

Trends and Risk Factors for Surgical Site Infection after Treatment of the Ankle Fracture: National Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
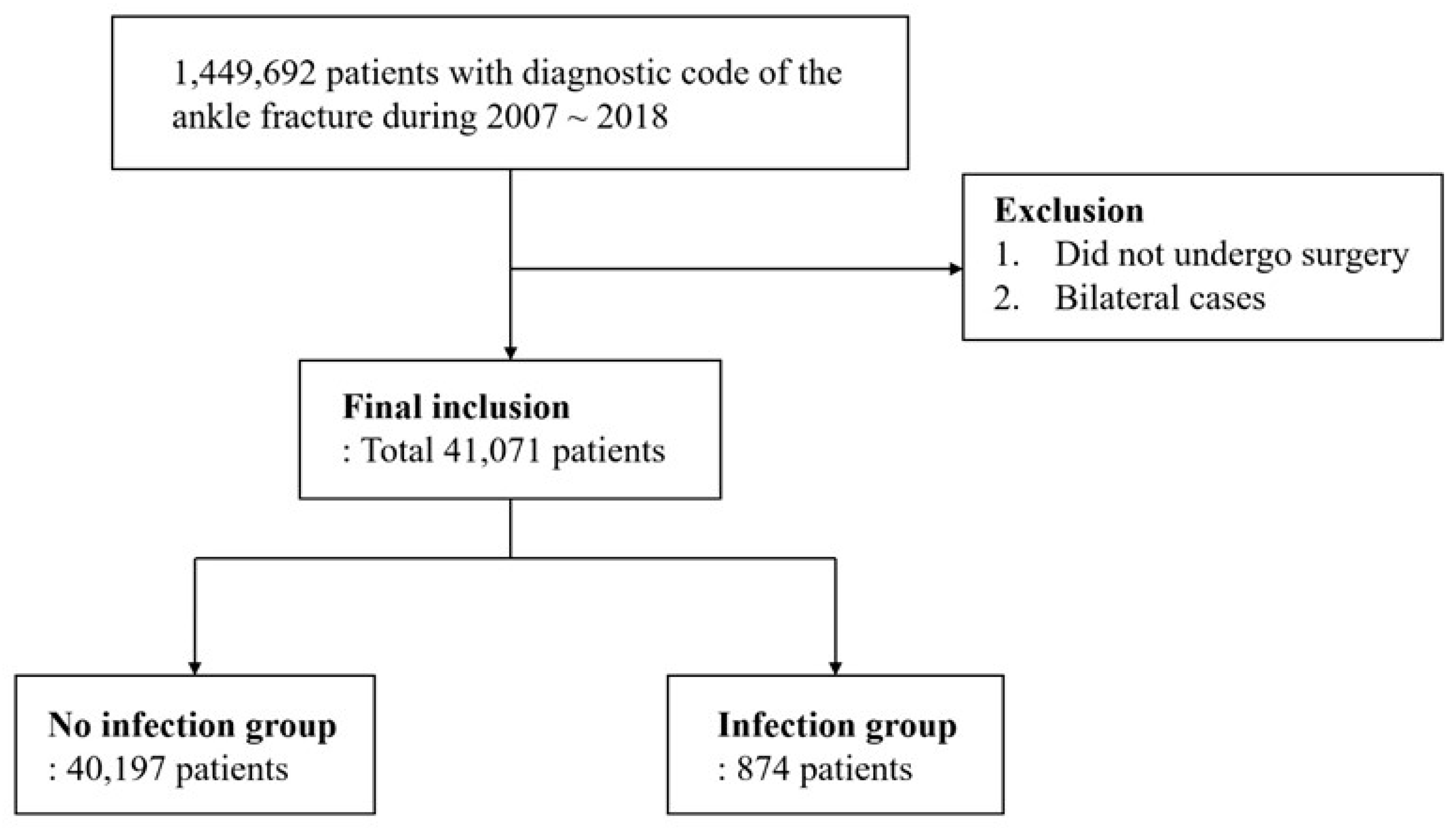
2.2. Study Design and Participants
2.3. Definition of the SSI
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amin, S.; Achenbach, S.J.; Atkinson, E.J.; Khosla, S.; Melton, L.J. Trends in Fracture Incidence: A Population-Based Study Over 20 Years. J. Bone Miner. Res. 2013, 29, 581–589. [Google Scholar] [CrossRef]
- Shibuya, N.; Davis, M.L.; Jupiter, D.C. Epidemiology of Foot and Ankle Fractures in the United States: An Analysis of the National Trauma Data Bank (2007 to 2011). J. Foot Ankle Surg. 2014, 53, 606–608. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, H.; Tang, Y.; Zhao, H.; Qin, S.; Xu, L.; Xia, Z.; Zhang, F. Incidence and risk factors for surgical site infection after open reduction and internal fixation of ankle fracture: A retrospective multicenter study. Medicine 2018, 97, e9901. [Google Scholar] [CrossRef]
- Sato, T.; Takegami, Y.; Sugino, T.; Bando, K.; Fujita, T.; Imagama, S. Smoking and trimalleolar fractures are risk factors for infection after open reduction and internal fixation of closed ankle fractures: A multicenter retrospective study of 1,201 fractures. Injury 2021, 52, 1959–1963. [Google Scholar] [CrossRef]
- Zalavras, C.G.; Christensen, T.; Rigopoulos, N.; Holtom, P.; Patzakis, M.J. Infection Following Operative Treatment of Ankle Fractures. Clin. Orthop. Relat. Res. 2009, 467, 1715–1720. [Google Scholar] [CrossRef] [Green Version]
- SooHoo, N.F.; Krenek, L.; Eagan, M.J.; Gurbani, B.; Ko, C.Y.; Zingmond, D.S. Complication Rates Following Open Reduction and Internal Fixation of Ankle Fractures. J. Bone Jt. Surg. 2009, 91, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Sun, T.; Zhang, F.; Qin, S.; Li, Y.; Zhao, H. Deep surgical site infection after ankle fractures treated by open reduction and internal fixation in adults: A retrospective case-control study. Int. Wound J. 2018, 15, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.G.; Sigurdsen, U.; Utvåg, S.E.; Stavem, K. Functional outcomes following surgical-site infections after operative fixation of closed ankle fractures. Foot Ankle Surg. 2017, 23, 311–316. [Google Scholar] [CrossRef]
- Metsemakers, W.-J.; Smeets, B.; Nijs, S.; Hoekstra, H. Infection after fracture fixation of the tibia: Analysis of healthcare utilization and related costs. Injury 2017, 48, 1204–1210. [Google Scholar] [CrossRef]
