
Morphology and Anatomical Classification of Pericardial Cavities: Oblique and Transverse Sinuses
 , , , ,
, , , , 
Abstract
:1. Introduction
1.1. Minimally Invasive Surgical Procedures Challenges
1.2. Anatomy of Pericardial Sinuses
1.3. Aim of the Study
2. Materials and Methods
2.1. Study Population
2.2. Image Processing and Analysis
2.3. Definitions
2.4. Oblique Sinus Types
2.5. Transverse Sinus Types
2.6. Statistical Analyses
3. Results
3.1. OS Morphometry
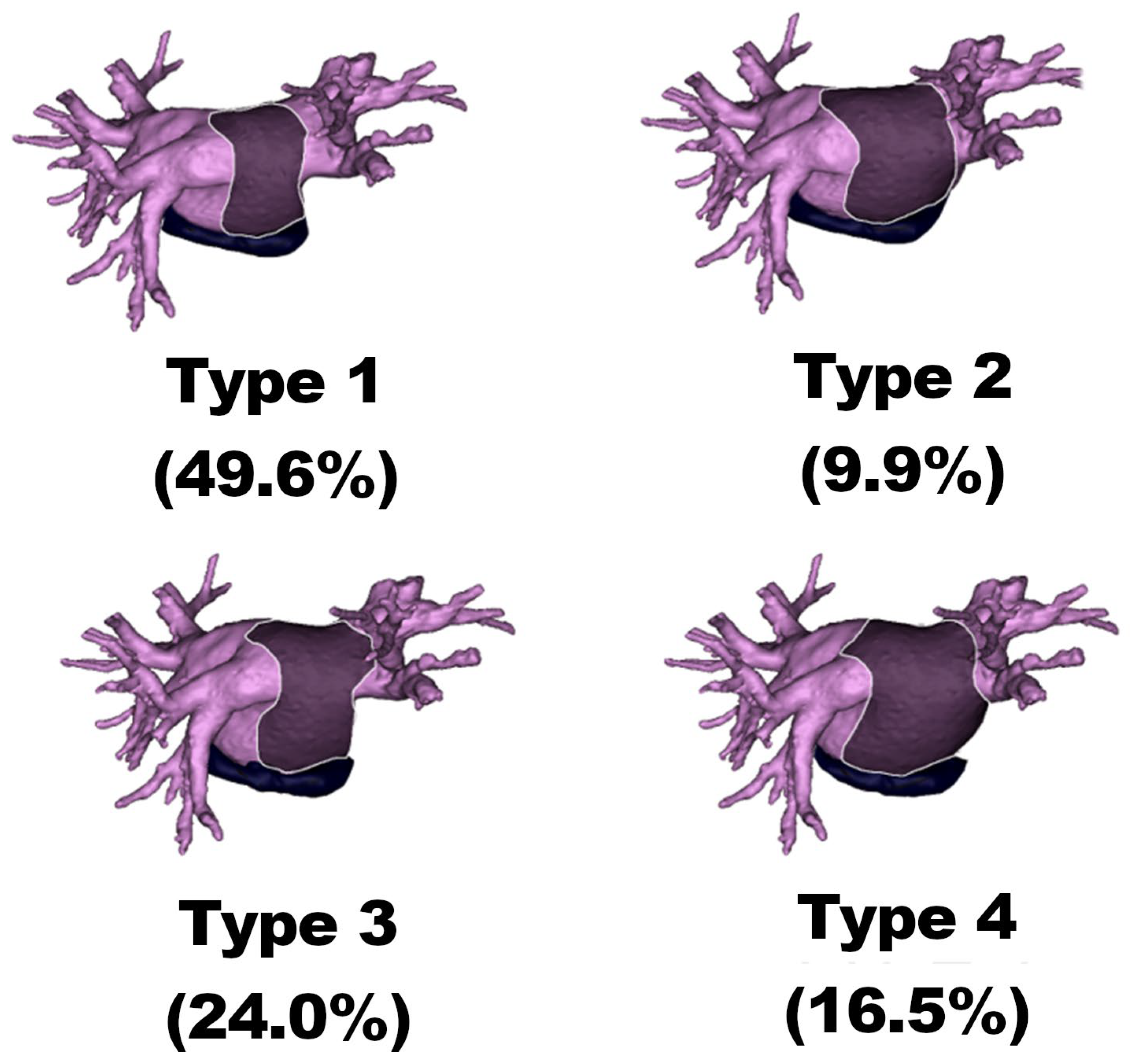
3.2. OS Types
3.2.1. Type 1
3.2.2. Type 2
3.2.3. Type 3
3.2.4. Type 4
3.3. Statistical Differences
3.4. TS Morphometry
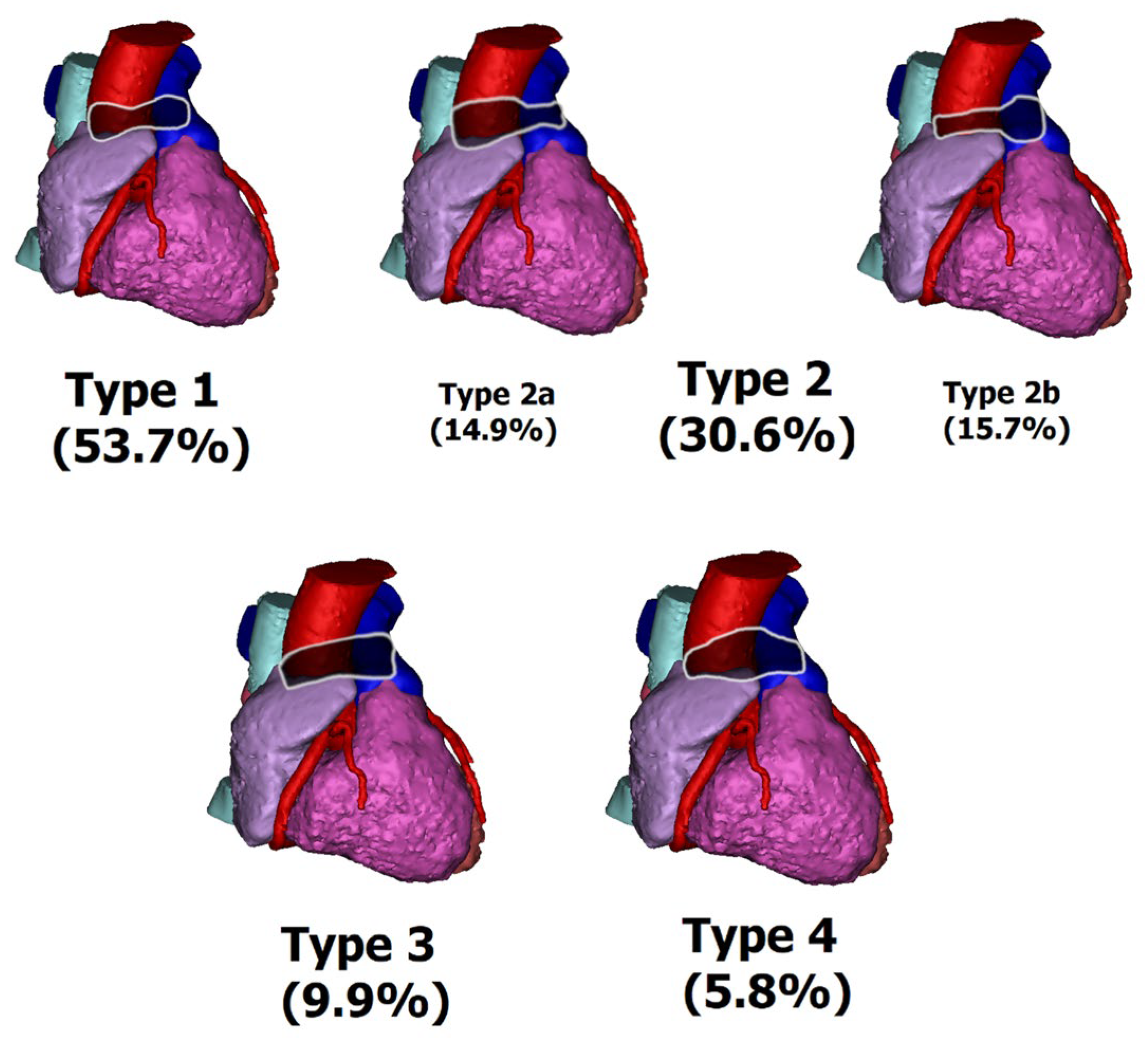
3.5. TS Types
3.5.1. Type 1 (Concave Type)
3.5.2. Type 2 (Wine Type)
3.5.3. Type 2a (Wine Bottle Type)
3.5.4. Type 2b (Wine Glass Type)
3.5.5. Type 3 (Straight Type)
3.5.6. Type 4 (Convex Type)
3.6. Statistical Differences
4. Discussion
4.1. Atrial Fibrillation Management and Treatment
4.2. Minimally Invasive Atrial Fibrillation Treatment
4.3. Video-Assisted Thoracoscopic Procedures
4.4. Lack of Anatomical Foundation for Minimally Invasive Procedures
4.5. Pericardial Sinuses Types Clinical Impact in MIAFS Procedures
4.6. Future Research Direction
- -
- Do the type of AF and prior treatment affect OS and TS types and morphometry?
- -
- Are certain TS or OS types associated with more or less intra- and post-operative complications?
- -
- Do TS or OS morphometry and types change throughout life?
- -
- What comorbidities affect TS or OS morphometry?
- -
- Does successful AF treatment affect TS and OS morphometry?
- -
- Do clinical outcomes differ between TS and OS types?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- La Meir, M.; Gelsomino, S.; Luca, F.; Pison, L.; Parise, O.; Colella, A.; Gensini, G.F.; Crijns, H.; Wellens, F.; Maessen, J.G. Minimally invasive surgical treatment of lone atrial fibrillation: Early results of hybrid versus standard minimally invasive approach employing radiofrequency sources. Int. J. Cardiol. 