
Analysis of Ischemia-Modified Albumin (IMA) and Coagulation Parameters in Patients with SARS-CoV-2 Pneumonia

Abstract
:
1. Introduction
2. Material and Methods
2.1. Study Design and Participants
2.2. Clinical Classification
- Patient group admitted to the service: patients who met the following criteria by confirming the COVID-19 diagnosis through clinical exam, CT, and rRT-PCR test positivity in nasal and/or pharyngeal swab samples.
- Healthy control group: non-pregnant individuals over the age of 18 who have negative clinical examination, CT, and rRT-PCR tests, and have no additional disease.
2.3. Biochemical Analysis
2.4. Ethic
2.5. Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gussow, A.B.; Auslander, N.; Faure, G.; Wolf, Y.I.; Zhang, F.; Koonin, E.V. Genomic determinants of pathogenicity in SARS-CoV-2 and other human coronaviruses. Proc. Natl. Acad. Sci. USA 2020, 117, 15193–15199. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pang, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 19 June 2023).
- Available online: https://covid19.who.int/region/euro/country/tr (accessed on 19 June 2023).
- National Institutes of Health (NIH). COVID-19 Treatment Guidelines, Clinical Spectrum of SARS-CoV-2 Infection. 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 17 September 2022).
- Şener, G. The effectiveness of coagulation parameters in classifying patients and predicting mortality in COVİD-19. J. Exp. Clin. Med. 2022, 39, 232–236. [Google Scholar] [CrossRef]
- Castelli, V.; Cimini, A.; Ferri, C. Cytokine Storm in COVID-19: When You Come out of the Storm, You Won’t Be the Same Person Who Walked in. Front. Immunol. 2020, 11, 2132. [Google Scholar] [CrossRef]
- Wong, C.K.; Lam, C.W.K.; Wu, A.K.L.; Ip, W.K.; Lee, N.L.S.; Chan, I.H.S.; Lit, L.C.W.; Hui, D.S.C.; Chan, M.H.M.; Chung, S.S.C.; et al. Plasma inflammatory cytokines and chemokines in severe acute respiratory syndrome. Clin. Exp. Immunol. 2004, 136, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.Q. Cytokine Release Syndrome in Severe COVID-19: Interleukin-6 Receptor Antagonist Tocilizumab may be the Key to Reduce Mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Ind. J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, B.G.; Gasalla, J.M.; Sánchez-Chapado, M.; Bort, A.; Diaz-Laviada, I. Increase in Ischemia-Modified Albumin and Pregnancy-Associated Plasma Protein-A in COVID-19 Patients. J. Clin. Med. 2021, 10, 5474. [Google Scholar] [CrossRef]
- Rahman, A.; Tabassum, T.; Araf, Y.; Al Nahid, A.; Ullah, A.; Hosen, M.J. Silent hypoxia in COVID-19: Pathomechanism and possible management strategy. Mol. Biol. Rep. 2021, 48, 3863–3869. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020, 295, 200370. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health. Republic of Turkey Guidance to COVID-19 (SARS-CoV-2 İnfection). 2020. Available online: https://covid19bilgi.saglik.gov.tr (accessed on 3 March 2022).
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance V.1.2.13; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/331446 (accessed on 13 March 2020).
