
An Alternative Treatment Option for Blauth III B Thumb Hypoplasia—Thumb Stabilization with Iliac Crest Bone Graft and Intermetacarpal Arthrodesis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
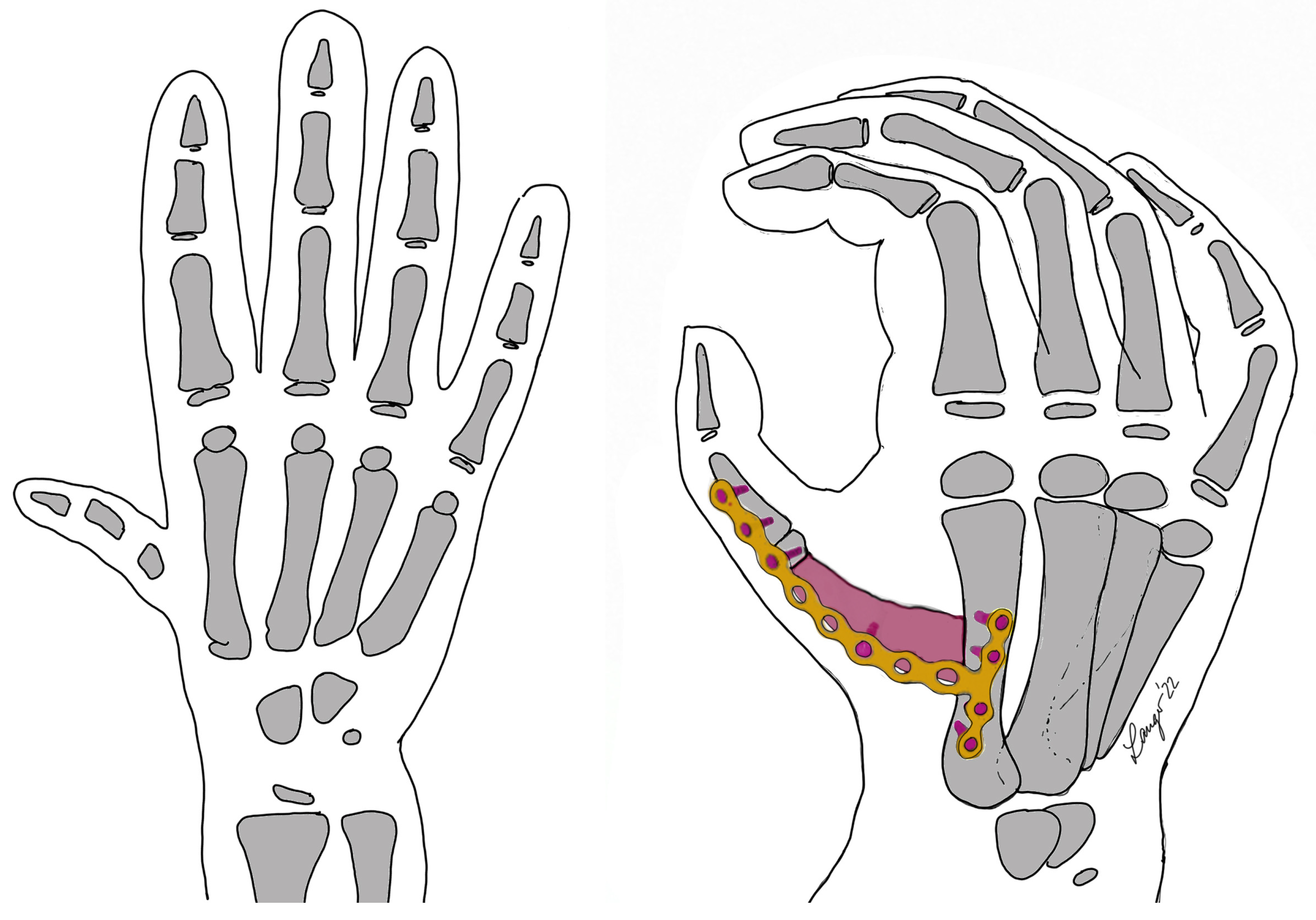
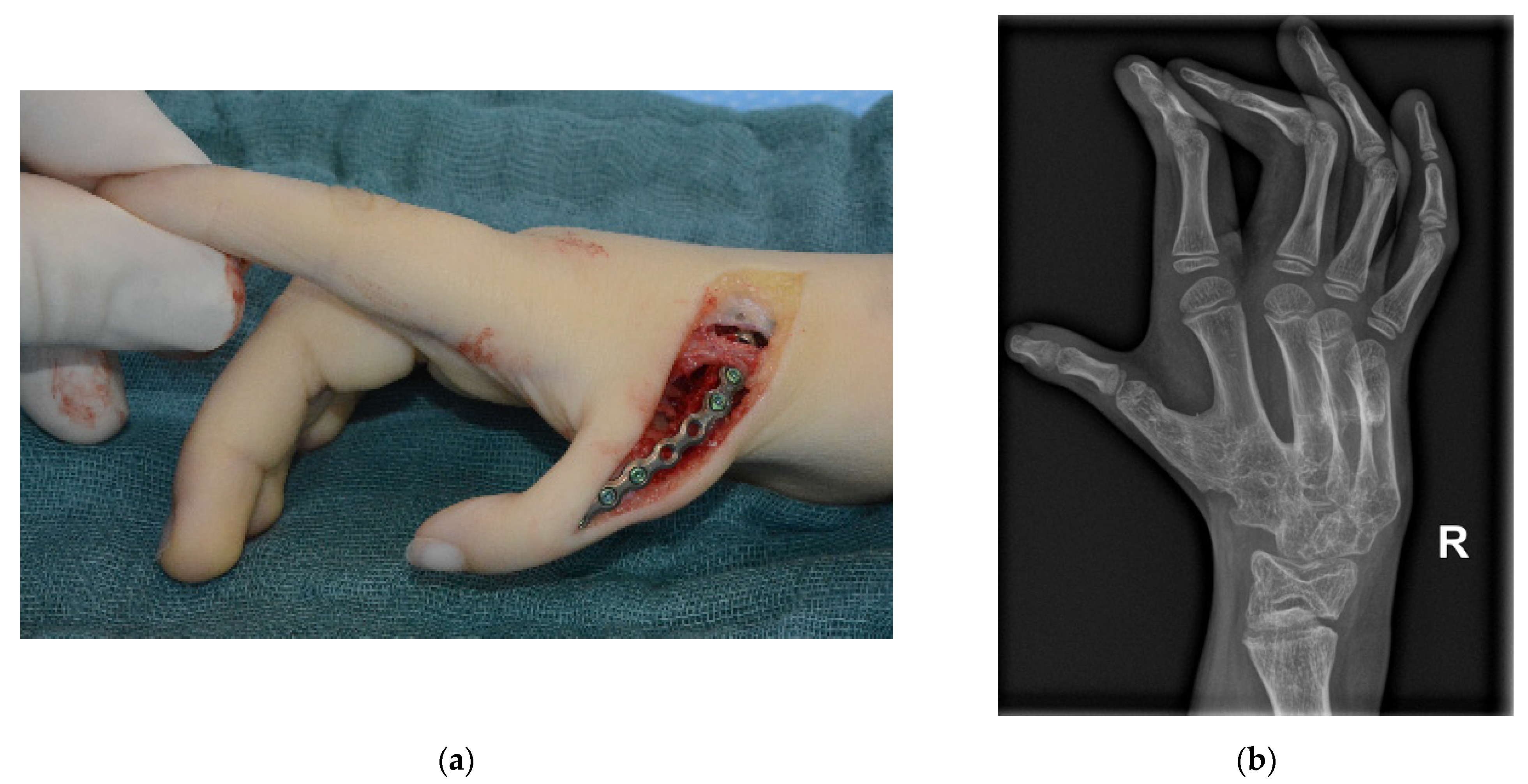
Surgical Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, S.; Michelsen-Jost, H. Anatomy and function of the thenar muscles. Hand Clin. 2012, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kozin, S.H.; Zlotolow, D.A. Common Pediatric Congenital Conditions of the Hand. Plast. Reconstr. Surg. 2015, 136, 241e–257e. [Google Scholar] [CrossRef] [PubMed]
- Carli, D.; Garagnani, L.; Lando, M.; Fairplay, T.; Bernasconi, S.; Landi, A.; Percesepe, A. VACTERL (vertebral defects, anal atresia, tracheoesophageal fistula with esophageal atresia, cardiac defects, renal and limb anomalies) association: Disease spectrum in 25 patients ascertained for their upper limb involvement. J. Pediatr. 2014, 164, 458–462.e2. [Google Scholar] [CrossRef] [PubMed]
- Buck-Gramcko, D. Congenital malformations of the hand and forearm. Chir. Main 2002, 21, 70–101. [Google Scholar] [CrossRef] [PubMed]
- Blauth, W. The hypoplastic thumb. Arch. Orthop. Unfallchir. 1967, 62, 225–246. [Google Scholar] [CrossRef] [PubMed]
- Manske, M.W. Evolutionary development of the human thumb. Hand Clin. 1992, 8, 1–8. [Google Scholar]
- Manske, P.R.; McCarroll, H.R., Jr.; James, M. Type III-A hypoplastic thumb. J. Hand Surg. 1995, 20, 246–253. [Google Scholar] [CrossRef]
- Christen, T.; Dautel, G. Type II and IIIA thumb hypoplasia reconstruction. J. Hand Surg. 2013, 38, 2009–2015. [Google Scholar] [CrossRef]
- Soldado, F.; Zlotolow, D.A.; Kozin, S.H. Thumb hypoplasia. J. Hand Surg. 2013, 38, 1435–1444. [Google Scholar] [CrossRef]
- James, M.A.; McCarroll, H.R., Jr.; Manske, P.R. Characteristics of patients with hypoplastic thumbs. J. Hand Surg. 1996, 21, 104–113. [Google Scholar] [CrossRef]