2013, 167, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Gelsomino, S.; Corradi, D.; Lorusso, R.; Parise, O.; Callegari, S.; Macchi, E.; Maessen, J.; La Meir, M. Anatomical basis of minimally invasive epicardial ablation of atrial fibrillation. Eur. J. Cardiothorac. Surg. 2013, 43, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Lachman, N.; Syed, F.F.; Habib, A.; Kapa, S.; Bisco, S.E.; Venkatachalam, K.L.; Asirvatham, S.J. Correlative anatomy for the electrophysiologist, Part I: The pericardial space, oblique sinus, transverse sinus. J. Cardiovasc. Electrophysiol. 2010, 21, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R.; Burysz, M.; Mazur, P.; Kapelak, B.; Bartus, M.; Lakkireddy, D.; Lee, R.J.; Malec-Litwinowicz, M.; Bartus, K. Endocardial versus epicardial left atrial appendage exclusion for stroke prevention in patients with atrial fibrillation: Midterm follow-up. J. Cardiovasc. Electrophysiol. 2021, 32, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Burysz, M.; Litwinowicz, R.; Bryndza, M.; Skowronek, R.; Ogorzeja, W.; Bartus, K. Percutaneous left atrial appendage closure using the LAmbre device. First clinical results in Poland. Postepy Kardiol. Interwencyjnej 2019, 15, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R.; Bartus, M.; Malec-Litwinowicz, M.; Michalski, M.; Banaszkiewicz, K.; Kapelak, B.; Lakkireddy, D.; Bartus, K. Left Atrial Appendage Occlusion for Secondary Stroke Prevention in Patients with Atrial Fibrillation: Long-Term Results. Cerebrovasc. Dis. 2019, 47, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Baudo, M.; Petruccelli, R.D.; D’Alonzo, M.; Rosati, F.; Benussi, S.; Di Bacco, L.; Muneretto, C. Rhythm outcomes of minimally-invasive off-pump surgical versus catheter ablation in atrial fibrillation: A meta-analysis of reconstructed time-to-event data. Int. J. Cardiol. 