
Comparative Analysis of Treatment Outcomes: Modified Ulnar Gutter Slab vs. Sugar Tong Slab for Distal Radioulnar Joint Instability Following Triangular Fibrocartilage Complex Repair
 ,
,
Abstract
:1. Introduction
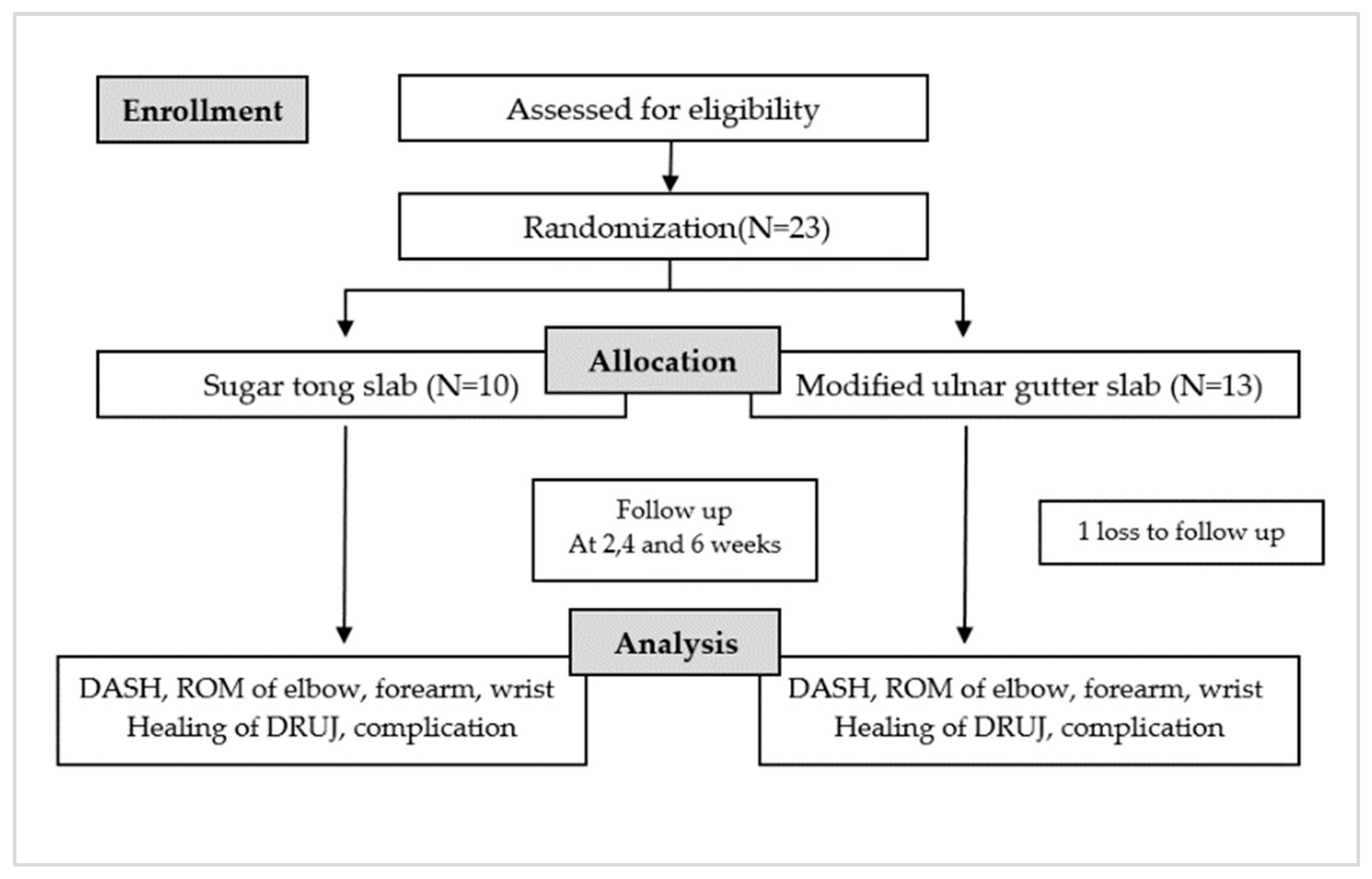
2. Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CRPS | Complex regional pain syndrome |
| DASH | Disabilities of Arm, Shoulder, and Hand |
| DRUJ | Distal radioulnar joint |
| ROM | Range of motion |
| TFCC | Triangular fibrocartilage complex |
References
- Qazi, S.; Graham, D.; Regal, S.; Tang, P.; Hammarstedt, J.E. Distal Radioulnar Joint Instability and Associated Injuries: A Literature Review. J. Hand Microsurg. 2021, 13, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.W.; Adams, B. Chronic Distal Radioulnar Joint Instability. Hand Clin. 2020, 36, 443–453. [Google Scholar] [CrossRef] [PubMed]
- May, M.M.; Lawton, J.N.; Blazar, P.E. Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J. Hand Surg. 2002, 27, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Geissler, W.B.; Fernandez, D.L.; Lamey, D.M. Distal Radioulnar Joint Injuries Associated with Fractures of the Distal Radius. Clin. Orthop. Relat. Res. 1996, 327, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.C.; Paksima, N. The distal radioulnar joint. Bull. NYU Hosp. Jt. Dis. 2009, 67, 90–96. [Google Scholar]
- Boyd, B.; Adams, J. Distal Radioulnar Joint Instability. Hand Clin. 2021, 37, 563–573. [Google Scholar] [CrossRef]
- Cole, D.W.; Elsaidi, G.A.; Kuzma, K.R.; Kuzma, G.R.; Smith, B.P.; Ruch, D.S. Distal radioulnar joint instability in distal radius fractures: The role of sigmoid notch and triangular fibrocartilage complex revisited. Injury 2006, 37, 252–258. [Google Scholar] [CrossRef]
- Huang, J.I.; Hanel, D.P. Anatomy and biomechanics of the distal radioulnar joint. Hand Clin. 2012, 28, 157–163. [Google Scholar] [CrossRef]
- Zimmerman, R.M.; Kim, J.M.; Jupiter, J.B. Arthritis of the distal radioulnar joint: From Darrach to total joint arthroplasty. J. Am. Acad. Orthop. Surg. 2012, 20, 623–632. [Google Scholar] [CrossRef]
- Faucher, G.K.; Zimmerman, R.M.; Zimmerman, N.B. Instability and Arthritis of the Distal Radioulnar Joint: A Critical Analysis Review. JBJS Rev. 2016, 4, e3. [Google Scholar] [CrossRef]
- Xiao, A.X.; Graf, A.R.; Dawes, A.; Daley, C.; Wagner, E.R.; Gottschalk, M.B. Management of Acute Distal Radioulnar Joint Instability Following a Distal Radius Fracture: A Systematic Review and Meta-Analysis. J. Hand Surg. Glob. Online 2021, 3, 133–138. [Google Scholar] [CrossRef]