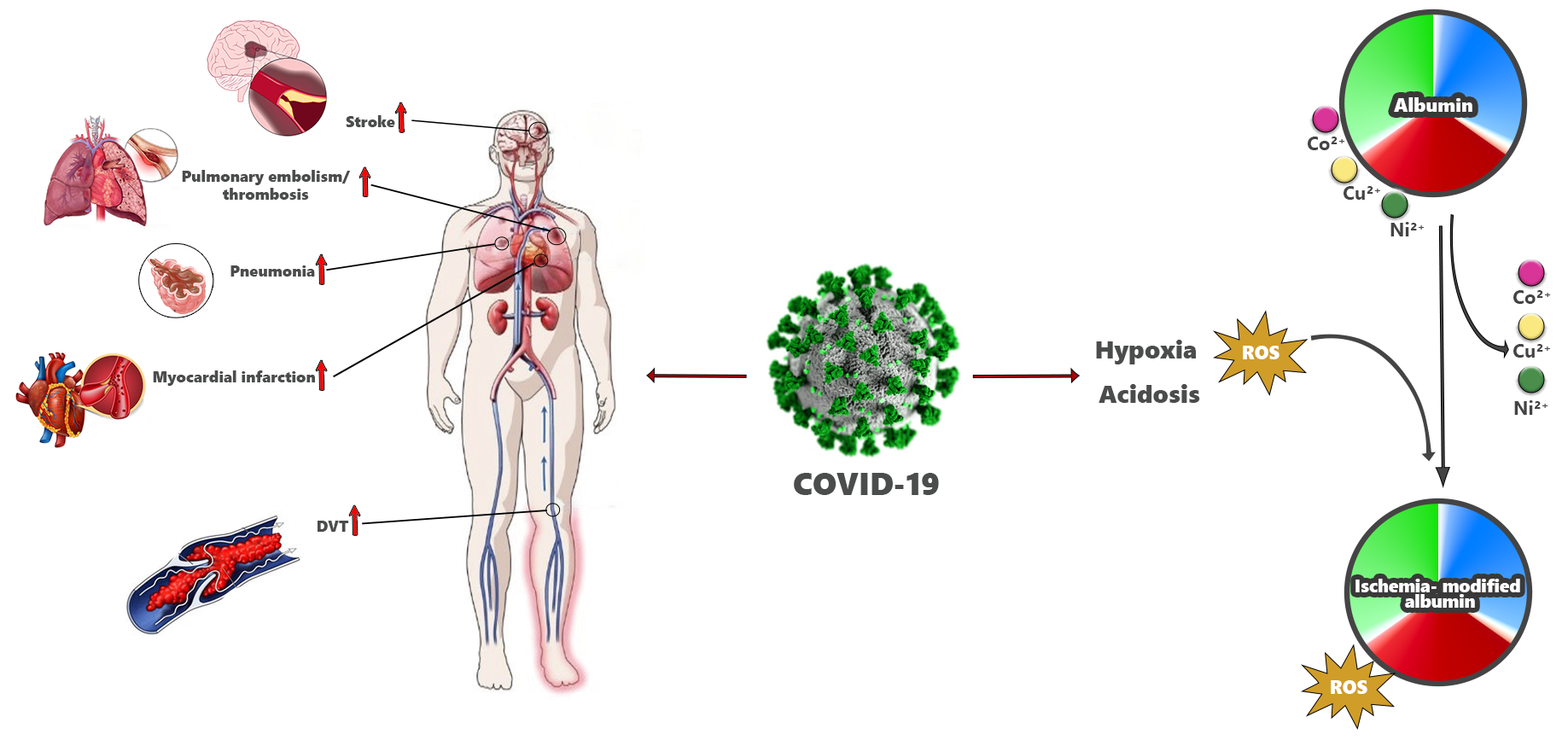
- Bar-Or, D.; Lau, E.; Winkler, J.V. A novel assay for cobalt-albumin binding and its potential as a marker for myocardial ischemia—A preliminary report. J. Emerg. Med. 2000, 19, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Samir, D. Oxidative Stress Associated with SARS-CoV-2 (COVID-19) Increases the Severity of the Lung Disease—A Systematic Review. J. Infect. Dis. Epidemiol. 2020, 6, 121–126. [Google Scholar] [CrossRef]
- Ducastel, M.; Chenevier-Gobeaux, C.; Ballaa, Y.; Meritet, J.-F.; Brack, M.; Chapuis, N.; Pene, F.; Carlier, N.; Szwebel, T.-A.; Roche, N.; et al. Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19. Int. J. Mol. Sci. 2021, 22, 7462. [Google Scholar] [CrossRef] [PubMed]
- Goud, P.T.; Bai, D.; Abu-Soud, H.M. A Multiple-Hit Hypothesis Involving Reactive Oxygen Species and Myeloperoxidase Explains Clinical Deterioration and Fatality in COVID-19. Int. J. Biol. Sci. 2021, 17, 62–72. [Google Scholar] [CrossRef]
- Koç, F.; Erdem, S.; Altunkaş, F.; Ozbek, K.; Gül, E.E.; Kurban, S.; TasYurek, E.; Erbay, E.; Sogut, E. Ischemia-modified albumin and total antioxidant status in patients with slow coronary flow: A pilot observational study. Anadolu Kardiyol. Derg. 2011, 11, 582–587. [Google Scholar] [CrossRef]
- Aykac, K.; Ozsurekci, Y.; Yayla, B.C.C.; Gurlevik, S.L.; Oygar, P.D.; Bolu, N.B.; Tasar, M.A.; Erdinc, F.S.; Ertem, G.T.; Neselioglu, S.; et al. Oxidant and antioxidant balance in patients with COVID-19. Pediatr. Pulmonol. 2021, 56, 2803–2810. [Google Scholar] [CrossRef]
- Yildiz, H.; Alp, H.H.; Ekin, S.; Arisoy, A.; Gunbatar, H.; Asker, S.; Cilingir, B.M.; Sunnetcioglu, A.; Celikel, M.; Esen, N.; et al. Analysis of endogenous oxidative damage markers and association with pulmonary involvement severity in patients with SARS-CoV-2 pneumonia. Infect. Dis. Now 2021, 51, 429–434. [Google Scholar] [CrossRef]
- Acar, T.; Ertekin, B.; Yortanli, M. Value of thiol and ischemia modified albumin (IMA) in predicting mortality in serious COVID-19 pneumonia. Heliyon 2022, 8, e12514. [Google Scholar] [CrossRef] [PubMed]