- Olesen, U.K.; Pedersen, N.J.; Eckardt, H.; Lykke-Meyer, L.; Bonde, C.T.; Singh, U.M.; McNally, M. The cost of infection in severe open tibial fractures treated with a free flap. Int. Orthop. 2017, 41, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Depypere, M.; Morgenstern, M.; Kuehl, R.; Senneville, E.; Moriarty, T.F.; Obremskey, W.T.; Zimmerli, W.; Trampuz, A.; Lagrou, K.; Metsemakers, W.-J. Pathogenesis and management of fracture-related infection. Clin. Microbiol. Infect. 2020, 26, 572–578. [Google Scholar] [CrossRef]
- Ovaska, M.T.; Mäkinen, T.J.; Madanat, R.; Vahlberg, T.; Hirvensalo, E.; Lindahl, J. Predictors of poor outcomes following deep infection after internal fixation of ankle fractures. Injury 2013, 44, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Korim, M.T.; Payne, R.M.; Bhatia, M. A case–control study of surgical site infection following operative fixation of fractures of the ankle in a large UK trauma unit. Bone Jt. J. 2014, 96, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Bezstarosti, H.; Van Lieshout, E.M.M.; Voskamp, L.W.; Kortram, K.; Obremskey, W.; McNally, M.A.; Metsemakers, W.J.; Verhofstad, M.H.J. Insights into treatment and outcome of fracture-related infection: A systematic literature review. Arch. Orthop. Trauma Surg. 2019, 139, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, N.; Sofianos, D.; Berkes, M.B.; Obremskey, W.T. Prevention of Perioperative Infection. J. Bone Jt. Surg. 2007, 89, 1605–1618. [Google Scholar] [CrossRef]
- Bosco, J.A.; Slover, J.D.; Haas, J.P. Perioperative strategies for decreasing infection: A comprehensive evidence-based approach. J. Bone Jt. Surg. 2010, 92, 232–239. [Google Scholar]
- Nåsell, H.; Ottosson, C.; Törnqvist, H.; Lindé, J.; Ponzer, S. The Impact of Smoking on Complications After Operatively Treated Ankle Fractures—A Follow-Up Study of 906 Patients. J. Orthop. Trauma 2011, 25, 748–755. [Google Scholar] [CrossRef]
- Ovaska, M.T.; Mäkinen, T.J.; Madanat, R.; Huotari, K.; Vahlberg, T.; Hirvensalo, E.; Lindahl, J. Risk Factors for Deep Surgical Site Infection Following Operative Treatment of Ankle Fractures. J. Bone Jt. Surg. 2013, 95, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.G.; Margules, A.; Raikin, S.M. Risk Factors for Wound Complications After Ankle Fracture Surgery. J. Bone Jt. Surg. 2012, 94, 2047–2052. [Google Scholar] [CrossRef] [Green Version]
- Olsen, L.L.; Møller, A.M.; Brorson, S.; Hasselager, R.B.; Sort, R. The impact of lifestyle risk factors on the rate of infection after surgery for a fracture of the ankle. Bone Jt. J. 2017, 99, 225–230. [Google Scholar] [CrossRef]