2023, 376, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Rattanawong, P.; Kanitsoraphan, C.; Kewcharoen, J.; Sriramoju, A.; Shanbhag, A.; Ko Ko, N.L.; Barry, T.; Vutthikraivit, W.; Shen, W.K. Surgical versus catheter ablation in atrial fibrillation: A systematic review and meta-analysis of randomized controlled trials. J. Cardiovasc. Electrophysiol. 2022, 33, 2152–2163. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Kapelak, B.; Lakkireddy, D.; Vuddanda, V.; Bartus, K. Changes in fibrinolytic activity and coagulation factors after epicardial left atrial appendage closure in patients with atrial fibrillation. J. Thorac. Dis. 2022, 14, 4226–4235. [Google Scholar] [CrossRef] [PubMed]
- Bartus, K.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Undas, A.; Kapelak, B.; Lakkireddy, D.; Lee, R.J. Coagulation factors and fibrinolytic activity in the left atrial appendage and other heart chambers in patients with atrial fibrillation: Is there a local intracardiac prothrombotic state? (HEART-CLOT study). Int. J. Cardiol. 2020, 301, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Zotov, A.; Vachev, S.; Borisov, D.; Troitskiy, A.; Khabazov, R. Thoracoscopic Pulmonary Vein and Left Atrial Posterior Wall Isolation Combined with Left Atrial Appendage Resection in Patients with Long-Standing Persistent Atrial Fibrillation. Braz. J. Cardiovasc. Surg. 2020, 35, 22–27. [Google Scholar] [CrossRef] [PubMed]
- van Laar, C.; Geuzebroek, G.S.; Hofman, F.N.; Van Putte, B.P. The totally thoracoscopic left atrial maze procedure for the treatment of atrial fibrillation. Multimed. Man. Cardiothorac. Surg. 2016, 2016, mmv043. [Google Scholar] [CrossRef] [PubMed]