- Yucel, K.; Gurbuz, A.F. Hypoxia-inducible factor-1α and ischemia-modified albumin levels in intensive care COVID-19 Patients. Horm. Mol. Biol. Clin. Investig. 2022, 43, 415–420. [Google Scholar] [CrossRef]
- Altintas, E.; Sabirli, R.; Yuksekkaya, E.; Kurt, O.; Koseler, A. Evaluation of Serum Ischemia Modified Albumin in Patients With COVID-19 Pneumonia: A Case-Control Study. Cureus 2022, 14, e28334. [Google Scholar] [CrossRef] [PubMed]
- Tepebaşı, M.Y.; Ilhan, I.; Temel, E.N.; Sancer, O.; Öztürk, Ö. Investigation of inflammation, oxidative stress, and DNA damage in COVID-19 patients. Cell Stress Chaperones 2023, 28, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, A.-L.; Vignes, D.; Sterpu, R.; Bussone, G.; Kansau, I.; Pignon, C.; Ben Ismail, R.; Favier, M.; Molitor, J.-L.; Braham, D.; et al. Factors associated with hospital admission and adverse outcome for COVID-19: Role of social factors and medical care. Infect. Dis. Now 2022, 52, 130–137. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Mang, S.G.; Wei, C.-L.; Hong, B.; Yu, W.-N. Ischemia-modified albumin in type 2 diabetic patients with and without peripheral arterial disease. Clinics 2011, 66, 1677–1680. [Google Scholar] [CrossRef]
- Sushith, S.; Krishnamurthy, H.N.; Reshma, S.; Janice, D.; Madan, G.; Ashok, K.J.; Prathima, M.B.; Kalal, B.S. Serum Ischemia-Modified Albumin, Fibrinogen, High Sensitivity C- Reactive Proteins in Type-2 Diabetes Mellitus without Hypertension and Diabetes Mellitus with Hypertension: A Case-Control Study. Rep. Biochem. Mol. Biol. 2020, 9, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Ogihara, Y.; Yachi, S.; Takeyama, M.; Nishimoto, Y.; Tsujino, I.; Nakamura, J.; Yamamoto, N.; Nakata, H.; Ikeda, S.; Umetsu, M.; et al. CLOT-COVID Study Investigators. IInfluence of obesity on incidence of thrombosis and disease severity in patients with COVID-19: From the CLOT-COVID study. J. Cardiol. 2023, 81, 105–110. [Google Scholar] [CrossRef]