- Richardson, N.G.; Swiggett, S.J.; Pasternack, J.B.; Vakharia, R.M.; Kang, K.K.; Abdelgawad, A. Comparison study of patient demographics and risk factors for surgical site infections following open reduction and internal fixation for lateral malleolar ankle fractures within the medicare population. Foot Ankle Surg. 2021, 27, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhu, Y.; Chen, W.; Li, M.; Liu, S.; Zhang, Y. Multiple preoperative biomarkers are associated with incidence of surgical site infection following surgeries of ankle fractures. Int. Wound J. 2020, 17, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E.G.; Cashman, J.P.; Groarke, P.J.; Morris, S.F. Risk factors for surgical site infection following operative ankle fracture fixation. Ir. J. Med. Sci. 2013, 182, 453–456. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Number of Patients | 41,071 |
|---|---|
| Age (years) | 47.3 ± 18.64 |
| Sex (male:female) | 22,064:19,007 |
| Hospital day (day) | 16.7 ± 12.69 |
| Fracture type (closed:open) | 38,942:2129 |
| Fixation type (CRIF:ORIF) * | 1220:39,851 |
| Hospital grade (A/B/C/D) ** | 2870/15,155/16,368/6678 |
| Periprosthetic infection (n, %) | 874 (2.13%) |
| Mean time of SSI *** (days, mean, SD) | 35.8 ± 28.02 |
| Treatment for SSI (A:B:C) **** | 744 (85.1%):93 (10.6%):37 (4.3%) |
| No Infection | Infection | p Value | |
|---|---|---|---|
| Number of patients | 40,197 | 874 | |
| Age (mean, standard deviation) | 47.2 ± 18.61 | 49.7 ± 19.99 | <0.001 |
| Sex (male: female) | 21,484:18,713 (53.4%: 46.6%) | 580:294 (66.4%: 33.6%) | <0.001 |
| Admission duration (day) | 17.3 ± 11.27 | 16.4 ± 10.3 | 0.300 |
| Season | <0.001 | ||
| Spring | 9420 | 191 | |
| Summer | 8486 | 231 | |
| Fall | 9658 | 238 | |
| Winter | 12633 | 214 | |
| Fracture type (closed/open) * | 38,226/1971 (95.1%: 4.9%) | 716/158 (81.9%: 18.1%) | <0.001 |
| Fixation type (CRIF/ORIF) ** | 1195/39,002 | 25/849 | 0.926 |
| Hospital grade (A/B/C/D) | 2827/14,899/15,994/6477 (7.0%/37.1%/39.8%/16.1%) | 43/256/374/201 (4.9%/29.3%/42.8%/23.0%) | <0.001 |
| Comorbidities (n, %) | |||
| Myocardial infarction | 484 (1.2%) | 21 (2.4%) | 0.003 |
| Congestive heart failure | 1091 (2.7%) | 32 (3.7%) | 0.111 |
| Peripheral vascular disease | 3839 (9.6%) | 80 (9.2%) | 0.736 |
| Cerebrovascular disease | 2053 (5.1%) | 65 (7.4%) | 0.003 |
| Dementia | 522 (1.3%) | 23 (2.6%) | 0.001 |
| Chronic pulmonary disease | 8048 (20.0%) | 187 (21.4%) | 0.336 |
| Connective tissue disease | 2668 (6.6%) | 52 (5.9%) | 0.459 |