- Harlaar, N.; Verberkmoes, N.J.; van der Voort, P.H.; Trines, S.A.; Verstraeten, S.E.; Mertens, B.J.A.; Klautz, R.J.M.; Braun, J.; van Brakel, T.J. Clamping versus nonclamping thoracoscopic box ablation in long-standing persistent atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2020, 160, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Batko, J.; Rams, D.; Filip, G.; Bartoszcze, A.; Kapelak, B.; Bartuś, K.; Litwinowicz, R. Left Atrial Appendage Morphology and Course of the Circumflex Artery: Anatomical Implications for Left Atrial Appendage Occlusion Procedures. Innovations 2022, 17, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Rams, D.; Batko, J.; Bartuś, K.; Filip, G.; Kowalewski, M.; Litwinowicz, R. Left Internal Mammary Artery Operative Topography for MIDCAB and TECAB Procedures. Innovations 2022, 17, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Muneretto, C.; Baudo, M.; Rosati, F.; Petruccelli, R.D.; Curnis, A.; Di Bacco, L.; Benussi, S. Thoracoscopic Surgical Ablation of Lone Atrial Fibrillation: Long-term Outcomes at 7 Years. Ann. Thorac. Surg. 2023. ahead of print. [Google Scholar] [CrossRef]
- Li, X.; Li, M.; Shao, Y.; Gu, W.; Ni, B.; Gu, J.; Chen, M. Thoracoscopic ablation delays progression from paroxysmal to persistent atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2023, 165, 1387–1394. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OS Classification | General (n = 121) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type 1 (n = 60) | Type 2 (n = 12) | Type 3 (n = 29) | Type 4 (n = 20) | |||||||
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | |
| OS volume [mL] | 6.9 | 3.7 | 9.6 | 6.6 | 8.2 | 4.5 | 13.6 | 6.0 | 8.4 | 5.3 |
| OS entry [mm] | 29.4 | 9.0 | 45.7 | 3.9 | 31.8 | 7.9 | 47.5 | 8.9 | 33.0 | 13.2 |
| OS depth [mm] | 33.2 | 5.0 | 36.2 | 5.2 | 44.5 | 5.9 | 52.1 | 13.4 | 38.2 | 11.8 |
| OS entry/height ratio | 0.9 | 0.3 | 1.3 | 0.3 | 0.7 | 0.3 | 0.9 | 0.2 | 0.9 | 0.3 |
| OS/Atrial volume ratio [%] | 2.9 | 2.0 | 3.4 | 1.5 | 2.8 | 1.3 | 3.6 | 1.2 | 3.1 | 1.7 |
| OS/LA volume ratio [%] | 5.8 | 3.1 | 7.5 | 3.9 | 5.3 | 1.8 | 6.8 | 2.2 | 5.9 | 2.9 |