- Mulford, J.S.; Axelrod, T.S. Traumatic Injuries of the Distal Radioulnar Joint. Hand Clin. 2010, 26, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Robba, V.; Fowler, A.; Karantana, A.; Grindlay, D.; Lindau, T. Open Versus Arthroscopic Repair of 1B Ulnar-Sided Triangular Fibrocartilage Complex Tears: A Systematic Review. Hand 2020, 15, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.K.; Åhlén, M.; Andernord, D. Open versus arthroscopic repair of the triangular fibrocartilage complex: A systematic review. J. Exp. Orthop. 2018, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- McCarron, L.; Bindra, R.; Coombes, B.K.; Bisset, L. Wrist and forearm range of motion commencement time following primary triangular fibrocartilage complex foveal repair surgery: A scoping review. J. Hand Ther. 2023, 36, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Feitz, R.; Teunissen, J.S.; van der Oest, M.J.W.; van der Heijden, E.P.A.; Selles, R.W.; Hovius, S.E.R.; Blomme, R.A.M.; Sluijter, B.J.R.; van der Avoort, D.J.J.C.; Kroeze, A.; et al. Factors associated with return to work after open reinsertion of the triangular fibrocartilage. Hand Surg. Rehabil. 2021, 40, 405–412. [Google Scholar] [CrossRef]
- Atzei, A.; Luchetti, R.; Garagnani, L. Classification of ulnar triangular fibrocartilage complex tears. A treatment algorithm for Palmer type IB tears. J. Hand Surg. Eur. Vol. 2017, 42, 405–414. [Google Scholar] [CrossRef]
- Atzei, A.; Luchetti, R.; Braidotti, F. Arthroscopic foveal repair of the triangular fibrocartilage complex. J. Wrist Surg. 2015, 4, 22–30. [Google Scholar]
- Kanjanapiboonwong, A.; Pongathimoke, P. Immobilization of Forearm Rotation: Sugar Tong Splint Versus Volar-dorsal short Arm Splint. Vajira Med. J. J. Urban Med. 2018, 62, 305–314. [Google Scholar]
- Vezeridis, P.S.; Yoshioka, H.; Han, R.; Blazar, P. Ulnar-sided wrist pain. Part I: Anatomy and physical examination. Skelet. Radiol. 2010, 39, 733–745. [Google Scholar] [CrossRef]
- Nakamura, R.; Horii, E.; Imaeda, T.; Tsunoda, K.; Nakao, E. Distal radioulnar joint subluxation and dislocation diagnosed by standard roentgenography. Skelet. Radiol. 1995, 24, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.; Siwiec, R.M. Forearm Splinting. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Lee, S.K.; Kim, K.J.; Cha, Y.H.; Choy, W.S. Conservative Treatment Is Sufficient for Acute Distal Radioulnar Joint Instability with Distal Radius Fracture. Ann. Plast. Surg. 2016, 77, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Schmittenbecher, P.P. State-of-the-art treatment of forearm shaft fractures. Injury 2005, 36 (Suppl. 1), A25–A34. [Google Scholar] [CrossRef]