- Lawson, A.T.D.-D.; Dieng, M.; Faye, F.A.; Diaw, P.A.; Kempf, C.; Berthe, A.; Diop, M.M.; Martinot, M.; Diop, S.A. Demographics and outcomes of laboratory-confirmed COVID-19 cases during the first epidemic wave in Senegal. Infect. Dis. Now 2022, 52, 44–46. [Google Scholar] [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Sarlata, S.; Agro, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Rahmani-Kukia, N.; Abbasi, A.; Pakravan, N.; Hassan, Z.M. Measurement of oxidized albumin: An opportunity for diagnoses or treatment of COVID-19. Bioorg. Chem. 2020, 105, 104429. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Cheng, A.; Kumar, R.; Fang, Y.; Chen, G.; Zhu, Y.; Lin, S. Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity. J. Med. Virol. 2020, 92, 2152–2158. [Google Scholar] [CrossRef]
- Uyar, E.; Merdin, A.; Yamanyar, S.; Ezgü, M.C.; Artuk, C.; Taşkin, G.; Arslan, Y.; Ceritli, S. Could serum albumin value and thrombocyte/lymphocyte ratio be an important prognostic factor in determining the severity of COVID 19? Turk. J. Med. Sci. 2021, 51, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Subcommittee on Perioperative, Critical Care Thrombosis, Haemostasis of the Scientific, Standardization Committee of the International Society on Thrombosis and Hae-mostasis. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Mean ± SD | Min–Max (Median) | |
|---|---|---|
| Age | 48.48 ± 17.22 | 18–95 (48.5) |
| Ischemia-modified albumin (IMA) | 0.65 ± 0.12 | 0.39–0.97 (0.64) |
| White blood cell (WBC) | 8.09 ± 2.98 | 3.33–20.99 (7.42) |
| Hemoglobin (HGB) | 12.8 ± 1.84 | 7.7–17.6 (12.85) |
| Platelet (PLT) | 268.32 ± 84.74 | 102–577 (263) |
| Glucose | 118.19 ± 46.54 | 74–314 (100) |
| Urea | 36.49 ± 23.61 | 11.9–149.3 (30.75) |
| Creatine | 0.87 ± 0.68 | 0.39–5.13 (0.75) |
| Albumin | 3.8 ± 0.63 | 1.88–5 (3.83) |
| C-reactive protein (CRP) | 38.82 ± 62.13 | 0.33–315.93 (8.63) |
| Procalcitonin (PRC) | 0.83 ± 5.7 | 0.01–47.82 (0.04) |