- Hellevuo, C.; Leppanen, O.V.; Kapanen, S.; Vilkki, S.K. Long-term outcomes after pollicization: A mean 11-year follow-up study. J. Hand Surg. 2020, 45, 173–180. [Google Scholar] [CrossRef] [PubMed]
- McCarroll, H.R. Congenital anomalies: A 25-year overview. J. Hand Surg. 2000, 25, 1007–1037. [Google Scholar] [CrossRef] [PubMed]
- Tonkin, M. Surgical reconstruction of congenital thumb hypoplasia. Indian J. Plast. Surg. 2011, 44, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Buck-Gramcko, D. Pollicization of the index finger. Method and results in aplasia and hypoplasia of the thumb. J. Bone Jt. Surg. 1971, 53, 1605–1617. [Google Scholar] [CrossRef]
- Tu, Y.K.; Yeh, W.L.; Sananpanich, K.; Ueng, S.W.; Chou, Y.C.; Ma, C.H.; Lee, Z.L. Microsurgical second toe-metatarsal bone transfer for reconstructing congenital radial deficiency with hypoplastic thumb. J. Reconstr. Microsurg. 2004, 20, 215–225. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Quatman-Yates, C.C.; Gupta, R.; Paterno, M.V.; Schmitt, L.C.; Quatman, C.E.; Ittenbach, R.F. Internal consistency and validity of the QuickDASH instrument for upper extremity injuries in older children. J. Pediatr. Orthop. 2013, 33, 838–842. [Google Scholar] [CrossRef]
- Percival, N.J.; Sykes, P.J.; Chandraprakasam, T. A method of assessment of pollicisation. J. Hand Surg. 1991, 16, 141–143. [Google Scholar] [CrossRef]
- Kellor, M.; Frost, J.; Silberberg, N.; Iversen, I.; Cummings, R. Hand strength and dexterity. Am. J. Occup. Ther. 1971, 25, 77–83. [Google Scholar]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef]
- Ploegmakers, J.J.; Hepping, A.M.; Geertzen, J.H.; Bulstra, S.K.; Stevens, M. Grip strength is strongly associated with height, weight and gender in childhood: A cross sectional study of 2241 children and adolescents providing reference values. J. Physiother. 2013, 59, 255–261. [Google Scholar] [CrossRef]