- Slaughter, A.; Miles, L.; Fleming, J.; McPhail, S. A Comparative Study of Splint Effectiveness in Limiting Forearm Rotation. J. Hand Ther. 2010, 23, 241–248. [Google Scholar] [CrossRef]
- Kim, J.K.; Park, E.S. The Effect of Short Arm Cast Length on Forearm Rotation. J. Hand Surg. 2014, 39, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Kook, S.H.; Kim, Y.K. Comparison of forearm rotation allowed by different types of upper extremity immobilization. J. Bone. Jt. Surg. Am. Vol. 2012, 94, 455–460. [Google Scholar] [CrossRef]
- Jung, H.S.; Park, J.G.; Park, H.J.; Lee, J.S. Postoperative immobilization using a short-arm cast in the semisupination position is appropriate after arthroscopic triangular fibrocartilage complex foveal repair. Bone Jt. J 2022, 104-b, 249–256. [Google Scholar] [CrossRef]
- Lerma, E.G.; Garcia, F.J.L.; Caraballo, A.M.; Royo, D.S. Rehabilitation in Triangular Fibrocartilage Complex Injuries: Treatment Algorithm. Rev. Iberoam. Cirugía Mano 2022, 50, e49–e59. [Google Scholar] [CrossRef]
- Handoll, H.H.; Madhok, R. Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst. Rev. 2001, Cd000314. [Google Scholar] [CrossRef]
- Bong, M.R.; Egol, K.A.; Leibman, M.; Koval, K.J. A comparison of immediate postreduction splinting constructs for controlling initial displacement of fractures of the distal radius: A prospective randomized study of long-arm versus short-arm splinting. J. Hand Surg. 2006, 31, 766–770. [Google Scholar] [CrossRef]
- Trocchia, A.M.; Elfar, J.C.; Hammert, W.C. Biomechanical measurements of forearm pronosupination with common methods of immobilization. J. Hand Surg. 2012, 37, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.M.; Montero-Lopez, N.; Hinds, R.M.; Gottschalk, M.; Melamed, E.; Capo, J.T. Assessment of Forearm Rotational Control Using 4 Upper Extremity Immobilization Constructs. Hand 2018, 13, 202–208. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sugar Tong Slab (N = 10) | Modified Ulnar Gutter Slab (N = 12) | |
|---|---|---|
| Age (year), mean (SD) | 47 (14) | 45 (19) |
| Gender (%) | ||
| Male | 5 (50) | 4 (33) |
| Female | 5 (50) | 8 (67) |
| BMI (mean) | 24.8 | 26.7 |
| Type of injury (%) | ||
| Isolated traumatic DRUJ instability | 3 (30) | 5 (41.6) |
| Distal radius fracture with DRUJ instability | 7 (70) | 7 (58.3) |
| Galeazzi fracture with DRUJ instability | 0 | 0 |