| Alanin aminotransferase (ALT) | 28.23 ± 29.12 | 6–175 (18) |
| Aspartate aminotransferase (AST) | 29.59 ± 20.9 | 10–142 (23) |
| Gama glutamyl transferase (GGT) | 34.66 ± 27.89 | 9–135 (25) |
| Alkaline phosphatase (ALP) | 85.83 ± 34.56 | 34–248 (80) |
| Lactate dehydrogenase (LDH) | 255.75 ± 106 | 124–724 (222.5) |
| Prothrombin time (PT) | 13.98 ± 1.3 | 11.1–19.4 (13.8) |
| International normalized ratio (INR) | 1.09 ± 0.11 | 0.92–1.49 (1.07) |
| Activated partial thromboplastin time (APTT) | 34.52 ± 4.26 | 20.1–45.4 (34.6) |
| D-dimer | 0.41 ± 0.59 | 0.01–3.51 (0.24) |
| Fibrinogen | 430.37 ± 106.5 | 266–754 (416) |
| Ferritin | 123.85 ± 185.54 | 4.5–1053 (57.45) |
| Variables | n | IMA | p | ||
|---|---|---|---|---|---|
| Mean ± SD | Min–Max (Median) | ||||
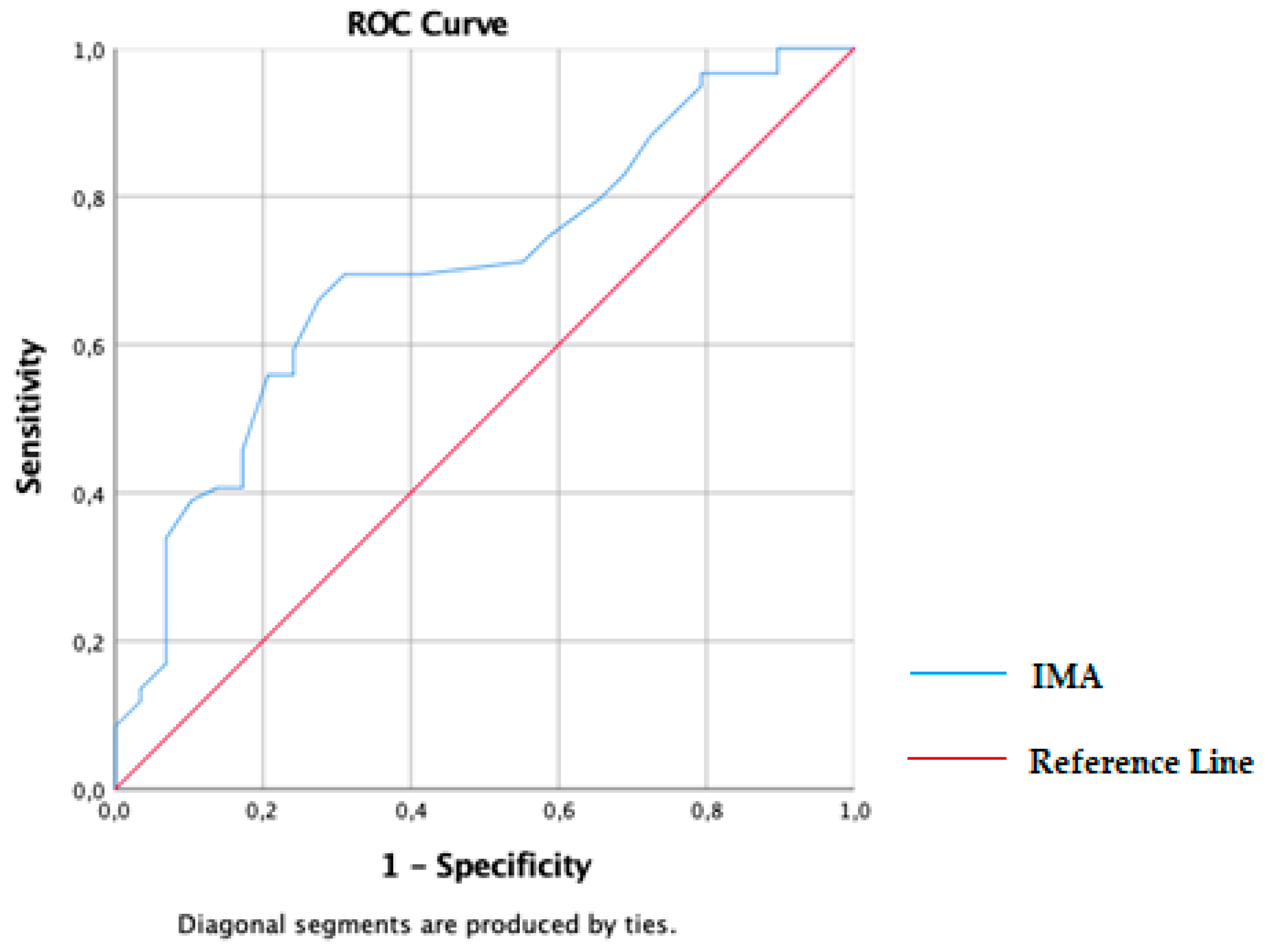
| Groups | COVID-19 | 59 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | 0.002 a |
| Control | 29 | 0.59 ± 0.1 | 0.39–0.84 (0.59) | ||
| Gender | Male | 40 | 0.66 ± 0.13 | 0.39–0.89 (0.65) | 0.433 a |
| Female | 48 | 0.65 ± 0.11 | 0.49–0.97 (0.64) | ||
| Diabetes Mellitus | Yes | 11 | 0.64 ± 0.08 | 0.54–0.8 (0.64) | 0.875 a |
| No | 77 | 0.69 ± 0.12 | 0.49–0.97 (0.68) | ||
| Hypertension | Yes | 8 | 0.66 ± 0.11 | 0.54–0.87 (0.64) | 0.983 a |
| No | 80 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | ||
| Chronic Obstructive Pulmonary Diseases | Yes | 5 | 0.67 ± 0.1 | 0.54–0.78 (0.65) | 0.620 a |
| No | 83 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | ||
| Cardiovascular Diseases | Yes | 3 | 0.68 ± 0.17 | 0.54–0.87 (0.64) | 0.854 a |
| No | 85 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | ||
| Chronic Kidney Disease | Yes | 3 | 0.65 ± 0.09 | 0.57–0.74 (0.64) | 0.918 a |
| No | 85 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | ||
| Cancer | Yes | 2 | 0.68 ± 0.01 | 0.67–0.68 (0.68) | 0.538 a |
| No | 87 | 0.68 ± 0.11 | 0.49–0.97 (0.67) | ||
| COVID-19 Pneumonic Infiltration | Control | 29 | 0.59 ± 0.1 | 0.39–0.84 (0.59) | 0.007 b |