| Peptic ulcer | 8505 (21.2%) | 197 (22.5%) | 0.344 |
| Liver disease | 6704 (16.7%) | 161 (18.4%) | 0.187 |
| Diabetes | 3857 (9.6%) | 93 (10.6%) | 0.328 |
| Hemiplegia | 508 (1.3%) | 19 (2.2%) | 0.027 |
| Cancer (no metastasis) | 921 (2.3%) | 26 (3.0%) | 0.223 |
| Cancer (metastasis) | 215 (0.5%) | 8 (0.9%) | 0.200 |
| Acute renal failure | 303 (0.8%) | 10 (1.1%) | 0.264 |
| Chronic renal failure | 51 (0.1%) | 1 (0.1%) | 1.000 |
| Rheumatoid arthritis | 390 (1.0%) | 5 (0.6%) | 0.309 |
| Osteoporosis | 2174 (5.4%) | 47 (5.4%) | 1.000 |
| Hyperlipidemia | 3677 (9.1%) | 92 (10.5%) | 0.181 |
| Crude OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
|---|---|---|---|---|
| Season | ||||
| Spring | Reference | Reference | ||
| Summer | 1.343 (1.106–1.631) | 0.003 | 1.349 (1.110–1.641) | 0.003 |
| Autumn | 1.215 (1.003–1.475) | 0.047 | 1.221 (1.007–1.484) | 0.043 |
| Winter | 0.835 (0.686–1.018) | 0.074 | 0.850 (0.697–1.036) | 0.107 |
| Sex (female as reference) | 1.718 (1.493–1.982) | <0.001 | 1.841 (1.590–2.136) | <0.001 |
| Age | 1.007 (1.004–1.011) | <0.001 | 1.010 (1.006–1.014) | <0.001 |
| Fixation type (CRIF vs. ORIF) | 1.041 (0.712–1.596) | 0.846 | 0.945 (0.645–1.453) | 0.783 |
| Open fracture | 4.280 (3.51–5.100) | <0.001 | 4.220 (3.515–5.038) | <0.001 |
| Comorbidities | ||||
| Myocardial infarction | 2.020 (1.259–3.061) | 0.002 | 1.628 (0.998–2.516) | 0.038 |
| Congestive heart failure | 1.362 (0.933–1.915) | 0.091 | 1.184 (0.799–1.694) | 0.377 |
| Peripheral vascular disease | 0.954 (0.751–1.196) | 0.693 | 0.823 (0.638–1.049) | 0.124 |
| Cerebrovascular disease | 1.493 (1.144–1.913) | 0.002 | 1.274 (0.957–1.671) | 0.088 |
| Dementia | 2.054 (1.308–3.061) | 0.001 | 1.720 (1.074–2.628) | 0.017 |
| Chronic pulmonary disease | 1.087 (0.921–1.277) | 0.315 | 1.147 (0.965–1.358) | 0.114 |
| Connective tissue disease | 0.890 (0.663–1.168) | 0.419 | 0.862 (0.635–1.145) | 0.322 |
| Peptic ulcer | 1.084 (0.921–1.270) | 0.323 | 1.034 (0.871–1.222) | 0.702 |
| Liver disease | 1.128 (0.946–1.337) | 0.172 | 1.057 (0.874–1.273) | 0.561 |
| Diabetes | 1.122 (0.897–1.387) | 0.300 | 0.956 (0.752–1.204) | 0.709 |
| Hemiplegia | 1.736 (1.056–2.679) | 0.020 | 1.313 (0.787–2.062) | 0.266 |
| Cancer (no metastasis) | 1.308 (0.859–1.900) | 0.184 | 1.036 (0.671–1.529) | 0.867 |
| Cancer (metastasis) | 1.718 (0.775–3.261) | 0.135 | 1.563 (0.695–3.033) | 0.229 |
| Acute renal failure | 1.524 (0.755–2.717) | 0.192 | 1.201 (0.587–2.184) | 0.582 |
| Chronic renal failure | 0.902 (0.051–4.111) | 0.918 | 0.575 (0.032–2.720) | 0.588 |
