n (%) | 1 (2.5) | 11 (7.6) | 4 (3.7) |
| b-DMARDs, n (%) | 6 (15.0) | 28 (19.3) | 23 (21) |
| Total EARP, mean (SD) score | 6.2 (1.7) | 4.9 (1.7) | 4.4 (1.6) |
| Individual EARP items * | |||
| Joints pain, n (%) | 23 (100) | 84 (100) | 66 (95.7) |
| NSAIDs used twice last 3 months, n (%) | 8 (34.8) | 39 (4.4) | 20 (29.0) |
| Low back pain at night, n (%) | 11 (47.8) | 27 (32.1) | 16 (23.2) |
| Morning stiffness ≥ 1 h, n (%) | 16 (69.6) | 32 (38.1) | 21 (30.4) |
| Wrist and finger pain, n (%) | 18 (78.3) | 67 (79.8) | 51 (73.9) |
| Swollen joints, n (%) | 18 (78.3) | 38 (45.2) | 20 (29.0) |
| Swollen wrist/fingers ≥ 3 days, n (%) | 13 (56.5) | 13 (15.5) | 7 (10.1) |
| Elbow and hip pain, n (%) | 9 (39.1) | 41 (48.8) | 37 (53.6) |
| Feet and ankle pain, n (%) | 15 (65.2) | 55 (66.5) | 40 (58.0) |
| Swollen Achilles tendon, n (%) | 5 (21.7) | 9 (10.7) | 8 (11.6) |
| Therapy modification after PsA diagnosis, n (%) | 34 (85.9) | - | - |
| Introduction cs-DMARD, n (%) | 21 (55.2) | - | - |
| Introduction b-DMARD, n (%) | 13 (32.5) | - | - |
| Injection joint therapy, n (%) | 0 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Floris, A.; Mugheddu, C.; Sichi, L.; Dessì, M.; Anedda, J.; Frau, A.; Pau, A.; Lari, S.A.; Sorgia, J.; Li Volsi, L.; et al. The Challenging Differentiation of Psoriatic Arthritis from Other Arthropathies and Nonspecific Arthralgias in Patients with Psoriasis: Results of a Cross-Sectional Rheumatologic Assessment of a Large Dermatologic Cohort. J. Clin. Med. 2023, 12, 6090. https://doi.org/10.3390/jcm12186090
Floris A, Mugheddu C, Sichi L, Dessì M, Anedda J, Frau A, Pau A, Lari SA, Sorgia J, Li Volsi L, et al. The Challenging Differentiation of Psoriatic Arthritis from Other Arthropathies and Nonspecific Arthralgias in Patients with Psoriasis: Results of a Cross-Sectional Rheumatologic Assessment of a Large Dermatologic Cohort. Journal of Clinical Medicine. 2023; 12(18):6090. https://doi.org/10.3390/jcm12186090
Chicago/Turabian StyleFloris, Alberto, Cristina Mugheddu, Leonardo Sichi, Martina Dessì, Jasmine Anedda, Alessia Frau, Andrea Pau, Simone Aldo Lari, Jessica Sorgia, Laura Li Volsi, and et al. 2023. "The Challenging Differentiation of Psoriatic Arthritis from Other Arthropathies and Nonspecific Arthralgias in Patients with Psoriasis: Results of a Cross-Sectional Rheumatologic Assessment of a Large Dermatologic Cohort" Journal of Clinical Medicine 12, no. 18: 6090. https://doi.org/10.3390/jcm12186090