- Werle, S.; Goldhahn, J.; Drerup, S.; Simmen, B.R.; Sprott, H.; Herren, D.B. Age- and gender-specific normative data of grip and pinch strength in a healthy adult Swiss population. J. Hand Surg. 2009, 34, 76–84. [Google Scholar] [CrossRef]
- Kawabata, H.; Tamura, D.; Goldfarb, C.A. Treatment of Blauth Type IIIB Thumb Hypoplasia Using a Nonvascularized Toe Phalanx. J. Hand Surg. 2021, 46, 68.e1–68.e7. [Google Scholar] [CrossRef] [PubMed]
- Bachy, M.; Victoria, C.; Martinot-Lagarde, C.; Romana, C.; Vialle, R.; Fitoussi, F. Global assessment of pollicization outcomes: An analysis in 27 patients. J. Hand Surg. 2021, 46, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Kollitz, K.M.; Tomhave, W.; Van Heest, A.E.; Moran, S.L. Change in Hand Function and Dexterity with Age after Index Pollicization for Congenital Thumb Hypoplasia. Plast. Reconstr. Surg. 2018, 141, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Netscher, D.T.; Aliu, O.; Sandvall, B.K.; Staines, K.G.; Hamilton, K.L.; Salazar-Reyes, H.; Thornby, J. Functional outcomes of children with index pollicizations for thumb deficiency. J. Hand Surg. 2013, 38, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Chow, C.S.; Ho, P.C.; Tse, W.L.; Hung, L.K. Reconstruction of hypoplastic thumb using hemi-longitudinal metatarsal transfer. J. Hand Surg. 2012, 37, 738–744. [Google Scholar] [CrossRef]
- Hu, W.; Gasnier, P.; Le Nen, D.; Kerfant, N.; Boloorchi, A. Description of an original conservative method for the surgical management of the Blauth IIIb thumb hypoplasia: “relative lengthening—Thumb stabilization”. Ann. Chir. Plast. Esthet. 2012, 57, 342–349. [Google Scholar] [CrossRef]
- Vekris, M.D.; Beris, A.E.; Lykissas, M.G.; Soucacos, P.N. Index finger pollicization in the treatment of congenitally deficient thumb. Ann. Plast. Surg. 2011, 66, 137–142. [Google Scholar] [CrossRef]