| Rheumatoid arthritis | 0.587 (0.209–1.276) | 0.238 | 0.531 (0.188–1.163) | 0.164 |
| Osteoporosis | 0.994 (0.729–1.322) | 0.968 | 0.944 (0.683–1.274) | 0.716 |
| Hyperlipidemia | 1.168 (0.933–1.446) | 0.163 | 1.099 (0.866–1.380) | 0.426 |
| Charlson comorbidity index | ||||
| 0~2 (n = 27746) | Reference | Reference | ||
| 3–5 (n = 6499) | 1.481 (1.189–1.840) | <0.001 | 1.484 (1.191–1.843) | <0.001 |
| 6- (n = 2047) | 1.725 (1.258–2.340) | 0.001 | 1.730 (1.261–2.345) | <0.001 |
| Odds Ratio (95% CI) | p Value | |
|---|---|---|
| Child Group (n = 2358) | ||
| Season | ||
| Spring | Reference | |
| Summer | 2.219 (0.960–5.397) | 0.066 |
| Autumn | 1.281 (0.524–3.210) | 0.586 |
| Winter | 0.623 (0.190–1.819) | 0.400 |
| Fixation type | 6.190 (1.330–110.245) | 0.073 |
| Open fracture | 4.804 (1.760–11.151) | 0.001 |
| Adult Group (n = 31,298) | ||
| Season | ||
| Spring | Reference | |
| Summer | 1.350 (1.070–1.707) | 0.012 |
| Autumn | 1.233 (0.981–1.554) | 0.074 |
| Winter | 0.862 (0.681–1.093) | 0.218 |
| Sex | 1.870 (1.570–2.237) | <0.001 |
| Open fracture | 4.837 (3.933–5.908) | <0.001 |
| Cerebrovascular disease | 1.550 (1.034–2.230) | 0.025 |
| Chronic pulmonary disease | 1.297 (1.062–1.572) | 0.009 |
| Rheumatic arthritis | 0.185 (0.011–0.827) | 0.092 |
| Elderly Group (n = 7415) | ||
| Sex | 1.921 (1.467–2.520) | <0.001 |
| Age | 1.042 (1.017–1.066) | 0.001 |
| Open fracture | 2.570 (1.628–3.893) | <0.001 |
| Myocardial infarction | 1.694 (0.939–2.844) | 0.060 |
| Peripheral vascular disease | 0.721 (0.499–1.019) | 0.060 |
| Dementia | 1.578 (0.908–2.571) | 0.084 |
| Liver disease | 1.365 (1.008–1.832) | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.-J.; Kwon, Y.-M.; Byeon, S.-j.; Kim, H.N.; Sung, I.-H.; Subramanian, S.A.; Kim, S.J. Trends and Risk Factors for Surgical Site Infection after Treatment of the Ankle Fracture: National Cohort Study. J. Clin. Med. 2023, 12, 4215. https://doi.org/10.3390/jcm12134215
Kang H-J, Kwon Y-M, Byeon S-j, Kim HN, Sung I-H, Subramanian SA, Kim SJ. Trends and Risk Factors for Surgical Site Infection after Treatment of the Ankle Fracture: National Cohort Study. Journal of Clinical Medicine. 2023; 12(13):4215. https://doi.org/10.3390/jcm12134215
Chicago/Turabian StyleKang, Hwa-Jun, Young-Min Kwon, Sun-ju Byeon, Hyong Nyun Kim, Il-Hoon Sung, Sivakumar Allur Subramanian, and Sung Jae Kim. 2023. "Trends and Risk Factors for Surgical Site Infection after Treatment of the Ankle Fracture: National Cohort Study" Journal of Clinical Medicine 12, no. 13: 4215. https://doi.org/10.3390/jcm12134215