| Unilateral | 12 | 0.7 ± 0.14 | 0.49–0.89 (0.73) | ||
| Bilateral | 47 | 0.67 ± 0.1 | 0.53–0.97 (0.67) | ||
| Classifications of COVID-19 Pneumonic Infiltration on chest CT | 0-none (0%) | 29 | 0.59 ± 0.1 | 0.39–0.84 (0.59) | 0.001 b |
| 1-mild (1–50%) | 13 | 0.67 ± 0.13 | 0.49–0.84 (0.68) | ||
| 2-moderate (51–75%) | 34 | 0.68 ± 0.11 | 0.53–0.97 (0.67) | ||
| 3-severe (76–100%) | 12 | 0.69 ± 0.1 | 0.54–0.87 (0.67) | ||
| Variables | Groups | n | Mean ± SD | Min–Max (Median) | p |
|---|---|---|---|---|---|
| Age | COVID-19 | 59 | 53.03 ± 17.36 | 19–95 (54) | 0.001 |
| Control | 29 | 39.21 ± 12.8 | 18–68 (37) | ||
| Glucose | COVID-19 | 59 | 129.78 ± 53.89 | 74–314 (106.5) | 0.003 |
| Control | 29 | 98.21 ± 17.3 | 78–157 (95) | ||
| Urea | COVID-19 | 59 | 37.43 ± 25.75 | 11.9–149.3 (30.35) | 0.881 |
| Control | 29 | 32.58 ± 10.73 | 17.5–52.3 (32.2) | ||
| Creatinine | COVID-19 | 59 | 0.96 ± 0.82 | 0.39–5.13 (0.78) | 0.091 |
| Control | 29 | 0.7 ± 0.15 | 0.47–0.96 (0.74) | ||
| Albumin | COVID-19 | 59 | 3.6 ± 0.58 | 1.88–4.86 (3.65) | 0.001 |
| Control | 29 | 4.39 ± 0.34 | 3.57–5 (4.33) | ||
| C-reactive protein (CRP) | COVID-19 | 59 | 56.99 ± 69.38 | 1.34–315.93 (23.1) | 0.001 |
| Control | 29 | 5.89 ± 20.11 | 0.33–110 (1.86) | ||
| Procalcitonin (PRC) | COVID-19 | 59 | 1.32 ± 7.22 | 0.01–47.82 (0.06) | 0.001 |
| Control | 29 | 0.02 ± 0.02 | 0.01–0.09 (0.02) | ||
| Alanin aminotransferase (ALT) | COVID-19 | 59 | 30.23 ± 32.42 | 6–175 (20) | 0.304 |
| Control | 29 | 24.24 ± 21 | 7–100 (16) | ||
| Aspartate aminotransferase (AST) | COVID-19 | 59 | 33.4 ± 24.02 | 10–142 (25) | 0.002 |
| Control | 29 | 22.1 ± 9.21 | 13–53 (19) | ||
| Gama glutamyl transferase (GGT) | COVID-19 | 59 | 38.47 ± 29.82 | 11–135 (27) | 0.026 |
| Control | 29 | 22.08 ± 15.14 | 9–64 (18) | ||
| Alkaline phosphatase (ALP) | COVID-19 | 59 | 90.34 ± 39.17 | 34–248 (80) | 0.334 |
| Control | 29 | 79.21 ± 25.66 | 38–148 (78.5) | ||
| Lactate dehydrogenase (LDH) | COVID-19 | 59 | 291.48 ± 112.38 | 162–724 (248.5) | 0.001 |