- Staines, K.G.; Majzoub, R.; Thornby, J.; Netscher, D.T. Functional outcome for children with thumb aplasia undergoing pollicization. Plast. Reconstr. Surg. 2005, 116, 1314–1323, discussion 1324–1315. [Google Scholar] [CrossRef]
- Foucher, G.; Medina, J.; Navarro, R. Microsurgical reconstruction of the hypoplastic thumb, type IIIB. J. Reconstr. Microsurg. 2001, 17, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.L.; Burtner, P.A.; Torres, T.A.; McMullen, C.K.; Markham, A.; Marcum, M.L.; Anderson, J.B.; Qualls, C. Measuring dexterity in children using the Nine-hole Peg Test. J. Hand Ther. 2005, 18, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Ince, B.; Dadaci, M. Thumb Reconstruction Using Transfer of the Ring Finger Without Vascular Anastomosis. J. Hand Surg. 2022, 47, 686.e1–686.e6. [Google Scholar] [CrossRef] [PubMed]
- Lahiji, F.A.; Asgari, F.; Mirzaee, F.; Zafarani, Z.; Aslani, H. Clinical and functional results of radial club hand with centralization and pollicization using the second metacarpus: A clinical case series. Int. J. Surg. Case Rep. 2019, 61, 285–290. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Patients (n = 9) |
| Sex | 4 female, 5 male |
| Median age at primary surgery | 3 years and 8 months |
| Median age at follow-up examination | 11 years and 11 months |
| Median follow-up time | 7 years and 4 months |
| Patients with complications | 1/9 (plate failure, but bony consolidation) |
| Age at Surgery | Age at Follow Up | Sex | Comorbidity | Kapandji Score | Force [kg] (Norm Value) | Percival Score | Q-DASH®® Score | 9-Hole Peg | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 yr. 9 mos. | 9 yr. 1 mo. | f | Oligosyndactyly with one os metacarpale for the fourth and fifth finger and delta phalanx on the index finger, reduction defect with radiohumeral synostosis at the elbow | 5 | 5 (15.1) | 14.25 | 31.8 | 56 |