| TS Classification | General (n = 121) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type I (n = 65) | Type II (n = 37) | Type IIa (n = 18) | Type IIb (n = 19) | Type III (n = 12) | Type IV (n = 7) | |||||||||
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | |
| TS volume [mL] | 14.7 | 6.9 | 15.1 | 7.7 | 16.5 | 8.5 | 14.6 | 6.7 | 15.1 | 11.5 | 13.3 | 6.8 | 14.8 | 6.5 |
| TS length [mm] | 52.9 | 17.1 | 50.6 | 17.5 | 48.7 | 25.4 | 54.5 | 15.9 | 52.2 | 19.6 | 46.3 | 24.2 | 52.8 | 17.7 |
| TS venous entry height [mm] | 12.4 | 4.0 | 13.7 | 4.9 | 16.5 | 2.8 | 11.4 | 3.7 | 13.6 | 4.6 | 9.3 | 3.6 | 12.8 | 4.3 |
| TS middle height [mm] | 6.1 | 2.4 | 11.9 | 5.2 | 13.0 | 4.1 | 9.8 | 5.7 | 13.1 | 4.3 | 21.0 | 4.8 | 8.3 | 6.2 |
| TS arterial height [mm] | 11.9 | 4.0 | 12.2 | 5.5 | 12.4 | 7.8 | 12.2 | 5.6 | 11.9 | 5.4 | 11.4 | 4.2 | 12.1 | 4.4 |
| TS/atrial volume ratio [%] | 5.3 | 3.0 | 5.4 | 2.9 | 5.6 | 4.3 | 4.8 | 2.7 | 4.8 | 2.2 | 4.2 | 2.2 | 5.0 | 2.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burysz, M.; Batko, J.; Olejek, W.; Piotrowski, M.; Litwinowicz, R.; Słomka, A.; Kowalewski, M.; Suwalski, P.; Bartuś, K.; Rams, D. Morphology and Anatomical Classification of Pericardial Cavities: Oblique and Transverse Sinuses. J. Clin. Med. 2023, 12, 4320. https://doi.org/10.3390/jcm12134320
Burysz M, Batko J, Olejek W, Piotrowski M, Litwinowicz R, Słomka A, Kowalewski M, Suwalski P, Bartuś K, Rams D. Morphology and Anatomical Classification of Pericardial Cavities: Oblique and Transverse Sinuses. Journal of Clinical Medicine. 2023; 12(13):4320. https://doi.org/10.3390/jcm12134320
Chicago/Turabian StyleBurysz, Marian, Jakub Batko, Wojciech Olejek, Michał Piotrowski, Radosław Litwinowicz, Artur Słomka, Mariusz Kowalewski, Piotr Suwalski, Krzysztof Bartuś, and Daniel Rams. 2023. "Morphology and Anatomical Classification of Pericardial Cavities: Oblique and Transverse Sinuses" Journal of Clinical Medicine 12, no. 13: 4320. https://doi.org/10.3390/jcm12134320