| Control | 29 | 184.29 ± 29.76 | 124–261 (185.5) | ||
| Ferritin | COVID-19 | 59 | 206.63 ± 228.03 | 6.9–1053 (105.6) | 0.001 |
| Control | 29 | 35.36 ± 33.56 | 4.5–121.8 (22.7) |
| Variables | Groups | n | Mean ± SD | Min–Max (Median) | p |
|---|---|---|---|---|---|
| White blood cell | COVID-19 | 59 | 8.34 ± 3.49 | 3.33–20.99 (7.3) | 0.878 |
| Control | 29 | 7.58 ± 1.41 | 4.79–9.46 (7.55) | ||
| Hemoglobin | COVID-19 | 59 | 12.72 ± 1.82 | 8.6–17.6 (12.8) | 0.651 |
| Control | 29 | 12.96 ± 1.91 | 7.7–16.4 (12.9) | ||
| Platelet | COVID-19 | 59 | 262.09 ± 93.04 | 102–577 (255) | 0.141 |
| Control | 29 | 280.79 ± 64.76 | 158–422 (271) | ||
| PT | COVID-19 | 59 | 14.24 ± 1.48 | 11.1–19.4 (14) | 0.040 |
| Control | 29 | 13.65 ± 0.95 | 12.3–16.6 (13.5) | ||
| INR | COVID-19 | 59 | 1.11 ± 0.12 | 0.92–1.49 (1.09) | 0.044 |
| Control | 29 | 1.06 ± 0.09 | 0.93–1.34 (1.04) | ||
| APTT | COVID-19 | 59 | 34.87 ± 5.11 | 20.1–45.4 (35.1) | 0.337 |
| Control | 29 | 34.13 ± 3.06 | 28.6–40.8 (33.6) | ||
| D-dimer | COVID-19 | 59 | 0.5 ± 0.69 | 0.08–3.51 (0.25) | 0.007 |
| Control | 29 | 0.28 ± 0.37 | 0.01–1.8 (0.15) | ||
| Fibrinogen | COVID-19 | 59 | 476.97 ± 105.07 | 281–754 (473.5) | 0.001 |
| Control | 29 | 375.72 ± 79.86 | 266–675 (356) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. IMA | r | 1 | ||||||||||||
| p | ||||||||||||||
| 2. Age | r | 0.154 | 1 | |||||||||||
| p | 0.246 | |||||||||||||
| 3. WBC | r | 0.065 | 0.013 | 1 | ||||||||||
| p | 0.630 | 0.920 | ||||||||||||
| 4. Hemoglobin | r | 0.125 | −0.227 | −0.038 | 1 | |||||||||
| p | 0.354 | 0.089 | 0.777 | |||||||||||
| 5. PLT | r | −0.091 | −0.099 | 0.325 * | 0.004 | 1 | ||||||||
| p | 0.499 | 0.460 | 0.013 | 0.979 | ||||||||||
| 6. CRP | r | 0.085 | 0.07 | 0.205 | 0 | 0.122 | 1 | |||||||
| p | 0.526 | 0.602 | 0.127 | 0.157 | 0.365 | |||||||||
| 7. PRC | r | 0.207 | 0.264 | 0.265 | −0.244 | 0 | 0.513 ** | 1 | ||||||
| p | 0.178 | 0.083 | 0.086 | 0.120 | 0.68 | 0.000 | ||||||||