| 2 | 9 yr. 9 mos. | 13 yr. 3 mos. | f | 2 | 8 (24.5) | 8.75 | 25 | 53 | |
| 3 | 17 yr. 0 mos. | 25 yr. 10 mos. | f | Thumb hypoplasia opposite side Blauth 1 | 3 | 21 (33.6) | 8.75 | 2.27 | 17 |
| 4 | 6 yr. 4 mos. | 8 yr. 1 mo. | m | Thumb hypoplasia opposite side Blauth 1 | 1 | 8 (15.9) | 8.75 | - | 43 |
| 5 | 3 yr. 8 mos. | 18 yr. 7 mos. | m | 5 | 24 (48.3) | 11.25 | 0 | 40 | |
| 6 | 2 yr. 11 mos. | 8 yr. 7 mos. | m | Radial aplasia with radial club hand | 5 | 2 (14.6) | 12.25 | 20.4 | 44 |
| 7 | 2 yr. 6 mos. | 8 yr. 1 mos. | m | Bayne and Klug grade II radial hypoplasia | 0 | 2 (14.6) | 11.75 | 2.3 | 27 |
| 8 | 4 yr. 5 mos. | 12 yr. 4 mos. | f | Thumb hypoplasia opposite side Blauth 1 | 4 | 10 (22.3) | 12.5 | 2.3 | 26 |
| 9 | 3 yr. 2 mos. | 11 yr. 11 mos. | m | Radial aplasia with radial club hand | 3 | 4 (20.6) | 8.75 | 38.6 | 89 |
| Average | 3.1 | 9.3 | 10.77 | 15.3 | 43.9 | ||||
| Median | 3 | 8 | 11.25 | 11.4 | 43 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oeckenpöhler, S.; Langer, M.F.; Wichmann, A.; Glasbrenner, J.; Riesenbeck, O. An Alternative Treatment Option for Blauth III B Thumb Hypoplasia—Thumb Stabilization with Iliac Crest Bone Graft and Intermetacarpal Arthrodesis. J. Clin. Med. 2023, 12, 5977. https://doi.org/10.3390/jcm12185977
Oeckenpöhler S, Langer MF, Wichmann A, Glasbrenner J, Riesenbeck O. An Alternative Treatment Option for Blauth III B Thumb Hypoplasia—Thumb Stabilization with Iliac Crest Bone Graft and Intermetacarpal Arthrodesis. Journal of Clinical Medicine. 2023; 12(18):5977. https://doi.org/10.3390/jcm12185977
Chicago/Turabian StyleOeckenpöhler, Simon, Martin Franz Langer, Anna Wichmann, Johannes Glasbrenner, and Oliver Riesenbeck. 2023. "An Alternative Treatment Option for Blauth III B Thumb Hypoplasia—Thumb Stabilization with Iliac Crest Bone Graft and Intermetacarpal Arthrodesis" Journal of Clinical Medicine 12, no. 18: 5977. https://doi.org/10.3390/jcm12185977