| Essex-Lopresti fracture with DRUJ instability | 0 | 0 |
| Dominant hand (%) | ||
| Right | 8 (80) | 6 (41.6) |
| Left | 2 (20) | 7 (58.3) |
| Side of operation (%) | ||
| Right | 4 (40) | 11 (91.6) |
| Left | 6 (60) | 1 (8.4) |
| Sugar Tong Slab | Modified Ulnar Gutter Slab | p-Value between 2 Groups | |
|---|---|---|---|
| DASH score | |||
| 4 weeks | 59.0 ± 14.0 | 45.3 ± 19.5 | 0.295 |
| 6 weeks | 42.6 ± 18.5 | 44.6 ± 19.7 | |
| Range of motion (degree) | |||
| Elbow flexion | |||
| 4 weeks * | 132.5 ± 8.6 | 127.5 ± 6.2 | 0.048 * |
| 6 weeks | 131.6 ± 8.6 | 127.5 ± 6.2 | |
| Extension lag | |||
| 4 weeks * | 20.0 ± 17.6 | 6.5 ± 7.9 | 0.011 * |
| 6 weeks | 5.5 ± 5.8 | 2.9 ± 4.5 | |
| Forearm supination | |||
| 4 weeks | 32.0 ± 19.0 | 35.4 ± 23.6 | 0.394 |
| 6 weeks | 61.1 ± 18.3 | 68.1 ± 17.9 | |
| Forearm pronation | |||
| 4 weeks | 36.5 ± 16.2 | 39.4 ± 27.3 | 0.732 |
| 6 weeks | 57.2 ± 15.2 | 58.7 ± 21.6 | |
| Wrist flexion | |||
| 4 weeks | 28.0 ± 6.3 | 20.9 ± 10.9 | 0.230 |
| 6 weeks | 43.3 ± 15.8 | 39.1 ± 22.3 | |
| Wrist extension | |||
| 4 weeks | 11.5 ± 11.0 | 15.3 ± 11.8 | 0.654 |
| 6 weeks | 42.7 ± 15.8 | 42.6 ± 15.0 |
| Sugar Tong Slab (N = 10) | Modified Ulnar Gutter Slab (N = 12) | |
|---|---|---|
| Piano key test | ||
| Positive | 0 | 0 |
| Negative | 10 | 12 |
| Ulnar displacement ≥ 5 mm. | ||
| Positive | 0 | 0 |
| Negative | 10 | 12 |
| Complication | ||
| Positive * | 1 | 0 |
| Negative | 9 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tawonsawatruk, T.; Phoophiboon, P.; Kanchanathepsak, T.; Tuntiyatorn, P. Comparative Analysis of Treatment Outcomes: Modified Ulnar Gutter Slab vs. Sugar Tong Slab for Distal Radioulnar Joint Instability Following Triangular Fibrocartilage Complex Repair. J. Clin. Med. 2023, 12, 6574. https://doi.org/10.3390/jcm12206574
Tawonsawatruk T, Phoophiboon P, Kanchanathepsak T, Tuntiyatorn P. Comparative Analysis of Treatment Outcomes: Modified Ulnar Gutter Slab vs. Sugar Tong Slab for Distal Radioulnar Joint Instability Following Triangular Fibrocartilage Complex Repair. Journal of Clinical Medicine. 2023; 12(20):6574. https://doi.org/10.3390/jcm12206574
Chicago/Turabian StyleTawonsawatruk, Tulyapruek, Pheeraphat Phoophiboon, Thepparat Kanchanathepsak, and Panithan Tuntiyatorn. 2023. "Comparative Analysis of Treatment Outcomes: Modified Ulnar Gutter Slab vs. Sugar Tong Slab for Distal Radioulnar Joint Instability Following Triangular Fibrocartilage Complex Repair" Journal of Clinical Medicine 12, no. 20: 6574. https://doi.org/10.3390/jcm12206574