| 8. PT | r | −0.033 | −0.096 | 0.149 | −0.184 | 0.026 | −0.045 | −0.165 | 1 | |||||
| p | 0.845 | 0.572 | 0.379 | 0.283 | 0.881 | 0.793 | 0.367 | |||||||
| 9. INR | r | −0.055 | −0.109 | 0.156 | −0.181 | 0.019 | −0.064 | −0.181 | 0.998 ** | 1 | ||||
| p | 0.746 | 0.522 | 0.355 | 0.291 | 0.911 | 0.711 | 0.321 | 0.000 | ||||||
| 10. APTT | r | −0.061 | 0.03 | −0.045 | −0.480 ** | −0.137 | 0.056 | −0.113 | 0.084 | 0.094 | 1 | |||
| p | 0.734 | 0.869 | 0.803 | 0.005 | 0.449 | 0.761 | 0.566 | 0.646 | 0.609 | |||||
| 11. D−dimer | r | 0.077 | −0.012 | 0.433 ** | −0.305 * | 0.201 | 0.303 * | 0.397 * | 0.169 | 0.158 | 0.266 | 1 | ||
| p | 0.615 | 0.938 | 0.003 | 0.047 | 0.191 | 0.043 | 0.018 | 0.389 | 0.421 | 0.208 | ||||
| 12. Fibrinogen | r | 0.011 | −0.17 | −0.073 | −0.112 | 0.029 | 0.577 ** | −0.006 | 0.01 | −0.013 | −0.062 | −0.058 | 1 | |
| p | 0.951 | 0.337 | 0.683 | 0.536 | 0.872 | 0.000 | 0.975 | 0.962 | 0.950 | 0.770 | 0.771 | |||
| 13. Ferritin | r | 0.207 | −0.233 | −0.366 * | 0.413 * | −0.415 * | 0.05 | 0.263 | −0.265 | −0.283 | −0.437 * | −0.303 | 0.129 | 1 |
| p | 0.265 | 0.206 | 0.046 | 0.026 | 0.023 | 0.793 | 0.185 | 0.221 | 0.190 | 0.037 | 0.141 | 0.578 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saglam, E.; Sener, G.; Bayrak, T.; Bayrak, A.; Gorgulu, N. Analysis of Ischemia-Modified Albumin (IMA) and Coagulation Parameters in Patients with SARS-CoV-2 Pneumonia. J. Clin. Med. 2023, 12, 4304. https://doi.org/10.3390/jcm12134304
Saglam E, Sener G, Bayrak T, Bayrak A, Gorgulu N. Analysis of Ischemia-Modified Albumin (IMA) and Coagulation Parameters in Patients with SARS-CoV-2 Pneumonia. Journal of Clinical Medicine. 2023; 12(13):4304. https://doi.org/10.3390/jcm12134304
Chicago/Turabian StyleSaglam, Emel, Gulsen Sener, Tulin Bayrak, Ahmet Bayrak, and Numan Gorgulu. 2023. "Analysis of Ischemia-Modified Albumin (IMA) and Coagulation Parameters in Patients with SARS-CoV-2 Pneumonia" Journal of Clinical Medicine 12, no. 13: 4304. https://doi.org/10.3390/jcm12134304